
Abstract
Purpose:
Objectives were to evaluate if gait was improved after multilevel surgery on the involved leg and simultaneously performed guided growth procedure on the uninvolved leg and whether simultaneously performed guided growth is efficient in limb length discrepancy management in hemiplegic children.
Methods:
Gait pattern of 78 hemiplegic children (mean age 10.4 years) was evaluated using instrumented gait analysis before surgery and at 2 years. This study involved children with type 2a (Rodda and Graham classification) – 12, type 3 – 20, type 4 – 23, type 4s (undergone triceps lengthening at early age) – 23.
Results:
The mean limb length discrepancy was 2.3 cm before surgery and 0.4 cm at final control. In all patients aged over 144 months, the residual length discrepancy was over 10 mm. The improvement in gait kinematics was observed on both the uninvolved and hemiplegic limbs. Finally, control on uninvolved leg kinematics presented values similar to reference values. On the involved leg, there were significant improvements in sagittal and transverse kinematics. Only patients of the 4s (patients undergone previous triceps lengthening surgery at an early age) group had no improvements in ankle flexion moment and power generation.
Conclusion:
Multilevel surgery including simultaneous guided growth ensures improvements on both the uninvolved and hemiplegic limb gait kinematics. We suggest guided growth surgery before the age of 12 years for more exact equalization. Isolated triceps performed at an early age represent negative conditions for plantar flexion strength development in long term.
Introduction
The prevalence of cerebral palsy (CP) ranges from 1.5 to 4.2 per 1000 live births.1,2 Unilateral spastic cerebral palsy (USCP) is characterized by unilateral involvement with an asymmetrical gait pattern, but most patients reach an adequate level of motor function and independent walking.3–7
Most publications agree that a combination of factors, such as muscle tone, impaired motor control, muscle contractures, skeletal deformities and leg length discrepancy affect gait in children with spastic hemiplegia.8–12 As a result, instrumented gait analysis reveals gait deviations on the involved side, such as foot drop, fixed equinus, reduced range of motion (ROM) at knee and hip, transverse plan deviation at hip and pelvis, increased pelvic obliquity and hip abduction.10,13,14 It has also been demonstrated that limb length discrepancy (LLD) can lead to equinus recurrence after initial surgery.15,16 Traditionally, it is widely accepted within orthopaedic surgery that the affected side may benefit from a variety of interventions and procedures, however how best to resolve a LLD remains controversial include the effect on the contralateral side.
It is known that a LLD results in adverse effects on the kinematics of the uninvolved limb: significant longer stance phase, slower velocity and shorter stride length on conditions of bare foot and LLD of more than 1 cm.17,18 The long leg compensates with excess flexion of hip and knee.11,17–19 In terms of kinetics, on the uninvolved side are observed increased knee extension moments and excessive ankle power absorption.17,19 Since it is extremely common for children with USCP to have a LLD, all of these patients should be assessed for this and consideration given to treatment.11,18,20–22
Despite numerous studies on the results of surgery to the involved lower limb in USCP, there is very little published regarding the outcomes of leg length equalization surgery. To our knowledge, there are no studies on the outcomes of multilevel surgery accompanied with guided growth with instrumented gait analysis assessment of results. Our first objective was to evaluate the results of guided growth using temporary epiphyseodesis in terms of treating the LLD in this patient group. Our second objective was to evaluate the gait function before and after multilevel surgery on the involved leg with simultaneous guided growth on the uninvolved leg. The null hypothesis of the study was that multilevel surgery with guided growth does not improve parameters of gait analysis.
Materials and methods
Patient selection
Between January 2018 and February 2022, we conducted an institutional review board-approved nonrandomized, prospective study with retrospective analysis (Figure 1).
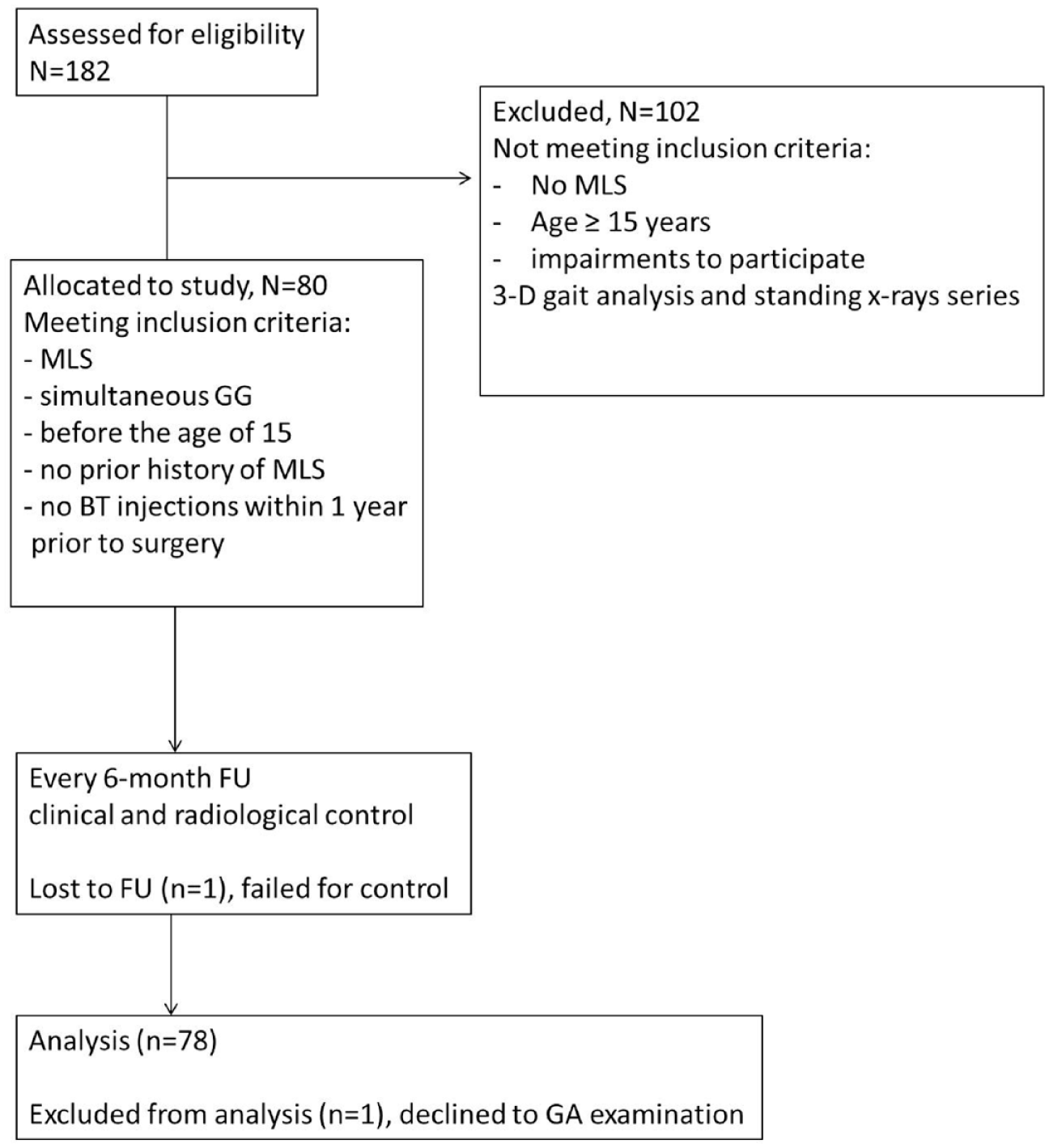
Flow-chart of the study.
