
Abstract
Purpose:
Radial neck fractures in children are rare, representing less than 1% of all pediatric fractures. While conservative treatments are often sufficient, displaced fractures may require closed or open reduction. The Metaizeau technique is widely accepted for closed reduction and internal fixation. This study aims to assess the long-term functional and radiological outcomes of this technique and identify any complications that may arise.
Methods:
This retrospective study analyzed 22 pediatric patients treated with the Metaizeau technique for proximal radius fractures between 2005 and 2018. Data on demographics, preoperative radiographs, and postoperative complications were reviewed. Outcomes were evaluated using radiographic and functional measures, including grip strength, the Mayo elbow performance score (MEPS), and the Tibone and Stolz classification.
Results:
The mean age at the time of injury was 9.9 years, with a mean follow-up period of 139 months (range: 72–213 months). Patients were classified as Judet type 3 (n = 9), type 4a (n = 9), or type 4b (n = 4). The functional outcomes showed a mean MEPS score of 99 (range: 90–100), with 86% of patients achieving excellent results according to the Tibone and Stolz classification. Excellent outcomes were recorded in 100% of type 3, 77.7% of type 4a, and 75% of type 4b cases. Documented complications included one case of radioulnar synostosis and two cases of heterotopic ossification.
Conclusions:
The Metaizeau technique represents an efficacious treatment option for pediatric radial neck fractures, offering favorable long-term functional and radiological outcomes with a low complication rate. Long-term follow-up data further support the reliability of this technique.
Types of Studies:
Level IV.
Keywords
Introduction
Pediatric elbow injuries are relatively common, but radial neck fractures, although they constitute 1% of all pediatric fractures, have an important place in pediatric elbow injuries.1,2 These injuries predominantly affect children aged 4–14 years, with the highest incidence occurring between ages 8 and 10.3,4 The typical mechanism involves a valgus force causing impaction at the radiocapitellar joint, usually from a fall onto an outstretched hand while the forearm is supinated and the elbow extended. 5
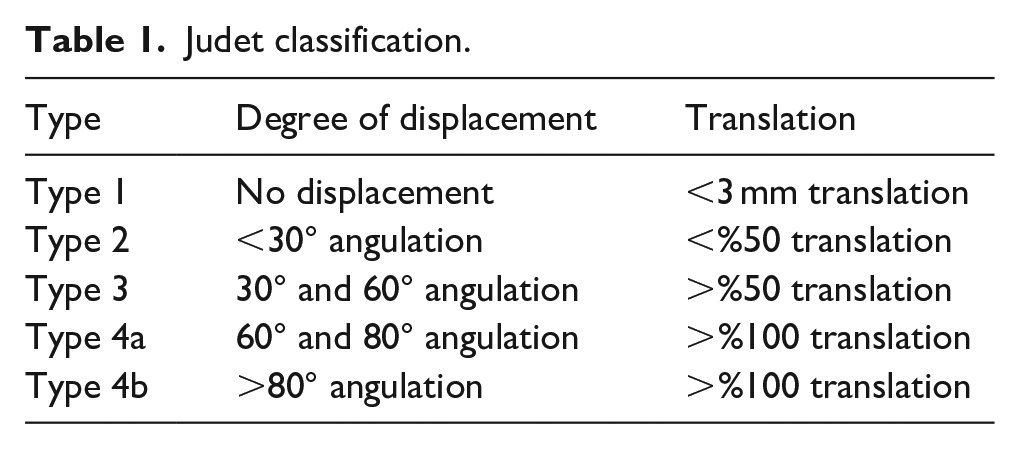
Radial neck fractures are categorized anatomically into two types: metaphyseal fractures, which are more common, and epiphyseal separation fractures. The treatment approach depends on the fracture’s angulation, displacement, and patient age. Mildly angulated fractures are often managed with immobilization, while more displaced fractures may require closed or open reduction.6,7 When there is significant displacement, conservative management may be inadequate, making surgical intervention necessary. In cases of displaced radial neck fractures with angulation exceeding 30°, surgical intervention is recommended. This is consistent with the classification of Judet type 3 and 4 fractures.8,9
A variety of surgical techniques have been employed, including percutaneous joystick reduction with Kirschner wires (K-wires) and open reduction, with or without internal fixation. However, the Metaizeau technique, introduced in 1980, popularized the use of elastic stable intramedullary nailing for stabilization.6,7 The Metaizeau technique supports bone healing through minimally invasive fixation, avoiding direct interference with the physis and reducing the risk of growth disturbances while promoting early functional recovery.
