
Abstract
Purpose:
Neuroblastoma (NB) is a common extracranial solid tumor in children, often requiring surgical resection. Post-resection NB near the spine can lead to spinal deformities, but treatment strategies are not well-documented.
Methods:
We retrospectively reviewed our patients who developed spinal deformities after NB resection at our hospital from 2013 to 2021. Treatment included the traditional growing rod (TGR) technique for patients with growth potential, posterior spinal fusion (PSF) for skeletally mature patients, and intermittent cast therapy for infants.
Results:
Five female patients underwent chemotherapy and surgical resection for NB, with no recurrence during follow-up. Single curves were seen in Cases 1, 2, 4, and 5, and Case 3 had double curves. NB tumors were on the convex side in Cases 1, 3, and 5, and on the concave side in Cases 2 and 4. TGR was used for Cases 1 and 2 due to growth potential and inadequate height. PSF was chosen for Cases 3 and 4, achieving satisfactory scoliosis and kyphosis correction. Case 5, diagnosed with scoliosis at 16 months, underwent intermittent cast therapy for 2 years, significantly correcting scoliosis and avoiding surgery. The average time from NB resection to scoliosis onset was 65.2 ± 49.3 months, with scoliosis treatment starting at 82.6 ± 58.1 months. The mean follow-up was 38.2 ± 12.1 months. All patients showed significant improvement in spinal deformities, with no significant correction loss at the last follow-up.
Conclusions:
After NB resection, spinal deformities should be closely monitored, with intervention preferably within 6 months of discovery. TGR, PSF, and casting are effective interventions, with the treatment modality based on the patient's skeletal maturity and height.
Introduction
Neuroblastoma (NB) is the most common extracranial solid tumor in children, accounting for 8%–10% of all childhood tumors, and comprehensive treatment followed by surgical resection is required upon detection. 1 With the continuous advancement of medical technology, the prognosis and quality of life of NB patients have steadily improved. 2 However, NB near the spine may involve the vertebral bodies or penetrate the spinal canal through the intervertebral foramina. Surgical resection often entails a wide range and significant injury, which may disrupt the local spinal anatomy. Consequently, there has been an increasing number of reports on spinal deformities following NB resection.3 –14 Patients undergoing NB resection are often in the pre-pubertal growth spurt, and postoperative body growth may lead to severe spinal deformities. However, there is limited literature on the treatment of such spinal deformities. To summarize the diagnostic and therapeutic experience of such patients, we retrospectively collected clinical data of patients who developed spinal deformities after NB resection in our center. We analyzed and summarized the characteristics of the cases, treatment strategies, and prognosis to improve clinical diagnosis and treatment efficiency, providing reference for spinal surgeons.
Materials and methods
We retrospectively collected clinical data of patients who developed spinal scoliosis deformities after undergoing NB resection in our hospital from January 2013 to January 2021. Inclusion criteria were as follows: (1) age ≤14 years; (2) NB involvement of the spine or adjacent structures; and (3) follow-up duration ≥24 months. Exclusion criteria were as follows: (1) NB recurrence or patient death during the follow-up period; (2) incomplete clinical or radiological data; (3) scoliosis caused by congenital, traumatic, or other reasons; and (4) refusal of patient’s family to participate in the study. This study was approved by the Medical Ethics Committee of our hospital (Approval No.: [2024]-E-049-R). Informed consent forms were signed by the guardians of all included patients during outpatient follow-up visits (consenting to the collection of their clinical data for research purposes).
