
Abstract
Abstract
Purpose
Displaced supracondylar humerus fractures are treated with open or closed reduction and percutaneous pinning. In 2012, our management of patients with a displaced fracture changed from closed reduction in the emergency department (ED) to in situ splinting prior to closed reduction and pinning in the operating room (OR). The purpose of this study was to investigate if outcomes or complications differ between these two management methods.
Methods
Patients less than ten years old with a Gartland type II or III supracondylar humerus fracture between 2008 and 2016 were included. Cases of polytrauma were excluded. Radiographic outcomes were assessed at follow-up. The Fisher's exact test was used for categorical variables and the Wilcoxon rank sums tests for continuous variables.
Results
In all, 157 patients were included, 89 with reduction in the ED and 68 without. There was no significant difference between the groups related to demographic factors or fracture characteristics. Patients managed without reduction in the ED had a lower average delay from ED to OR compared with those treated with reduction (16 hours versus 22 hours, p < 0.005) and a shorter hospital length of stay (34 hours versus 40 hours, p < 0.005).
Conclusion
No difference in complications or outcomes was found between patients with Type II or III supracondylar fractures treated initially with or without closed reduction in the ED. Patients treated without ED reduction were taken to the OR sooner and remained in the hospital for a shorter period of time. Splinting in situ reduces anaesthesia exposure without increasing postoperative complications or suboptimal outcomes.
Level of Evidence
Level III, retrospective comparative study
Introduction
Supracondylar humerus fractures are the most common elbow fracture in children. 1 They occur with a reported incidence rate of 20.7/100 000 and at an average six years of age, with extension type occurring in over 90% of cases.2–5 Although some studies report a slight male preponderance, recent literature has noted equivalent incidence rates between male and female children.2,5
Supracondylar humerus fractures are usually classified according to the modified Gartland classification system.1,6–8 A minimally displaced, or a type I, supracondylar fracture is typically treated with casting alone. A type II fracture is > 2 mm displaced with an intact posterior cortex and may benefit from surgical management depending on the amount of displacement. Gartland type III fractures are characterized by a displaced supracondylar fracture that lacks an intact cortex. Finally, Gartland type IV fractures are defined by multidirectional instability. Type III and IV fractures almost always need surgery. 9
Immediate reduction in the operating room (OR) and possible surgical treatment is indicated for supracondylar humerus fractures with vascular compromise. For vascularly intact supracondylar fractures, a delay in operative management post-injury can be tolerated and does not affect perioperative complications or the need for open reduction.10–13 The most common operative treatment for displaced supracondylar fractures is closed reduction followed by percutaneous pinning.1,14–17 Many studies have investigated the demographics, risk factors and complications associated with this treatment modality.4,5,18–20 Multiple attempts at reduction may increase the risk of neuropraxia, elbow stiffness, myositis ossificans and anaesthetic complication.9,21–25 No studies, however, have specifically compared the outcomes associated with closed reduction performed in the emergency department (ED) versus in situ splinting and definitive management in the OR.
Prior to 2012, patients presenting to our institution with a displaced supracondylar humerus fracture usually underwent a closed reduction in the ED prior to definitive management. Since 2012, our protocol transitioned to in situ splinting in the ED followed by hospital admission until closed reduction and pinning are attempted solely in the OR. The purpose of this study was to investigate if there are differences in outcomes or complications between these two management methods.
Materials and methods
Following Institutional Review Board approval, 157 patients aged one to ten years who presented with a supracondylar humerus fracture Gartland type II or type III between 01 January 2008 and 31 December 2015 and complete ED records were identified. Departmental databases and billing records from a single institution were searched using the International Classification of Diseases, Ninth Revision, Clinical Modification (ICD-9-CM; https://www.cdc.gov/nchs/icd/icd9cm.htm) code 812.41 for closed supracondylar fracture of humerus. Electronic medical records and radiographs were retrospectively reviewed to determine demographic information, fracture classification, hospital time course, neurovascular status and radiographic outcome data. Length of stay was based on the time between inpatient admission and inpatient discharge.
