
Abstract
Abstract
Incidence and cause
Cerebral palsy (CP) is characterized by poor motor control. The more severe the affection is, the more patients are prone to deformities. Patients with Gross Motor Function Classification System level V run an up to 90% risk for spinal deformities. These are caused by poor trunk control under load. Although trunk tone is impossible to assess it seems to be low in the majority of patients, leading to collapse under gravity. The constant malposition results in growth asymmetry which leads to fixation and deterioration of the deformity.
Brace treatment
Brace treatment has a poor reputation in respect to the final outcome. Conventional braces as constructed for other spinal deformities are indeed difficult for patients with CP as they cannot change position in the brace and do not tolerate pressure on the belly for reflux problems. Respecting these points improves the tolerance of braces but still the time of use is far from the necessary when the trunk is upright. Nevertheless, they can help to postpone surgery for scoliosis, but they are very inefficient for sagittal plane deformities.
Aim of treatment
The lack of trunk control further leads to an impairment of head control and upper extremity function. Providing stability improves these problems. Braces are superior to seating shells for both treating deformity and providing stability as they remain close to the skin and follow movements. Supports on seating shells in contrast are too far away for controlling the deformity and provide stability only if the patient doesn't move forward.
Keywords
Introduction
The spine, apart from the pelvis, consists of 24 vertebrae which have 6° of freedom to move. Under load and gravity, this chain of mobile bodies requires functional control to keep a straight upright posture and allow for mobility in all directions. An effective motor control requires adequate proprioception, equilibrium and muscle activation. In patients with cerebral palsy, all these functions are disturbed. While the motor affection is obvious and thus widely known, the sensory affection got recognized only in the recent past when functional MRI and tractography revealed the lack of sensory connections in the brain.1,2 It is, therefore, not a surprise that the more severely the cerebral palsy is expressed the more trunk control is impaired 3 and the more frequent and pronounced spinal deformities are,4,5 peaking at over 90% in patients with Gross Motor Function Classification System (GMFCS) level V. 6 Also the probability for progression of the deformity is higher. 5 These patients although presenting with high muscle tone in the extremities typically have a relatively low tone at the trunk. Tone assessment requires testing resistance against fast movements, which is impossible for the trunk and hence there are no reports in the literature. 7 The clinical impression of low trunk tone results from the floppy posture which deteriorates with muscle relaxants. The result is a collapse of posture in either the frontal plane (scoliosis), the sagittal plane (kyphosis) or a combination. 7 Some of the patients realise this deficit and use their arms to hold themselves up. Other patients most probably perceive this lack of stability and react with an increase of tone which is called spasticity. Unfortunately, it is impossible to objectively assess such a reaction as these patients are non-communicative and cannot be asked about their sensations and feelings. However, some patients grasp their spinal brace first after getting up to gain stability.
This article was conceived by the neuromuscular and spine study groups of the European Paediatric Orthopaedic Society based on the presentations of the authors given at the society's 37th annual meeting in Tel Aviv, Israel (05 April 2019) in a two-hour focus session on cerebral palsy and associated spine deformities.
Natural history
Natural history of spinal deformities is described as beginning below the age of ten years. During the growth periods progression is faster 5 but a view on the aetiology is missing. Understanding the reasons and causes, however, provides a rationale for prevention and adequate treatment. The condition of low tone, poor sensory information and poor motor control makes it difficult to hold the relatively rigid thorax over the highly mobile lumbar spine. As a consequence, the trunk bends. 8 It can be erected voluntarily by some patients but they are unable to keep this position over time. Finally, the time spent in the deformity influences bone growth and formation. According to the law of Volkmann 9 and Hueter, 10 bone grows less under pressure and more under tension. Thus, with time the initially functional deformity becomes structural. The consequence is a bow at the thoracolumbar junction which can be considered as the typical curve (Fig. 1), the curve being long C-shaped or short. Pure thoracic curves in contrast require either a very supple thoracic spine or they may have another aetiological cause. Restrictions of hip movement as another cause are discussed in the paper ‘Spine deformities in patients with cerebral palsy the role of the pelvis’ in this issue.
