
Abstract
Knee periarticular and intra-articular fractures in children and adolescents have specific features and should be carefully detected. Typical non-contact and contact mechanisms that may lead to an anterior cruciate ligament injury in a skeletally immature patient can cause a tibial eminence fracture. During patellar dislocation or other traumatic events, pure chondral fractures can occur and should be excluded. During sports, traumatic events leading to a forceful quadriceps contraction can cause specific paediatric fracture patterns such as patella sleeve and tibial apophyseal fractures. This review will highlight controversies and innovative aspects of non-operative and operative treatment, basic science, new evidence and unanswered questions for these fractures.
Background
Children’s sport activities are increasing and consequently paediatric knee injuries and fractures.1,2 Paediatric knee periarticular and intra-articular fractures have specific features and should be carefully detected. A typical non-contact and contact sprain that may lead to an anterior cruciate ligament (ACL) injury in a skeletally immature patient can cause a tibial eminence fracture (TEF) in a skeletally immature patient.3,4 In children under the age of 9 also, specific cartilaginous TEF should be considered as a potential fracture pattern, and in selected cases, a magnetic resonance imaging (MRI) is recommended.5,6
Developments in imaging techniques and knowledge, 7 new arthroscopic devices, methods of fixation and a growing awareness about specific fracture patterns lead to a more defined treatment in paediatric fractures around the knee.8 –10
This review will highlight developments over the last few years about four particular fractures in skeletally immature patients: TEF, patella sleeve fracture, tibial apophyseal fracture, and pure chondral fractures.
Innovative aspects in non-operative and operative treatment, basic science, new evidences and unanswered question were reached and stressed for all these fractures.
Tibial eminence factures
Due to tibial spine bony immaturity in children, TEF is more likely to occur than ACL, with peak incidence between 13–14 years for males and 11–12 years for girls. It is always a serious injury of the knee joint and management remains challenging. Meyers and McKeever (MMK) classification system based on the degree of fragment displacement help in TEF management (Figure 1). 11 For TEF type I MMK, non-operative management produces good result, but distinguishing between type I and type II MMK is sometimes challenging on plain X-rays (Figure 2). In case of conservative treatment, MRI should always be performed to confirm classification diagnosis and exclude associated intra-articular lesions, especially meniscal tears, meniscal or inter-meniscal ligament entrapment and osteochondral lesion that have been reported in up to 31.9% of cases. 