
Abstract
Purpose:
The purpose of this study was to determine the incidence and trends of both hip spica casting and elastic stable intramedullary nailing in children aged 2–12 years who sustained femoral diaphyseal fracture between 1998 and 2016 in Finland. We also evaluated the actual hospital costs of both treatment methods as well as calculating the length of hospital stay.
Methods:
This study included all 2- to 12-year-old children with femoral diaphyseal fracture who were treated in Finland between 1998 and 2016. Data were collected from the National Hospital Discharge Register of Finland. Children were classified by age into five groups. The annual incidences per 100,000 persons were calculated using annual mid-year population census data obtained from Statistics Finland. Data on the annual actual daily hospital costs were collected from the Finnish Institute for Health and Welfare.
Results:
In total, 1064 patients aged 2–12 years who had sustained femoral diaphyseal fracture were treated with elastic stable intramedullary nailing or hip spica casting between 1998 and 2016. In children aged 4–5 years, the incidence of elastic stable intramedullary nailing increased during the study period from 5.4 per 100,000 persons in 1998 to 8.1 per 100,000 persons in 2016.
Conclusions:
The length of hospitalization in patients treated with elastic stable intramedullary nailing was shorter and, therefore, the total costs of hospital treatment were lower than in those children treated with hip spica cast.
Level of evidence:
level III.
Introduction
Femoral fractures in growing children are rare, accounting for less than 2% of all fractures in children. However, they represent the most common musculoskeletal injury requiring hospitalization in childhood.1,2 Based on our recent research, the incidence of femoral fractures in Finnish children younger than 17 was 13.3 per 100,000 persons, and around 70% of pediatric patients with femoral fractures were boys. 3 The majority of femoral fractures were located on the femoral shaft, with an incidence of 11.6 per 100,000 persons in boys and 3.5 per 100,000 persons in girls aged 1–7. In children aged 7–12 years, the corresponding incidences were 12.7 and 4.8 per 100,000 persons, respectively. 3
The treatment of femoral fractures is determined by the patient’s age, weight, fracture type, and social and individual circumstances.4 –6 During the past decades, the operative treatment of femoral diaphyseal fractures with elastic stable intramedullary nailing (ESIN) has shown an increasing trend. Previously, preschool-aged children were mostly treated with traction and hip spica cast, but operative treatment with ESIN has also been increasing in this age group. As it is based on semirigid fixation, the ESIN technique provides the best possible outcome for patients who are younger than 12 years and weigh less than 50 kg. Moreover, the ESIN technique is minimally invasive and offers early knee joint mobilization to maintain muscle tone and reduce joint stiffness. Another benefit of ESIN is that the hospitalization period is relatively short, allowing early psychological recovery and a rapid return to school and ordinary family life.7 –10
Gordon et al. 11 recently stated that there is a paucity of prospective published data available regarding the optimal treatment (early hip spica cast versus ESIN) of 2- to 6-year-old children with femoral shaft fracture. Based on American Academy of Orthopaedic Surgery (AAOS) guidelines, the early hip spica casting or traction with delayed casting is recommended for children aged 6 months to 5 years.6,11
The main aim of this study was to evaluate the changing trends in the treatment of pediatric femoral shaft fractures with hip spica casting and ESIN in Finnish children aged 2–12 years between 1998 and 2016. We also aimed to determine the true costs of hospital treatment during the study period by assuming that the trend toward increased operative treatment with ESIN would shorten the length of hospital stay and thereby lessen the cost of treatment.
According to Finnish research legislation and the Finnish National Board on Research Integrity appointed by the Ministry of Education and Culture, a review by a formal ethics committee is not required for research involving public and published data, registry and documentary data, and archive data.