Fractures were assessed radiographically post-reduction and during the follow-up period. Baumann's angle, the intersection of a line drawn along the axis of the humeral shaft and a line drawn through the physis of the lateral condyle of the humerus was measured on anteroposterior radiographs.26,27 The anterior humeral line was evaluated on lateral radiographs. The anterior humeral line was considered normal if a line drawn along the anterior aspect of the humeral shaft intersected the capitellum on the lateral radiograph (Fig. 1a) and abnormal if it did not intersect the capitellum (Fig. 1b). 28
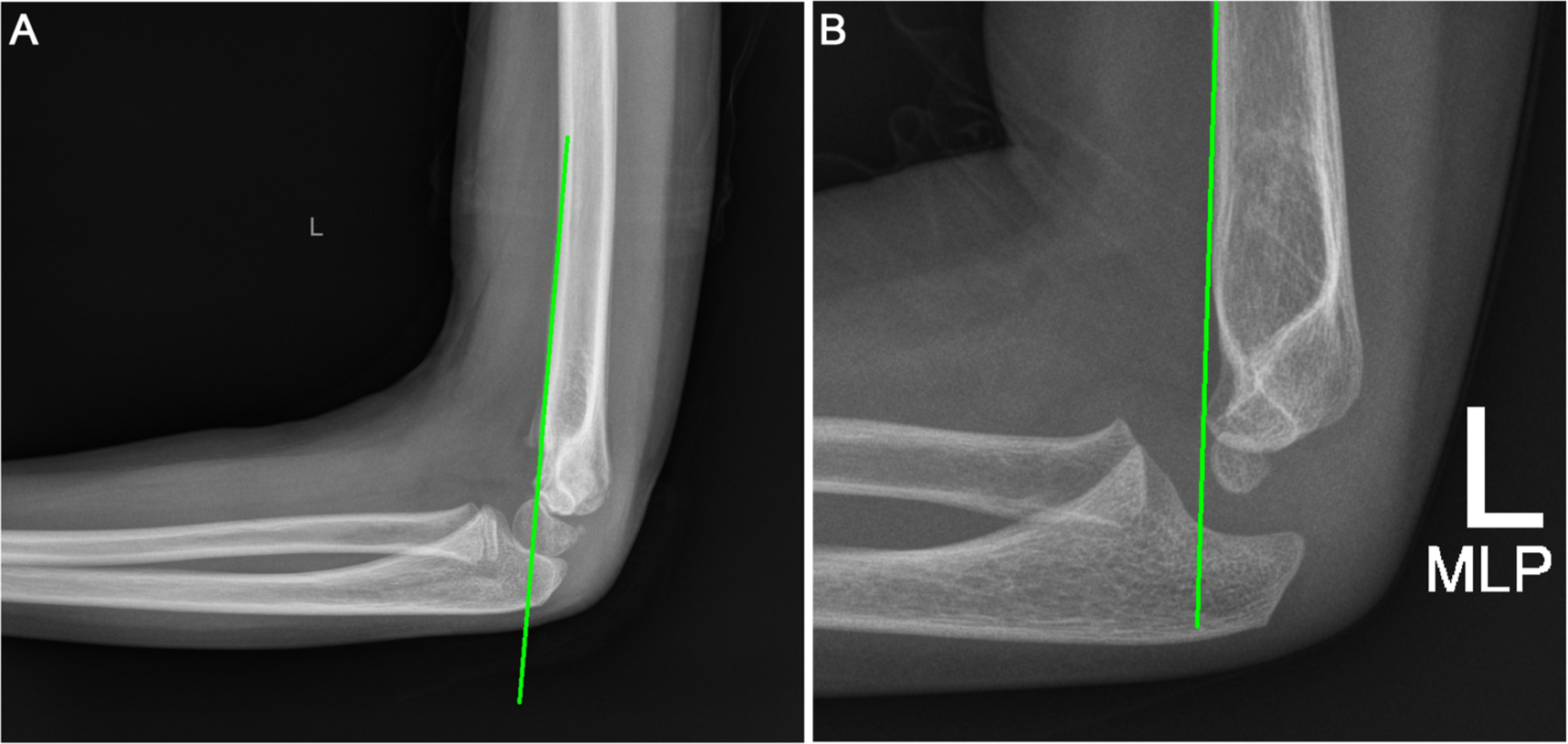
Evaluation of elbow alignment using the anterior humeral line drawn along the anterior aspect of the humeral shaft on a lateral radiograph. Alignment is considered:
The initial management of patients varied at our institution. Prior to 2012, per surgeon preference, patients with displaced supracondylar humerus fractures were treated with closed reduction and splinting under conscious sedation in the ED. They would then be admitted and taken to the OR for definitive management. Since 2012, we have transitioned to a protocol in which all of these patients are splinted in situ without ED reduction. As this transition in practice was gradual, there was no definitive cutoff date and assignment to each treatment group was based on surgeon preference at the time of presentation.
