
Abstract
Purpose:
The purpose of this study is to develop an evidence-based algorithm for the management of symptomatic bipartite patella in the pediatric and adolescent population based on a systemic review of the published literature.
Methods:
A systematic review of the literature was conducted using the Preferred Reporting Items for Systematic Reviews and Meta-analyses guidelines on PubMed and Embase, selecting for studies discussing the management of symptomatic bipartite patella.
Results:
Five studies met criteria, involving 315 knees (314 patients, average age 15.8 years). All patients presented with symptomatic bipartite patella and underwent an initial trial of conservative management. Seventy-six percent (239 knees) achieved full resolution of symptoms after conservative management at a median of 1.9 months. The remaining 76 knees (24.12%) had persistent symptoms requiring operative intervention. Surgical techniques included surgical excision, screw fixation, synchondrosis drilling, lateral release, and both arthroscopic and open interventions (92.1%). Most patients (90.79%) who underwent surgical intervention had partial or complete resolution of their symptoms. Seven of 76 knees (9.21%) needed management postoperatively for pain due to trauma, residual symptomatic ossicles, and hardware complications. Of these, four patients required reoperations (average 2 years). The remaining three patients had satisfactory outcomes with an additional course of conservative management and oral analgesics.
Conclusion:
Management of symptomatic bipartite patella should begin with a trial of conservative management. With refractory symptoms lasting greater than 3 months, surgical intervention may be considered with positive outcomes of partial or complete resolution of symptoms. The proposed algorithm is provided to guide physician management of symptomatic BPP in pediatric or adolescent patients.
Keywords
Introduction
Bipartite patella (BPP) is the developmental anomaly of the patella, resulting in two unfused patellar ossification centers. The patella is the largest sesamoid bone with multiple ossification centers that fuse together. When two or more of these ossification centers fail to fuse, a bipartite (2 pieces), tripartite (3 pieces), or multipartite (4 pieces) patella may be the result. Typically, these ossification centers fuse between ages 2 and 6 years to create one large center1,2; however, in a subset of the population, the un-fused portions will persist as a fibrocartilaginous synchondrosis and are evident by 8–12 years of age. 3
Saupe proposed a classification system for BPP in 1943. 4 Type 1 involves an accessory fragment that is inferior to the patella (5% of patients); Type 2 involves an accessory fragment that is on the lateral margin of the patella (20%). Type 3 involves an accessory fragment that is superolateral to the patella and is the most common anomaly (70%; Figure 1).3 –5
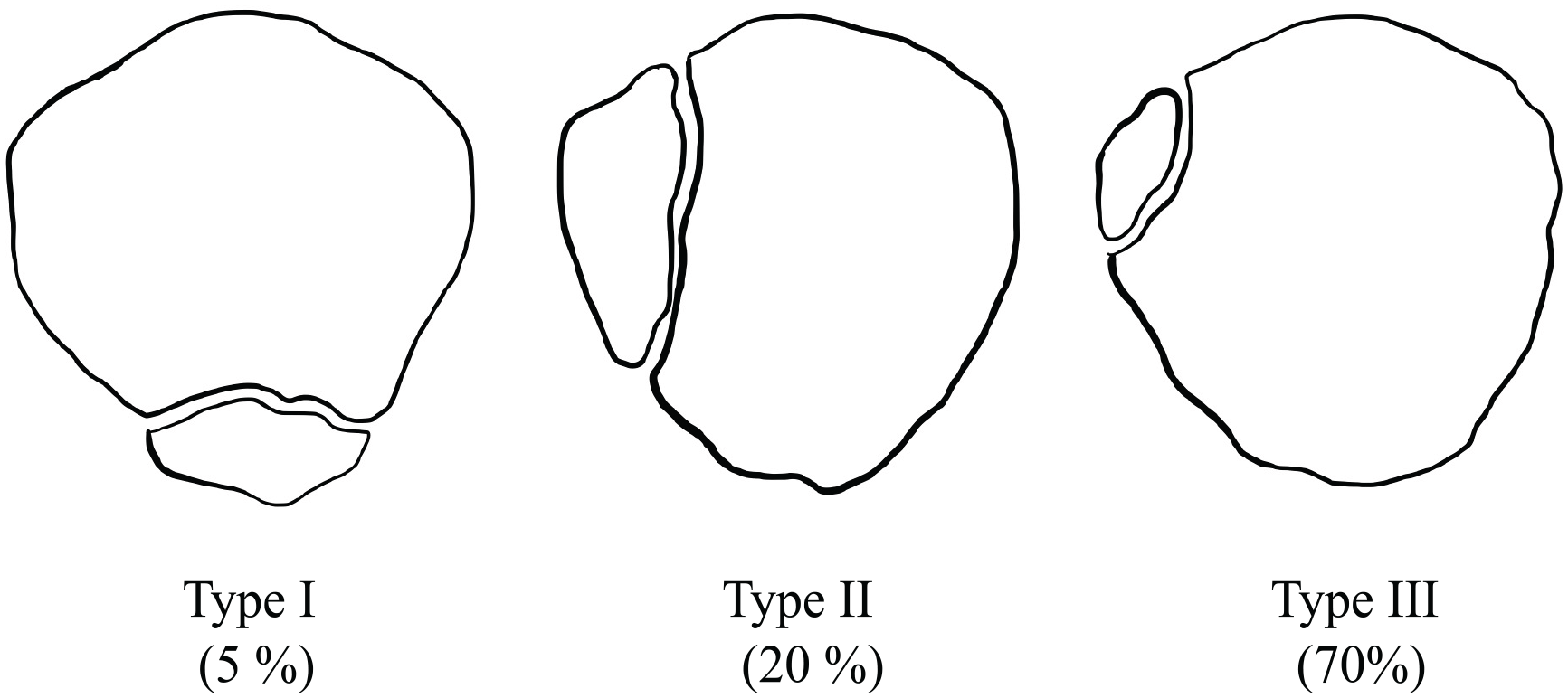
Illustration of Saupe 6 (1943) classification of bipartite patella with prevalence.
