
Abstract
Purpose:
To describe foot abnormalities in proximal femoral focal deficiency and their correlation to the severity.
Methods:
Eighty-nine extremities in 87 patients were evaluated between 1996 and 2020 clinically and radiologically. Fibula length, ankle shape, tarsal coalitions, and the number of foot rays were recorded. Extremities with proximal femoral focal deficiency were classified according to Pappas and divided into severe (classes II and V), medium severe (classes III and IV), and mild groups (classes VII, VIII, and IX).
Results:
The fibula was short in 89% and absent in 11% of cases. An absent fibula occurred mostly in severe class III and only in 4% of mild grades (statistically significant, p = 0.004). The valgus ankle joint prevailed in 82% of cases. Spherical ankle joints (18% of cases) were associated in all cases with a tarsal coalition. Tarsal coalitions occurred in 14.6% and were present in all classes except class IV. Five ray feet were found in 83% of cases, four ray feet were found in 16%, and three ray feet in one extremity. Reduction in the number of foot rays occurred more commonly in association with fibular aplasia (30%).
Conclusions:
Abnormalities of the fibula and ankle joint represent a constant part of proximal femoral focal deficiency, whereas tarsal coalition and a reduction of foot rays do not. The severity of foot abnormalities does not correlate to the severity of proximal femoral focal deficiency but does with fibular aplasia.
Keywords
Introduction
Congenital short femur or proximal femoral focal deficiency (PFFD) represents a very rare and complex deformity. The basic characterization of PFFD encompasses aplasia, hypoplasia, or pseudarthrosis of the femur; hypoplasia of the lateral femoral condyle; aplasia, or hypoplasia of the cruciate ligaments of the knee1 –3; aplasia or hypoplasia of the fibula and shortening of the tibia (Figure 1); and variable abnormalities of the foot. The abnormalities in the foot include valgus or spherical ankle joint (ball and socket joint), tarsal coalition, and reduction of foot rays.4 –6 PFFD is included in the group of nonhereditary diseases with congenital lower limb deficiency which is described as a postaxial limb hypoplasia. 7 From these descriptions and further literature review8,9 as well as our own long-term experience in patients with PFFD, it is not clear, how often the foot in PFFD is morphologically changed and if there is a correlation between the severity of foot abnormalities and the severity of the PFFD. This study aimed to describe the incidence of foot abnormalities in PFFD and the correlation of the abnormalities of the foot with the class (severity) of PFFD. Our hypotheses were as follows: (1) all cases of PFFD have associated morphological abnormalities of the foot and (2) the severity of the morphological abnormalities of the foot correlates with the classification and severity of the PFFD.
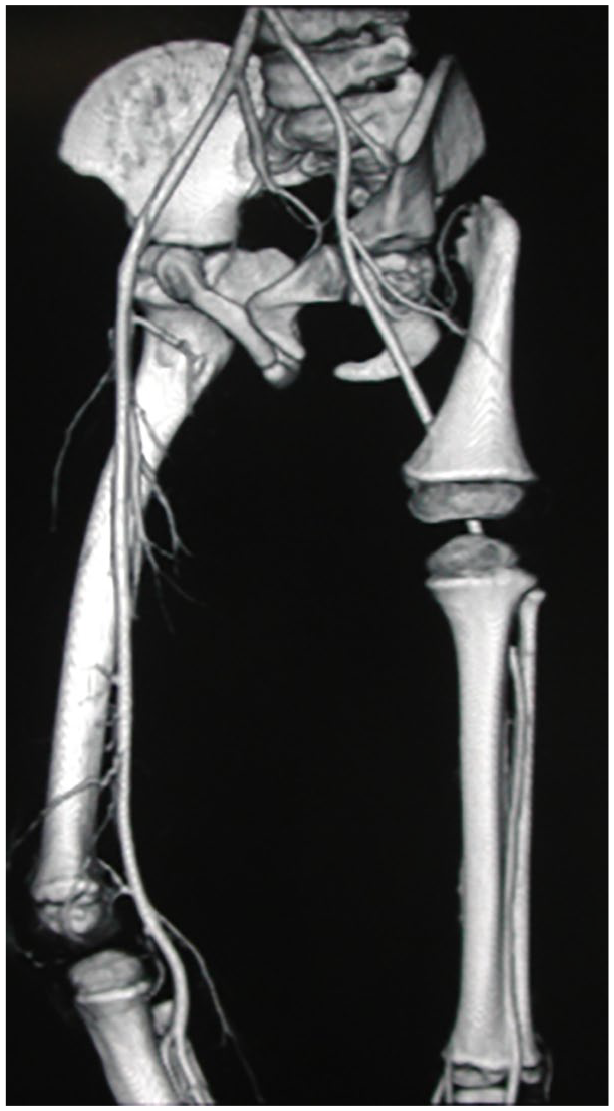
CT angiography of PFFD type IV left, boy, age 7 years. Pseudarthrosis and shortening of the femur, valgus knee, shortening of the fibula, and reduction of the diameter of the femoral artery are seen.