While previous research has largely focused on short- to mid-term outcomes or comparing different techniques, this study seeks to evaluate the long-term functional and radiological results of the Metaizeau technique for treating pediatric radial neck fractures.
Materials and methods
This retrospective study was approved by the institutional ethics review board (approval number: 4487) and conducted in accordance with the Declaration of Helsinki. Prior to their inclusion in the study, all patients or their guardians provided informed consent. The medical records of patients presenting with radial neck fractures between 2005 and 2018 were reviewed retrospectively.
The study included patients who were 15 years of age or younger at the time of injury, had a minimum follow-up period of 5 years, and had both initial and follow-up radiological imaging available for evaluation. Patients with incomplete data, polytrauma, or an age greater than 15 years were excluded, as were patients lacking adequate radiological images. Radiographs were classified according to the Judet classification (Table 1), and only patients classified as Judet type 3 or 4 were included, while types 1 and 2 were excluded from the analysis (Figure 1). Patients treated with a method other than the Metaizeau technique (open or direct percutaneous reduction, etc.) were excluded from the study.
Judet classification.
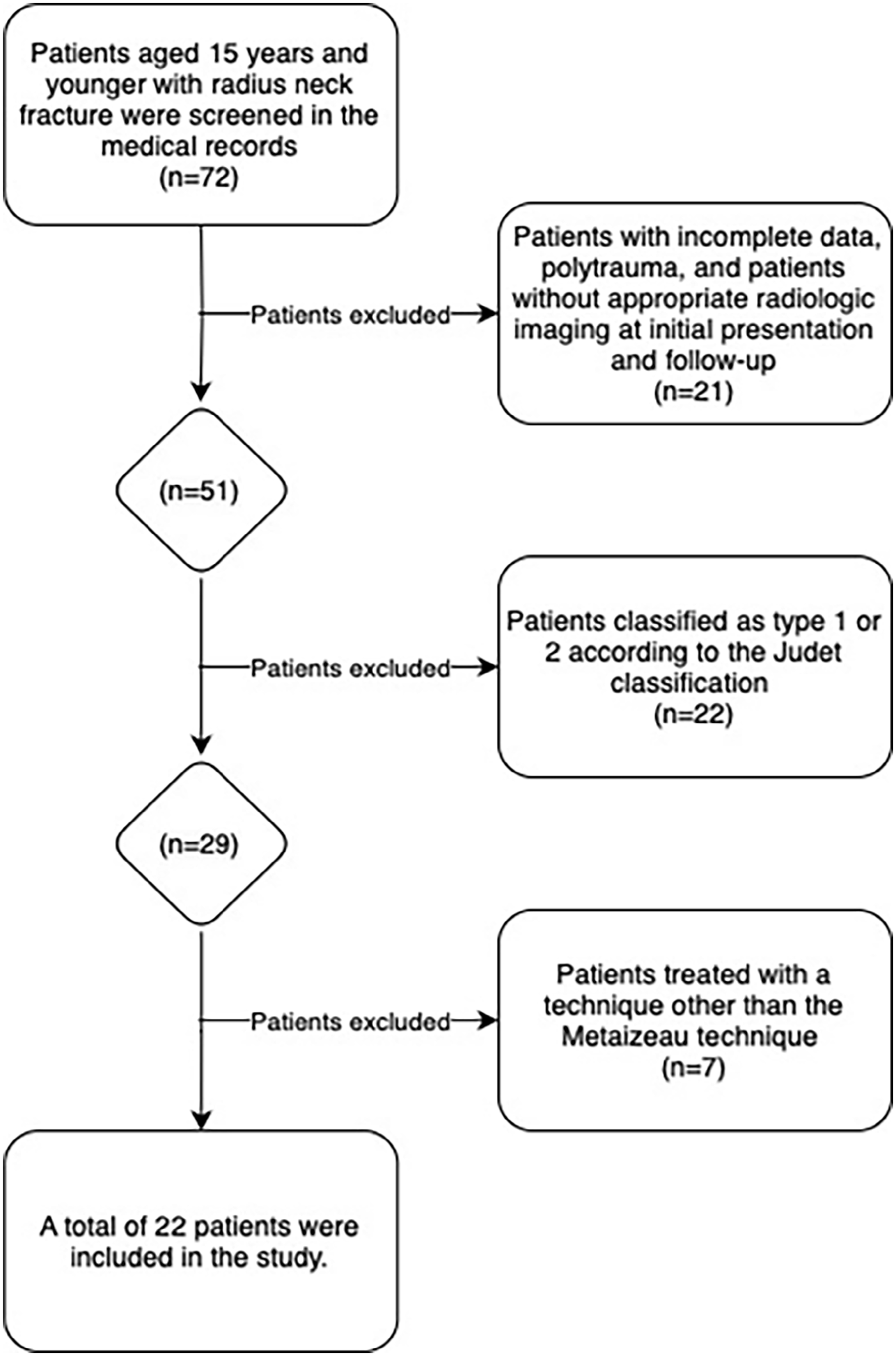
Study flow chart of patients screened, excluded, and included.
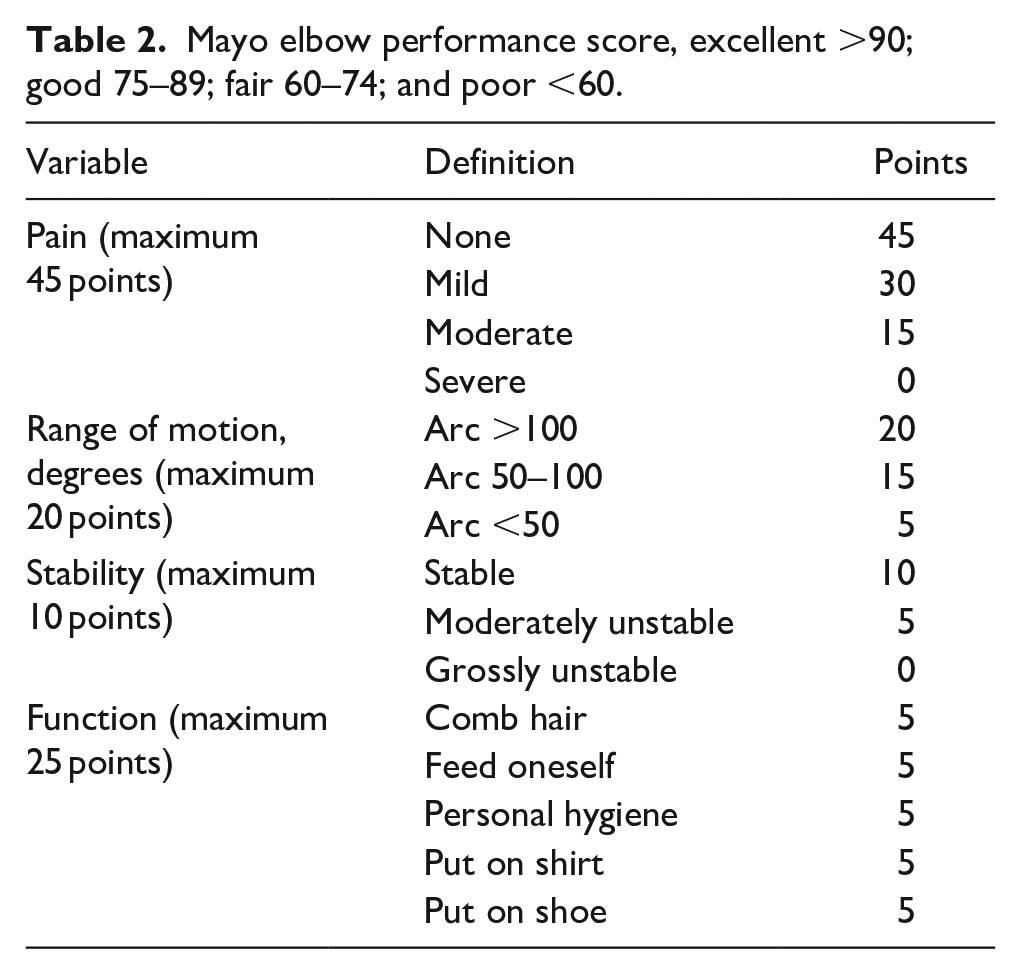
Demographic data, including age, gender, side of injury, and follow-up duration, were collected and analyzed. Preoperative and postoperative radiographs and functional status at final follow-up were evaluated (Figures 2 and 3). Functional outcomes were measured using a range of motion and grip strength, as well as the Mayo elbow performance score (MEPS) and Tibone and Stolz scores (Tables 2 and 3). Postoperative complications were also documented.