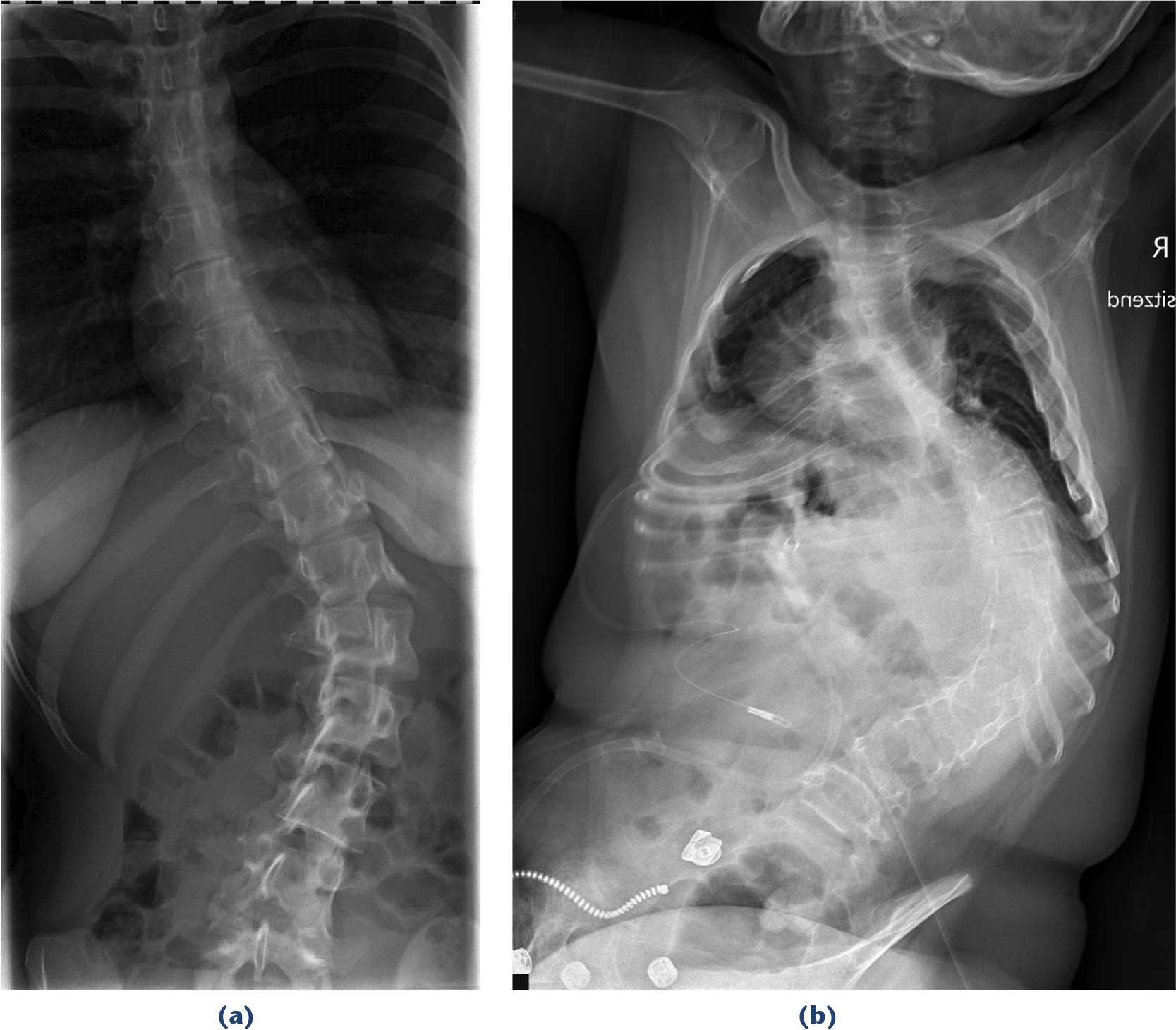
Typical scoliotic curves in cerebral palsy:
Beside the development of a structural deformity, functional impairment is another consequence. This problem increases when the spine becomes deformed and control is even more challenged. Trunk control has been identified as a central point for gross motor function. 11 Impeded trunk control results in poor head control and limited bimanuality. Providing stability has been shown to improve these functions especially in patients at GMFCS level V.12,13 The Trunk Control Measurement Scale has been developed to objectively assess the impairment of trunk control. 14 Checking sitting stability without a push of the arms is one item which we use as a simple and fast clinical test (‘hands-up test’; Fig. 2). If the trunk collapses with the arms raised, we see an indication for treating the instability even without the presence of any spinal deformity.

Collapsing trunk when hands are lifted (‘hands up-test’).