Seventy-eight consecutive children with USCP (45 males, 33 females, average age: 10.4 ± 3.9 years) presenting with a LLD greater than 1.5 cm were included in the study from a cohort of 182 patients with USCP. Two of these children were later excluded from analysis (one failed to attend examination, one declined to participate in gait analysis.
We included the patient if a multilevel surgical procedure was performed in combination of simultaneous guided growth for LLD 1.5 mm and more on the uninvolved side before the age of 15 (radiologically open growth plates of distal femur and proximal tibia, before skeletal maturity). Participants had no prior history of multilevel orthopaedic surgery and had not received botulinum toxin injections within 1 year prior to enrollment.
Patients were excluded if they had impairments interfering with their ability to participate in 3D gait analysis and a standing full-length X-ray series at final FU examination. Participants were also excluded if surgery was not multilevel.
Demographic data collected included age, sex, operative segments and elements of surgery. For analysis, patients were grouped according to the Rodda and Graham classification 10 of gait deviation.
The study complies with the Declaration of Helsinki statement on medical protocols and ethics and was approved by the local ethic committee. All patients enrolled in the study or their representatives provided written informed consent.
Surgical procedures
On the uninvolved leg, all the patients underwent guided growth procedures using the medial and lateral ‘eight plate’ technique on tibia or femur. 23 The risks and benefits of intervention were disclosed to individuals participating in the study and their parents. Most parents preferred a single segment guided growth procedure, having concerns about ‘surgery on the healthy leg’. Therefore, the procedure was performed in the segment contributing most to the LLD.
Radiological evaluation of LLD and gait analysis
Weight-bearing full-length AP radiographs of the lower extremities were taken in a standing position using wooden blocks under the involved limb to obtain a level pelvis. In four patients due to fixed hip or knee contractures, we assessed segment length discrepancy using non-weight-bearing computed tomography.
For instrumented gait analysis, patients walked independently or assisted by one hand of their parents, at self-selected speed, barefoot condition, on a 7-m walkway. Data was recorded by Qualisys 7+ camera motion capture system (Oqus 4; Qualisys AB, Göteborg, Sweden) synchronized with six floor-mounted dynamometer platforms (Kistler Instruments Limited, Winterthur, Switzerland). For each patient, a minimum of five trials were captured. The data combined as an average. We compared to age-matched reference values in healthy children established in previous studies. 24 Radiological length parameters, hemiplegic and uninvolved leg gait were evaluated at inpatient facilities immediately before initial surgery and then before the surgery for eight-plate removal.
The same senior paediatric orthopaedic surgeon with expertise in CP patient treatment performed all surgical procedures. Postoperative rehabilitation followed a standardized protocol. 25 Follow-up controls were performed every 3–6 months for clinical and radiological assessment. Hardware (eight-plates) was removed if the patient achieved limb length equalization or at 24 months after surgery in order to avoid unwanted permanent growth arrest. A LLD less than 1 cm was established as the target length discrepancy at the end of treatment.
Statistical analysis
Statistical analysis was conducted with AtteStat 12.0.5 software ((с) 2002-2025 Igor Gaydyshev). Means, standard deviations, and median (25% ÷ 75%) were used to describe continuous variables. We compared pre- and postoperative gait parameters using a paired Wilcoxon signed-rank test. Significance was set at p < 0.05.
Results
A total of 78 patients meeting the inclusion criteria were divided into 4 groups (Table 1) according to Rodda and Graham classification: type 2a, type 3, type 4 and type 4s. The 4s group corresponded to gait deviation classified as type 4, but we grouped there patients who underwent isolated tendo achillis lengthening or myofibrotenotomies at an early age (3–6 years). Within each of these groups, there were no statistically significant differences (p > 0.05) regarding age, gender distribution and preoperative LLD.
Demographic characteristics of the groups.