12 Treatment for type II MMK TEF remains controversial. Comparison between conservative and surgical treatment of type II MMK TEF seems to show a higher rate of residual laxity and subsequent tibial spine or ACL surgeries, when treated conservatively. In the surgical group, higher rate of post-operative arthrofibrosis was reported. 13 This controversy should be the subject of research to standardize the management of type II MMK TEFs.
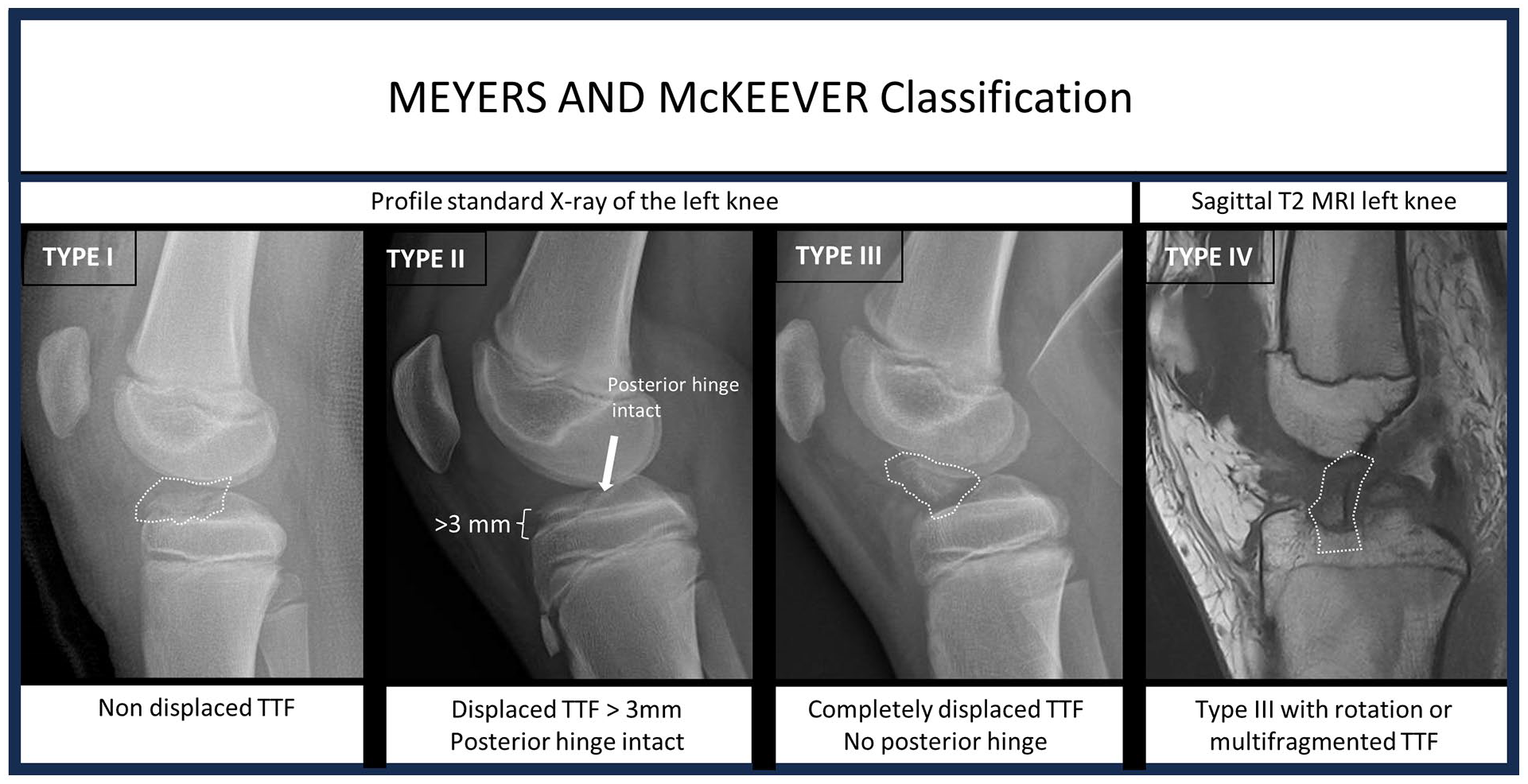
Meyers and Mckeever classification system grades tibial spine fractures as type I (non-displaced, <3 mm), type II (hinged, >3 mm), type III (completely displaced without rotation of the fragment) and type IV (completely displaced with rotation).

(a) Profile standard X-ray of a tibial eminence fracture in the cast, (b) sagittal cross section T2 MRI. (c) Arthroscopic view of a tibial eminence fracture. 1 indicates medial meniscus, 2 indicates medial femoral condyle, 4 indicates fracture line through the medial tibial plateau.
Standard knee X-rays clearly identify grade III and IV MMK TEFs. For those cases, surgical indication is clear and require anatomical reduction and fixation of the fracture. Direct open reduction by parapatellar mini-arthrotomy or arthroscopy are suitable options for reduction and repair. 14 There are many types of fixations described with K-wires, anchors, screws and sutures, bio-absorbable or not. All fixation types have offered satisfactory results, and the best technique is yet to be determined. 15 Currently, there is insufficient scientific evidence comparing open and arthroscopic fixation. There is no clear advantage of one method of fixation over another: the standard of care remains based on the surgeon’s skills and preference.12,16 Preoperative MRI is recommend to detect concomitant injuries, especially in patients treated without arthroscopic evaluation. 17 Neglecting associated lesions can lead to poor results.
A recent meta-analysis of 1922 TEF described the main complications. Non-union has been reported as uncommon and occurs mainly with conservative treatment of type III lesions which is an incorrect treatment. Arthrofibrosis (11.2%) and post-treatment residual laxity (10.1%) occur more often. 12 Reducing those complications should be a priority. Bram et al. identified four significant predictive factors of arthrofibrosis: concomitant ACL injury and severe traumatic injury not resulting from athletics, age less than 10 years and cast immobilization. 18 The fourth factor being potentially influential, standardizing the rehabilitation protocol after TEF (type and duration of immobilization, physiotherapy) will probably help reduce arthrofibrosis.
