
Abstract
Objective
Subcutaneous fat tissue thickness (SFTT) is a representative marker of obesity. This study was performed to determine the relationship between SFTT and chondromalacia patella (CP) through routine 1.5-Tesla magnetic resonance imaging (MRI) of the knee.
Methods
In this retrospective cross-sectional study, 440 knee MRI scans were re-examined and divided into those with and without CP. A 1.5-Tesla MRI machine with a standard knee coil was used. Prepatellar SFTT (PSFTT) and medial SFTT (MSFTT) were measured on each MRI scan. PSFTT and MSFTT were compared between patients with and without CP.
Results
Both the PSFTT and MSFTT values were significantly higher in patients with than without CP. Women had significantly higher PSFTT and MSFTT values than men. A statistically significant correlation was found between the PSFTT and MSFTT values and the CP grades.
Conclusions
The results of this study indicate an association between SFTT and CP. A positive correlation was also found between SFTT and CP severity.
Keywords
Introduction
Chondromalacia patella (CP) is a clinical condition characterized by hyaline cartilage degeneration of the patella. It ranges in severity from a small fissure to total loss of the subchondral cartilage, which may cause anterior knee pain. CP can be encountered in both young adults and older individuals. 1 Factors that play a role in the development of CP include knee trauma, morphological abnormalities that increase the mechanical stress on the articular cartilage, and vascular insufficiency of the subchondral bone. 2 Obesity is another factor associated with patellar cartilage damage.3–5 Some authors have described a relationship between obesity and CP, 6 and some have presented a relationship between CP and the body mass index with a stronger correlation in women than in men. 7 Subcutaneous fat is widely used as a surrogate marker of obesity.8,9 Although arthroscopy is the gold standard for diagnosing CP, it is an invasive procedure, and surgical treatment of CP is indicated in only 5% to 10% of patients.2,10,11 By contrast, magnetic resonance imaging (MRI) is a noninvasive diagnostic method that provides excellent visualization of soft tissues. With its potential for multiplanar imaging, MRI is a reliable diagnostic tool that can detect morphological alterations and cartilage deformations.
This study was performed to reveal the relationship between subcutaneous fat tissue thickness (SFTT) and CP, which has been investigated in only a few studies to date. To the best of our knowledge, this is the largest patient series in which this relationship has been investigated using both the medial and prepatellar approaches to measuring SFTT.
Methods
Patients
In this retrospective cross-sectional study, we analyzed MRI scans to reveal the relationship between SFTT and CP. The reporting of this study conforms to the STROBE guidelines. 12 All patient details are deidentified in this article to preserve patient data privacy. The institutional ethics committee approved the study and waived the requirement for informed consent because of the methodology of the investigation. After ethics committee approval, all patients who had undergone a knee MRI examination from 1 January to 31 March 2022 were re-evaluated.
The inclusion criteria were (1) readily available knee MRI scans in our hospital’s medical records from 1 January to 31 March 2022, (2) age ranging from ≥18 years (to ensure skeletal maturity) to <65 years (to avoid the effect of high-grade osteoarthritis on CP), and (3) complete knee MRI examination data with no missing MRI sequences. The exclusion criteria were (1) a history of knee trauma (to avoid the effect of traumatic impaction on CP), (2) a history of a knee operation, (3) patellar location anomalies (e.g., transient patellar dislocation, patella alta, or patella baja) as a potential cause of CP, (4) moderate to severe osteoarthritis (compatible with Kellgren–Lawrence types 3 and 4) to avoid the effect of degenerative arthritis on CP, and (5) unusable knee MRI scans (e.g., incomplete knee examinations, knee MRI scans with motion artifacts).
In total, MRI scans of 503 patients’ knees were identified in our hospital’s picture archiving and communication system (PACS). Patients with a history of trauma (n = 61), a history of any knee operation (n = 23), transient patellar dislocation (n = 11), patella alta (n = 1), and moderate and severe osteoarthritis (n = 4) were excluded from the study because these conditions might affect the results. Seventeen patients with motion artifacts on MRI scans that might cause false interpretations were also excluded from the investigation. Therefore, 440 knee MRI scans of 386 patients (54 with bilateral knee MRI examinations) were included.