BPP has an incidence of 2%–6%, with a 9:1 male-to-female ratio.1,6 –8 BPP is typically found incidentally 3 on imaging and is asymptomatic in most patients. 5 Of diagnosed cases, BPP is bilateral 50% of the time. 6 In the subset that are symptomatic, they tend to present with anterior knee pain that is exacerbated by activities or sports with repetitive force through the extensor mechanism.2,9 They may present with tenderness to palpation over the synchondrosis of the unfused ossification center,10,11 which tends to correlate superolateral on the radiograph. 12 Pain typically begins after a traumatic blow to the patella or repetitive forces, such as running and jumping. A commonly believed hypothesis is that either of these mechanisms leads to symptoms by disrupting the fragile fibrocartilaginous interface between the accessory and main fragment. 13
Management options for symptomatic BPP range from nonoperative interventions to surgical management. Optimal management is multifactorial including severity, duration of symptoms, activity level, and additional associated symptoms. Conservative management consists of activity modification, rest, ice, bracing, gentle stretching, and physical therapy.9,10 Generally, a course of conservative management is attempted prior to surgical intervention. Surgical management includes a wide variety of techniques with equal efficacy per the sparse available literature. 12 This review will not comment on the described operative techniques.
There are a small number of patients with BPP who are symptomatic while the majority are asymptomatic. There is sparse literature focusing on those with symptomatic BPP. There are no previous studies that propose a treatment algorithm for symptomatic patients. The purpose of this study is to review the current literature via systematic review to determine an evidence-based management algorithm for symptomatic BPP in patients less than 21 years old.
Materials and methods
Search strategy
A systematic review was conducted according to Preferred Reporting Items for Systematic Reviews and Meta-Analyses guidelines. A meta-analysis was not performed due to the heterogeneity of operative techniques and limited data availability. A digital search of MEDLINE (PubMed) and Embase was conducted for papers between 1990 and 2023. The search strategy included the following key terms: “pediatric” OR “adolescent” OR “child” AND “symptomatic” AND “BPP.” All potential studies were stored in EndNote20 (www.endnote.com), a software program used as a bibliographic citation manager.
Study selection
All studies that were retrieved by this process were screened by title and abstract. A full literature review was conducted for those remaining that described management strategies for symptomatic BPP. Exclusion criteria included (a) adult patient populations, defined as age > 21 years; (b) case series with fewer than five pediatric patients; (c) case series lacking sufficient follow-up, defined as a minimum of 6 months if there is surgical intervention and until resolution of symptoms in conservative management; (d) studies involving cadaveric specimens; and (e) studies published in languages other than English without available translations.