Mitchell reported in his cohort 19% of patients with delayed ACL reconstruction after treatment for TEF during a mean follow-up of 6.9 years, especially for type II MMK TEF. 19 This was supported by the Tibial Spine Research Interest Group. 12 Several groups have raised the hypothetical possibility of a partial ACL lesion occurring during TEF, which would compromise the biomechanical properties and proprioceptive function of the ACL. Functional recovery after treatment, assessed by standardized functional tests, is a prerequisite for a return to pivot sports. It has never been studied after TEF treatment in children, but seems to be an essential step, as already confirmed in ACL reconstruction. Establishing tests and standards for recovery after TEF treatment is one of the challenges we face when trying to reduce the number of complications or reinjuries.
In summary, MRI should be performed to rule out any TEF-associated lesion, particularly in non-operative management and in patients treated non-arthroscopically.
The best fixation method is yet to be determined.
Arthrofibrosis and residual laxity are the most common complications that should be reduced as a priority.
Consensual post-operative regime and duration of immobilization, physiotherapy protocol and functional evaluation remains highly diversified and habit-based, which could be improved to reduce TEF complications.
Patella sleeve fractures
Although rare occurrences, patella sleeve injuries may be increasing in incidence as the paediatric population increases in body weight and size with more involvement in organized sports from a younger age. Occurring more commonly around the age of 10 years and in male patients, the rapid quadriceps contraction that is seen in contact sport is often the mechanism seen with these injuries. Controversies in treatment are significant, based on the lack of any prospective studies with case series from large centres and over long follow-up. 20 Areas that require further clarification include the role of imaging, who can be treated non-operatively and the best method of surgical management.
The clinical features often described are the presence of a knee effusion, a high (or low) lying patella, palpable gap and absence of straight leg raising. None of these features are specific or sensitive. The role of radiographs in diagnosis is well established, but in the absence of an osseous fragment can only be diagnosed with indirect measures such as hemarthrosis and altered patella height. MRI gives good understanding of the nature of the injury and degree of displacement (Figure 3). This may not be available acutely but is helpful in differentiating cases for operative management, and in the differentiation of a sleeve fracture from Sinding–Larsen–Johansson syndrome. The use of ultrasound has not been well described.

MRI example of an inferior patella sleeve injury (T2 sagittal).
There are still no evidence-based criteria for deciding on which injuries need surgery and the ideal mode of non-operative management. The evidence from case series suggests non-operative management works well, but often these are the cases with minimal displacement and therefore not comparable. Most treat these injuries in a knee brace, allow weight bearing as tolerated with a gradual increase in range of movement over a 6-week period. MRI may be useful in preventing later surgery for missed chondral lesions. However, the incidence of chondral lesions in patellar sleeve fractures was never defined.
The technique of tension band wiring with metal cerclage nearly always requires removal of hardware due to irritation. Advances in technology have led some to use a non-absorbable tape as an alternative but again, the knots can irritate. There are no comparisons of methods of fixing these injuries in the contemporary literature, although a multitude of techniques exist.21,22 As the technology of suture anchors improves, this remains an alternative that may reduce the need for second surgery. 23 Until proven, a tension band construct remains the tried and tested technique as in the management of other patella fractures. The delayed presentation of a displaced sleeve also remains an area with little data to guide us. The best mode of treatment for these remains elusive.
Sleeve fracture management would benefit from prospective, multicentre research to answer specific questions, such as the identification of cases for non-operative management, the method of non-operative management, fixation techniques and the role of imaging. 24
Rapid quadriceps contraction during contact sport is the typical mechanism that causes patellar sleeve fractures.
A new classification system based on specific criteria such as fracture displacements, may help in the identification of the best management of paterllar sleeeve fractures.
There is no clear advantage of one surgical treatment over another: the standard of care remains based on the surgeon’s preference. However, more research is recommended.