The CP group comprised patients who had signal alterations consistent with CP in their knee MRI scans, and the control group comprised patients without CP.
MRI
All MRI examinations were performed using a 1.5-Tesla MRI machine (MAGNETOM Aera; Siemens Healthineers, Erlangen, Germany) with standard (15-channel) knee coils. Turbo spin-echo images with different sequences were obtained. The parameters used in each imaging series were as follows: sagittal-plane T1-weighted imaging (time of repetition [TR], 1110 ms; time of echo [TE], 9.7 ms; number of excitations [NEX], 1; field of view [FOV], 180 mm; slice thickness [ST], 3 mm; voxel size [VS], 0.5 × 0.5 × 3 mm), axial-plane proton density-weighted fat-saturated imaging (TR, 3440 ms; TE, 30 ms; NEX, 2; FOV, 180 mm; ST, 3 mm; VS, 0.6 × 0.6 × 3 mm), coronal-plane fat-saturated proton density imaging (TR, 2390 ms; TE, 20 ms; NEX, 2; FOV, 200 mm; ST, 4 mm; VS, 0.6 × 0.6 × 4 mm), and sagittal-plane fat-saturated proton density imaging (TR, 3060 ms; TE, 38 ms; NEX, 1; FOV, 180 mm; ST, 3 mm; VS, 0.7 × 0.7 × 3 mm).
Interpretation and measurements
All MRI scans were reviewed in consensus by two radiologists with 17 and 20 years of experience, respectively. A PACS system (Akgun PACS Viewer v7.5; Akgun Software, Ankara, Turkey) was used to analyze the cross-sectional images in standard Digital Imaging and Communications in Medicine (DICOM) format.
The prepatellar SFTT (PSFTT) was measured using mid-sagittal T1-weighted images from the mid-level of the patella, similar to the technique used in a previous study. 13 The medial SFTT (MSFTT) was measured using axial T2-weighted images. Using a modification of the method reported by Kok et al., 14 the measurements were performed at the cross-sectional level at which the maximum patellar cartilage was monitored on the image. In this cross-sectional image, the maximum SFTT was measured near the posterior aspect of the medial femoral condyle (Figure 1). A modified Noyes classification was used to classify the cartilage damage in patients with CP, similar to previous studies.10,11 According to this classification, grade 0 represented normal cartilage with homogenous signal intensity with an intact surface and thickness, grade 1 represented a normal cartilage surface but with focal abnormal signal intensity, grade 2 represented a cartilage defect of <50% thickness (2A) or a cartilage defect of >50% thickness but less than full thickness (2B), and grade 3 represented a full cartilage thickness defect with exposed bone (Figure 2).

(a) The prepatellar subcutaneous fat tissue thickness was measured on the mid-sagittal T1-weighted images and (b) The medial subcutaneous fat tissue thickness was measured on axial T2-weighted images at the level at which the maximum patellar cartilage was observed in the image.

Chondromalacia patella was classified using a modified Noyes classification as follows. Normal patellar cartilage, grade 0; (a) focal abnormal signal intensity, grade 1; cartilage defect of <50% thickness, grade 2A; (c) cartilage defect of >50% thickness but less than full thickness, grade 2B and (d) full cartilage thickness defect with exposed bone, grade 3.
Statistics
All statistical analyses were performed using IBM SPSS Statistics for Windows version 22.0 (IBM Corp., Armonk, NY, USA). The Shapiro–Wilk test was conducted to determine the data distribution. The Mann–Whitney U test was used for all statistical comparisons between the control group and the CP group. Correlation analyses were calculated using Spearman’s rho test. Receiver operating characteristics analysis was performed to determine the optimal cutoff MSFTT and PSFTT values indicative of the presence of CP. For all analyses, p-values of <0.05 were considered statistically significant.
Results
A study flow diagram is shown in Figure 3. No patients were excluded because of missing data; however, 17 patients whose images showed motion artifacts that prevented accurate measurement of SFTT were excluded. The Shapiro–Wilk test indicated that the PSFTT and MSFTT values were non-normally distributed; therefore, a non-parametric test (Mann–Whitney U test) was carried out to compare the SFTT measurements between patients with and without CP.