Materials and methods
This is a single-institution retrospective study of a cohort of 87 patients (89 extremities) with PFFD evaluated between 1996 and 2020. The patients were examined by four pediatric orthopedic surgeons. Plain radiographs and computed tomography (CT) scans were interpreted by independent radiologists. The clinical assessment included: the length of extremities and morphology of the knee, ankle, and foot. The radiological assessment included standardized anterior and lateral plain radiographs of both extremities from the hip to the foot. CT scans and 3D reconstructions were obtained and evaluated since 2002 and were used for more accurate evaluation of tarsal coalitions. Length of the femur and tibia were measured, and the morphology of the fibula, ankle, and foot was assessed and compared to the contralateral healthy side. The Pappas classification of PFFD 10 was applied because our institution has used this classification for previous studies. In this classification, there are nine classes (Figure 2); class I represents the absence of the femur, classes II (Aitken D), III (Aitken C), and IV (Aitken B) represent the involvement of the proximal femur and hips. Classes V and VI represent the involvement of the knee. Classes VII (Aitken A), VIII, and IX are less severe, with a nearly normal hip joint.
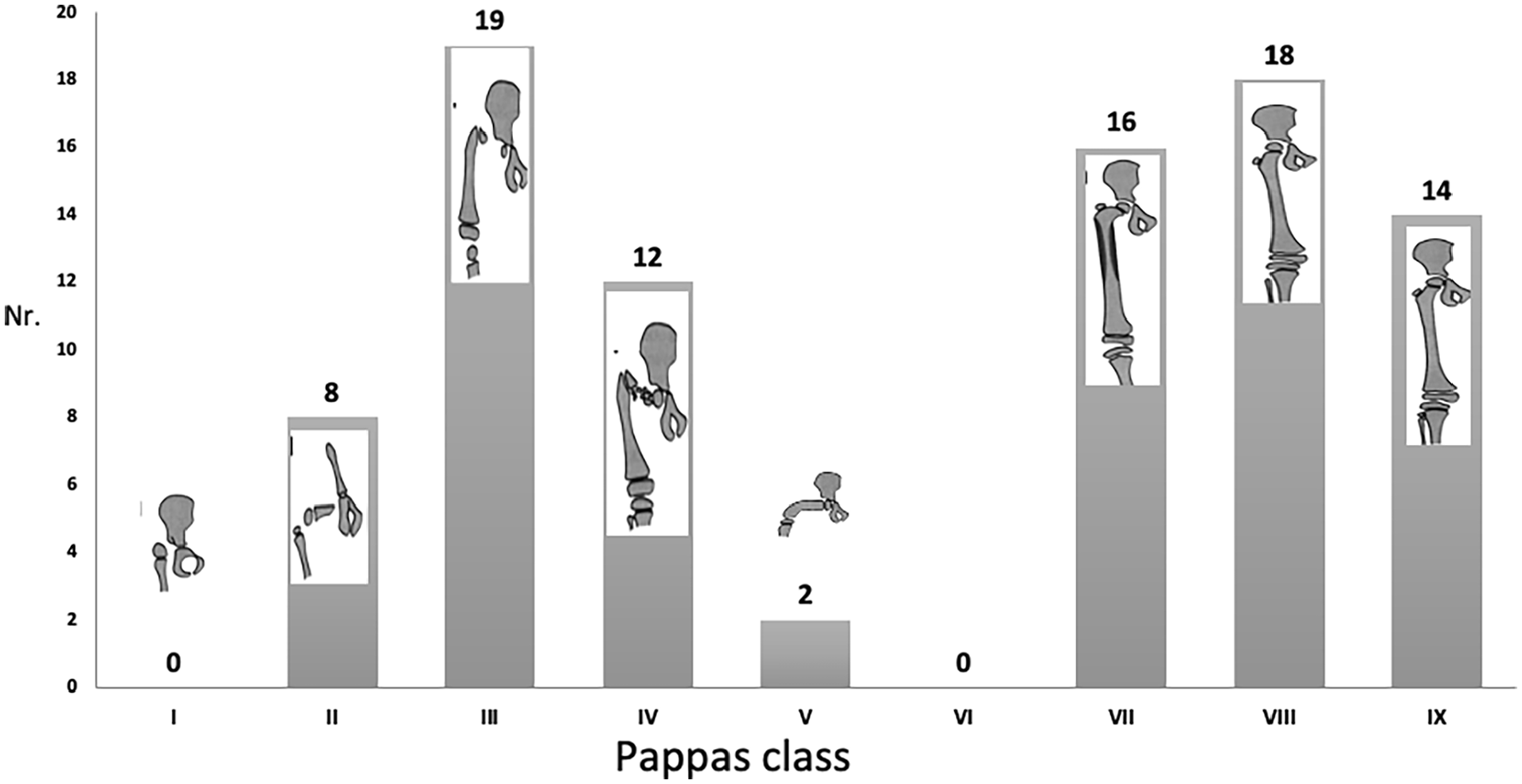
Diagram of the distribution of PFFD in relation to Pappas classes.