Functional images of our 22-year-old patient, who underwent surgery at the age of 10 for a radii neck fracture treated with the Metaizeau technique.

Preoperative and postoperative radiographs of our patient with radii neck fracture treated with the Metaizeau technique.
Mayo elbow performance score, excellent >90; good 75–89; fair 60–74; and poor <60.
Tibone and Stoltz classification for functional results of radial neck fractures.
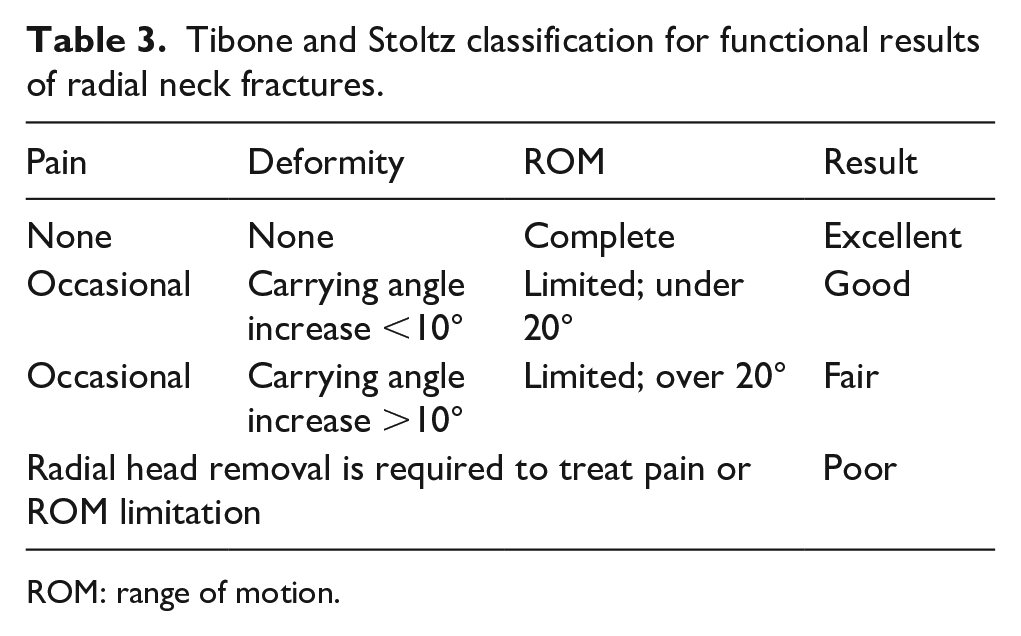
ROM: range of motion.
Descriptive data, including preoperative radiographic findings and postoperative functional outcomes, were expressed as numbers, percentages, means, and ranges (minimum–maximum). All radiological evaluations were performed by orthopedic surgeons and classified using the Judet system. Statistical analysis was conducted using SPSS software version 29 (IBM Corporation, New York, NY, USA).