Patients initially treated with or without closed reduction in the ED were compared using Fisher's exact test for categorical variables and the Wilcoxon rank sums tests for continuous variables. Median values were selected for use to reduce biased means related to outliers. Demographic and radiographic parameters were analyzed, including age, sex, race, weight, height, body mass index (BMI), BMI for age percentile (BMI%), fracture classification, total number of pins, number of medial pins, number of lateral pins, preoperative neurovascular injury, postoperative neurovascular injury, mechanism of injury, side of injury, hospital time course, Baumann's angle and anterior humeral line position at most recent follow-up.
Results
A total of 157 patients with displaced supracondylar humerus fractures met inclusion criteria for analysis. Prior to 2012, these patients were treated with closed reduction and splinting under conscious sedation in the ED before admission and surgical management. After 2012, these patients were splinted in situ without ED reduction before admission and surgical management. Between both protocols there was a gradual transition period, in which assignment to each treatment group was based on surgeon preference. In total, 89 patients (57%) were reduced in the ED and 68 patients (43%) were not reduced in the ED on initial presentation (Table 1).
Patient demographics
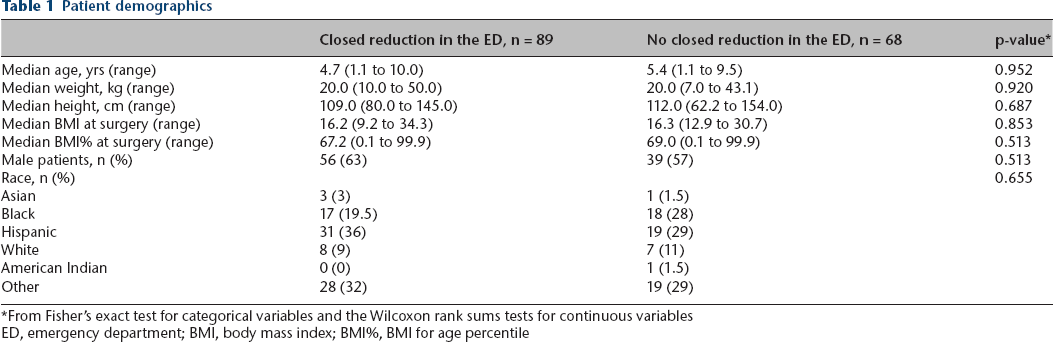
From Fisher's exact test for categorical variables and the Wilcoxon rank sums tests for continuous variables
ED, emergency department; BMI, body mass index; BMI%, BMI for age percentile
Of the 89 patients reduced in the ED, 56 (63%) were male and 33 (37%) were female. The median age at presentation was 4.7 years (1.1 to 10.0). In total, 34 fractures were classified as Gartland type II, 55 were classified as Gartland type III, three patients had preoperative nerve palsies and one patient had a pink pulseless hand. Pulse returned after reduction and nerve injuries resolved.