Data extraction
Fourteen articles underwent full-text review. The following information was collected from each article: number of patients; age range; symptom duration; laterality; preoperative imaging; treatment used; prior treatments; additional procedures performed on knee; follow-up length; classification/fragment location; follow-up symptoms; return to sport/activity; and rate of reoperation for BPP. The outcomes of the therapies used were investigated for each of the patients. Lastly, if supplied in the study, specific function and/or pain scores were recorded as well; however, these metrics were not included in all articles. For studies that did not explicitly describe the prior categories, the data collection was left unrecorded.
Results
Search results
The search strategy found 24 studies for screening via PubMed and Embase search. After title and abstract screening for relevance to the listed criteria, 14 underwent full-text review, and 5 studies qualified after exclusion criteria and exceptions (Figure 2). One of the five studies 14 included an age range from 18 to 27 and those patients older than 21 years and unsegregated data were excluded from the review.
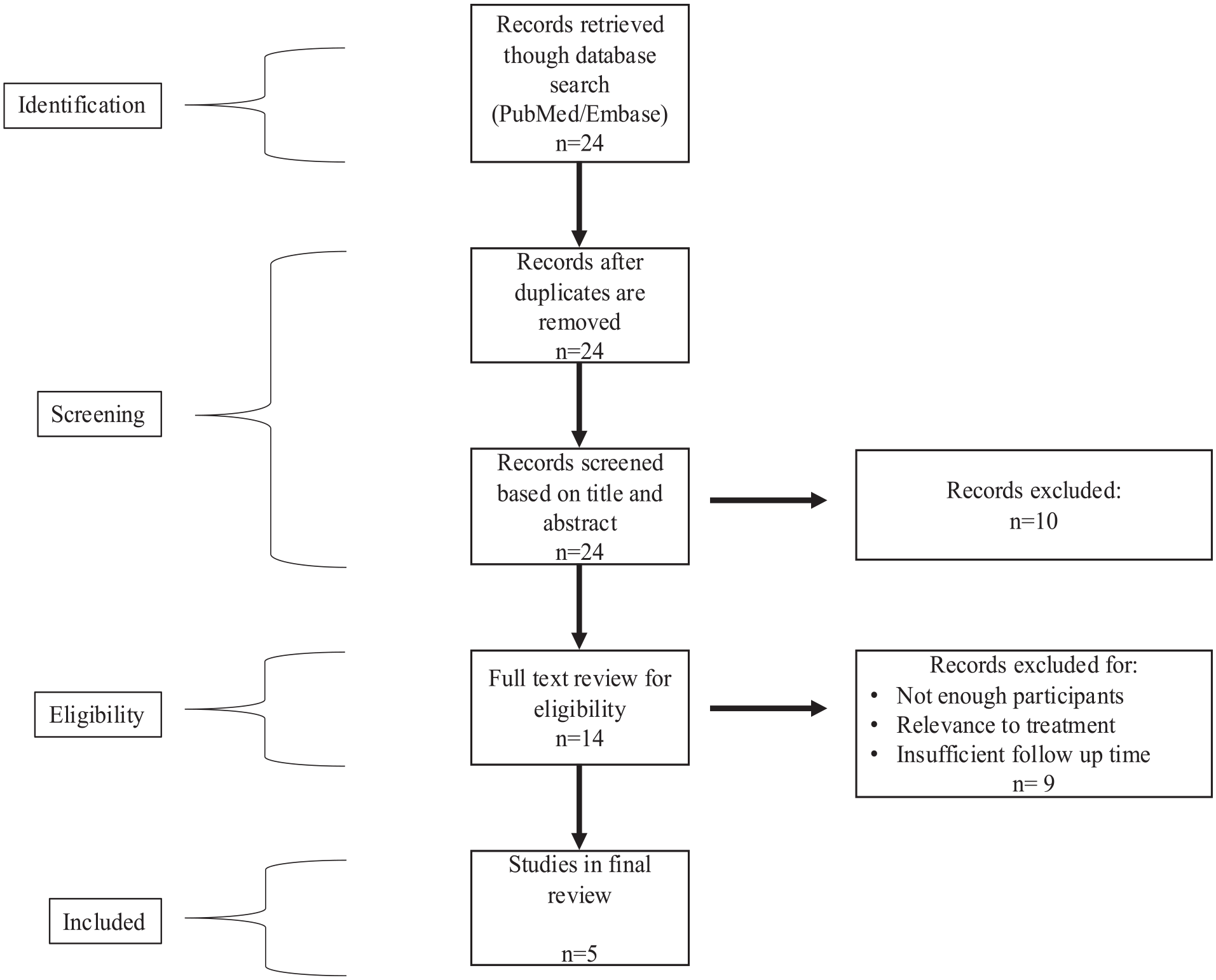
PRISMA flow diagram of the records retrieved from the database search and review process.