Report of cases
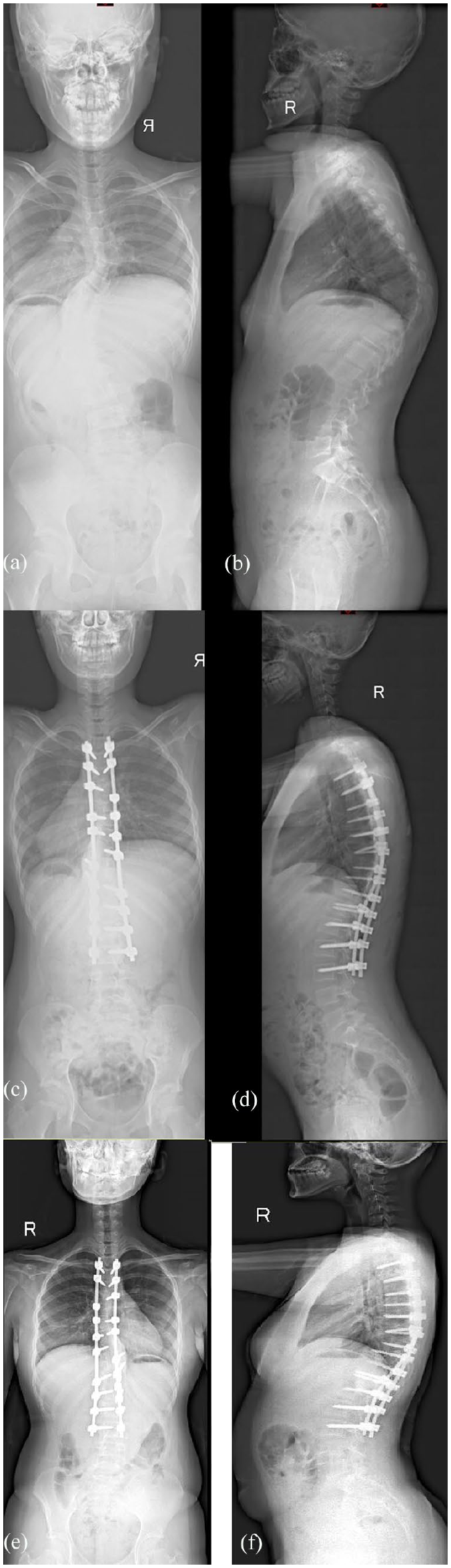
Case 1. This is a female who presented at 31 months of age and had NB in the posterior mediastinum and spinal canal. Prior treatment included laminectomy (T7–T10), resection, and chemotherapy 24 months prior to treatment of the spinal deformity. She was asymptomatic at presentation. She had a single curve, convex at the side of the NB of 94° (Table 2). The vertebral body and pedicle were deformed at the site of the prior laminectomy (Figure 7). She was treated with TGR (Figure 1)

Case 1, 31 months, TGR. (a, b) Pre-operation scoliosis 94.1°, kyphosis 73.5°. (c, d) Post-operation scoliosis 55.5, kyphosis 34.4°. (e, f) Last follow-up scoliosis 36.6°, kyphosis 44.8°.
Case 2. This is a female who presented at age 8 + 6 and had NB in the posterior mediastinum which did not invade the spine. Prior treatment included resection and chemotherapy 81 months prior to treatment of the spinal deformity. Her symptom at presentation was decreased activity. She had a single curve, concave at the side of the NB of 51° (Table 2). There was vertebral scalloping at the site of the prior laminectomy (Figure 8). She was treated with TGR (Figure 2).

Case 2, 90 months, TGR. (a, b) Pre-operation scoliosis 51.1°, kyphosis 64.2°. (c, d) Post-operation scoliosis 18.8°, kyphosis 35.2°. (e, f) Last follow-up scoliosis 27.3°, kyphosis 59.4°.
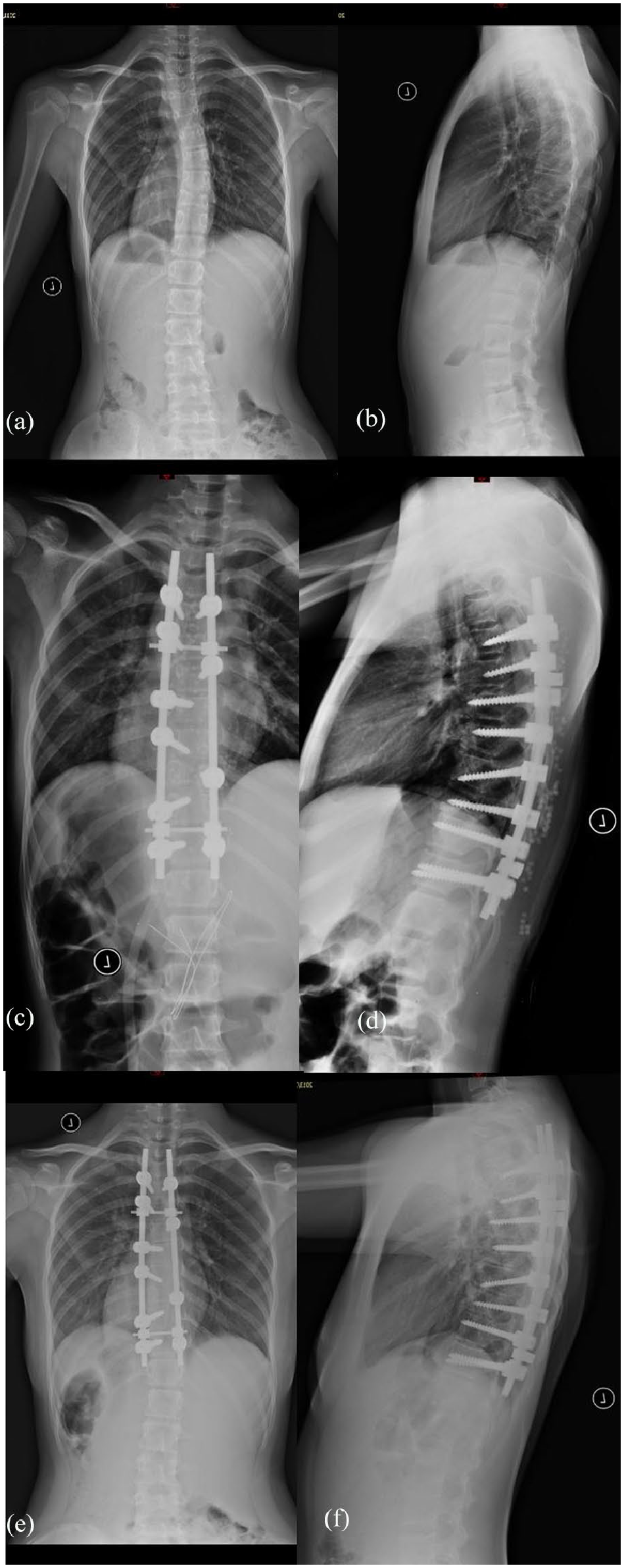
Case 3. This is a female who presented at age 10 + 8 and had NB in the posterior mediastinum and spinal canal. Prior treatment included laminectomy (T8–T11), resection, and chemotherapy 120 months prior to treatment of the spinal deformity. She had back pain at the presentation. She had a double curve, concave at the side of the NB measuring 66°, and a lumbar curvature of 46° (Table 2). The most severe region of spinal deformity was at the site of laminectomy (Figure 6). She was treated with posterior spinal fusion (PSF; Figure 3).
Case 3, 128 months, PSF. (a, b) Pre-operation scoliosis 65.5°/45.9°, kyphosis 65.9°. (c, d) Post-operation scoliosis 33.2°/33.3°, kyphosis 36.4°. (e, f) Last follow-up scoliosis 32.0°/31.1°, kyphosis 39.5°.
