
Abstract
Purpose
The purpose of this case series study is to report on the intermediate-term outcomes following a femoral varus derotational osteotomy (FVDO) performed in conjunction with a Dega osteotomy (DO) in management of hip instability in Down syndrome (DS) patients.
Methods
Ten hips in seven children with DS suffering from hip dislocation were included. All patients included in this study had hip dislocation in the habitual phase and painless mobile hip to full abduction. All patients were firstly subjected to FVDO. An additional DO was added if intraoperative assessment demonstrated posterior instability. The mean age at time of surgery was 5.6 years (3 to 7). There were three male and four female patients. All patients were followed up after two years with a mean follow-up of 3.27 years (2 to 5). All operations were performed by the first author.
Results
There was improvement of neck shaft angles (130° to 175°, median = 160° preoperatively, to 120° to 140°, median =130° postoperatively). The Shenton line was restored in all our cases. There was also improved percentage of the femoral head uncovered by the lateral wall of the acetabulum (25° to 100° with median = 45° preoperatively, to 0° to 15° with median = 5° postoperatively) and improved posterior acetabular coverage, which was assessed by CT.
Conclusion
FVDO combined with DO without capsulorrhaphy is efficient in the management of hip instability in DS, as it corrects hip biomechanics and increases posterior acetabular coverage.
Level of Evidence
IV - retrospective case series
Introduction
Down syndrome (DS) or Trisomy 21 is one of the most common non-lethal chromosomal disorders with an incidence of one in 795 live births. Life expectancy of a child born with DS has increased up to 55 years with hip instability reported to occur in up to 7.0% of patients during childhood. (1) As the life expectancy of patients with DS increases, the incidence of painful arthritis in adulthood is also increased, so early intervention in hip dysplasia is of great value. 1
In contrast to patients with idiopathic developmental dysplasia of the hip, patients with DS do not characteristically exhibit hip dysplasia before walking age. Capsular insufficiency, ligamentous laxity and hypotonia are important contributors to hip instability in DS. Over time, secondary hip dysplasia may occur with subsequent acetabular retroversion. The combination of soft tissue and bony factors may eventually result in symptomatic hip subluxation or dislocation, with subsequent gait disturbance and risk of degenerative arthritis in the long run. 2
The bony hip structure in DS is characterized by a deeper and more horizontal acetabulum as well as decreased acetabular anteversion and increased femoral anteversion which increases hip stability; however, capsular laxity, hypermobility and increased external rotation appear to play a large role in hip joint instability, including dislocation. Dysplastic changes occur over time, including posterior acetabular deficiency, which can be identified with the aid of 3D CT.1,3–5
The natural history of the hip in Trisomy 21 can be classified into one of four overlapping groups, that of initial phase (0 to two years), dislocation phase (two to eight years), subluxation phase (more than eight years), and fixed phase (> 15 years). 6 The hip dislocation phase is subdivided into acute and habitual dislocation. Children in the acute dislocation group often present with sudden onset of limp or refusal to walk. Their hips are dislocated but can be reduced closed with the patient under anesthesia. Children in the habitual dislocation phase have hips that dislocate without trauma and spontaneously reduce, starting at walking age. 6
There is controversy concerning the methods of treatment of habitual hip dislocation in DS patients, a lack of consensus between conservative or surgical intervention, and a debate about the surgical method of treatment as posterior capsular plication alone, periacetabular osteotomy alone, 7 femoral osteotomy alone 8 or combined femoral and innominate pelvic osteotomy. 9
Literature citations on management of hip instability in children with DS are too inadequate to allow for establishment of valid and reliable treatment guidelines. The objective of this study is to investigate the intermediate-term clinicoradiologic response of children with DS to bony hip reconstruction using a combined femoral varus derotation osteotomy (FVDO) and Dega pelvic osteotomy (DO).
Patients and Methods
Ten hips in seven children with DS suffering from habitual non-traumatic hip dislocation were firstly subjected to FVDO. An additional DO was added if intraoperative assessment demonstrated posterior instability. All operations were performed by A. S. Aly.
All patients included in this study had hip dislocation in the habitual phase, and painless mobile hip to full abduction. Patients with fixed hip dislocation, stiff painful hip and adolescent with arthritic changes were excluded from this study.
The chief complaint noted by parents of all our cases on presentation was spontaneous dislocation of their hips during manipulative physiotherapy and/or activities of daily life. On physical examination, the hips of all our cases were reproducibly dislocated, with 90° of hip flexion in either neutral or adduction positions, and were easily reduced with abduction and extension with palpable, visible or audible click.