Study flow diagram.
The mean values in each group according to the modified Noyes classification are presented in Table 1. The PSFTT and MSFTT measurements were significantly different between patients with and without CP (p < 0.001 for both) (Table 2). The PSFTT and MSFTT values were higher in patients with than without CP for both women and men (p < 0.001) (Figure 4). The PSFTT and MSFTT measurements were higher in women than in men (p < 0.001); this result was observed in all CP grades and in patients without CP.
Mean PSFTT and MSFTT values according to CP classification and sex differences.
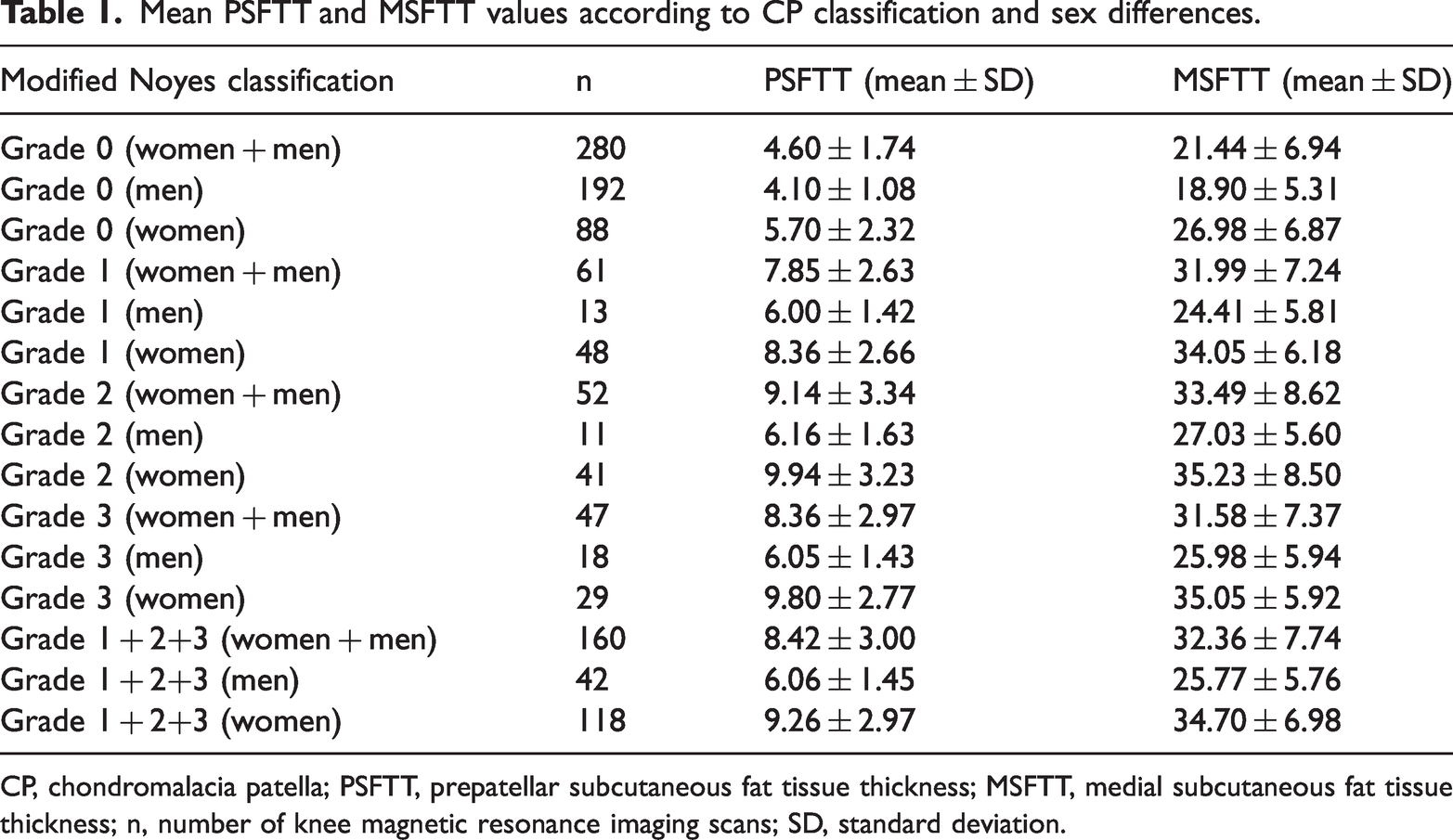
CP, chondromalacia patella; PSFTT, prepatellar subcutaneous fat tissue thickness; MSFTT, medial subcutaneous fat tissue thickness; n, number of knee magnetic resonance imaging scans; SD, standard deviation.