Case 4. This is a female who presented at age 14 + 4 and had NB in the posterior mediastinum and spinal canal. Prior treatment included laminectomy (T6–L1), resection, and chemotherapy 97 months prior to treatment of the spinal deformity. She was asymptomatic at presentation. She had a single curve, concave at the side of the NB of 20° (Table 2). Vertebral wedging and Schmorl’s nodes were seen. She was treated with PSF (Figure 4).
Case 4, 148 months, PSF.
Case 5. This is a female who presented at age 16 months and had NB in the posterior mediastinum. Prior treatment included resection and chemotherapy 4 months prior to treatment of the spinal deformity. She was asymptomatic at presentation. She had a single curve, concave at the side of the NB of 29° (Table 2). She was treated with a plaster vest (Figure 5).

Case 5, 16 months, Serial casting. (a, b) Pre-operation scoliosis 28.5°. (c, d) Post-operation scoliosis 11.2°. (e, f) Last follow-up scoliosis 7.3°, kyphosis 25.4°.
Results
Summary of cases
This study included a total of five patients, all of whom were female. They all received chemotherapy and surgical resection for NB, and none experienced recurrence during the follow-up period. Among them, NB extended into the spinal canal through the intervertebral foramina in Cases 1, 3, and 4, and destruction of the lamina and surrounding spinal structures was performed during tumor resection. Within 16 months after tumor resection, all patients exhibited a spinal asymmetry on forward bending. In addition, Case 2 showed a significant decrease in motor endurance, and Case 3 experienced symptoms of lower back pain, while Cases 4 and 5 did not manifest significant physical symptoms.
Among the five cases, Cases 1, 2, 4, and 5 presented with single curves (80%), while Case 3 presented with double curves (20%). The original NB in Cases 1, 3, and 5 was located on the convex side, while the tumors in Cases 2 and 4 were located on the concave side. Specific clinical data are detailed in Table 1.