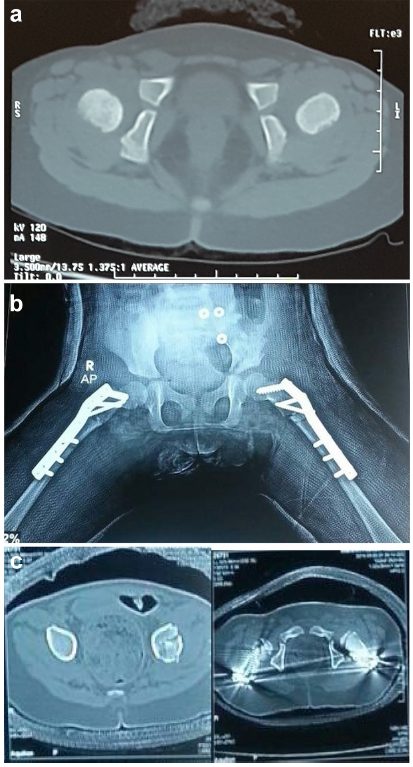
Radiographs were done for all patients in the form of plain pelvis radiographs showing both hips anteroposterior in neutral rotation, frog lateral and abduction with internal rotation views. We recorded the neck shaft angles, integrity of Shenton's line, head migration index 10 and lateral subluxation of femoral heads (Fig. 1). Patients received CT scans of the pelvis and both hips in all cuts. We assessed acetabular dysplasia of the hip joints as a deficient posterior acetabular wall (Fig. 2a).
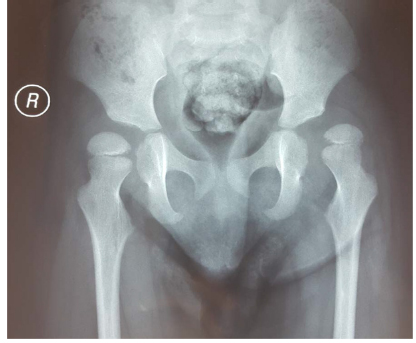
Preoperative radiograph revealed bilateral coxa valga, broken Shenton lines and lateral sublaxation of both femoral heads which was more on the left side with a migration index= 100% compared with a migration index= 50% on the right side.
(
Surgical technique
The stage in which our patients received their surgical treatment was the habitual dislocation phase. FVDO to correct coxa valga and to improve head coverage by the acetabulum, with the judicious use of derotation and acetabular osteotomies to improve posterior coverage of femoral heads, were performed.
Particular attention to the use of derotation is needed so as not to cause posterior instability in the face of a retroverted acetabulum. Femoral derotation osteotomy of 10° to 15° was done followed by examination of stability to avoid posterior dislocation of the hip.
The femoral osteotomies were fixed by contoured narrow or small dynamic compression plates. Hip stability was improved after femoral osteotomy, and no dislocation occurred till neutral and 90° flexion. However, posterior dislocation was still present with adduction beyond neutral and 90° flexion of hips with minimal posteriorly directed force, so DOs 11 of the acetabulum were added to increase the posterior coverage, using iliac crest bone grafts which were placed more posterior in osteotomy sites (Figs 2b and 2c).
Again, hip stability was tested intraoperatively and posterior dislocation no longer occurred after DOs in either neutral or adduction positions. In all our cases, DO was required.
In these cases, we did not carry out capsulorrhaphy 6 as its laxity is of a genetic predisposition which make it liable to fail and stretch again in postoperative course.
Postoperative protocol
Postoperative immobilization with a hip Spica cast is recommended for eight weeks to allow bony union. 6
To combat the vitamin D deficiency that is endemic in our country due to a lack of sun exposure, all patients were on a prophylactic dose of vitamin D in the form of oral cholecalciferol drops (ten drops per day for three months) to prevent disuse osteopenia and pathological fractures after removal of the Spica.
Radiographs were done which revealed improved neck shaft angles, increased femoral heads coverage and restored Shenton lines (Fig. 2b).
The parents and physiotherapist reported no hip dislocation during manipulation postoperatively, and all hip joints were stable on physical examination with no dislocations occurring when the hip joints were at full adduction and 90° of flexion (Fig. 3b).

(
Results
The mean age at time of surgery was 5.6 years (3 to 7). There were three male and four female patients. Affected sides were two left, two right and three bilateral. All patients were followed-up over two years with a mean of 3.27 years (2 to 5).
At the final follow-up, none of the parents reported habitual hip dislocation of their children. On physical examination, the hip joint stability was noticed postoperatively, with no dislocations occurring when the hip joints were at full adduction and 90° of flexion compared with preoperative instability.