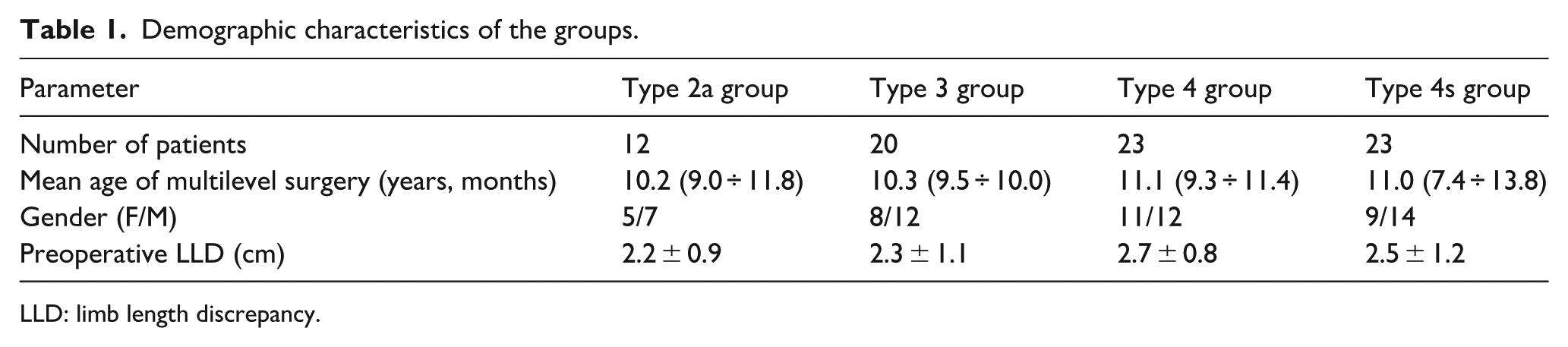
LLD: limb length discrepancy.
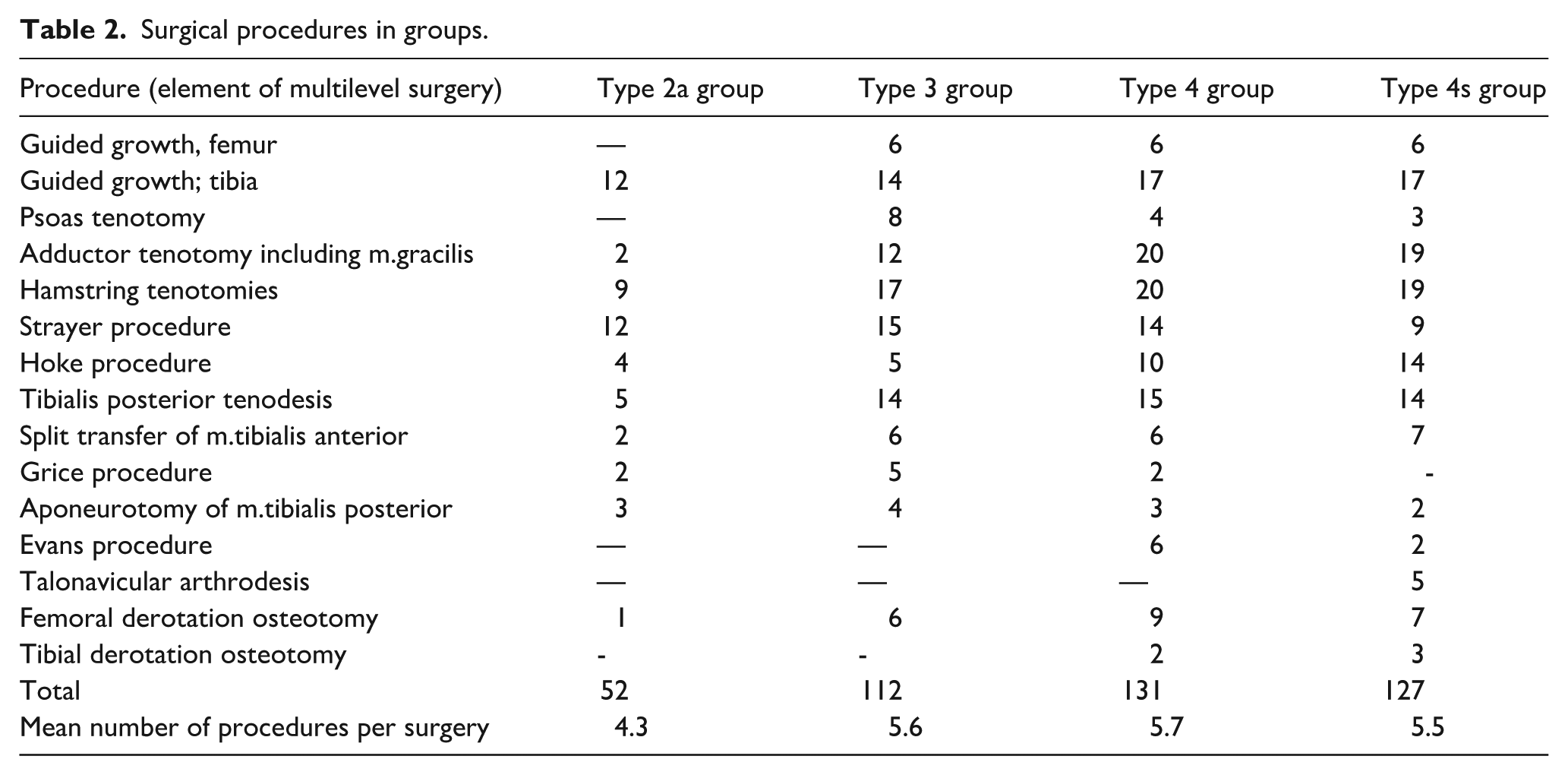
Table 2 represents the type and number of surgical procedures performed in the series. In most cases, guided growth was performed at the proximal tibia. There were 5 cases of talonavicular arthrodesis in the type 4s group in order to correct symptomatic foot deformity. No patient in groups 1–3 required this type of foot arthrodesis. Guided growth in both segments: distal femur and proximal tibia, was performed in one patient only from the type 4 group.