Materials and methods
This study included the entire Finnish pediatric population aged 2–12 years who were diagnosed with a primary or secondary femoral diaphyseal fracture between 1 January 1998 and 31 December 2016. Femoral fracture data were obtained from the National Hospital Discharge Register of Finland (FNHDR). The register includes all hospitalized children, and diagnoses are coded according to the International Classification of Diseases (ICD-10 since 1997). In this study, the main outcome variables were the number of individual patients hospitalized with a primary or secondary diagnosis of femoral shaft fracture (ICD-10 code S72.3) and a primary femoral fracture procedure related to casting (NFJ40 closed reduction of fracture of femur and bandage, NFJ42 open reduction of fracture of femur and bandage) or intramedullary nailing (NFJ60 internal fixation of fracture of femur with intramedullary nail or NFJ64 internal fixation of fracture with nailing). Children with a femoral shaft fracture treated with other procedures, such as plating, were excluded from this study. The actual annual daily hospital costs data concerning the treatment of femoral diaphyseal fractures were collected from the Finnish Institute for Health and Welfare. 12
Statistical analyses were performed similarly to our previous trauma register–based study in femoral childhood fractures. 3 To calculate the incidence rates of femoral diaphyseal fractures, the annual mid-year population of Finland was obtained from Statistics Finland, which serves as an electronic national population register. 13 The annual incidences per 100,000 persons were calculated using annual mid-year population census data obtained from Statistics Finland. All analyses were performed using R version 4.0.5 (R Foundation for Statistical Computing, Vienna, Austria). As the incidence figures were the true results of the entire adolescent population in Finland rather than cohort-based estimates with sampling variability, 95% confidence intervals were not calculated. 3
Results
During the 18-year study period, a total of 1064 children aged 2–12 years, 786 boys (73.9%) and 278 girls (26.1%), with a femoral fracture treated with ESIN or hip spica casting were included (Figure 1). The total incidence of femoral diaphyseal fractures was 12.1 per 100,000 persons in boys and 4.5 per 100,000 persons in girls. Of the 1064 diaphyseal fractures, 249 (23.4%) were treated with hip spica casting and 815 (76.6%) with ESIN. The total incidence of children treated with ESIN decreased from 6.9 to 5.9 per 100,000 persons (from 10.0 to 9.1 in boys and from 3.8 to 2.5 in girls) during the study period (1998–2016) (Figure 2). The incidence of children treated with hip spica cast also decreased during the study period from 4.0 to 1.8 per 100,000 persons (from 5.6 to 2.9 in boys and from 2.3 to 0.6 in girls).
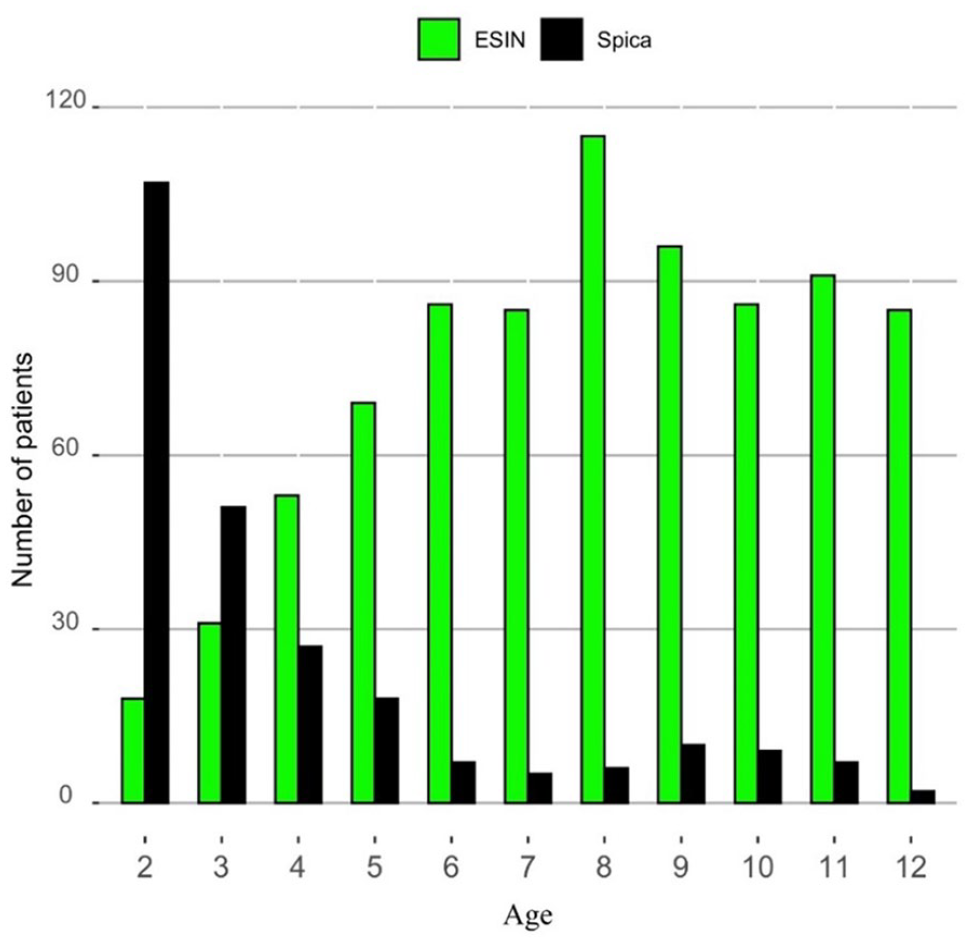
Number of children treated with ESIN or hip spica casting between 1998 and 2016.