Results
A total of 22 patients were included in the study. All surgeries were performed with closed reduction using the Metaizeau technique. In all patients, intramedullary K-wire was removed in an average of 6–8 weeks. The mean age at the time of injury was 9.9 years (range: 5–15 years), with the cohort comprising 13 males and 9 females. The majority of patients (64%) sustained fractures on the left elbow, while 36% had right elbow fractures. The average angulation of the fractures was 62.13° (range: 35°–86°). All patients underwent surgery within the first 24 h using the Metaizeau technique. 9 The average follow-up duration was 139 months (range: 72–213).
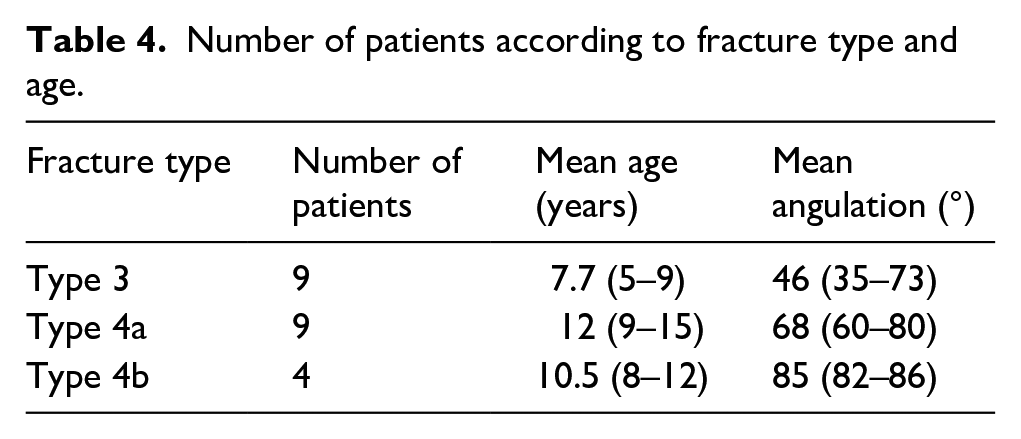
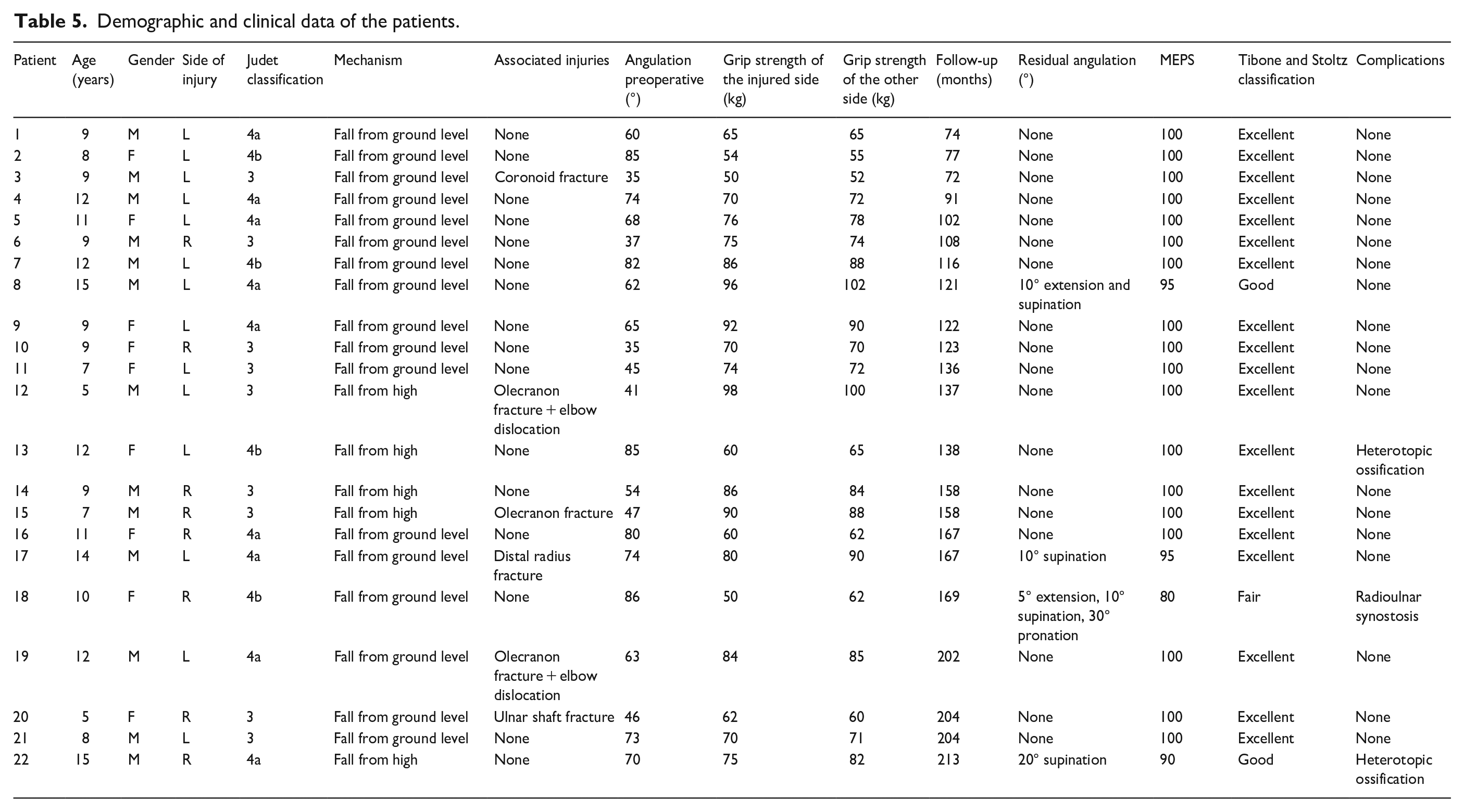
Table 4 presents a summary of the number of patients, mean age, and mean fracture angles of fracture types according to the Judet classification. When evaluating all patients, regardless of demographic characteristics or fracture type, the functional assessment yielded a mean MEPS of 98 (range: 80–100). According to the Tibone and Stolz classification, 86% of patients achieved excellent results. The average grip strength on the injured side was 73.8 kg (range: 50–98), while on the uninjured side, it was 75.8 kg (range: 52–102). Only four patients experienced movement limitations, specifically in extension, supination, and pronation, with maximum limitations of 10° in extension and supination, and 30° in pronation (Table 5).
Number of patients according to fracture type and age.
Demographic and clinical data of the patients.
The most common complication observed was heterotopic ossification in two patients, while one patient developed radioulnar synostosis (Figure 4). It is noteworthy that none of the complications frequently cited in the literature, such as posterior interosseous nerve palsy, avascular necrosis of the radial head, malunion, or nonunion, were observed in this study. Patients who experienced complications were all classified as Judet type 4a or type 4b and exhibited lower functional outcomes. The patient with radioulnar synostosis had 5° of extension, 10° of supination, and 30° of pronation limitation, and his MEPS was 80. One patient with heterotopic ossification had 20° of supination limitation, and his MEPS was 90, while no limitation was observed in the other patient, and his MEPS was 100.