The clinical characteristics of five patients.

NB, neuroblastoma; T, thoracic.
For Cases 1 and 2, due to the patients’ significant growth potential and inadequate height, we opted for the traditional growing rod (TGR) technique to control their spinal scoliosis and kyphosis. The postoperative scoliosis correction rates were 41.0% and 63.2% for Cases 1 and 2, respectively. Subsequently, TGR lengthening surgeries were performed every 6–9 months. Although some correction loss was observed at the last follow-up, the degree of scoliosis control remained acceptable, with good trunk and shoulder balance (Figures 1 and 2).
Considering the age and skeletal maturity of Cases 3 and 4, PSF was chosen as the definitive treatment. Immediate postoperative results showed satisfactory correction of both scoliosis and kyphosis, and good trunk balance was maintained at the last follow-up (Figures 3 and 4).
Case 5 developed spinal scoliosis at the age of only 16 months, making surgical treatment inappropriate. To control the progression of spinal deformity, we opted for intermittent cast therapy for 2 years. At the last follow-up, X-rays showed excellent treatment outcomes, with significant correction of local scoliosis and no indication for surgery (Figure 5).
The average time from undergoing NB resection to the onset of spinal scoliosis in these five patients was 65.2 ± 49.3 months (range: 4–120 months), while the average age at the initiation of scoliosis treatment was 82.6 ± 58.1 months (range: 16–148 months). The mean follow-up duration was 38.2 ± 12.1 months (range: 24–55 months). All patients showed significant improvement in spinal deformity compared to pre-treatment conditions, and there was no significant loss of correction at the last follow-up. Detailed radiological data are shown in Table 2.
The radiographic characteristics of five patients.

NB, neuroblastoma; TGR, traditional growing rods; PSF, posterior spinal fusion.
Discussion
Spinal deformities, including scoliosis and kyphosis, are common physiological problems in NB survivors. 7 This may be due to tumor invasion or damage to adjacent structures during NB resection. Laminectomy, a common adjunctive procedure for the treatment of NB that invades the spinal canal or erodes adjacent structures, may disrupt the posterior spinal ligamentous complex, leading to spinal instability, especially in children at their growth spurt. Paulino and Fowler 5 found that laminectomy is one of the important independent risk factors for the development of scoliosis in young children. In addition, various factors during comprehensive NB treatment, such as initial tumor grading, tumor recurrence, secondary malignancy after treatment, adverse effects of chemotherapy on bone formation, and secondary osteoporosis, may contribute to the development of scoliosis. 8 NB may damage paraspinal musculature or promote metabolic changes in the region, which can lead to spinal curvature. Even in the absence of neurosurgery, damage to the vertebral body and surrounding structures caused by NB may contribute to the development of scoliosis.15,16 Notably, according to Cooke-Barber et al., 17 open-heart surgery in childhood for certain diseases is also an important cause of scoliosis.
In our series, the NBs were all located laterally to the spine, and in Cases 1, 3, and 4, tumor infiltration extended into the spinal canal, leading to canal compression. To achieve complete tumor resection, pediatric tumor orthopedic surgeons excised the vertebral plates in these three patients. However, during follow-up, the spinal deformity in the area of vertebral plate excision was most pronounced (Figure 6), with substantial deformation observed in the vertebral bodies and pedicles (Figure 7). Vertebral body destruction due to NB was evident in Cases 1, 2, and 3. Cases 2 and 3 exhibited scalloping changes in the vertebrae (Figure 8). Interestingly, Case 2 also presented spinal deformity without undergoing vertebral plate excision surgery, suggesting that tumor-induced vertebral destruction might be a significant contributing factor. Case 4 showed vertebral body wedging and Schmorl’s nodes (Figure 9), likely secondary to spinal deformity and NB.

The most severe area of spinal deformity was located in the laminectomy area in Case 3.
