
Abstract
Background
Patients with spinal cord injury without radiographic abnormality (SCIWORA) are prone to develop spinal deformities. The purpose of this study is to report on the clinical and radiological features of post-SCIWORA spinal deformities.
Methods
Four patients with SCIWORA and spinal deformities requiring surgery were analyzed clinically and radiographically.
Results
All four SCIWORA patients developed progressive neuromuscular scoliosis. There were 2 males and 2 females. The mean age at spinal cord injury was 3.9 years (range 6 months to 7 years). Spinal deformity was first noticed at a mean of 17 months after their initial injury (range 9 months to 2 years), and surgical intervention was performed at a mean of 6.5 years following their injury (range 4–11 years). The mean preoperative curve was 54° (range 50–62°). The mean postoperative curve was 9.5° (range 5–16°). The level of injury was T5 in two patients, and T10 and L2 in one patient each. All but the lumbar level injury patient had complete paraplegia. One patient with complete injury (T10) and another with incomplete injury (L2) improved neurologically and were able to walk with the aid of orthoses and crutches. Pelvic obliquity improved in all patients following spinal reconstruction surgery, and none of the patients required additional surgery for spinal deformity. The mean postoperative follow-up was 51.75 months (range 24–93 months).
Conclusions
Long scoliotic curves extending to the pelvis should be expected in SCIWORA. Early intervention may prevent severe deformities. Modern instrumentation techniques employing pedicle screws provided satisfactory correction, improved hip subluxation, and did not adversely affect the ambulatory ability or functional level of the patients in this series.
Introduction
Spinal deformities often accompany neurological and muscular pathologies, such as cerebral palsy, myelomeningocele, poliomyelitis, muscular dystrophies and spinal cord injury [1]. Axial muscle imbalance and/or weakness are recognized as the causes of spinal deformities in these disorders [1]. These disorders include a wide variety of etiologies, pathogeneses, natural histories and associated disorders [3]. However, the rarity of some of these disorders, such as spinal cord injury without radiographic abnormality (SCIWORA), has prevented the creation of a large patient series with long-term follow-up.
It is known that SCIWORA patients are prone to developing spinal deformity [2]. The incidence of deformity is directly related to the level of neurological status, and most of these deformities require surgical intervention. Thus far, SCIWORA deformities have been classified as neuromuscular deformities, but to the best of our knowledge, curve characteristics and the surgical features of those that require surgery have not been clarified.
This study analyzes the structural features and the surgical details of post-SCIWORA spinal deformities in a small group of patients who had their SCIWORA episode early in life and whose secondary spinal deformities were treated surgically during childhood or adolescence. Our objective is to contribute to a better understanding of post-SCIWORA spinal deformities and the results of treatment.
Materials and methods
Between 1997 and 2006, four patients were diagnosed with post-SCIWORA spinal deformities at our institution. The inciting injuries were motor vehicle accidents in all patients, and the mean age at injury was 3.9 years (range 6 months to 7 years). Two of these patients were male and 2 were female.
Results
All four SCIWORA patients developed progressive neuromuscular scoliosis. There were 2 males and 2 females. The mean age at spinal cord injury was 3.9 years (range 6 months to 7 years). The spinal deformities were noticed either by the family or during routine follow-up by the attending physician after a mean of 17 months after their initial injury (range 9 months to 2 years). The level of injury was T5 in two patients and T10 and L2 in one patient each. All but the lumbar-level injury patient had complete paraplegia. Pelvic obliquity was observed in all patients with pelvis tilted to the concave side of the curve. Surgical intervention was performed at a mean of 6.5 years following the injury (range 4–11 years). During surgery the mean age was 10.8 years (9–13 years). All of the patients were treated with posterior spinal fusion (PSF) and segmental spinal instrumentation (SSI) including pelvic fixation. The mean preoperative curve was 54° (range 50–62°). The mean postoperative curve was 9.5° (range 5–16°). One patient with complete injury (T10) and another with incomplete injury (L2) improved neurologically and were able to walk with the aid of orthoses and crutches. Pelvic obliquity improved in all patients following spinal reconstruction surgery, and none required additional surgery for the spinal deformity. The mean postoperative follow-up was 51.75 months (range 24–93 months).