Study characteristics
All five of the included studies1,12,14,15,16 were retrospective cohort studies. In total, these studies represented 315 knees of 314 patients with an average age of 15.8 years. The results are presented in the order published. The level of evidence of this study is 3 given the selected papers.
Diagnosis
All the knees that were evaluated for this review were diagnosed via imaging in addition to clinical evaluation.
Treatments and outcomes
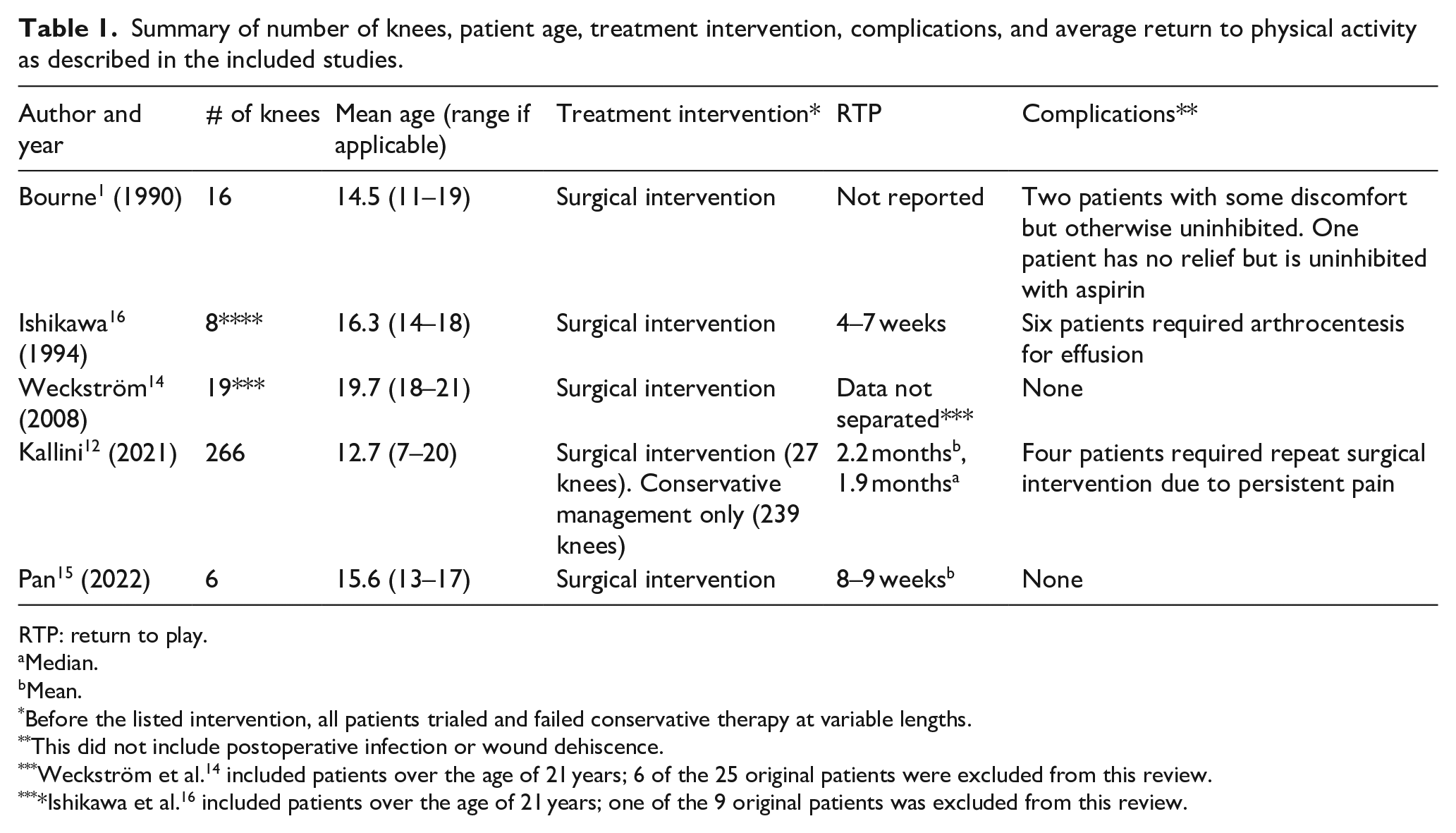
Bourne and Bianco 1 examined 16 patients (16 knees) with an average age of 14.5 years and an average follow-up period of 7 years. All patients had attempted conservative treatment for >2 months without adequate resolution and ultimately underwent operative excision of the BPP fragment. Patients were followed until they became asymptomatic and were assessed on pain relief, range of motion, ability to resume previous activity level, patient satisfaction, and subsequent surgeries needed. In all, 13 of the 16 patients experienced complete relief and were able to resume activities at the same level as prior. The article did not comment on the time to return to the previous level of activity. Two patients experienced occasional discomfort; however, it did not limit their ability to return to the previous level of activity nor did it require additional interventions. The remaining patient experienced no relief of symptoms but was able to resume normal physical activity with oral nonsteroidal anti-inflammatory drugs at the 3-year follow-up (Table 1).
Summary of number of knees, patient age, treatment intervention, complications, and average return to physical activity as described in the included studies.
RTP: return to play.
Median.
Mean.
Before the listed intervention, all patients trialed and failed conservative therapy at variable lengths.
This did not include postoperative infection or wound dehiscence.
Weckström et al. 14 included patients over the age of 21 years; 6 of the 25 original patients were excluded from this review.
Ishikawa et al. 16 included patients over the age of 21 years; one of the 9 original patients was excluded from this review.
Ishikawa et al. 16 examined nine patients (nine knees) between ages 14 and 21. One patient over the age of 21 was excluded from our analysis. In total, there were eight patients (eight knees), with an average age of 16.3 years and an average follow-up period of 5.34 years. All patients were initially treated with 3 months of nonoperative management including nonsteroidal anti-inflammatory