Tibial tuberosity fractures
Fractures of the proximal tibial apophysis are uncommon, comprising not more than 3% of all proximal tibial fractures. However, due to increased participation in organized sports, the incidence of these rare fractures has increased during the recent years, similarly to many other paediatric long bone fractures.25,26 The fractures usually occur in children aged 12–14, and more often among males. Osgood–Schlatter disease may be a potential predisposing factor, but the causative association is still unclear.27,28 Trauma mechanism includes forceful eccentric quadriceps muscle contraction and it usually happens in sports, particularly in ball games such as soccer, basketball and volleyball. 29
When diagnosing tibial tuberosity fracture with using conventional anterior–posterior and lateral radiographs, potential associated injuries need to be investigated, preferable by using MRI.25,30 Further, standard or Cone-beam computed tomography are sensitive but accurate in evaluating the extension of the fracture line up to the proximal tibia epiphyses or joint surface. Although the majority of the cases may be uncomplicated, there is a risk of meniscal injury, ACL injury, or even compartment syndrome.
Treatment of tibial tuberosity fracture aims to ensure the extensor function of the knee, restore the knee joint anatomy and keep meniscus intact. Hairline fractures or those with minimal (<2 mm) displacement can be treated with immobilization for 4–6 weeks, with limited weight bearing. Surgical fixation is the most usual treatment, and it is indicated for displaced fractures (Figure 4). Fixation is preferably performed by using two cannulated screws. Screw fixation of the tibial apophysis is rather free of complications, except from hardware irritation and anterior knee pain post-operatively. Due to transphyseal screw fixation, tibial apophysis may fuse. Nevertheless, that is mostly harmless, while tibial apophyses doesn’t contribute to either longitudinal growth of the tibiae or the shape of the knee joint surface, theoretically, surgical fixation and the injury per se can result in recurvatum, which is found in less than 4% of the cases.31,32
Osgood–Schlatter disease may be a potential risk factor but specific studies are recommended.
Incidence of associated injuries should be defined; however, MRI is the best method to investigate them.
Transphyseal screw fixation is the most described surgical treatment method.
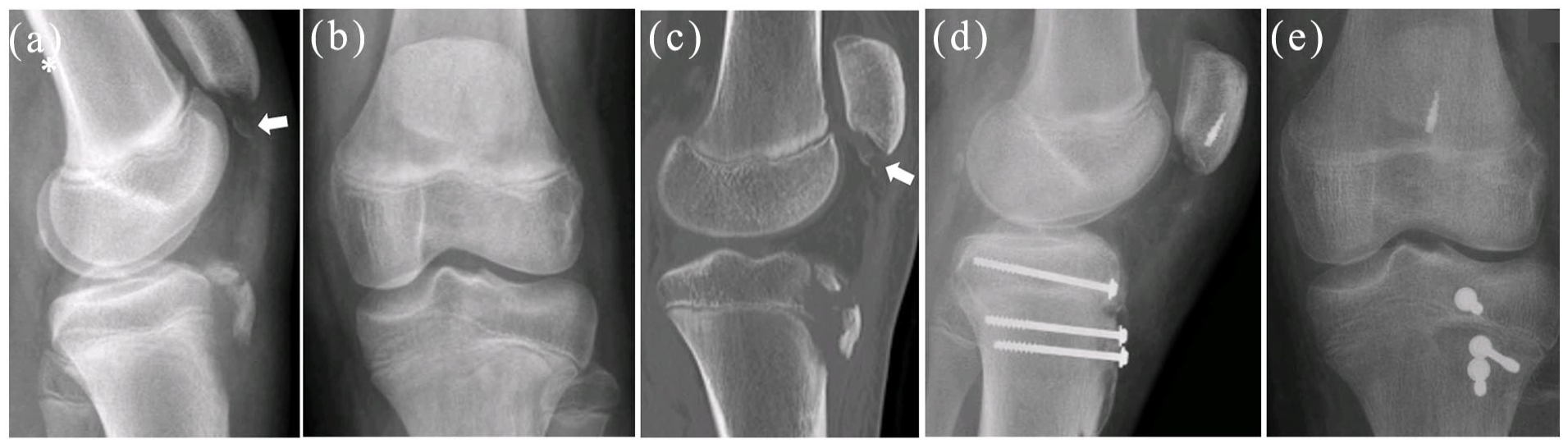
Thirteen years old boy with a tibial tuberosity aphophyseal fracture with an associated distal patellar fracture. (a and b) Show preoperative X-rays, (c) show a sagittal cross section of preoperative CT scan, (d and e) show post-operative X-rays. White arrows indicate distal patellar fracture.