We modified the classification system of fibular hemimelia published by Stanitski and Stanitski to categorize changes in the fibula, ankle, and foot. Plain AP and lateral radiographs of the distal lower leg were interpreted as follows: (1) fibular length (type I-normal length—fibular physis is below the level of trochlea tali; type II—shortening, when the fibular physis is at the level or proximal to the trochlea tali; type III—fibular absence); (2) shape of the ankle joint: H—horizontal, when lateral distal tibial angle—LDTA 11 is in a range between 86° and 92°; V—valgus, when LDTA is under 86°; S—spherical (“ball and socket,” describing the round convex shape of talar dome and concave distal tibial epiphysis); (3) the presence of tarsal coalition: (plus—present, minus—not present); and the number of foot rays: 1–5. In addition, all short fibulae were evaluated proximally as well as distally and fibula length was described as follows: distal shortening; both proximal and distal shortening; distal shortening; and proximal fibular aplasia.
The differences between PFFD groups regarding fibular aplasia, the shape of the ankle joint, reduction of foot rays, and the presence of tarsal coalitions were statistically evaluated using a G-test (G-quadrate test). The value 0.05 was chosen as the significance level. For statistical evaluation, it was necessary to simplify the categories to three grades according to the severity of classes of PFFD: severe (classes II and V), medium severity (classes III and IV), and mild (classes VII, VIII, and IX).
Results
The cohort of patients includes 38 boys and 49 girls (with 89 involved limbs) ranging in age from 2 to 16 years (median age 6.4 years, STD 4.2 years) at the time of examination of the feet. The distribution of PFFD in the Pappas classification includes the following: 8 class II, 19 class III, 12 class IV, 2 class V, 16 class VII, 18 class VIII, and 14 class IX (Figure 2). The right side was involved more frequently than the left (49 versus 40 extremities). In two patients, there was bilateral involvement (class IV right and class VII left in one patient and bilateral class VIII in the other). Femoral shortening ranged between 2.5 and 26 cm. The tibia was shortened in all patients between 0.5 and 5 cm in comparison to the contralateral side.
Fibular length
A short fibula was present in 79 extremities (89%) with the absence of the fibula occurring in 10 extremities (11%). Applying the fibular involvement to the Pappas classification (Figure 3) revealed fibular shortening in all classes. The absence of the fibula occurred in 30% of severe grades of PFFD (classes II and V); 16% in medium severe grades (classes III and IV); and in 4% of the less severe grades (classes VII, VIII, and IX). The differences are statistically significant (p = 0.004).