drugs, steroid injections, or immobilization. All eight patients continued to have persistent pain and underwent excision of BPP. No functional assessment scale was provided in this study; however, it is noted that five to six patients experienced a knee effusion requiring arthrocentesis 1–2 weeks after surgery. All patients were able to return to their prior level of sports performance within 4–7 weeks.
Weckström et al. 14 examined 25 military recruits (25 knees) between the ages of 18 and 27. Patients over the age of 21 were excluded from our analysis. In total, there were 19 patients (19 knees) with an average age of 19.7 years and an average follow-up period of 15 years. All the patients were initially treated conservatively with restriction of activities and nonsteroidal anti-inflammatory drugs, however, continued to have persistent pain. 94.7% of patients in this cohort underwent open subperiosteal excision of the bipartite fragment and the remaining one patient had an arthroscopic removal of the fragment. Postoperatively, patients’ functional ability was measured on the Kujala et al. 17 scale that is scored out of 100, with 100 being consistent with no symptoms or difficulties with physical activity. The average Kujala score was 94 for the cohort of 19 patients screened postoperatively.
Kallini et al. 12 conducted a retrospective study of 266 patients, with an average age of 12.7 years and a minimum follow-up of 6 months. Of the 266 patients, 27 (10%) underwent surgical intervention. Operative treatments included fragment excision (n = 9), fragment excision with lateral release (n = 8), isolated lateral release (n = 5), fragment screw fixation (n = 4), and arthroscopic drilling (n = 1). Those who were treated operatively were more likely to be older, competitive athletes, female, and have longer duration of symptoms compared to the conservatively managed patients. Four of the 27 patients had persistent symptoms that required additional surgical intervention, which included repeat fragment excision for retained pieces, hardware removal, and a lateral release after sustained trauma to the knee. Reoperation happened at a mean interval of 2 years after initial surgery. The other 23 were able to return to physical activities on average 2.2 months postoperatively. The remaining 239 patients in this retrospective review were treated with conservative management alone; 233 patients successfully returned to sport at a median of 1.9 months (range: 1.4–3.1). Six of the 239 patients had residual symptoms but declined operative intervention.