Surgical procedures in groups.
The mean LLD was 2.3 cm before surgery (range 1.5 to 3.1) and 0.4 cm (range −0.4 to 1.8) at time of hardware removal. The mean amount of LLD correction was 2.2 cm (range 0.5–3.2). Table 3 details segment length discrepancy before surgery and at final follow-up depending on the operated segment. We found out an undercorrection of length discrepancy with residual LLD over 10 mm in 8 of 12 patients (67%) operated after the age of 12 (Figure 2).
Results of guided growth on the operated segment (femur or tibia).

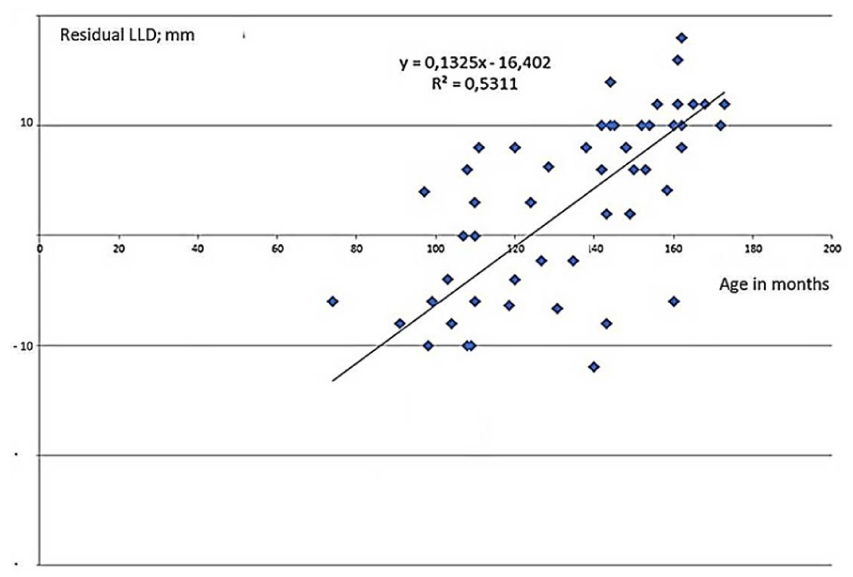
Plot illustrating residual length discrepancy at the last follow-up control depending on the age of surgery.
Gait profile score and spatial-temporal parameters demonstrated a general improvement in gait function (Table 4). There was a decrease in GPS for groups 3 and 4s. We also noticed a significant difference (p = 0.012) between type 2a and type 3 groups in preoperative values of GPS and stride width. Data demonstrated postoperative tendency to prolongation of stance phase on the involved leg.
GPS, selected spatial-temporal parameters.
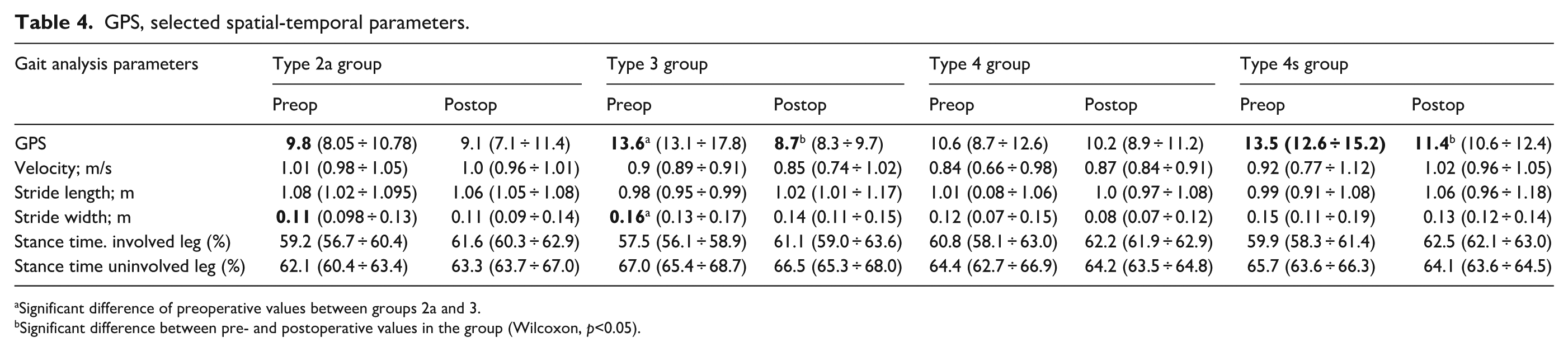
Significant difference of preoperative values between groups 2a and 3.
Significant difference between pre- and postoperative values in the group (Wilcoxon, p<0.05).
Selected kinematic and kinetic parameters before and after surgery are presented in Tables 5 and 6.
Pre- and postoperative values for the involved limb.