Comparison of PSFTT and MSFTT values between patients with and without CP.

CP, chondromalacia patella; PSFTT, prepatellar subcutaneous fat tissue thickness; MSFTT, medial subcutaneous fat tissue thickness; n, number of knee magnetic resonance imaging scans; SD, standard deviation.
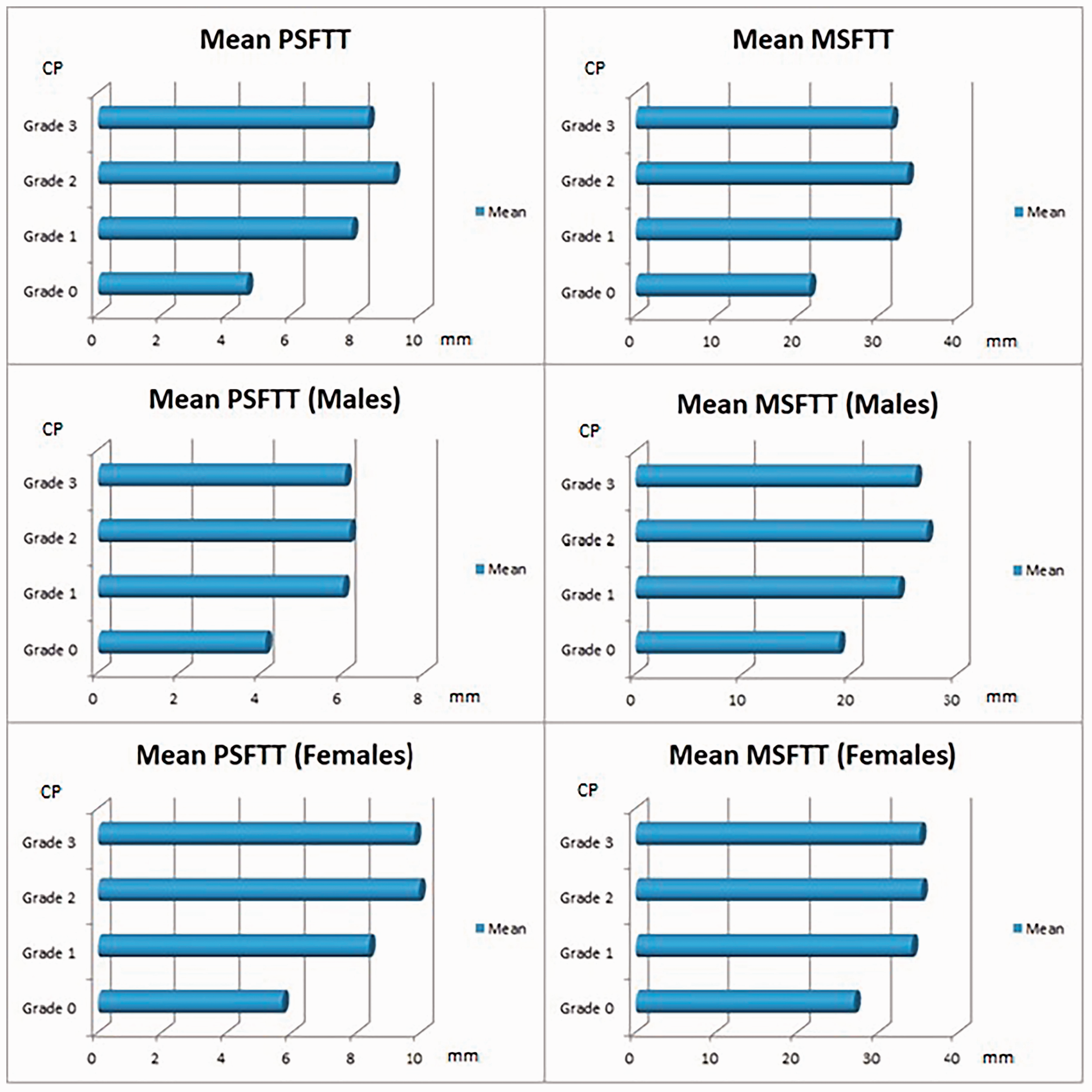
Comparison of the mean values of each CP group for all patients, men, and women
A significant and positive moderate correlation was found between the PSFTT and MSFTT measurements and the CP classification ranks for both women and men. For all patients (women + men, women, and men), the MSFTT measurements were positively and moderately correlated with the CP classification ranks, whereas the PSFTT measurements were positively and strongly correlated with CP classification ranks. A significant, positive, and strong correlation was found between PSFTT and MSFTT for all patients and for women. A significant, positive, and moderate correlation was observed between PSFTT and MSFTT for men (Table 3).