Pure chondral knee fractures
Traumatic cartilage injuries of the knee are mainly consequences of high-energy shear at the level of the lateral compartment of patella-femoral joint. Patellar dislocation is the most frequent event. 33 Pure articular chondral knee fractures differ from osteochondral defects due to the absence of bone layer on the deep side of the fragment. Second, they are considerably less frequent. 34 Even if pure chondral fractures are infrequent, their clinical consequences especially in a young patient are relevant.35,36 Pure chondral fragments were historically thought to have very limited healing potential. 37 Recently several study reports demonstrated promising results after surgical chondral fragment fixation, especially in paediatric population.38 –40 The most appropriate method of restoring joint surface appears to be reinsertion of the native hyaline cartilage fragment (Figure 5), if per operative conditions are appropriate. 41
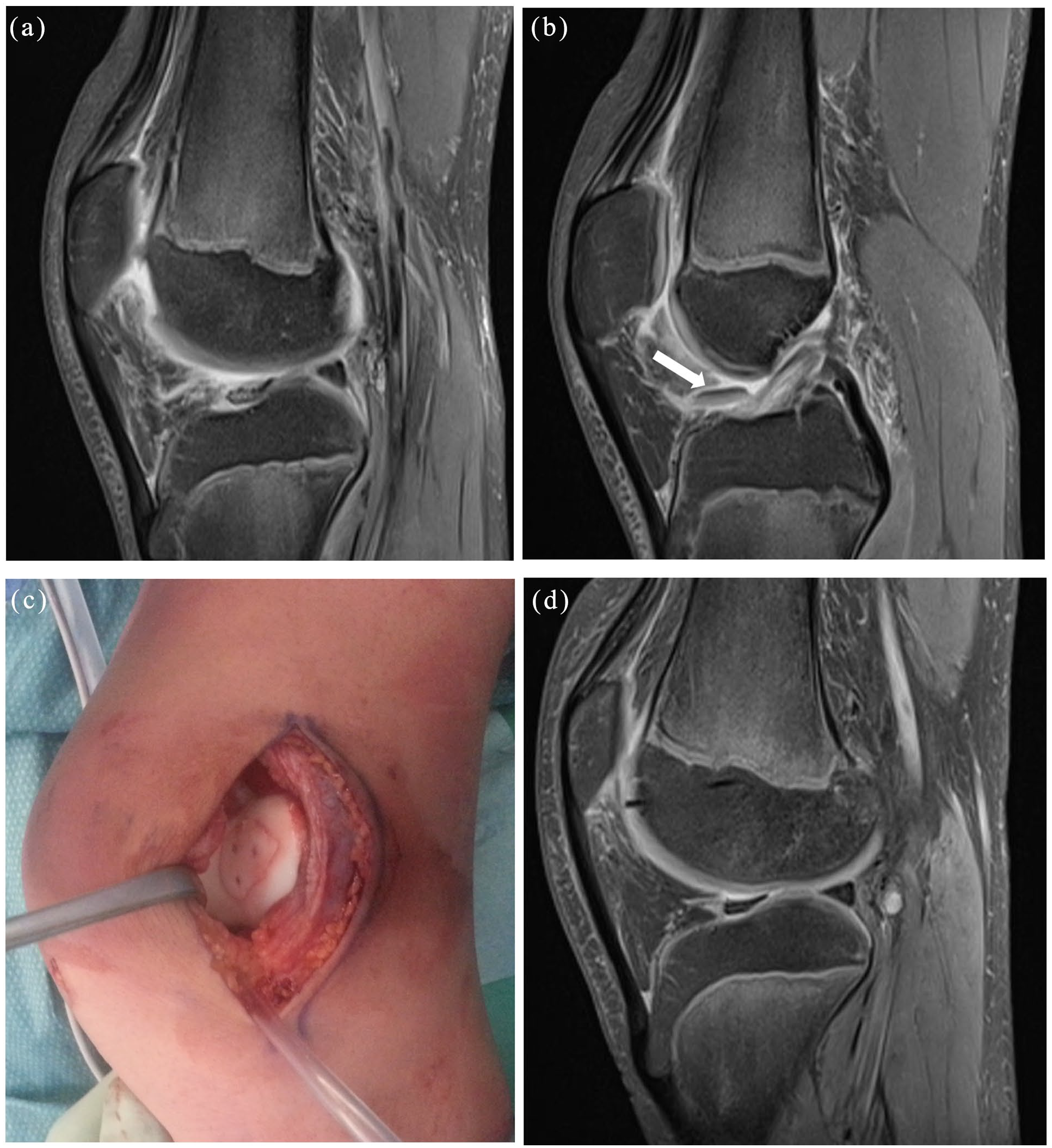
Twelve-year-old boy with a patellar pure chondral fracture associated with a patellar dislocation occurred in a traumatic ski accident. (a and b) Show preoperative T2 sagittal MRI (white arrow indicate the pure chondral fracture in the sagittal MRI), (c) shows intraoperative image after fragment fixation, (d) shows good chondral healing in a T2 sagittal MRI at 12 months of follow-up.