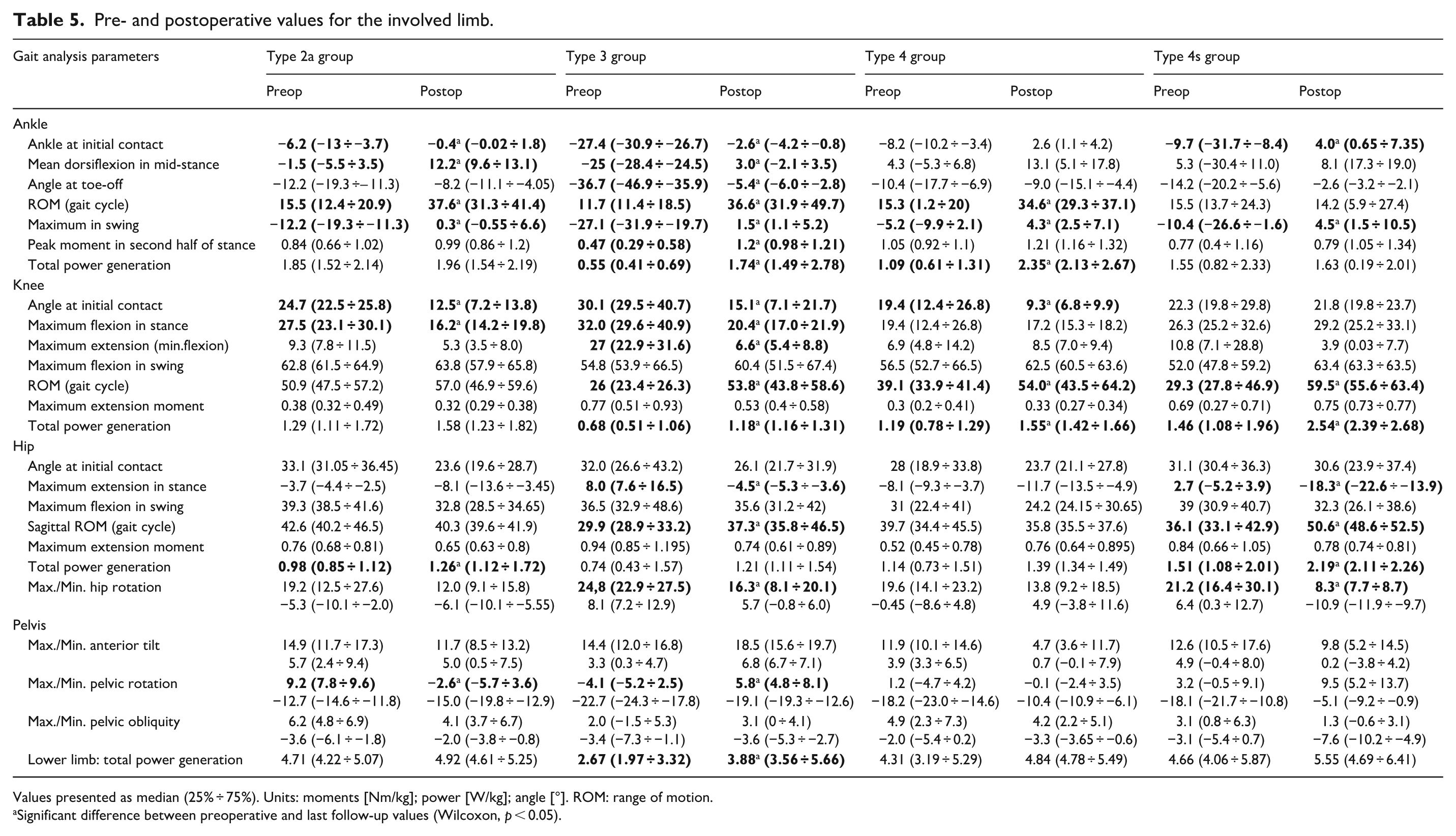
Values presented as median (25% ÷ 75%). Units: moments [Nm/kg]; power [W/kg]; angle [°]. ROM: range of motion.
Significant difference between preoperative and last follow-up values (Wilcoxon, p < 0.05).
Pre- and postoperative values for the
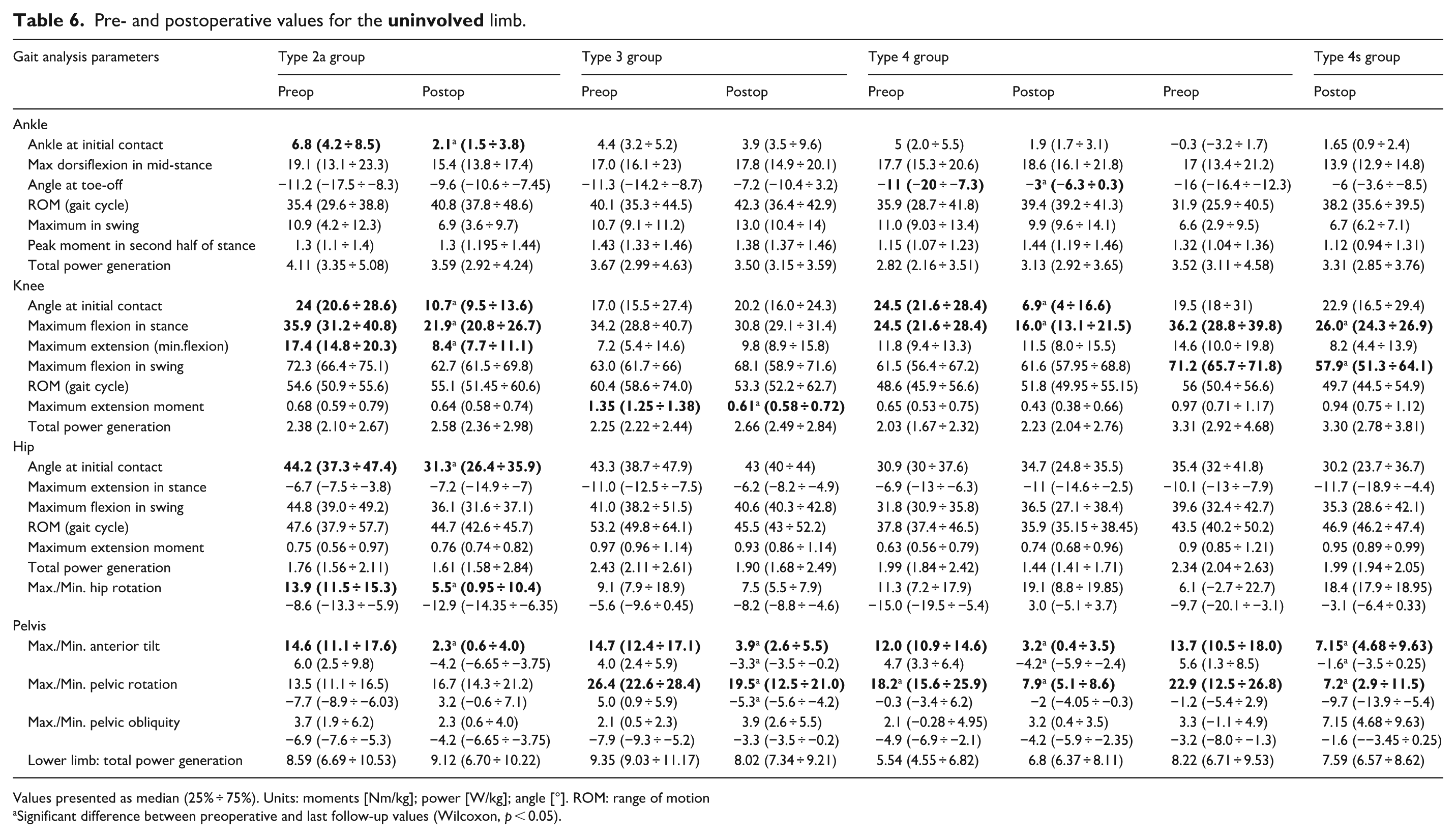
Values presented as median (25% ÷ 75%). Units: moments [Nm/kg]; power [W/kg]; angle [°]. ROM: range of motion
Significant difference between preoperative and last follow-up values (Wilcoxon, p < 0.05).