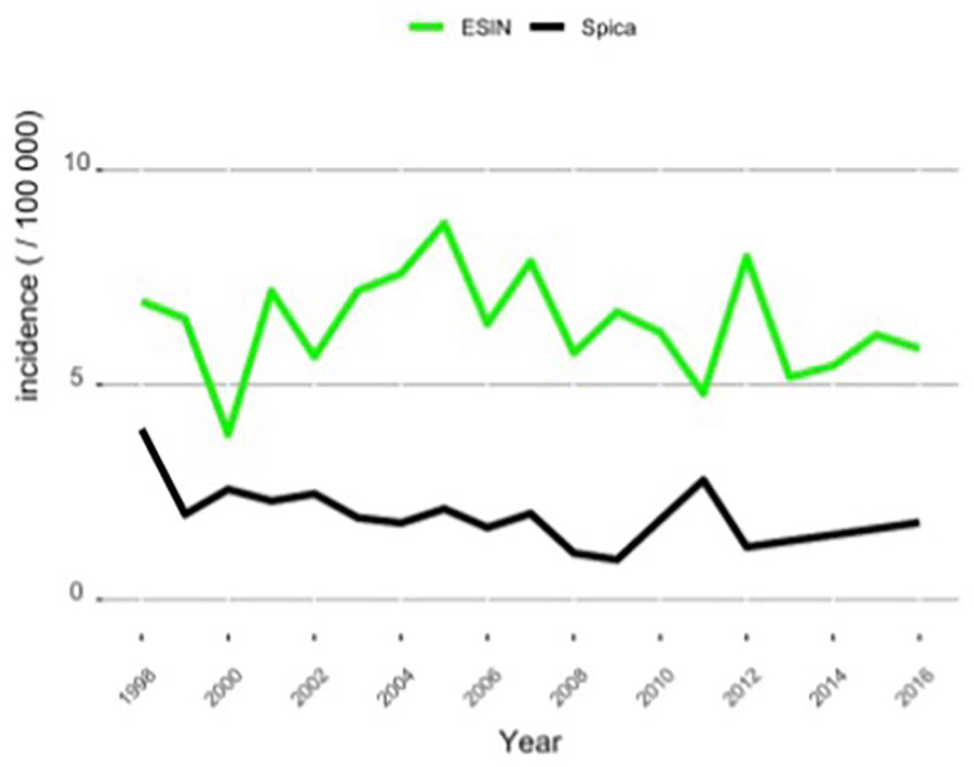
Incidence of femoral shaft fractures treated with ESIN or hip spica casting.
In the youngest age group (2–3 years), most children were treated with hip spica casting (Figure 3). There were no significant changes in the treatment method chosen for the children in this age group during the study period. In this age group, the incidence of spica casting was 7.0 per 100,000 persons and 2.2 per 100,000 persons for ESIN.