Correlation between PSFTT and MSFTT values and CP

CP, chondromalacia patella; PSFTT, prepatellar subcutaneous fat tissue thickness; MSFTT, medial subcutaneous fat tissue thickness.
The highest value of sensitivity times specificity was obtained for PSFTT of 5.80 mm as a cutoff value for indicating the presence of CP (80.0% sensitivity, 82.9% specificity). Moreover, MSFTT of 25.615 mm showed 84.4% sensitivity and 75.7% specificity according to the receiver operating characteristics analysis (Figure 5).

(a) A prepatellar subcutaneous fat tissue thickness value of 5.80 mm showed 80.0% sensitivity and 82.9% specificity as a cutoff value to indicate the presence of chondromalacia patella (area under the curve, 0.888) and (b) A medial subcutaneous fat tissue thickness value of 25.615 mm showed 84.4% sensitivity and 75.7% specificity when considered a cutoff value to indicate the presence of chondromalacia patella (area under the curve, 0.856). ROC, receiver operating characteristics.
Discussion
This study revealed a significant relationship between SFTT and CP (using both prepatellar and medial measurement approaches) and identified certain cutoff values with high sensitivity and specificity for the presence of CP. This significant relationship was observed not only for all study patients but also for men and women separately.
CP is one of the most common patellofemoral disorders causing anterior knee pain. Trauma, patellofemoral instability (subluxation or dislocation), increased cartilage vulnerability (congenital conditions and the postarthrotomy rehabilitative period), abnormal kinematics of the patella (e.g., patella alta, knees with valgus deformity), and certain anatomical variations of the bone (osteochondral ridge and flattened lateral femoral condyle) are factors that play a role in the etiology of CP. 15 In a study with a large series of patients (n = 301), the sulcus angle, patellar angle, trochlear depth, and patellar tilt were measured to investigate a possible relationship between these anatomical factors and CP. The trochlear depth and lateral patellar tilt angle were significantly lower and the sulcus angle was higher in patients with than without CP. 16 Moreover, in another study of 200 patients with knee pain, a lower lateral patellar tilt angle, higher sulcus angle, and lower trochlear depth were observed in patients with than without CP. 17
Adiposity reportedly has a positive association with cartilage defects, and an increased body mass index is associated with an increased prevalence of patella cartilage defects. 4 Additionally, baseline obesity (body mass index, weight, and adiposity [fat mass and percentage of body fat]) was found to be associated with an increased annular rate of patellar cartilage volume loss over a 2-year period in healthy adults without clinical osteoarthritis of the knee. 3 Not only the biomechanical factors of increased weight and adiposity but also the metabolic effect of increased adipose tissue play a role in CP development. Adipose tissue was historically thought to store energy, but it is now considered to act like an endocrine organ responsible for releasing cytokines such as tumor necrosis factor and interleukin-1 as well as adipokines such as leptin, resistin, and adiponectin. 18 Interleukin-1 and tumor necrosis factor alpha have been found to be associated with cartilage destruction and osteoarthritis. 19
Few studies have compared the results of research such as that described above. To ensure comparability of the results with other studies, similar methodologies and classifications were chosen in this study. Grades 2A and 2B were not used for this reason; all patients were considered to have grade 2 CP according to the modified Noyes classification. Kok et al. 14 analyzed 170 patients, and MSFTT was measured in each patient’s MRI scan to determine its relationship with CP. The mean SFTT was significantly higher in all grades of CP than in the control group. A significant correlation was found between SFTT and the CP grade. Women had higher SFTT values than men. 14 Duran et al. 13 studied 175 patients and measured PSFTT to identify any relationship with CP. The authors reported that PSFTT was higher in the CP group than in the control group, a positive correlation was found between PSFTT and CP (r = 0.47), and thicker SFTT was observed in women than men. 13 The results of the present study were very similar to both of these studies and underlined the main results. In addition, when compared with the results of previous studies, the PSFTT measurements in the present study indicated a stronger correlation between SFTT and the CP grade. Moreover, the present study revealed the cutoff SFTT measurements for the medial and prepatellar approaches. In addition, PSFTT showed a strong positive correlation with MSFTT for all patients and for women.