Of the 68 patients not reduced in the ED, 39 (57%) were male and 29 (43%) were female. The median age at presentation was 5.4 years old (1.1 to 9.5). Regarding fracture characteristics, 32 were classified as Gartland type II, 36 were classified as Gartland type III and one patient had a preoperative nerve palsy.
There was no significant difference between the groups related to demographic factors such as age, BMI, sex or race (Table 1). Additionally, there were no differences in fracture characteristics, including laterality (p = 0.145), median Baumann's angle (closed reduction 75.5° versus no reduction 73.6°, p = 0.105), fracture classification (p = 0.328) or preoperative neurovascular insult (p = 0.390) (Table 2). Although the number of pins used was similar between groups, fewer patients in the non-reduction group received medial pins compared with patients with ED reduction (p = 0.014). No difference in number of lateral pins or follow-up was observed (p = 0.532) (Table 2).
Fracture characteristics and treatment
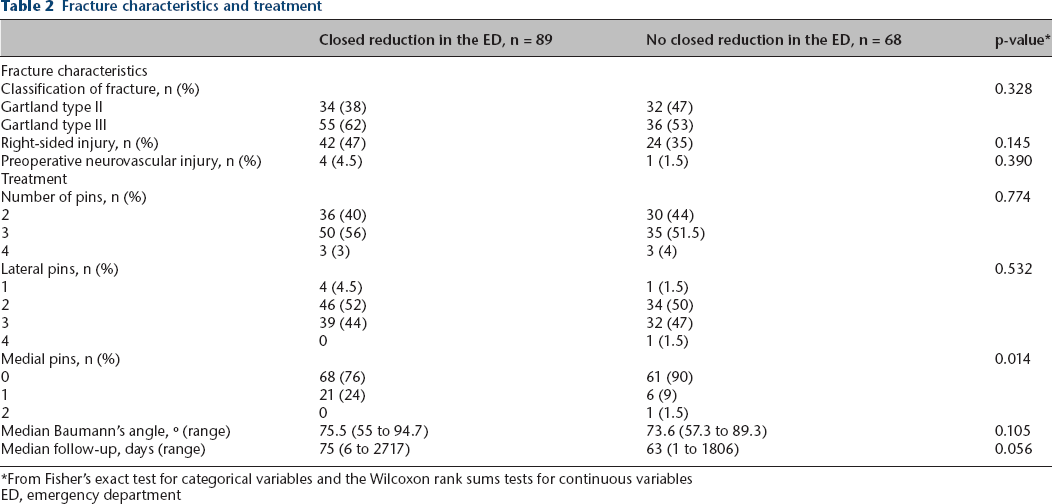
From Fisher's exact test for categorical variables and the Wilcoxon rank sums tests for continuous variables
ED, emergency department
Compliance with ethical standards
When comparing outcomes in both groups, we found that two of 68 patients (3%) without closed reduction and four of 89 patients (4.5%) with ED closed reduction received open surgical management (p = 0.699). Patients managed without reduction in the ED had a lower average delay from ED to OR (16 hours versus 22 hours, p < 0.005) and a shorter hospital length of stay (34 hours versus 40 hours, p < 0.005) compared with those treated with ED reduction. Lastly, there was no difference between the groups in the other outcomes we considered including total OR time (p = 0.298), postoperative neurovascular status (p = 1.000) or number of patients with a normal anterior humeral line at follow-up (p = 0.319) (Table 3).
Outcomes

From Fisher's exact test for categorical variables and the Wilcoxon rank sums tests for continuous variables
ED, emergency department; OR, operating room
Discussion
This study provides outcome data related to a series of patients treated for supracondylar humerus fractures at a single institution. Previous studies have not compared outcomes associated with initial closed reduction performed in the ED versus initial closed reduction performed in the OR. The aim of this study was to identify differences in outcomes or complications related to these two management techniques. While most centres perform in situ splinting, personal communication indicates that at least some practices still perform ED closed reduction.