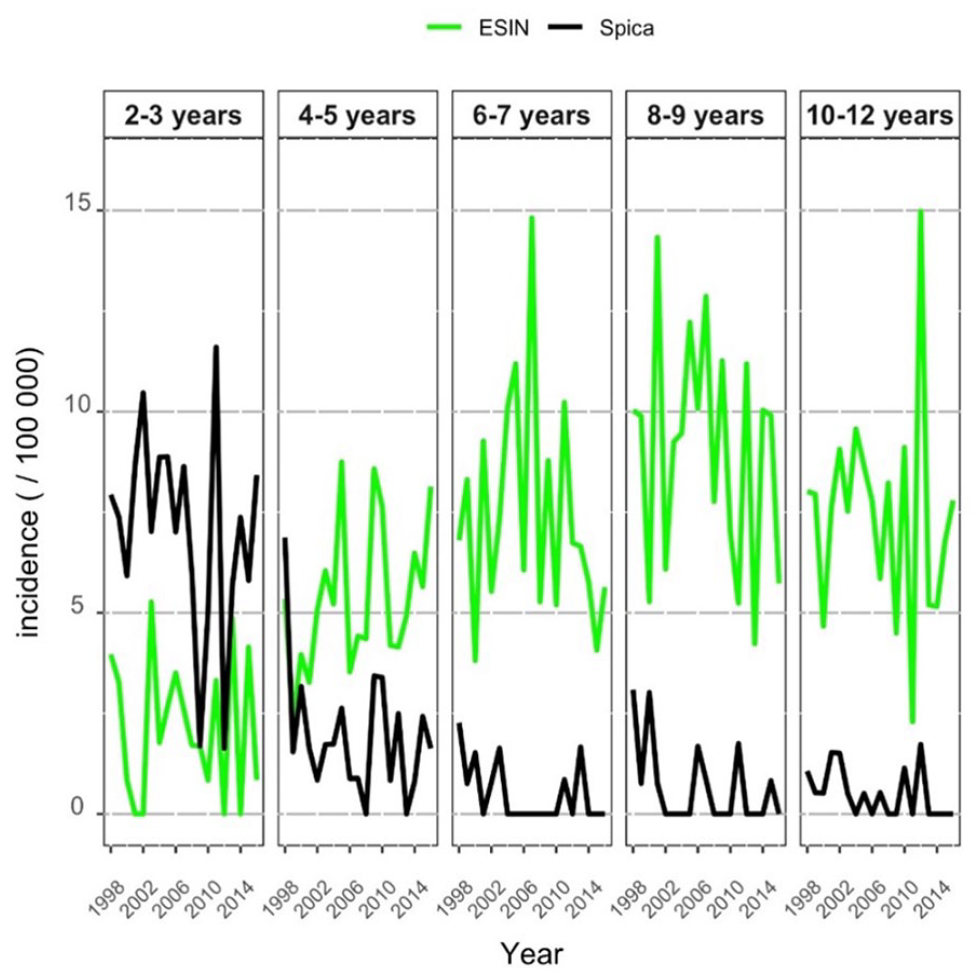
Incidence of femoral fractures treated with ESIN or hip spica casting in different age groups.
In patients aged 4–5 years, the incidence of ESIN increased during the study period from 5.4 in 1998 to 8.1 per 100,000 persons in 2016. The incidence of hip spica casting decreased, however, from 6.9 in 1998 to 1.6 per 100,000 persons in 2016. In patients older than 6 years, the incidence of ESIN was higher than that of spica casting. In patients aged 6–7 years, the incidence of ESIN was 7.4 and spica casting 0.5 per 100,000 persons. Accordingly, in the 8–9 years age group, the incidence of ESIN was 9.1 and hip spica casting 0.7 per 100,000 persons. In the 10–12 years age group, the incidence of ESIN was 7.4 and spica casting was 0.5 per 100,000 persons. The incidence of ESIN remained unchanged in those age groups older than 6 years (Figure 3).
For children treated with hip spica cast, the mean length of hospitalization was 9.4 days. For those children treated with ESIN, the hospitalization period was 6.3 days. During the study period, the length of hospital stay decreased in both treatment groups. In children treated with hip spica cast, hospital stay decreased from 13.5 to 6.1 days and in children treated with ESIN from 7.3 to 3.3 days.
Data on the annual actual daily hospital costs for the treatment of pediatric femoral diaphyseal fractures were available from 2002 onward and were collected from the Finnish Institute for Health and Welfare. 12 The actual daily cost of the hospitalization varied annually. In children treated with hip spica cast, the price per hospital day ranged from 793€ (2002) to 1286€ (2016), whereas in children treated with ESIN, the price ranged from 1006€ (2002) to 1920€ (2016). During the study period, the average cost of treatment fell. In 2002, for example, the average cost of hospital treatment for children treated with ESIN was 6757€. In 2016, the average cost was 6302€. In children treated with hip spica cast, the average cost of treatment was 8914€ in 2002 and 7825€ in 2016. The price per hospital day was more expensive in children treated with ESIN, but the length of hospital stay was shorter in both treatment groups.