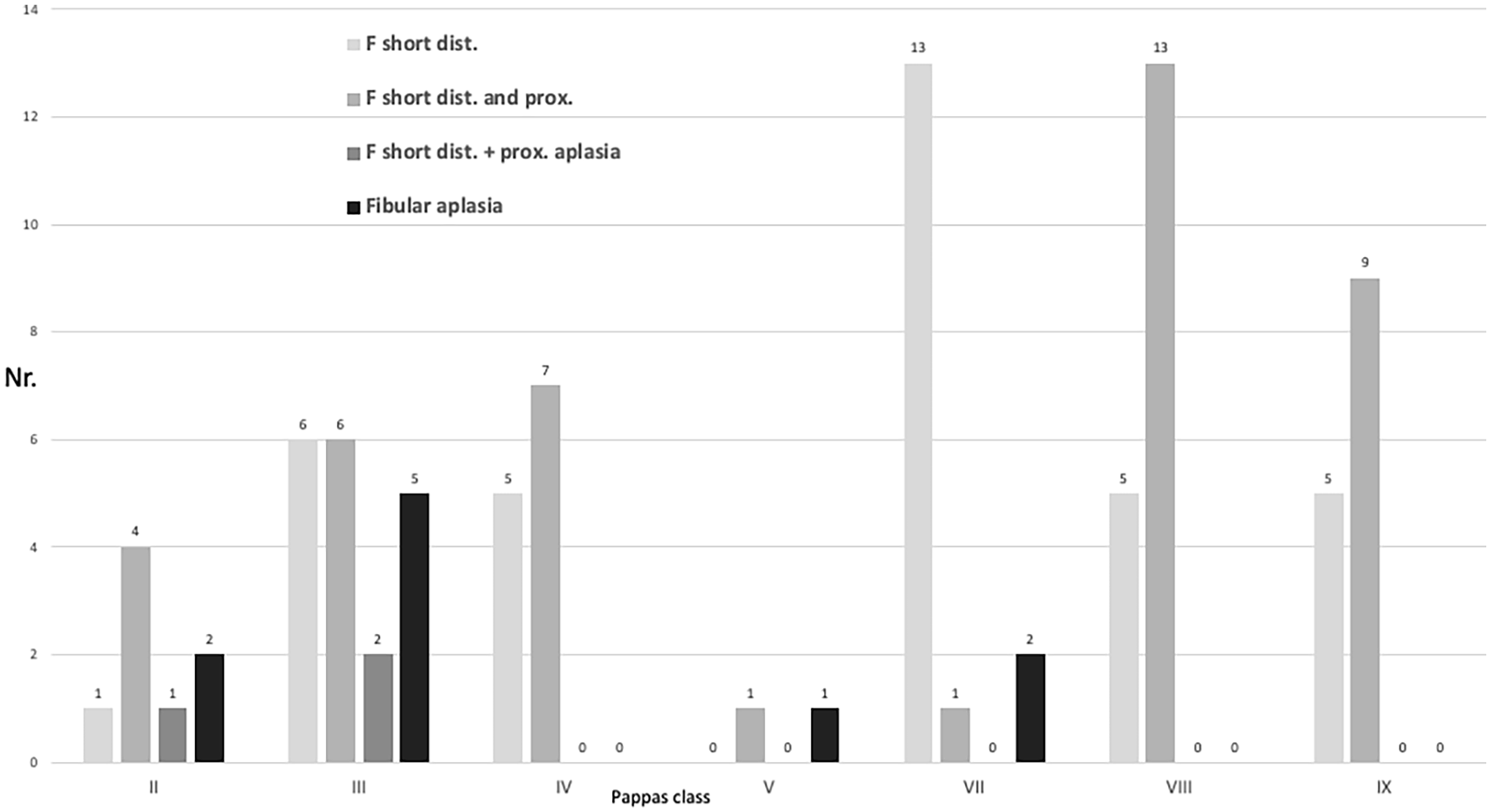
Diagram of the fibula length/deficiency in relation to Pappas classes. F short dist.: distal shortening; F short dist. and prox.: both proximal and distal shortening; F short dist.+prox. aplasia: distal shortening and proximal fibular aplasia; fibular aplasia: complete absence of fibula.
In all extremities, the distal fibula was shorter. In 41 extremities, in addition to the distal shortening, the proximal fibula was developed but shorter in comparison to the contralateral side. In three extremities, the proximal fibula was not developed.
Shape of the ankle joint
The ankle joint was valgus in 73 extremities (82%, Figure 4a), and spherical in 16 extremities (18%, Figure 4b). The shape of the ankle joint in relation to the Pappas classes is shown in Figure 5. The valgus shape prevailed in all classes while the spherical ankle occurred more commonly in mild grades of PFFD (23%) compared to 10% of severe grades. This difference is statistically significant (p = 0.002). A spherical ankle joint was associated with eight cases of fibular aplasia. In two cases of fibular aplasia, the ankle joint displayed a valgus deformity (Figure 6).

Plain radiographs of ankle joint, A-P view in two extremities with PFFD. Fibular shortening and valgus ankle joint (a) and spherical ankle joint (b) are apparent.