Patients treated without ED reduction were taken to the OR sooner and remained in the hospital for a shorter period of time than patients treated with ED reduction, with no observed difference in postoperative complications or outcomes. These findings are especially important when considering that patients undergoing a single reduction in the OR were not subjected to an additional round of conscious sedation to achieve reduction and place a temporary cast or splint in the ED.
In a recent review of adverse events following paediatric, procedural sedation in 1341 patients, Newman et al. 23 found that 13.7% of patients experienced an adverse event. In all, 12% of these were serious, including emesis, agitation, rash, nausea, dizziness, slurred speech, hypoxia, hypotension and stridor. A total of 92% of adverse events occurred during the procedure, and over half were observed during an orthopaedic reduction. Extended monitoring following procedural sedation increased the amount of time spent in the ED and was further compounded by an adverse event.
In addition to increased anaesthetic requirements, patients treated with closed reduction in the ED also underwent multiple reduction attempts at the time of their presentation. These additional attempts at reduction may increase the risk of neuropraxia, elbow stiffness and myositis ossificans.9,21–25 In 2015, Kwok et al 29 reported on 166 patients with nerve injuries following a supracondylar humerus fracture and reduction in the OR. Of the 30 patients in their cohort who suffered an iatrogenic injury, 40% were thought to be due to nerve entrapment at the time of fracture reduction. While the vast majority of these patients went on to achieve good outcomes, the potential for harm exists with every reduction attempt.
Although patients treated without closed reduction in the ED were taken to the OR sooner, the clinical significance of this factor is uncertain. Numerous studies have investigated the effect of delayed treatment on the outcome of supracondylar humerus fractures.10–13,30–35 These studies have shown that there is no correlation between surgical delay and outcomes such as neurovascular injury, infection, compartment syndrome, malalignment, range of movement or need for reoperation. However, one outcome that has proved to be controversial is the need for open reduction. In their retrospective review of 171 children with closed, neurovascularly intact, Gartland type III fractures, Walmsley et al. 35 reported that children with a surgical delay of more than eight hours after presentation were more likely to require an open reduction. In their population, 33% of the late treatment group and 11% of the early treatment group underwent open reduction. However, a more recent study by Abbott et al. 10 found no correlation between surgical timing and conversion to open reduction. In their retrospective review of 297 patients with closed Gartland type III supracondylar humerus fractures, 28 patients (9.4%) required open reduction, with no difference in time from presentation to OR or time from injury to OR between the two groups. These findings are similar to other studies in the literature,11,32,34 and a recent systematic review found that a delay in surgical treatment of 91 hours did not affect the need for open reduction or perioperative complications. 12 It is important to note that the methodology of these studies varies, and no specific cut-off has been established for what constitutes delayed treatment. Additionally, the exact time of injury is often difficult to determine retrospectively. To fully assess the clinical importance of our findings, further research with established protocols is warranted.
The limitations of this study include those associated with a retrospective review, including availability, accuracy and consistency of documentation. Additionally, current patient-reported outcomes were not able to be assessed, which would have allowed for supplementary comparison to similar studies. Lastly, due to the different time frames for sampling of the groups, chronology bias might have occurred and other parameters within the medical system could have affected outcomes. A more standardized protocol for assigning patients to treatment groups would decrease the risk of selection bias. However, for both groups similar inclusion/exclusion criteria existed, the same diagnosis criteria and outcome measures were used and our two groups did not differ in any of the presenting parameters. Besides a change of practice in the ED, we also observed a change in the use of medial pins during surgery based on surgeon preference after 2012.
In summary, we used an evolving practice protocol to examine specific outcomes following two different management strategies for patients presenting with displaced supracondylar humerus fractures. Analysis of our cohort found that compared with children with ED reduction, in situ splinting decreased time to the OR and decreased overall length of stay. Additionally, these patients underwent fewer anaesthesia events and reduction attempts, while maintaining similar outcomes. These findings help to confirm that in situ splinting is the most appropriate initial management for displaced supracondylar humerus fractures in the paediatric population.
Footnotes
Acknowledgements
The authors thank Vahag Kechejian and Todd A. Rubin, MD for their support of this project.