Pan and Hennrikus 15 performed a retrospective study that involved five patients (six knees), with an average age of 15.6 years and an average follow-up of 19 months. All patients had failed more than 6 months of conservative treatment including activity restriction, physical therapy, icing, nonsteroidal anti-inflammatory drugs, and stretching. All patients underwent fragment excision (4 open, 2 arthroscopic-assisted) ± lateral retinacular release. Patient function was measured via the Lysholm Score 18 comprised of questions about symptoms and physical function, with a maximum score of 100 representing complete resolution of symptoms without physical deficit. The average score at the final follow-up visit was 97. All patients had complete resolution of symptoms and were able to return to physical activity at an average of 9.8 weeks.
With these five studies combined, there were 315 knees (314 patients, average age 15.8 years) to study. Seventy-six percent (239 knees) achieved full resolution of symptoms after conservative management at a median of 1.9 months. The remaining 76 knees (24.12%) had persistent symptoms requiring operative intervention. Most patients (90.79%) who underwent surgical intervention had partial or complete resolution of their symptoms. Seven of 76 knees (9.21 %) needed management postoperatively for pain due to trauma, residual pain, and hardware complications. Of these, four patients required reoperations (average 2 years). The remaining three patients achieved a satisfactory outcome with an additional course of conservative management and oral analgesics.
Discussion
BPP affects 2%–6% of the population and is typically an incidental finding on imaging that remains asymptomatic.1,3,6 –8 For the subset of patients with symptomatic BPP, there is little consensus on best management practices given its rarity. Of the studies included, 76.85% of patients were successfully managed conservatively. The remaining 24% of patients underwent surgical intervention after the failure of conservative therapy with 9.21% achieving partial, and 90.79% achieving complete resolution. Of those who achieved partial relief with conservative therapy, 57.1% (4/7) required additional surgical management for persistent pain postoperatively and the remaining did not seek further surgical management despite incomplete resolution of symptoms. The following algorithm was created after a systematic review, to help guide the management of symptomatic BPP.
Diagnosis and evaluation
The diagnosis of BPP is typically an incidental finding on radiographic imaging. 3 If the patient is asymptomatic, there is no need to treat the radiographic finding, and no specific follow-up is known to be warranted. If a child or adolescent presents with anterior knee pain, with tenderness to palpation over the patella, and a symptomatic BPP is suspected, standard knee radiographs should be obtained. If the patient is presenting after an acute trauma, radiographs should be obtained and consideration for advanced imaging (MRI and/or CT) is warranted if further information is needed. 6 The advanced imaging can further delineate an acute, traumatic fracture from an acute exacerbation of an underlying chronic condition. 6 If BPP is found radiographically in one knee, and fracture has been ruled out, a contralateral X-ray should be performed as it has a bilateral incidence of 43%. 19 Of note, 16 patients included in these studies did not have explicit documentation of how the diagnosis was made. 1
Treatments and outcomes
Upon presentation and diagnosis of symptomatic BPP, management should start with conservative strategies including activity modification, rest, ice, immobilization, stretching, and physical therapy. 9 In this systematic review, all patients included were initially treated conservatively; 76% of patients were successfully able to return to their prior level of activity with conservative treatment alone at a median time of 1.9 months (1.4–3.1 months). 20
Once conservative management has been exhausted, if patients do not have adequate relief and the pain is affecting their quality of life, consideration of surgical intervention is warranted. In this systematic review, risk factors for patients who were more likely to fail conservative management included longer duration of symptoms before presentation, older age at initial presentation, and participation in competitive athletics. 12 In regard to operative management, the most common procedure performed was open surgical excision of the bipartite fragment. Kallini et al. 12 found in their investigation that there was no significant difference in time to return to sports between the surgical techniques, which was consistent with conclusions from adult systematic reviews and smaller case studies.21,22 Additional procedures performed included surgical fixation of the fragment via screw fixation, synchondrosis drilling, and lateral release (in isolation or combination). The majority of procedures were performed open and 5.26% of procedures were arthroscopic. Out of the patients managed operatively, 90.79% achieved full resolution of symptoms and returned to a prior level of activity anywhere from 6 to 13 weeks postoperatively. Overall, this was a longer time frame than the conservatively managed patients. Of the seven patients for which the initial surgical intervention did not adequately treat their pain, four underwent an additional operative intervention while the other three continued a conservative approach with an eventual return to physical activity. 1 Of the four patients who underwent additional operative intervention, it is notable that one sustained a dashboard trauma after full resolution of symptoms, two had complications with the hardware placed in original surgery, and the final had their original surgery at a different institution. One patient had no relief from surgical intervention and was managed long term with oral analgesics. 1
Kallini et al. 12 discusses that due to the retrospective nature of their study, there was often no identifiable indication to warrant one technique or another. At this point, there are no superior surgical techniques. Technique varied depending on Saupe classification; Saupe I was treated through an incision over the inferior pole of the patella, and Saupe II and III through a lateral incision.