Involved side
Surgery resulted in a significant increase in dorsiflexion angle at initial contact (groups 2a, 3, 4s), mean dorsiflexion during mid-stance (groups 2a and 3), and maximal dorsiflexion in swing phase. It correlated with an increase in plantar flexion moments except in group 4s where triceps strength remained similar to the preoperative value. It is worth mentioning that postoperative ankle ROM in group 4s is similar to the initial value in comparison to improvements in groups without previous early-age triceps lengthening.
Knee kinematics showed significant improvements in the angle at initial contact in groups 2a, 3 and 4. The maximum flexion in the stance phase significantly decreased in groups 2a and 3. There were no improvements in initial contact and maximum flexion in stance in patients of group 4s. Group 3 patients also demonstrated significant improvement in maximal extension in stance. In other groups, that parameter remained close to reference values in preoperative and postoperative periods. All patients achieved an increase in knee ROM throughout the gait cycle. The significant change in knee kinetics was an increase in the total knee power generation.
In hip and pelvic kinematics, we found no differences in angle at initial contact or in anterior tilt. There were significant improvements in hip sagittal kinematics in groups 3 and 4s. Evident reduction in hip or/and pelvic rotation was observed for all groups. Interestingly, instrumented gait analysis did not reveal significant changes in pelvic obliquity in all groups. Preoperative gait analysis revealed a mild tendency to upward obliquity on the involved side in 9 patients in group 3 and 10 patients in group 4. In other patients, the tendency was to the downward obliquity. Values remained close to reference data at preoperative assessment and last postoperative follow-up control. Total hip power generation increased in groups 2a and 4s. Total power generation demonstrated growth in all groups. It could correspond to improvement in walking ability. However, a significant difference was noticed only for group 3.
Uninvolved side
The ankle joint showed a decrease in the angle at initial contact in all groups. It was significant in group 2a. Angle at push-off showed a reduction from excessive plantar flexion before surgery to postoperative values comparable to the reference group. Most parameters remained comparable to age-matched reference values. Knee kinematics showed stance phase changes after surgery: postoperative values for the angle kinematics decreased significantly in groups 2a, 4 and 4s. Thereby, we found out the regression of the initial compensatory hyper-flexed compensatory mechanism. We noticed a significant reduction in the knee maximum extension moment for group 3. Maximum flexion in swing was comparable to the reference values in the postoperative period in all groups. The tendency for an increase in total power generation in the knee joint was observed.
The average pelvic tilt showed a significant reduction after surgery. The pelvic rotation became significantly lower in groups 2a, 3, 4 and 4s. There were also significant improvements in hip rotation in group 2a. Postoperatively, the values in group 2a only showed a change to normal. However, they remained comparable to reference values in pre- and postoperative period in groups 4 and 4a. We found no significant changes in hip total power generation.
Discussion
The efficacy of single-event multilevel surgery for gait dysfunction on the involved leg in patients with spastic hemiplegia has been established in several studies.7,14,26,27 Although more complex than single-level surgery, it allows greater ability to improve deviations in gait, although both primary and secondary orthopaedic issues should be addressed.10,27 In line with those results, our study found an improvement in the involved leg of children with USCP. Multilevel surgery enabled significant improvements in sagittal kinematics for ankle and knee joints for both stance and swing phases. At the level of the pelvis and hips, improvements in kinematics consisted of a reduction in excessive pelvic and hip rotation. Salazar-Torres et al. 13 recognize coronal plane motion deviation as one of the crucial elements in gait disorder in patients with USCP. In our study, the preoperative assessment data had comparable levels of pelvic obliquity to known matched reference values; we considered this was explained by efficient compensatory mechanisms such as equinus foot posture on the involved leg or flexion of the knee on the other side. We showed that surgical correction of muscle contractures did increase the ROM, most evident in group 3. Recognized classifications of gait deviation in unilateral CP emphasized the dominant role of muscle contractures, impaired ankle dorsiflexion and ‘stiff knee’ in type 3 gait deviation.8,10 In our study, an increase in ROM was obviously associated with a rise in plantar flexion moment and power generation for each joint and also overall for the whole involved limb. On the other hand, we found no changes in ankle kinetic parameters in patients of group 4s (undergone early-age isolated Achillis tendon lengthening or myofibrotenotomies). Pilloni et al. 28 demonstrated the negative impact of isolated tendo achillis lengthening on the kinematics of plantar-flexion knee extension coupling: weakened peak ankle power at push-off results in an increase in knee flexion and could be a predictor of crouch gait pattern. In addition, percutaneous myofibrotenotomies of the triceps 29 weaken plantar flexor function, which leads to crouch gait over the long term in spastic diplegia patients. 30 We noticed in our group 4s that knee flexion at initial contact and maximum knee flexion in stance increased in comparison to patients without previous triceps surgery. We speculate that an increase in knee flexion subsequent to weakness of the triceps could be an early indicator of crouch gait, even in hemiplegic patients requiring appropriate rehabilitation.