We compared pre- and postoperative plain pelvis radiographs for all patients showing both hips anteroposterior, frog lateral and abduction with internal rotation views and CT in all cuts. In all cases, we found increased neck shaft angles preoperatively (130° to 175°, median =160°), broken Shenton line and lateral subluxation of femoral heads by head migration index (measured by percentage of femoral head uncovered by lateral wall of acetabulum, 25° to 100°, median = 45°). Acetabular dysplasia of the hip joints was noticed as a deficient posterior acetabular wall by CT scanogram in all our cases (Table 1).
Pre- and postoperative radiographic findings
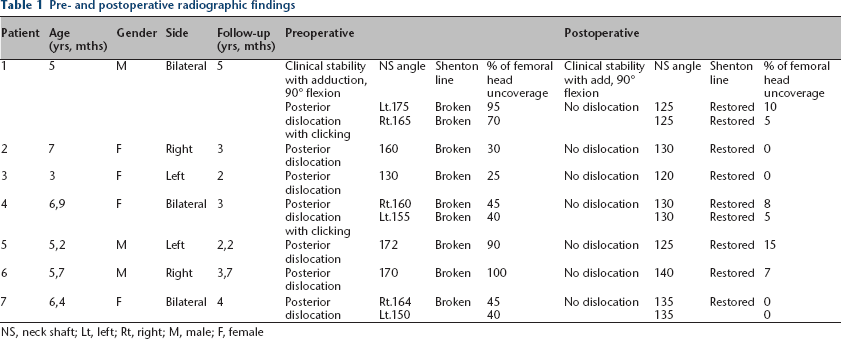
NS, neck shaft; Lt, left; Rt, right; M, male; F, female
Postoperative radiographs were done, revealing improved neck shaft angles (120° to 140°, median = 130°), increased femoral heads coverage (0° to 15°, median =5°) and restored Shenton lines in all our cases (Table 1).
Discussion
Hip dislocations in DS are considered a soft-tissue problem (capsular laxity with excessive range of movement), 12 as well as a bony problem (coxa valga, excessive femoral anteversion and deficient posterior acetabular wall).7,13
Aprin et al 9 performed Salter pelvic osteotomy, femoral varus osteotomy and capsular plication singularly or in combination in ten hip joints (six patients). Follow-up averaged 49 months. Four redislocations were reported, and these results demonstrated that neither conservative nor surgical treatments have provided consistent outcomes.
According to Woolf et al 3 in 2003, the direction of hip dislocation is almost always posterior, and is produced by flexion, adduction and internal rotation. The authors pointed out that the anterolateral-covering Salter osteotomy would at best not improve the posterior stability and at worst worsen the instability. In both cases reported in Woolf et al, 3 the instability was rectified with a modified Pemberton procedure in which the graft was placed posteriorly to help improve the posterior acetabular coverage.
Imagamma et al 7 described a case report of a 12-year-old girl with DS with nontraumatic habitual hip dislocation. Her hip joint was associated with acetabular dysplasia and hypoplasia of the posterior acetabular wall. Although conservative therapy was initially performed, no effects were observed. Rotational acetabular osteotomy and capsular plication were performed to reconstruct the posterior acetabular wall. No postoperative redislocation occurred, and the treatment effects were favourably sustained for two years.
Capsular plication was equally disappointing with a 50% failure rate whether combined with bony surgery or not. Those who underwent femoral osteotomy alone fared little better, with more redislocations. 6
According to Kelley and Wedge, 6 bony surgery is always required in habitual instability in DS patients. In the unlikely event that the hip remains unstable after an optimally positioned femoral osteotomy, then the addition of an acetabular reorienting procedure could be considered.
Our patients underwent femoral varus osteotomies to correct coxa valga with minimal femoral derotation osteotomies added. DOs of the acetabulum were added to increase the posterior coverage. Hip stability was tested intraoperatively, which was improved with no posterior hip dislocation. We did not need to perform capsular plication. No postoperative redislocation has occurred, and the hip joints remained stable for a median follow-up after three years (2 to 5) Fig. 3a).
The only reported complications were limb length discrepancy in unilateral cases who underwent varus osteotomies; this was partially improved by remodelling of the femoral shaft with growth. We had no cases of redislocation through follow-up. The drawback of this study is the limited number of patients; a much larger number of patients with a long-term follow-up period will be included in further studies.
Conclusion
In this study, we found that FVDO combined with acetabular DO without capsulorraphy is efficient in the management of hip instability in Trisomy 21, as it corrects biomechanics of the hip joint with an increase of posterior acetabular coverage.
DO of the acetabulum was added to increase the posterior coverage using iliac crest bone grafts which were placed more posterior in osteotomy sites.
Footnotes
No benefits in any form have been received or will be received from a commercial party related directly or indirectly to the subject of this article.
None declared.