Management algorithm
Based on this review of existing literature, the following management algorithm is proposed (Figure 3). Careful diagnostic workup is necessary, particularly in a patient with anterior knee pain with a radiographic finding of BPP. It is imperative to rule out acute fracture, intra-articular pathology, ligamentous injury, and extensor mechanism defects. If imaging studies are negative for acute findings, then a diagnosis of symptomatic BPP may be made. We recommend that all patients should undergo at least 3 months of conservative treatment. If conservative management fails, or the patient declines a 3-month trial, surgical intervention may be considered. Studies have shown no meaningful difference between the operative techniques described above. While data on screw fixation are not available, it has been recommended that for larger fragments, fixation may be favored over excision to preserve the anatomy of the patella and prevent patellofemoral incongruity. 9 As seen in the available literature, hardware prominence and irritation may require additional surgical procedures in the future.
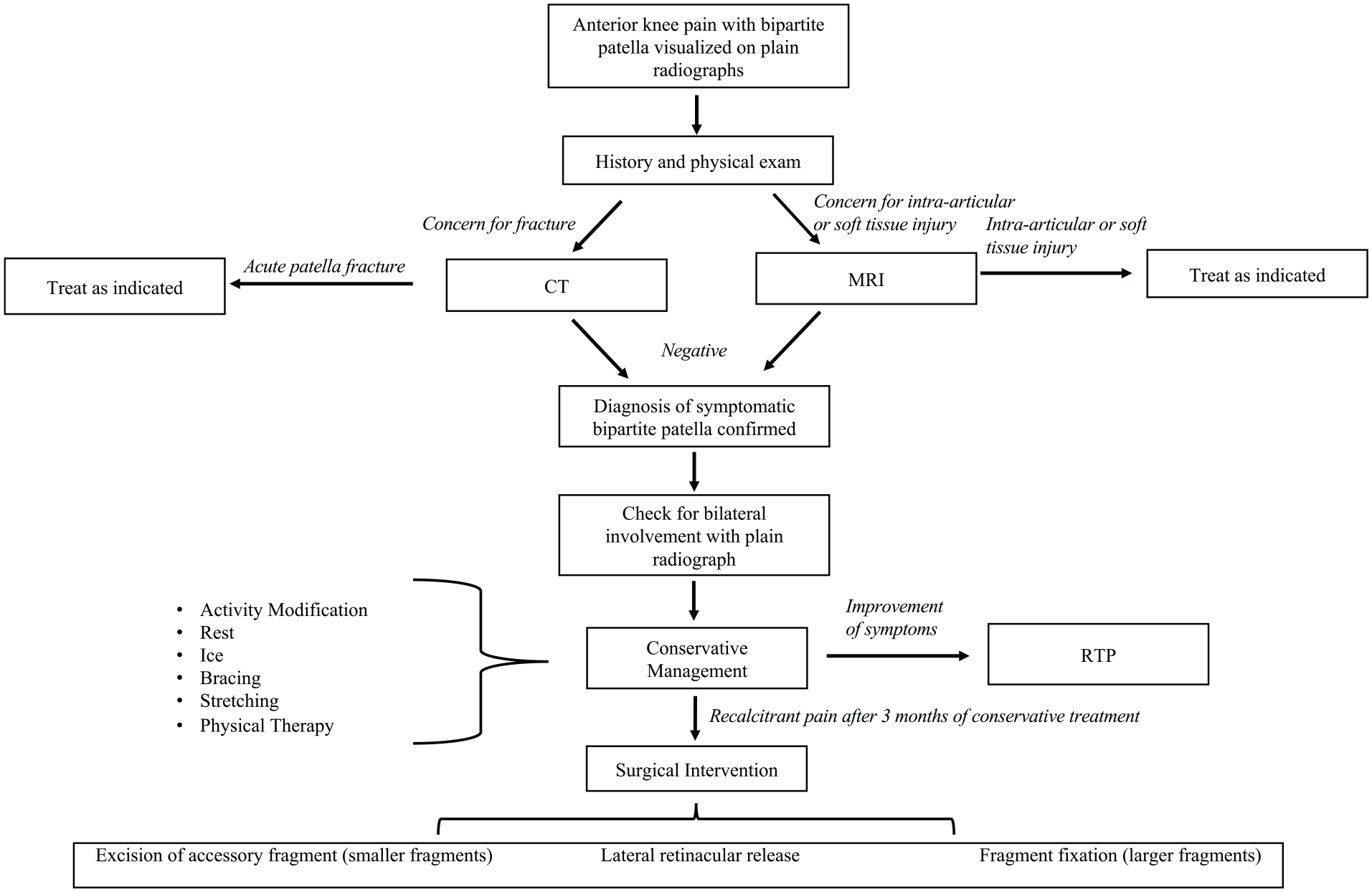
Management algorithm to guide treatment of pediatric symptomatic bipartite patella.