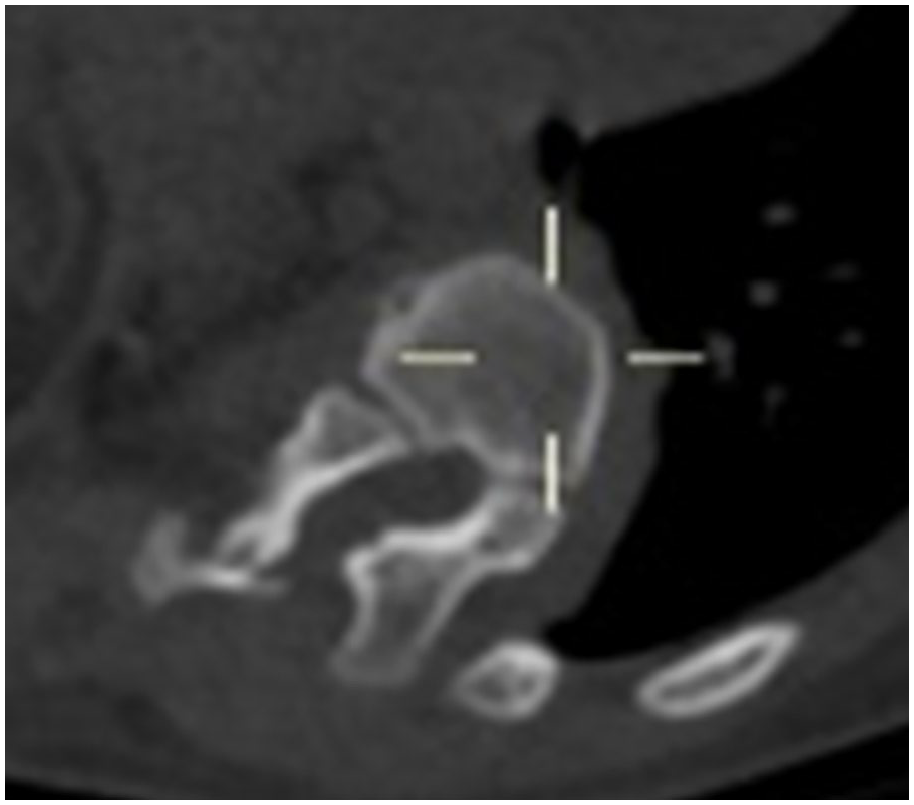
The vertebral body and pedicle were deformed after laminectomy in Case 1.

Scallop-like changes in Case 2.

The vertebral wedge and Schmorl’s nodes were seen in Case 4.
Postoperative spinal deformities in survivors of NB surgery should be given sufficient attention by clinical practitioners. Zaleske et al. 3 reported a case of postoperative spinal scoliosis with accompanying nerve injury after thoracic NB surgery in 1982. Improvement in nerve injury and spinal scoliosis was achieved through anterior decompression, posterior osteotomy fusion, and internal fixation. Anakwenze et al. 18 conducted a retrospective analysis of 255 cases of spinal cord tumor patients, suggesting that the use of instrumentation or in situ fusion during spinal cord tumor resection significantly reduced the occurrence of postoperative spinal deformities. In the study by Barrena et al., 10 various techniques such as TGR implantation, VEPTR (Vertical Expandable Prosthetic Titanium Rib), and joint fixation have been successful in treating postoperative spinal deformities following neurotumor surgery.
They proposed that spinal surgery should be considered for patients with a spinal scoliosis angle >60° or rapidly progressing deformities, including observable kyphosis. In their report, the median preoperative Cobb’s angle was 65° (range: 50°–90°), 2.9 (range: 0.4–11) years after tumor resection, and the median postoperative instrumented angle was 40° (range: 20°–50°), 3.1 (range: 0.2–12.2) years later, with an improvement rate of 38.4%. Hell et al. 8 stated that a considerable number of children with spinal tumors, intraspinal tumors, or tumors involving the spine would develop spinal deformities. Conservative treatment is often unsuccessful. Spinal implants conducive to growth can significantly correct spinal scoliosis and achieve definitive spinal fusion during adolescence. They also recommended that internal fixation surgery should be performed simultaneously with spinal tumor resection in adolescent patients, especially in cases involving the thoracic or thoracolumbar regions.