Discussion
The aim of this study was to define the changing trends in the treatment of diaphyseal femoral fractures in Finnish children aged 2–12 years during the past decades. We aimed to study the impact of the treatment method chosen (ESIN versus hip spica casting) on the hospitalization and the actual daily costs of hospital care. Previous studies have stated simultaneous decreasing incidence of pediatric femoral fractures and increasing incidence of operative treatment in children aged 5–9 years.10,14,15
The primary finding of this study was that the incidence of femoral fractures treated with ESIN in children aged 4–5 years has increased. Furthermore, the hospitalization period decreased for children treated with ESIN and spica casting during the study period. Overall, the hospitalization period was shorter in those children treated with ESIN, and the total cost of the hospitalization was also lower in children treated with ESIN.
Diaphyseal femoral fractures in children significantly affect the everyday life of their families as fracture treatment requires hospitalization and often surgical treatment in the operating room. A long hospitalization period is costly for society and a burden on families. Moreover, after discharge from hospital, home care is often needed, especially in children treated with hip spica cast.2,4,6 Both a long hospitalization period and home care necessitate parents or caregivers to be away from work, which may result in financial problems for the family.
Traditionally, children younger than 5 years who sustain diaphyseal femoral fractures have been treated with hip spica casting. However, a hip spica cast with or without traction causes a burden of care on the children and their families that results from the length of hospital stay and possible complications related to casting, such as loss of reduction, skin problems, and soiled casts, in addition to problems with the transport and transfer of a child wearing a cast.14,16,17 In the present study, the hospitalization decreased in both the ESIN and hip spica casting groups. At the beginning of the study, children treated with ESIN were hospitalized for 7 days. By the end of the study period in 2016, however, the hospitalization period had fallen to 3 days. Correspondingly, patients with hip spica cast were hospitalized initially for 13 days, but this had fallen to 6 days by the end of the study period.
The economic factors concerning parents or caregivers are also related to the treatment of femoral shaft fractures in children, as they often have to miss work to take care of the injured child both during the hospital stay and at home. The need for hospital stay varies according to the treatment method chosen. In this study, we noted that the daily cost of treatment was higher in patients treated with ESIN. However, as the hospitalization period needed after ESIN was shorter, the average cost of treatment was cheaper than in those children treated with hip spica cast.
The trend to treat younger, preschool-aged children with ESIN may decrease the burden of trauma on the injured children and their caregivers. The length of home care needed is also predicted to be shorter than in children treated with hip spica cast. Therefore, the trend to treat younger, preschool-aged patients with ESIN allows earlier mobilization, shortens the length of hospital stay, and reduces the cost of hospitalization.
However, operating on young children using the ESIN technique is challenging, as inserting the nail may be more difficult than in older patients. Complications related to ESIN can include scarring, superficial or deep wound infections, problems with protruding nail endings, and loosening correction of the fracture.11,18 Finally, the removal of the fixation materials in young children entails another visit to the operation room under general anesthesia and raises the total cost of treatment in patients treated with ESIN.
The strength of this study is the data collected from the FNHDR that provide an excellent database of patients treated in hospital.19,20 The most obvious weakness of this study was the poor or absent recording of the external causes of the fractures and other missing or incorrectly recorded events. Trauma register–based data used did not include the fixation material removal codes (NFU20), thus we could not include this information on our study.
Conclusion
To summarize, although the total incidence of children treated with ESIN for femoral diaphyseal fractures in Finnish children aged 2–12 years decreased slightly during our study period, the incidence of children treated with ESIN in the preschool age group of children aged 4–5 years has increased. The daily hospital costs were greater for children treated with ESIN, but the length of hospital stay was shorter. Therefore, the total cost of primary hospital treatment was lower in those children treated with ESIN than in those treated with hip spica cast.
Supplemental Material
sj-pdf-1-cho-10.1177_18632521231217267 – Supplemental material for The incidence, trends, and costs of treatment of femoral shaft fractures among Finnish children aged 2–12 years between 1998 and 2016
Supplemental material, sj-pdf-1-cho-10.1177_18632521231217267 for The incidence, trends, and costs of treatment of femoral shaft fractures among Finnish children aged 2–12 years between 1998 and 2016 by Elina Laitakari, Topias Koukkula, Tuomas T Huttunen, Ville M Mattila and Anne Salonen in Journal of Children’s Orthopaedics
Footnotes
Author contributions
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
All data were stored in accordance with the General Data Protection Regulation (GDPR). The regional ethical committee approved the study (Reference Nos. 2013/581-31/5 and 2016-2251-32, 2018/1823-32, 2020-04776, and 2020/06182) which was performed in line with the ethical standards of the 1964 Declaration of Helsinki and its later amendments.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.