Case 1
A seven-year-old female was admitted to our hospital after a motor vehicle accident with inability to move her legs. Her physical exam demonstrated paraplegia at the T5 level. Routine spinal radiographs did not reveal any evidence of a fracture or dislocation. Magnetic resonance imaging (MRI) showed no abnormalities. No recovery of function occurred. When she was 13 years of age, she was again seen at our clinic with a 62° right thoracolumbar kyphoscoliosis between T5 and L2. Her left hip was laterally subluxated with a Reimers migration index of 30%. Pelvis was tilted with left side up, with an obliquity of 10°. Surgical intervention was recommended. Posterior spine fusion (PSF) and segmental spinal instrumentation (SSI) between T2 and the pelvis was performed, including two posterior chevron osteotomies between T12 and L2. At 7 years postoperatively, her deformity correction was well maintained with a coronal Cobb angle of 7° and a level pelvis. No neurological improvement occurred, and bowel and bladder incontinence persisted. An AP pelvic radiograph showed no evidence of hip subluxation.
Case 2
A 3 year old female was involved in a motor vehicle accident. Her parents stated that after the accident she was paraplegic and hospitalized in an intensive care unit for 2 months. At 7 years of age she was seen at our facility. Spinal radiographs showed no signs of a previous fracture or dislocation. An MRI was not performed. She had not received any medical or surgical treatment since the accident. At 5 years of age, her parents recognized a spinal deformity. On radiographic evaluation at our facility, she had a 50° right thoracolumbar scoliosis between T9 and L3 with the apex at L1. There was an additional compensatory curve between T2 and T8 with a magnitude of 40°, as well as a pelvic obliquity of 25°. She had complete paraplegia below T5 and was nonambulatory, using a wheelchair for mobility. Surgical intervention was recommended. She underwent a PSF and SSI between T2 and the pelvis with pedicle and iliac screws at 8 years of age. The spinal deformity and pelvic obliquity significantly improved. She was discharged without any complications. Radiographs at last follow-up (24 months) showed no evidence of hip subluxation, and the deformity correction was well maintained with a coronal Cobb angle of 10° between T9 and L3.
Case 3
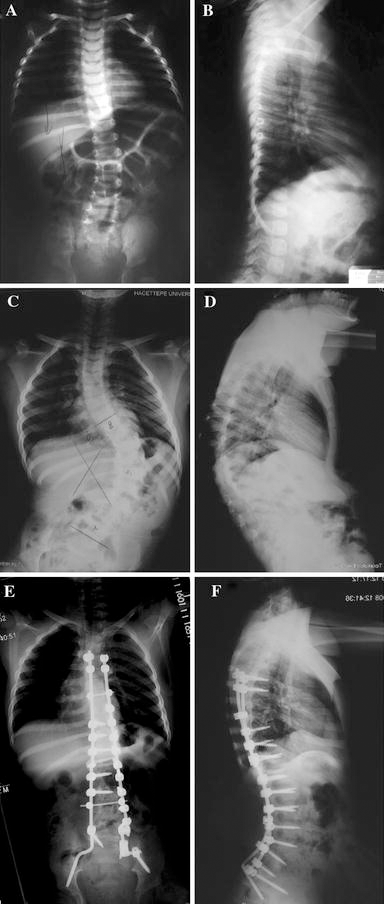
A 6-month-old male with an inability to move his lower extremities after a motorcycle accident was seen at our institution's emergency room. He had been an unrestrained passenger sittting on his mother's lap. No other injuries were detected. Imaging studies, including spinal radiographs and MRI, did not reveal any fractures or spinal cord abnormalities. Neurological examination demonstrated paraplegia at the T10 level. At follow-up at 15 months of age, his neurological status improved. Standing could be achieved with assistance and bowel and bladder control were maintained. However, the left hip was subluxated. It was operated on several occasions at our institution using different procedures, including external oblique tendon transfer, Pemberton osteotomy, proximal femoral osteotomy, and others, but concentric reduction of the femoral head in the acetabulum could not be maintained because of concomitant abductor weakness. The scoliosis progressed to 50° between T8 and L5 by 12 years of age (Fig. 1a–f). He had 25° of pelvic obliquity. The spine deformity was managed with a PSF and SSI between T4 and the pelvis with pedicle and iliac screws. Postoperatively, even though the hip subluxation persisted, femoroacetabular congruencey improved. Pelvis obliquity was completely corrected. Spinopelvic instrumentation did not alter his walking capacity. Three years postoperatively the correction of the spinal deformity was well maintained at 16°, and he was able to walk with orthoses and crutches.