After paraspinal NB surgery, close monitoring and follow-up of the child are necessary to promptly detect the onset of spinal curvature. The timing and method of intervention are crucial. Regarding the timing of intervention, we believe that close monitoring should be implemented upon discovery because spinal curvature after NB surgery typically continues to progress. Relying solely on observation may lead to serious consequences. Therefore, intervention by a pediatric spine surgeon is necessary within 6 months of the appearance of spinal curvature. As for the intervention method, younger patients often achieve better control of curvature through continuous spine casting. Older children, however, require a comprehensive assessment based on skeletal maturity and height to determine the application of fusion techniques (PSF) or non-fusion techniques (TGR). The initial age of spinal surgery for case 1 was 31 months, and for case 2, it was 90 months. Both patients exhibited pronounced back asymmetry deformity, with spinal scoliosis angles greater than 60° and observable kyphosis, suggesting a relatively flexible main curve position. TGR technique was employed to control spinal deformity, with lengthening performed every 9 months. At the last follow-up, spinal deformities had significantly improved compared to preoperative conditions. Case 3 was a teenager with back asymmetry deformity and back pain. The curve type was thoracolumbar, with spinal scoliosis angles of 65.5°/45.9° and flexibility indices of 29.3%/23.1%, indicating rigid spinal scoliosis. Preoperative spinal kyphosis was 65.9°. PSF was performed to correct spinal deformity. At the last follow-up, the spinal scoliosis angles were 33.2/33.3, and the kyphosis was 36.4°, showing significant improvement compared to preoperative conditions. Back asymmetry deformity was not evident, and back pain disappeared. Case 4, aged 148 months, had a preoperative spinal scoliosis angle of 19.8°, with normal kyphotic angles. The flexibility index was 62.1%, indicating a flexible curve. Due to rapid growth and development, PSF surgery was performed to prevent further development of spinal scoliosis. Postoperatively, spinal scoliosis was completely corrected. Two years later, at the last follow-up, the spinal scoliosis was 14.6°, with no kyphosis observed. Case 5, aged 16 months, had a preoperative spinal scoliosis angle of 28.5°, with a flexibility index of 19.3%, indicating a rigid curve. Due to the inability to obtain standing spine X-rays of the patient, the angle of spinal kyphosis could not be measured. A continuous casting technique under general anesthesia was employed, with casting changed every 6–12 weeks. After eight casts, the spinal scoliosis was corrected to 7.3, with normal vertebral kyphosis. The cast has been removed, and the patient is undergoing close follow-up.
Limitation
Such cases are relatively rare in clinical practice, and some guardians of NB patients may choose not to disclose or discuss their situation for various reasons. Therefore, our study has a limited number of cases, and further discussion on the selection of surgical indications and improvements in surgical techniques will be needed with the inclusion of more cases. At the same time, due to the limited number of cases, our study may suffer from some selection bias. However, these issues can be addressed as the number of cases increases in subsequent studies.
Conclusion
Overall, selecting an appropriate treatment approach for patients with scoliosis following NB resection is challenging. We believe that the TGR technique is an excellent choice for patients with immature skeletal development and unsatisfactory height, while PSF is preferable for patients with nearly mature skeletal development. Continuous casting correction is suitable for young children. Interventions, whether surgical or non-surgical, initiated upon the onset of scoliosis, typically yield favorable corrective outcomes.
Supplemental Material
sj-pdf-1-cho-10.1177_18632521241287031 – Supplemental material for Treatment of scoliosis in children after resection of neuroblastoma—A report of five cases
Supplemental material, sj-pdf-1-cho-10.1177_18632521241287031 for Treatment of scoliosis in children after resection of neuroblastoma—A report of five cases by Jianglong Xu, Yan Zou, Hanwen Zhang, Jinchen Chen, Haonan Liu, Dong Guo and Ziming Yao in Journal of Children’s Orthopaedics
Footnotes
Author contributions
Jianglong Xu, Yan Zou, and Hanwen Zhang: conceptualization, writing—original draft, writing—review and editing, patient management and literature review; Ziming Yao and Dong Guo: supervision, editing of the manuscript, critical appraisal, and final approval of the manuscript; Haonan Liu and Jinchen Chen: writing—review and editing, patient management, and literature review. All authors have finally confirmed and reviewed the manuscript content.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Supported by Sanming Project of Medicine in Shenzhen (code: SZSM202011012), National High Level Hospital Clinical Research Funding (code: 2022-PUMCH-D-004), and Key R&D Projects of Xinjiang (code: 2023B03018).
Ethics approval
Ethical approval was approved by the local ethics committee of Beijing Children’s Hospital at Capital Medical University (IEC-C-006-A04-V.07.1).
Consent to participate
Informed consent was obtained from the parents/guardians of all participants included in the study.
Consent to publish
The parents/guardians of participants consented to the submission of the original article to the journal.
Previous communication
None.
Availability of data and material
The data used during the current study are available from the corresponding author upon reasonable request.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.