As gravity plays an essential role, spinal deformities should be assessed under load. Usually radiographs are taken standing for adequately measuring spinal deformities. This is difficult in children and patients who are not cooperative, and impossible in patients who are unable to stand. In these cases, radiographs are performed sitting but upright. Any deformity still allows movement into either direction, increase or decrease. The more the patient is lacking posture control, the more he/she will fall into a position of maximal flexion. For this reason, the curve usually presents more severely than the true structural deformity and the amount of correction is usually large. With increasing age and stiffening, however, the correction becomes more limited. 8
Treatment
Treatment in general must focus on the two major problems: dynamic instability and spinal deformity. Dynamic instability is the inability to keep a stable trunk position. Gravity pushes the heavy upper part of the body down which goes along with curved positions of the spine. Even more difficulties occur when the heavy and poorly controlled head is moved or the arms are stretched out for grasping objects. The posture collapses in an unpredictable way for the patient which impedes head control and arm function. Finally, the lack of posture control even when sitting delays functional development due to restricted function. Whereas treating functional instability is still an issue, there is little discussion that treatment is required once a spinal deformity has developed. The method, conservative or surgical, may be discussed. In any case, the aim is to achieve the best correction possible in order to prevent pulmonary and cardiac restrictions at the long term.
Two principally different devices are used for conservative management: adapted seats or seating shells and spinal braces (Fig. 3). 15 Seating shells are attractive as handling is easy; the patient is placed into a system of lateral trunk supports which is completed with straps and vests especially in very unstable patients. The patient looks well controlled and stably fixed in this seat. The question is, however, in how far such devices fulfil the requirements for stability and correction of the deformity. Certainly these devices avoid a major collapse. 16 On the other side, the patient is fixed to the back of the seat. When grasping objects, we normally move our trunk forward and reach with our arms. When active we take a true upright or slightly bent forward posture. For a patient in a seating shell a change of position is not possible without losing the necessary support: he/she either remains fixed in the seat or loses stability and correction. A device which accompanies the body is more appropriate. The second aim, correcting a deformity, is mostly an illusion. Radiographs performed out of and in the seating shell show the same amount of curve (Fig. 4). The shells are adapted for any clothes but thick winter clothes are only worn for transportation outside. With only in-house clothes the supports are far from the body and unable to provide the necessary push for correction. Again, a device with a tight body contact is superior.
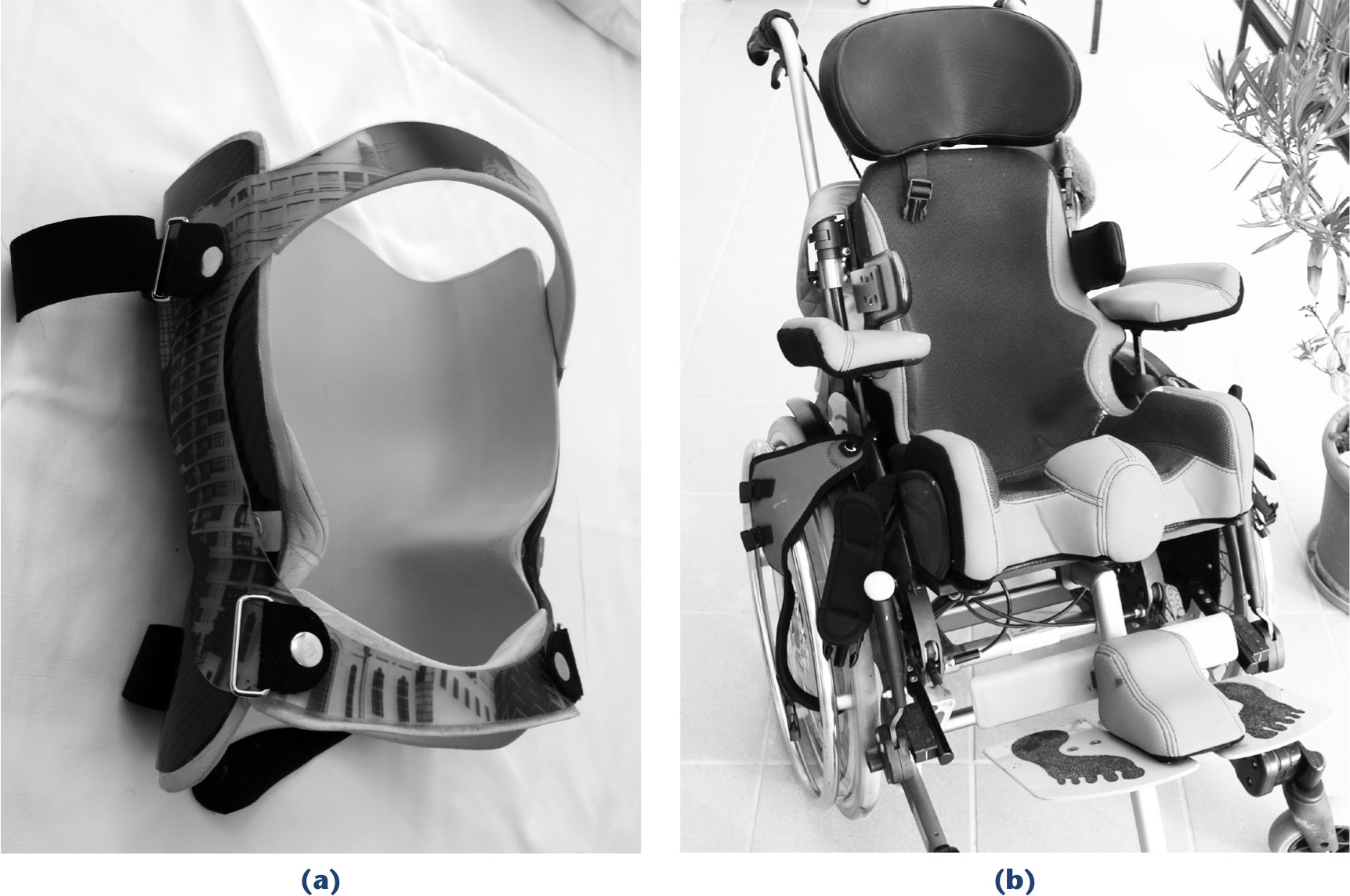
Tools for trunk control:
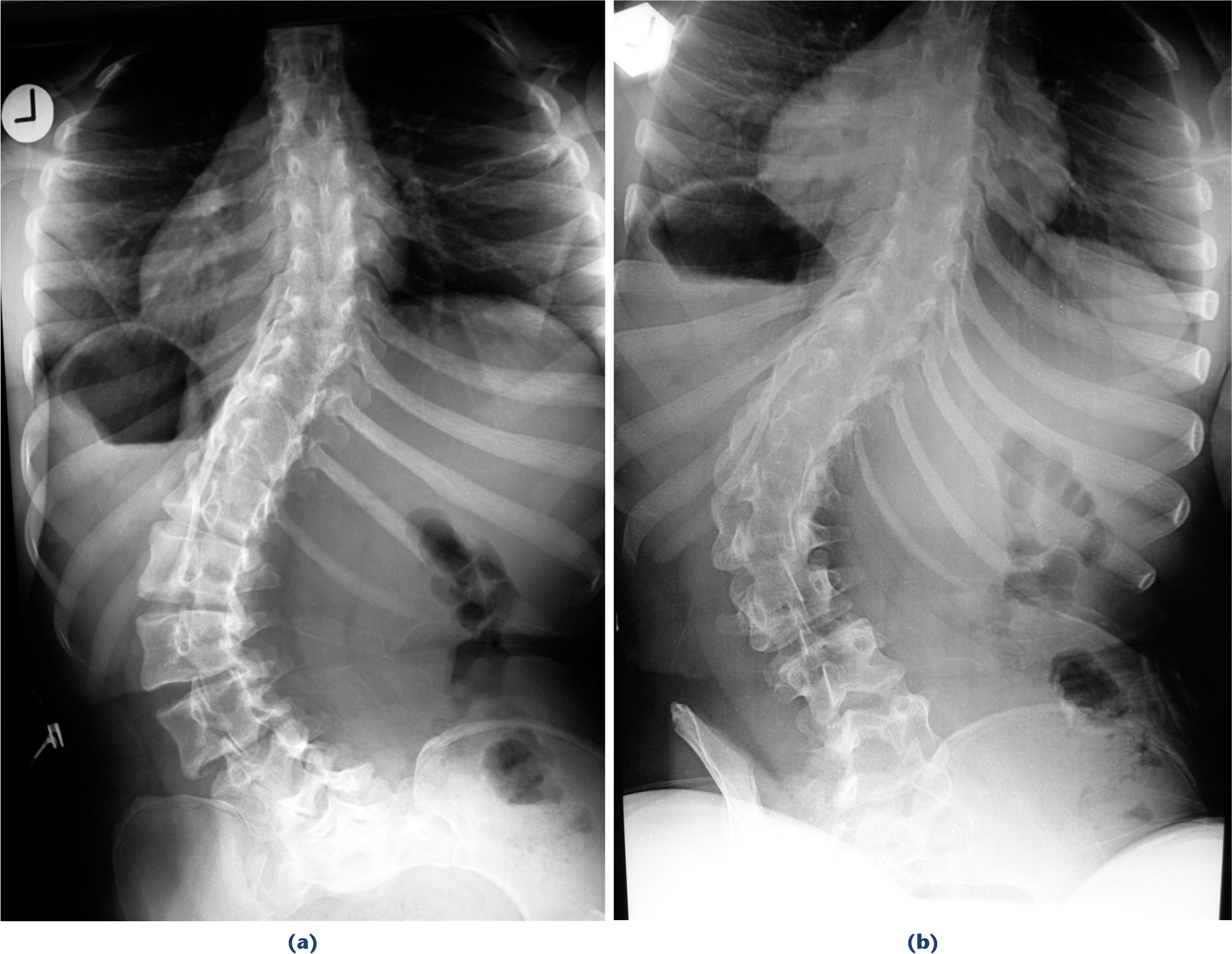
Correction by adapted seating shell: sitting
As a consequence, we prefer a corset which applies the necessary corrective forces independent from trunk position and postural device. Spinal braces on the other side are more difficult to handle and have a poor reputation. Optimal correction with braces can be obtained as long as the curves are flexible 8 (Fig. 5) although the proof for prevention of deterioration in the long-term is lacking.7,13,17,18 Efficacy and acceptance of a brace greatly depend on construction and use. Both but especially the construction are hardly ever described in publications, and reports on poor acceptance and efficacy thus need to be regarded very critically. As the main cause for instability and deformity is poor trunk control