To the best of our knowledge, this study involved the largest population to date among all studies evaluating the relationship between SFTT measurements and CP. Additionally, two methods were used in this investigation to show this possible relationship. However, few studies have focused on this subject, and it might be beneficial to use these values (PSFTT and MSFTT) because of their easy measurement on routine knee MRI. With this additional information in the literature, future research might benefit from the threshold values indicated in this study to predict the occurrence of CP earlier and may reveal a person’s tendency to develop chondral injuries of the patella.
Several limitations of this study should be considered before interpreting the results. First, although patients with moderate or severe osteoarthritis were excluded, the inclusion of older patients might have influenced the results because of the possible effect of age on CP. Second, patients with and without CP were compared using nonparametric tests because the Shapiro–Wilk test indicated non-homogeneous data distributions. Comparison of values gathered from larger populations might help obtain a normal data distribution in each group; thus, parametric tests should be performed to improve the accuracy of the results. Third, although SFTT is widely used as a surrogate marker of obesity and a strong relationship was found between subcutaneous fat and obesity, inclusion of the body mass index of each patient would have provided additional value to the investigation. Fourth, this study was conducted using a 1.5-Tesla MRI machine. Because 3.0-Tesla MRI scanners are preferable for assessment of chondromalacia, future studies with a higher magnetic field strength would provide more accurate results. Fifth, the patients’ lifestyle factors (e.g., sport activities, sedentary lifestyle) were underestimated in this investigation. Awareness of daily activities or sports habits would provide more detailed results for discussion of this topic. Finally, although the measurements were performed by two highly experienced radiologists, the interobserver and intraobserver differences along with the intraclass correlation coefficients would be more helpful for examination of the results.
Conclusions
According to the results of this study, the SFTT in the knee might be associated with the presence of CP. Additionally, the results of this investigation indicate that both MSFTT and PSFTT are significantly correlated with the CP grade of the knee. The prepatellar and medial threshold values of SFTT identified in this study, which indicate the presence of CP with high sensitivity and specificity, might be useful for prediction of CP and may be valuable in preventive medicine. More investigations with larger populations that take the limitations of this study into consideration would provide a better understanding of the exact relationship between SFTT and CP.
Footnotes
Author contributions
Data availability statement
The datasets generated and/or analyzed during the current study are not publicly available because of the risk of breaching patient data privacy. However, anonymized data are available from the corresponding author upon reasonable request.
Declaration of conflicting interests
The authors declare no conflict of interest regarding the publication of this paper.
Ethics approval
This study was approved by the institutional ethics committee (Erzincan Binali Yıldırım Universitesi, Tıp Fakültesi Dekanlığı, Klinik Araştırmalar Etik Kurulu, Erzincan/Turkey, Date: 6 October 2022, Number: 03487, Session: 10, Approval number: E-18532602-114.15-943185).
Funding
The authors declare no financial support or funding.