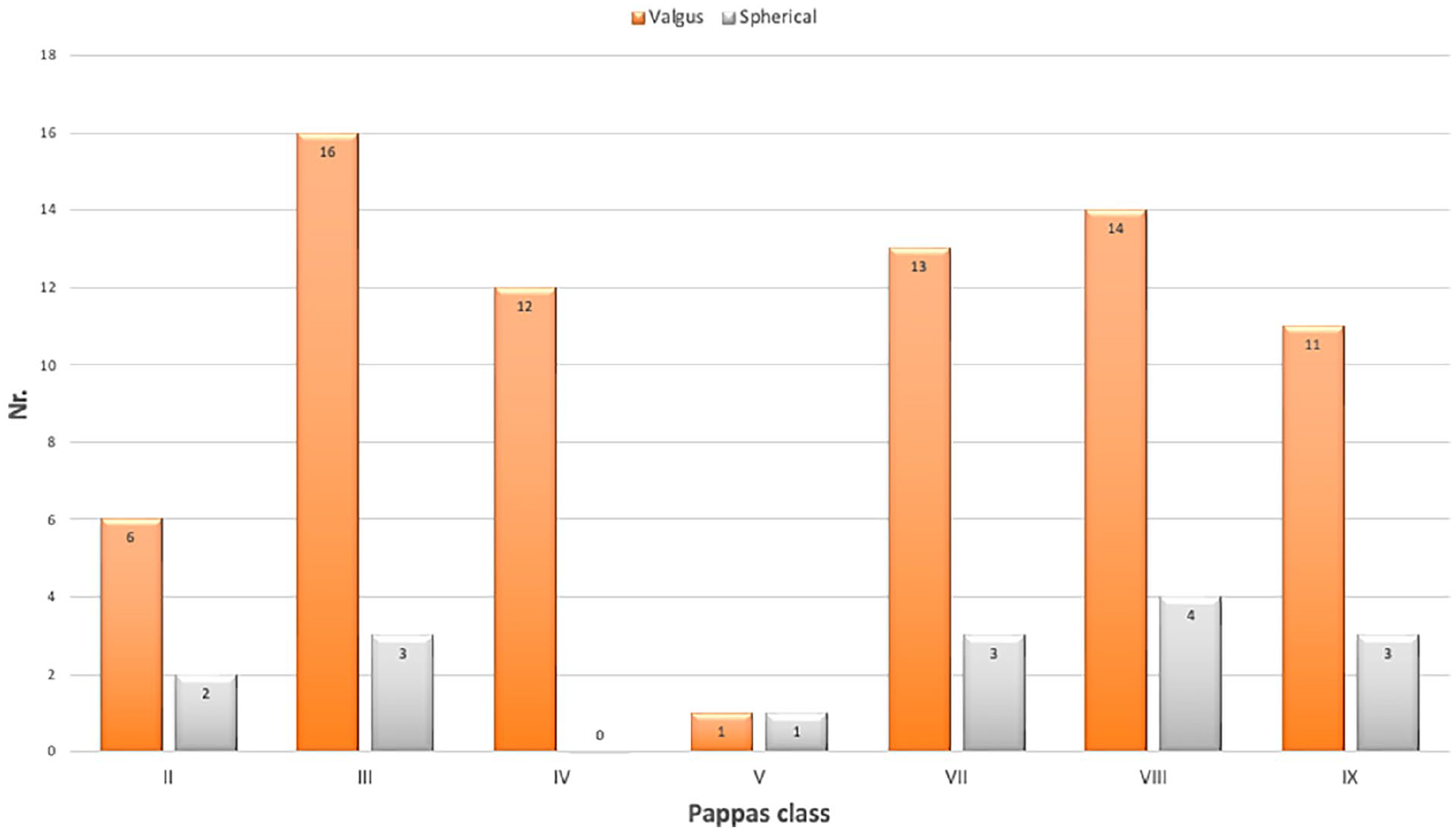
Diagram of the shape of the ankle joint (valgus, spherical) in relation to Pappas classes.

Plain radiograph, A-P view of ankle and foot in PFFD Pappas class III right, girl, age 17 years. Valgus shape of the ankle in fibular aplasia.
Tarsal coalition
Tarsal coalitions were identified in 13 extremities (14,6%, Figure 7). They were all associated with a spherical ankle joint if the fibula was present. In four of the five extremities with a tarsal coalition and fibular aplasia, the ankle joint also had a spherical shape. A talocalcaneal coalition was identified in the 13 extremities and was present in all Pappas classes except class IV (Figure 8). Additional coalitions were identified including the talonavicular joint (seven extremities), calcaneocuboid joint (three extremities), and cuneo-metatarsal joint (two extremities). Coalitions were identified in 5 of the 10 extremities with fibular aplasia (50%) and in 8 of the 79 extremities with fibular hypoplasia (10%). Six extremities with a reduction in foot rays (40%) had a tarsal coalition.