Timing plays a key role in the process to a successful treatment.
First, a timely/rapid diagnosis is crucial to treat acutely chondral lesions. X-rays and MRI are recommended after a traumatic event or at the onset of acute knee pain, especially when correlated with patella instability or dislocation. The use of knee MR-arthrography is still debated.
If surgical fixation of the chondral fragment during the first 2 months after a traumatic event is supported by the recent literature, it is still not clear which is the best treatment option in case of late presentation.41,42 One study described encouraging results with patellar chondral fracture fixation after 2 months, but further data are needed to confirm that it is reasonable to also attempt late fixation of the fragment. 43
Different devices are used according to the literature (screws, pins, darts). Screws provide greater compression but require a larger chondral chip to avoid further fragmentation. Pins or darts are suggested for smaller lesions (<1.5 cm). Absorbable devices are demonstrated to be reliable, and don’t require removal surgery.44,45 It still unclear which option is recommended for each case. Moreover, in case of patellar dislocation or instability as cause of chondral lesion, it is still not clear whether a concomitant medial patellofemoral ligament reconstruction is recommended at primary surgery.
Regenerative surgery produced promising results. Autologous cartilage implantation technique demonstrated to have equal or superior outcomes compared to mosaicplasty. 46 Autologous cartilage implantation is a safe procedure, but complications like failure of the graft or hypertrophic healing are described and often require secondary surgery. 47
Often caused by high-energy trauma like patellar dislocation.
Surgical fixation is a promising treatment but more specific research needed.
Early surgical fixation within 2 months is crucial; absorbable devices preferred.
Supplemental Material
sj-pdf-1-cho-10.1177_18632521251327129 – Supplemental material for Paediatric knee fractures: A current concept review
Supplemental material, sj-pdf-1-cho-10.1177_18632521251327129 for Paediatric knee fractures: A current concept review by Marco Turati, Franck Accadbled, Stéphane Tercier, Monika Thüsing, Luca Rigamonti, Jaakko Sinikumpu, Benjamin Tschopp and Nicolas Nicolaou in Journal of Children’s Orthopaedics
Footnotes
Author contributions
Design of the study: Franck Accadbled, Stéphane Tercier, Marco Turati, Monika Thüsing, Jaakko Sinikumpu.
Data collection: Benjamin.Tschopp, Luca Rigamonti, Nicolas Nicolaou, Franck Accadbled, Stéphane Tercier, Marco Turati.
Data analysis and interpretation: Marco Turati, Jaakko Sinikumpu, Benjamin.Tschopp, Luca Rigamonti, Nicolas Nicolaou, Franck Accadbled.
Drafting of the manuscript: Nicolas Nicolaou, Franck Accadbled, Luca Rigamonti, Benjamin.Tschopp, Stéphane Tercier, Marco Turati, Monika Thüsing.
Manuscript final revision: Jaakko Sinikumpu, Nicolas Nicolaou, Benjamin.Tschopp, Marco Turati, Monika Thüsing, Stéphane Tercier.
All authors approved the final version of manuscript for submission.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.
Ethical approval
Not applicable.
Submission declaration
This manuscript has not been published previously and is not under consideration for publication elsewhere. The publication of this article has been approved by all authors and by the responsible authorities where the work was carried out. We declare that, if accepted, this manuscript will not be published elsewhere, including electronically in the same form, in English or in any other language, without the written consent of the copyright-holder.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.