Lower LLD in children with USCP contributes to gait deviation observed in many studies: increased pelvic obliquity and pelvic retraction, 13 spinal deviation, 31 slower velocity and shorter stride length, 18 excessive stance phase hip and knee flexion and dorsiflexion at the ankle joint,11,20 reduced knee ROM on the uninvolved side, 20 increased knee extension moments and excessive absorbed ankle power in the first phase of stance on the uninvolved side,17,19 significantly longer stance phase on the uninvolved side, than in healthy children. 17 Furthermore, Joo and Miller observed valgus foot deformity of the uninvolved foot. 19 LLD has been recognized as one of the causes of equinus deformity recurrence after tendo achillis lengthening in hemiplegic patients.15,16 The recurrence rate can be up to 22.2% 15 to 62.5% among patients with hemiplegia. 16
Eek et al. demonstrated gait deviation related to LLD in barefoot conditions if shortening was more than or equal to 1.0 cm. 18 Deviation of gait pattern became particularly marked if LLD was greater than 1.5 cm. 20 Riad et al. investigated the degree of LLD in the lower limb in adolescents and young adults with hemiplegic CP using MRI. They found that the primary site of the length difference was distal in the lower limb (tibia, talus and calcaneus). 32 This was consistent with our own findings, hence why guided growth was applied to the proximal tibia more often than the distal femur.
LLD is common, and treatment can be considered in order to improve walking ability. 20 Zonta et al. demonstrated that increasing length discrepancy can be associated with a reduced degree of social activity. 33
There are several approaches to the equalization treatment of lower limbs. An orthotic correction can allow compensation while the child is actually wearing it.3,18 This method, however, has not been shown to provide an improvement in either spinal kinematics or prevention of equinus deformity recurrence.16,21,31 In an initial case series, Jahmani et al. demonstrated the efficiency of closed femoral-shortening osteotomy in terms of equalization. Only one patient represented hemiplegic palsy. 22 No gait analysis was performed to evaluate the functional outcome. Saraph et al. performed lengthening surgery on the shorter side using a monolateral external fixator. 11 Surgery included simultaneous femoral rotational deformity correction and some soft-tissue procedures. This short series of 11 patients revealed a significant increase in spatial-temporal parameters on the involved side. On the affected leg, all the kinematic values showed changes from reference normal values. This study has an important limitation: only the clinical examination method was used for postoperative assessments of LLD.
Bone lengthening on the affected side of CP children is well known to be challenging to the point of being almost contraindicated. As well as being technically demanding, whatever the technique, there are inherent risks, such as infection and temporary loss of walking ability. 34 Lengthening a bone in the context of a pre-existing muscle contracture (previously operated on or otherwise) is fraught with danger in terms of worsening contracture and even joint dislocation. It should be carried out with extreme caution by experienced limb reconstruction surgeons with consideration to spanning the affected joints with hardware or at least orthotics.
Allen et al. suggested considering guided growth of the uninvolved leg in children. 20 Consideration of this method should be given due to its advantages: less demanding surgical technique, patient convenience and regaining of growth after eight-plate removal.35–37
There are some controversies about the effectiveness of guided growth using eight plates for temporary epiphysiodesis in LLD correction. Lauge-Pedersen and Hägglund 38 in a short and interrupted series demonstrated no significant reduction of growth by eight plates at the site of the proximal tibia. However, a consecutive cohort study of Demirel et al. 39 revealed high effectiveness of the eight-plates technique in LLD in a series of patients with a mean age of 9 years where the mean longitudinal correction rate was 0.48 mm per month, accompanied by low complication rates. Although guided growth is a safe and reliable procedure, its effectiveness decreases in older children. It was demonstrated in the series (mean age 13.6 years) of Borbas et al. 40 where definitive percutaneous epiphysiodesis was preferable to guided growth with tension plates.
Corradin et al. reported results of epiphysiodesis on the uninvolved leg using the eight-plate technique or Blount’s staples in 10 patients. Guided growth procedure was always associated with several procedures on the involved foot and/or ankle joint. 21 We can state that this publication is the first to evaluate the results of multilevel surgery, including the guided growth procedure in children with USCP. However, in the study, only the Edinburgh visual gait score was applied for gait assessment. Significant improvements in kinematics in both hemiplegic and uninvolved legs were noticed. Corradin et al. demonstrated good outcomes of guided growth in terms of length equalization. The mean amount of correction was 2.3 cm. It was inferior to the expected 1 (2.8 cm). 21 The advanced age of patients in the series (12.7 years) could cause an undercorrection of LLD. Our findings of significant (over 1 cm) LLD undercorrection in patients undergoing a guided growth procedure at age greater than 12 are consistent with those outcomes. 21
The role of bone age evaluation during monitoring of LLD in hemiplegic children remains controversial. Erickson and Loder demonstrated no difference between chronologic and bone age for patients with right or left hemiplegia and found no necessity to obtain radiographs of both hands in children with USCP to determine bone age. 41 In contrast to that opinion, Lee et al. 42 emphasized that the bone age of the affected side is delayed in comparison to the unaffected one. In addition to this ambiguity, Feldkamp et al. found no increase in LLD after the age of 8 in children with USCP. 43 After all, taking into consideration the reversibility of guided growth after plate removal, we believe that the timing of epiphysiodesis surgery before the chronological age of 12 can be considered appropriate. Thus, in this patient group, we believe that bone age evaluation is not necessary.