Plain radiograph, lateral view of ankle and foot in PFFD Pappas class VII, girl, 15 years. Multiple tarsal coalitions and shortening of the fibula are present.
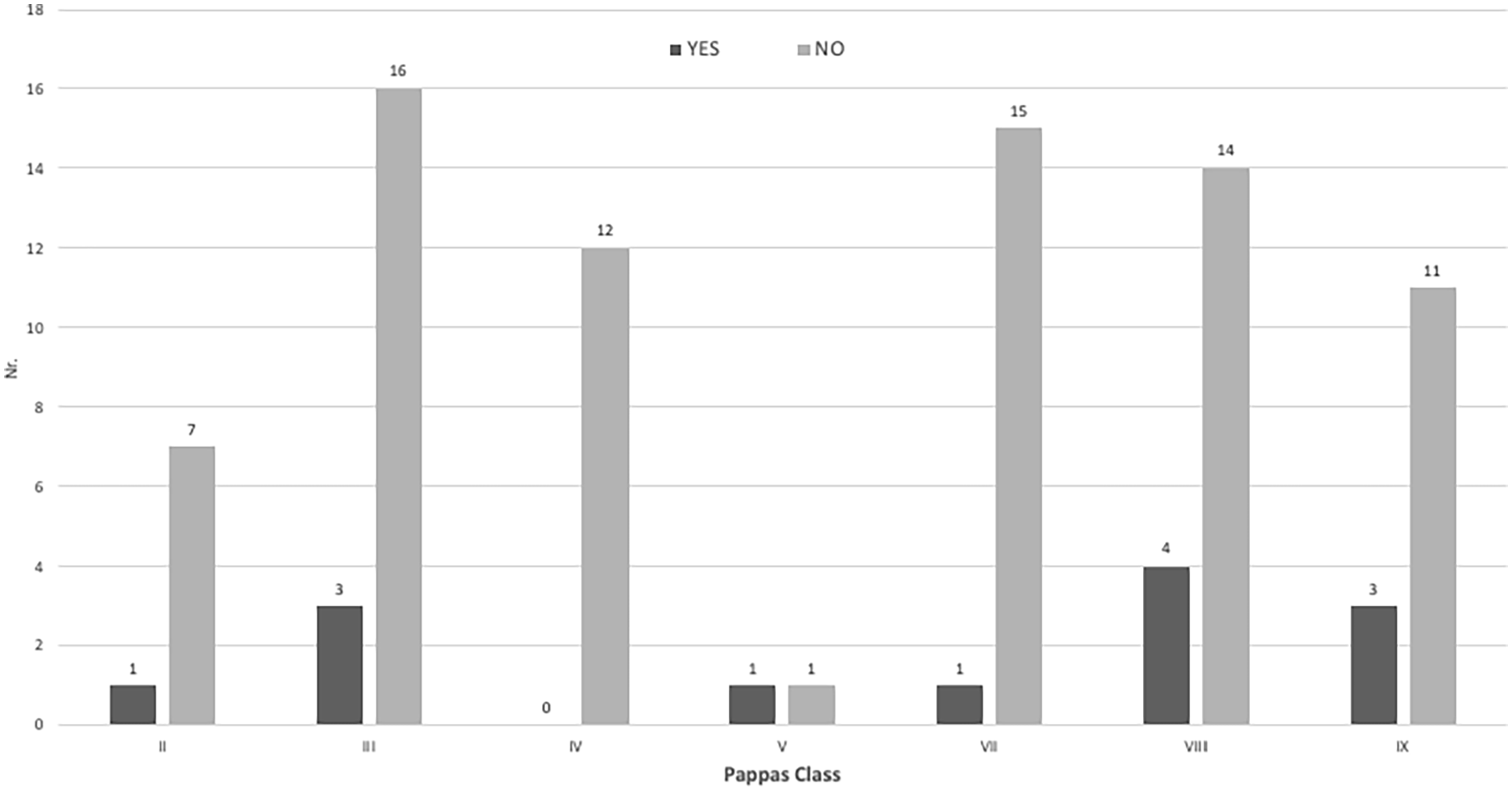
Diagram of the tarsal coalitions (yes—present, no—not present) in relation to Pappas classes.