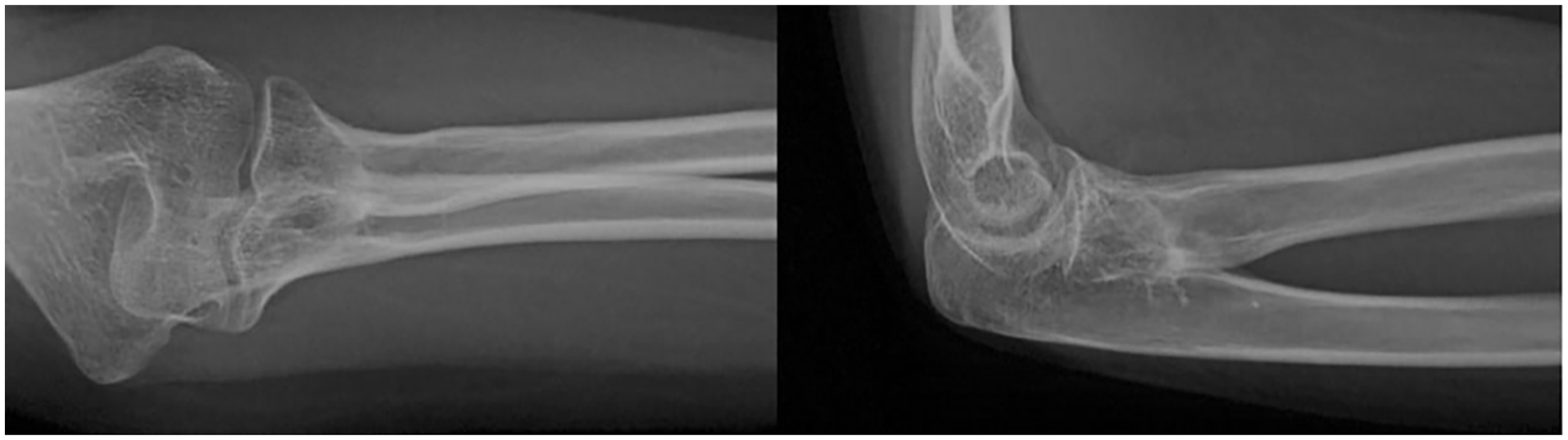
Elbow radiographs of a patient with radioulnar synostosis.
Discussion
The findings of this study suggest that long-term radiological and functional outcomes of pediatric radial neck fractures treated with the Metaizeau technique are highly favorable. With an average follow-up period of 12 years across 22 patients, this study represents one of the most comprehensive follow-up evaluations of this technique to date. Consistently positive outcomes, regardless of patient demographics or fracture type, highlight the reliability and efficacy of the Metaizeau technique as a preferred method for treating pediatric radial neck fractures.
Pediatric radial neck fractures are uncommon, and there is ongoing debate regarding the optimal angulation threshold for surgical intervention. Insufficient treatment can lead to complications and restricted elbow mobility. It can be reasonably deduced that fractures with angulation of less than 30° (Judet types 1 and 2) can be managed effectively with short-term immobilization, which often leads to a positive prognosis and satisfactory functional outcomes.7,10 Fractures with angulation greater than 60° (Judet type 4) typically necessitate surgical intervention, while the management of fractures with angulation between 30° and 60° (Judet type 3) remains a subject of debate, with no clear consensus on the optimal treatment approach.7,11 –14 The majority of studies in the existing literature recommend surgical intervention over conservative treatment, particularly in cases of angulated fractures exceeding 30° (Judet types 3 and 4).15 –21 It has been reported that surgical treatment has the potential to provide better radiological and functional outcomes in such severe fractures and is superior in terms of optimal bone healing and functional recovery in the long term.15 –18,20,21
The long-term functional outcomes of surgical treatment of Judet type 3 and 4 fractures were found to be quite favorable in our study, with a mean MEPS of 98. According to the MEPS, 95% of patients achieved excellent outcomes, while 86% achieved excellent outcomes according to the Tibone and Stoltz classification. In one study, the Métaizeau technique yielded MEPS of 95.2 and 68% excellent results in patients who underwent surgery. 19 In another study, the Métaizeau technique yielded 95% excellent results. 20 In patients who underwent surgery with the Métaizeau technique using K-wires or titanium elastic nails, the mean MEPS was found to be 89.50 and 92.83. 22 The results of this study were found to be superior to those documented in the existing literature regarding the surgical treatment of Judet type 3 and 4 fractures.19,20,22 The discrepancy between our findings and those previously documented in the literature may be attributed to a number of factors, including the younger average age of our patient cohort, the extended follow-up period, and the consistent application of the Metaizeau technique. Previous studies have indicated that younger patients (<10 years) tend to achieve better outcomes, while older age has been associated with poorer functional results, irrespective of fracture type.21,23,24
The mean age of the patient cohort was 9.9 years, with 45% of patients being 10 years of age or older. All patients who did not achieve excellent outcomes were also in this older age group. Among these patients, 10% demonstrated good results according to the MEPS, 30% achieved good outcomes based on the Tibone and Stoltz classification, and 30% experienced complications. These findings are consistent with existing literature; however, our functional outcomes surpass those reported in studies focusing on short- and mid-term results.