under load, we use the braces only when the trunk of the patient is in an upright position. This reduces the wearing time greatly and also the risk for important muscle atrophy. The second and very critical point is the construction. While patients with idiopathic type scoliosis can move in the brace and change position, and this way can avoid pressure at the same spot for a long time, patients with cerebral palsy and poor trunk control cannot. Using a corrective device which is built up from a mould which is modified by adding pressure imbedding is difficult for patients with cerebral palsy. We have changed our moulding technique: we best correct the deformity usually by having the patient lying on a roll below the convexity of the deformity (Fig. 6). We take the mould and do not modify it. Such braces usually fit without pressure sores. We use a very rigid posterior shell which provides all stability and does not close more than 180° in order to ease getting the patient into the brace. It is completed with an anterior shell which is widely open to avoid any pressure on the belly. Reflux is a very common problem in these patients and may be provoked by pressure on the stomach. The fit needs to be very tight at the pelvis but not at the thorax in order to leave space for respiration. Further we apply a prominent contour of the waist as the brace must not slip up. There is usually no problem for providing only stability but the more pronounced the curve is the more it becomes difficult to apply a corrective brace. Braces are increasingly less tolerated the more severe and the stiffer the curve is. 19 One reason can be seen in the fact that in these severe deformities the brace needs to carry the weight of the upper body in a situation where there is no movement between trunk and brace. Even a very soft imbedding and optimal contouring of the plastic shell does not solve this problem anymore in severe curves. The only alternatives are surgery or avoiding gravity which means to avoid any upright position.