Regarding the results of gait analysis in the uninvolved leg, our outcomes are aligned with results published by Saraph et al. and Corradin et al.11,21 There was a significant reduction in compensatory hyperflexed kinematic mechanisms. Interestingly, a significant decrease in excessive ROM in the transverse plan was also observed postoperatively. The values of pelvic obliquity close to the reference data at the preoperative assessment can be explained by compensatory mechanisms, whereas at the last postoperative follow-up, the values of this parameter, which were insignificantly different from the reference data, were determined by the corrected or reduced leg length discrepancy (LLD) and the improved range of motion (ROM) in the joints. Instrumented gait analysis revealed a tendency towards a decrease in total hip power generation and an increase in total knee power generation, while the total leg power generation did not change.
In the literature, the target residual LLD is estimated to range between 0.5 and 1.5 cm, taking into consideration the ankle dorsiflexion impairment on the involved side.21,39 However, as it was mentioned in the study of Eek et al., significant gait deviations were observed while LLD was 1.0 cm or more. 18 We speculate that an LLD of less than 1 cm ensures that the involved limb takes more weight, which stretches the calf complex more effectively every step, thus preventing equinus recurrence. In addition, our study demonstrated that mid-swing ankle dorsiflexion improved postoperatively, which could reflect an increase in dorsiflexion strength and selective motor control. Stance time on the involved leg tended to become longer postoperatively. Postoperative values of mid-swing dorsiflexion in our study are comparable to reference data but inferior to the averaged results in the series by Saraph et al. 11 Thus, we advise aiming for a target value of less than 1cm as the residual leg length discrepancy by the end of growth. However, we recognise that, as always, this should be on a case-by-case basis; an equal leg length might be detrimental to some patients, such as those with an uncontrolled foot drop.
The limitations of this study include the retrospective character of the analysis used to assess outcomes of guided growth performed simultaneously with multilevel surgery on the involved leg in children with USCP. Thus, we are not able to collect and study additional variables, such as the Functional Mobility Scale, the Gross Motor Function Measure, spine kinematics and quality of life assessment. These measures would complement gait analysis. Also, it is important to note that less than 50% of our patients were followed until skeletal maturity. There is only one article demonstrating no increase in LLD after the age of 8 years. 43 Nevertheless, a reassessment of LLD at skeletal maturity would be necessary for our cohort, even Zonta et al. 33 found an association between functional use of the extremities and improved limb growth. Thus, we have to follow all our patients until growth plate closure to evaluate post-maturity lower LLD with the same methods. Because of restrictions access to the gait analysis laboratory for some patients, we have no simultaneous comparative series of patients undergoing multilevel surgery without length equalization surgery. Thus, the specific effects of guided growth on the uninvolved leg cannot be definitively isolated. After all, guided growth of only one segment contributing most to length discrepancy can be criticized as it does not allow for directly comparing our results with the outcomes in the series of Corradin et al. 21 Furthermore, we may speculate that in some patients with advanced age a bisegmental (distal femur and proximal tibia) guided growth would be more beneficial for LLD correction. In our study, we used age 12 as an advised cut-off for the guided growth technique but other considerations such as gender, hormonal imbalance and race should also be taken into account on an individual basis for future prospective multicentre studies. Future work aimed to compare matched groups of hemiplegic patients with and without guided growth should be performed. Criteria of assessment could include radiological measures, gait analysis as well as functional outcome measures providing insights into how biomechanical improvements translate into potential clinical gains.
Conclusion
Multilevel orthopaedic surgery on the involved leg in children with USCP, accompanied by a guided growth procedure on the uninvolved leg, represents a reliable method ensuring significant improvements in the kinematics and kinetics on both sides. The main changes on the involved leg consist of kinematic improvements in sagittal and transverse planes and an increase in total power generation during joint motions. On the uninvolved side, a reduction of secondary compensatory mechanisms and related high-energy cost of movements are observed. We suggest performing a guided growth procedure before the age of 12 years to avoid length discrepancy undercorrection, having an LLD no more than 1 cm as a target at the end of growth. Isolated tendo achillis lengthenings or triceps myofibrotomies performed at an early age result in biomechanical alterations and represent negative conditions for plantar flexion strength development in the long term.
Footnotes
Contributions
Dmitry Popkov (0000-0002-8996-867X) conceived of the presented idea, performed all surgeries and supervised the findings of this work. Mamedov Ulvi (ORCID 0009-0008-0266-6515) developed the theory. Patrick Foster (Scopus: 7201517406; ORCID 0009-0005-4515-4219) developed the theory, reanalyzed the data and compared with literature, Gatamov Orkhan (ORCID 0009-0005-4244-5774) and Tomov Akhmed (ORCID 0009-0001-2981-7722) enabled follow-up, collected and analyzed the data. Dolganova Tamara (ORCID 0000-0002-0117-3451) performed gait analysis studies and verified the analytical methods. The final version of the manuscript has been reviewed and approved for publication by all the authors.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethical statement
This research was conducted ethically in accordance with the World Medical Association Declaration of Helsinki. The study was approved by the local ethic committee of the Ilizarov National Medical Research Center for Traumatology and Orthopaedics (Ministry of Health, Russian Federation on the 15 May 2018. Protocol Number 2(57). All patients enrolled in the study or their representatives provided oral and written informed consent.
Data availability
The data of this study are available from the corresponding author upon request.