Various surgical techniques, both with and without fixation, and utilizing either open or closed approaches, have been widely discussed in the literature. A review of the literature reveals that open methods are frequently linked to inferior radiological and functional outcomes, along with an elevated risk of complications, including avascular necrosis of the radial head.14,17,19,21 Comparisons between open and closed techniques have demonstrated that closed methods are both reliable and effective, offering better outcomes in terms of radiological and functional recovery. 19 Numerous studies have evaluated different closed surgical techniques in comparison to the Metaizeau technique; however, no single approach has consistently demonstrated superiority in radiological and functional outcomes.21,22,25 –27 Nevertheless, case–control studies have indicated that the Metaizeau technique produces favorable short- and mid-term outcomes, with a reduced incidence of complications in comparison to alternative techniques.10,15,16,18,20,26 In our study, the long-term outcomes of the Metaizeau technique were assessed, and our functional results, as well as complication rates, were superior to those reported in the existing literature.
Since this study focused on long-term outcomes, all patients had completed their rehabilitation, returned to daily activities, and reached. Therefore, the results presented here likely represent a comprehensive evaluation of the Metaizeau technique. A variety of complications have been documented in the medical literature related to the surgical management of radial neck fractures. These include radioulnar synostosis, avascular necrosis, heterotopic ossification, posterior interosseous nerve injury, elbow stiffness, nonunion, and malunion.19,21,23,28,29 The occurrence of these complications has typically been associated with more invasive surgical techniques. Nevertheless, severe complications such as avascular necrosis of the radial head and radioulnar synostosis are infrequently observed.21,23,28
In this study, complications included heterotopic ossification in two patients and radioulnar synostosis in one patient. Radioulnar synostosis was the most significant complication affecting functional outcomes, as it was the only complication that limited supination, pronation, and extension. 29
The primary limitation of this study is the relatively modest sample size, which is largely attributable to the scarcity of radial neck fractures. Furthermore, the retrospective design of the study, reliance on previously recorded patient data, and the fact that it was conducted at a single institution may limit the generalizability of the findings. In addition, the long-term results of a single technique were described and we were unable to compare the results with a control group using another technique.
Conclusions
The Metaizeau technique represents an efficacious treatment option for pediatric radial neck fractures, delivering optimal radiological and functional outcomes with a minimal incidence of complications. The positive results observed in long-term follow-up reinforce the technique’s reliability and effectiveness. To further validate the efficacy of the Metaizeau technique, future studies should focus on larger patient cohorts and extended follow-up periods.
Supplemental Material
sj-pdf-1-cho-10.1177_18632521241300878 – Supplemental material for The long-term results of treating radial neck fractures in children with the Metaizeau technique
Supplemental material, sj-pdf-1-cho-10.1177_18632521241300878 for The long-term results of treating radial neck fractures in children with the Metaizeau technique by Muharrem Kanar, Yusuf Sülek, Bilal Gök, Abdurrahman Demirhan, Farıd Samadov and Bahadır Balkanlı in Journal of Children’s Orthopaedics
Footnotes
Author contributions
All authors contributed to the conception and design or acquisition of data or analysis and interpretation of data; drafted the manuscript or critically revised it for important intellectual content; and contributed to the final approval of the version to be published.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
Health Sciences University Şişli Hamidiye Etfal Training and Research Health Practice And Research Center (SUAM) Ethics Committee For Clinical Research, Approval number: 4487.
Informed consent
All patients provided written informed consent prior to their inclusion in the study, in accordance with institutional and ethical guidelines.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.