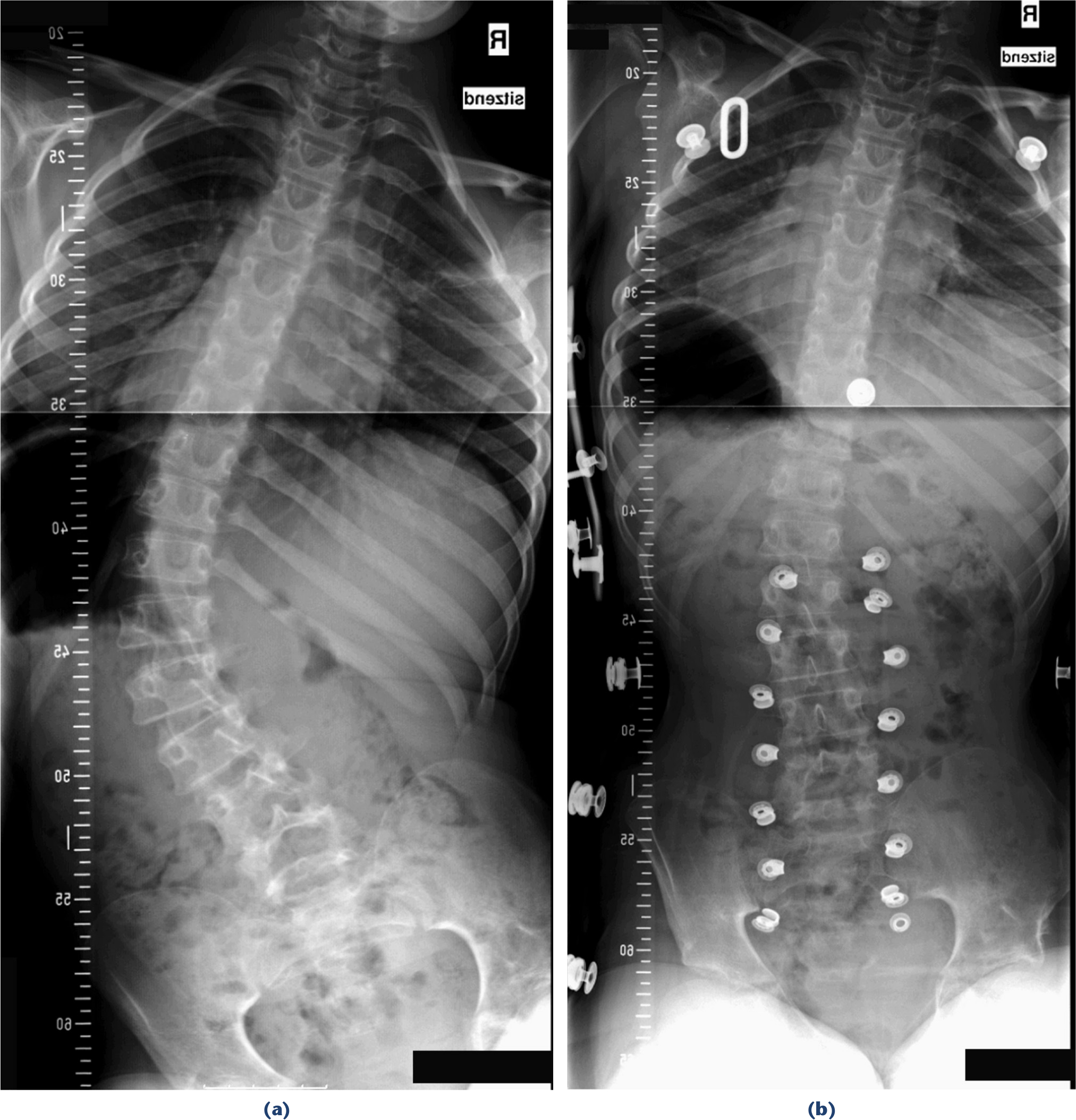
Typical correction by bracing: sitting

Moulding technique:
Braces for sagittal deformities are far more difficult. Hyperlordosis would require pressure from the front which is never accepted. Patients have difficulty eating and problems with reflux if the brace is worn for longer during the day. Treating thoracic hyperkyphosis works only a little better. Avoiding the compensatory lumbar lordosis and in this way forcing the patient to actively correct his posture does not work in patients with loss of trunk control. The brace must apply the corrective forces, and this is especially difficult at the upper sternum. If the brace is not worn tightly the patients slips down within the brace which then may even press against the throat. We have become disillusioned with conservative treatment of sagittal plane deformities in contrast to scoliosis.
Another obviously critical point is the duration the brace is worn. Indeed, information is usually poor and not reliable. It is certainly true that corsets are used much less then prescribed, especially at home. This issue is a major weakness of conservative treatment in our opinion as corsets made from a cast seem to be more efficient; they cannot be taken off. We try to explain the reason and the need for consistency of brace treatment to all involved persons as best as possible and hope that understanding helps acceptance of the treatment. It may be eased further as the brace is only needed when the trunk is upright, and thus for only part of the day and not at night. We must accept, however, that many cases do not make full use of the brace treatment and despite this there is still the potential to avoid early and repetitive spinal surgeries in very young patients.
Conclusion
Lack of trunk control leads to collapse of the trunk under load in upright position. The result is functional impairment of head control and upper extremity function, especially bimanuality. Frequent malposition in the same direction leads to growth asymmetry which results in fixation and progression. Corsets show an indication for functional trunk instability and spinal deformity. They are superior to seating shells. The effect, however, is limited in the long term as they are hardly ever used as required. Treating sagittal plane deformities is even less efficient.