Number of foot rays
Seventy-four extremities (83%) had a normal number of foot rays. A reduction of foot rays was found in 15 extremities: four ray feet in 14 extremities (16%, Figure 9) and three ray feet in one extremity (1%). The number of foot rays in connection to the Pappas class is displayed in Figure 10. A reduction in foot rays was present in all classes except class IV. It was most common in class VIII (7 of 18 patients). Three ray feet were found only once (class III). A reduction in the number of foot rays was not significant when stratifying to the class of PFFD, except class VIII. In class VIII, four ray feet were found in 39% of extremities, which is statistically significant (p = 0.01) (Figure 10).

Plain radiograph, A-P view of the left foot in PFFD Pappas class IV. Reduction of the foot rays (metatarsals), duplication of the fourth toe, and changes in tarsal bones are apparent.
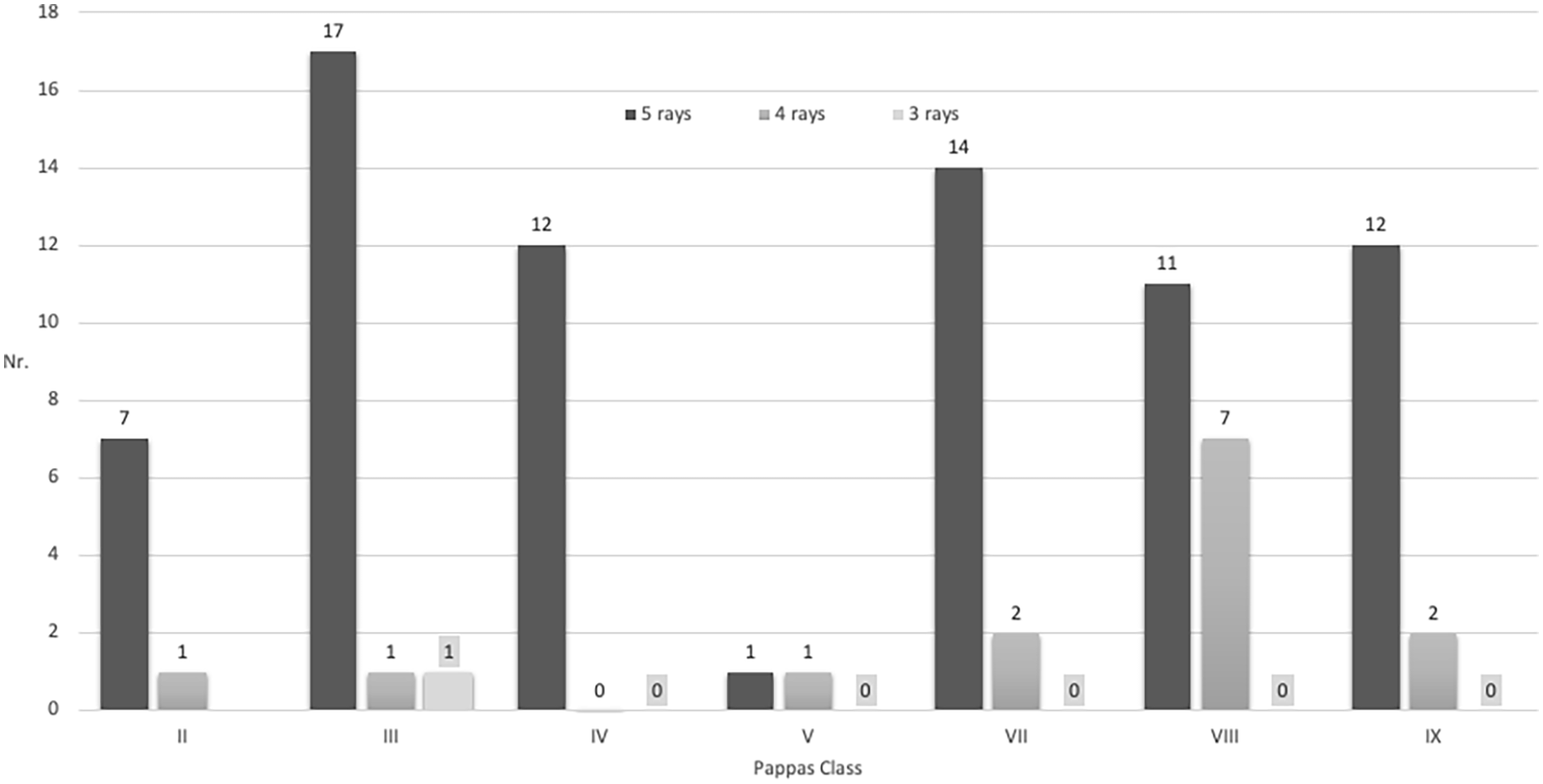
Diagram of the number of foot rays in relation to Pappas classes.