Alternative treatment modalities
Recent literature has introduced novel treatment modalities that require further investigation at this time, however, may have a role in the management algorithm in the future. These include ultrasound-guided injection of either steroid or lidocaine and fenestration of the capsule-tendinous structures. 23 The ultrasound-guided injection and fenestration were performed in an outpatient clinic under local anesthetic. Nakase et al. 23 examined 14 patients (15 knees), with an average age of 13 years and a follow-up of 3 months using this novel technique. Patient function was assessed via the Victorian Institute of Sport Assessment questionnaire, 24 comprised of questions referring to symptoms, functional status, and ability to perform tasks. The questionnaire was scored out of 100, with 100 being ideal physical health; the average at 3 months after treatment was 88.6. Two patients (three knees) required additional surgical intervention due to residual symptoms, while the other 12 patients returned to activity on average 4.2 weeks after the procedure. This study was limited to only Type 3 BPP, therefore potentially limiting its generalizability to all subtypes of BPP. More information is needed to determine whether this could be a viable option in the future. Given insufficient follow-up and data, this was not formally included in the review above.
Limitations
The analysis presented in this review is subject to the limitations of the included studies including retrospective study designs, small sample sizes, the lack of randomized trials, possible non-adherence to conservative management instructions, lack of a standardized nonoperative protocol, postoperative protocol or surgical technique utilized, and monitoring of functional outcomes. The lack of standardization of conservative treatment protocol causes inconsistent results and subsequently limits the analysis of the efficacy of the treatment. The studies in the review also do not consistently supply information about the method of confirmation of diagnosis.
Conclusion
BPP is a developmental anomaly that is usually asymptomatic and found incidentally. However, in a small subset, it can manifest as anterior knee pain and interfere with activity. This study utilizes a systematic review to help guide the management of symptomatic BPP in pediatric or adolescent patients (<21 years) and a proposal of a management protocol to help guide management.
Supplemental Material
sj-pdf-1-cho-10.1177_18632521241308410 – Supplemental material for Treatment of symptomatic bipartite patella in patients <21 years of age: A systematic review and treatment algorithm
Supplemental material, sj-pdf-1-cho-10.1177_18632521241308410 for Treatment of symptomatic bipartite patella in patients <21 years of age: A systematic review and treatment algorithm by Kristen E Hines, David S Liu, Amy E Steele, Daniel Gabriel, Angie M Prahbat, Yi-Meng Yen and Grant Douglas Hogue in Journal of Children’s Orthopaedics
Footnotes
Author contributions
Kristen E Hines: formal analysis, investigation, methodology, writing—original and draft, review and editing. David S Liu: Conceptualization, methodology, formal analysis, Writing—review and editing. Amy E Steele: Methodology, formal analysis, Writing—review and editing. Daniel Gabriel: Methodology, Writing—review and editing. Angie M Prahbat: Investigation, Writing—review and editing. Yi-Meng Yen: Conceptualization, Writing—review and editing. Grant Douglas Hogue: Conceptualization, Writing—review and editing.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics
There are no human participants in this article and informed consent is not required.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.