Length of the fibula and reduction of foot rays
In 11 of the 79 extremities with a hypoplastic fibula (13.9%), there was a reduction in foot rays; whereas in cases of fibular aplasia, 3 of 10 extremities had a reduction in foot rays (30%). The difference is not significant due to the low number of observations in the fibular aplasia category.
Discussion
Our first hypothesis was confirmed because all patients with PFFD had morphological abnormalities of the foot. Shortening or aplasia of the fibula and abnormalities of the ankle joint were found in all extremities, but the tarsal coalition and a reduction of foot rays were not a constant occurrence in PFFD.
Our second hypothesis was not confirmed. The severity of the morphological abnormalities of the foot did not directly correlate with the type or severity of the PFFD except when associated with fibular aplasia (classes II and V). A clear correlation was seen between fibular aplasia and tarsal coalition.
There are only a few papers in the literature with analysis of the foot abnormalities in PFFD.8,12 Most studies are oriented to fibular hemimelia.4,7,13 We found constant involvement of the foot in our cohort of patients, whereas Koman et al., 12 in a similar cohort of patients, described ipsilateral fibular hemimelia and valgus shape of the foot in 45% of patients. Bronfen et al. 8 described abnormal feet and fibular aplasia in 51% of 51 patients with PFFD. In comparison, we found more abnormalities in the feet, because we focused on all abnormalities. Grogan et al. 4 described a different rate of the talocalcaneal coalition in patients with fibular hemimelia or PFFD or both because they used different diagnostic methodologies. The true prevalence of tarsal coalition is unknown because this can be done only at the time of skeletal maturity. Talocalcaneal coalition prevailed, but talonavicular coalition (seven patients), calcaneocuboid coalition (three patients), and cuneo-metatarsal coalition (two patients) were also seen in our study. According to our findings, we cannot support the currently used theories. (1) Theory of lateral ray deficiencies, 13 when reduction of the lateral foot rays is the consequence of global lateral limb developmental abnormality, including lateral distal femoral hypoplasia, fibular hypo/aplasia, ankle deformity and tarsal coalition and (2) theory of Hootnick et al. 14 and Reys et al. 15 that abnormal development of the vascular system is associated with the musculoskeletal defects seen in congenital fibular deficiency and other lower extremity long bone deficiencies.
Our study has the following limitations. This is a retrospective study encompassing a long period of time involving a rare condition in a relatively small geographic area with a population of 10 million inhabitants. The second limitation is that the study was performed by physicians from a single institution, so the effects of institutional bias may be possible. A third limitation is the wide range of age at the evaluation so radiographs, CT scans, and magnetic resonance imaging of the feet were not always provided after skeletal maturity and the shortening of the extremity and foot deformities in skeletally immature patients could be not definitive. But ankle and foot changes at the time of evaluation were always compared to the contralateral healthy side. It can lead also to the possible presence of non-osseous talocalcaneal coalitions in youth patients. A talocalcaneal coalition can be determined only at the time of skeletal maturity 4 and not all patients in the study were skeletally mature. Concerning the wide range of age at evaluation, we included in the cohort all patients with clear signs of PFFD independently of age because of a very rare condition in a small geographic area, and knowing the fact that some patients will not continue in the treatment and follow-up in our institution.
Conclusions
In contrast to literature reports, abnormalities of the fibula and ankle joint represent a constant part of PFFD, while tarsal coalition and a reduction of foot rays do not.
The severity of the foot abnormalities generally does not correlate to the severity of PFFD, except when associated with fibular aplasia. There was a tendency for more severe involvement of the foot in severe classes of PFFD (II and V). Reconstructive management of PFFD including length discrepancy must take into account the abnormalities presenting in the ankle joint and foot.
Supplemental Material
sj-pdf-1-cho-10.1177_18632521241301942 – Supplemental material for Ankle and foot deformities and malformations in proximal femoral focal deficiency
Supplemental material, sj-pdf-1-cho-10.1177_18632521241301942 for Ankle and foot deformities and malformations in proximal femoral focal deficiency by Jiri Chomiak, Monika Frydrychova, Martin Ošťádal and Pavel Dungl in Journal of Children’s Orthopaedics
Footnotes
Author contributions
Jiri Chomiak: Preparation of manuscript. Monika Frydrychova: Data collection. Martin Ošťádal: Data collection. Pavel Dungl: Data collection and correction of the manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed consent
All participants (parents) gave informed consent to the publishing of this paper.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.