Case 4
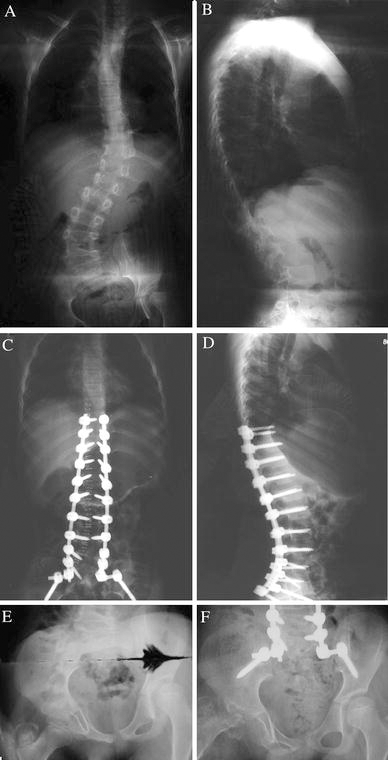
A 5-year-old male was admitted to our emergency room after a motor vehicle accident with a right femur distal physeal fracture and right frontoparietal skull fracture. Cranial computed tomography (CT) did not reveal any intracranial pathology. The skull fracture was treated conservatively, whereas the right distal femur fracture was managed by open reduction and internal fixation. On his initial examination, he was not able to move his right lower extremity, his left lower extremity was paretic, and the neurological level was L2. Although no bony or disk abnormality was detected on the conventional spinal radiographs and MRI (Fig. 2a–b), focal signal intensity was observed at the right anterolateral portion of the spinal cord at the level of the T11 vertebra (Fig. 2c). Additionally, a lumbar epidural space occupying lesion was identified on the axial MRI at L2, pushing the conus to the right with a mass effect (Fig. 2d). Although the level of this space occupying lesion did not explain the clinical findings, L2–L3 laminectomy was performed by the neurosurgery team, intraoperatively the lesion was identified as a pseudomeningocele, and the dura was repaired. After completing the rehabilitation program, the right side did not improve but the left lower extremity gained full muscle strength. We categorized the patient as SCIWORA with severe partial cord involvement, according to Pang [9]. The patient could walk inadequately with a KAFO. He maintained bowel and bladder continence. A spinal deformity was recognized 2 years following injury. Radiographs demonstrated 30° of pelvic obliquity with a concurrent left acetabular dysplasia. At follow-up at 4 years post-injury, the deformity was observed to have progressed. He had a 52° right lumbar curve between L2 and L5 and a 40° left thoracolumbar curve between T9 and L2. His pelvic radiograph showed a right greater trochanteric avulsion fracture. The patient did not recall an apparent trauma to the hip, but as that leg had a plegic history of trauma it could not be ruled out. Since the association between greater trochanter avulsion fractures and femoral head avascular necrosis has been well described in the literature [4–6], the potential outcome of this injury was discussed with the family. Surgery for spinal deformity was not deferred because of the avulsion fracture. A PSF and SSI between T9 and S1 was performed using pedicle and iliac screws (Figs. 3a through 3f). Complete three-dimensional correction was achieved by multiple lumbar chevron osteotomies, all pedicle screw fixation, and direct vertebral rotation maneuvers. After the pelvis was leveled by the spinal deformity correction, the left hip subluxation spontaneously reduced and no change was noted on the right hip. At 67 months postoperatively the correction was maintained with Cobb angles of 5° for both curves with a level pelvis, but changes secondary to avascular necrosis of the right femoral head were visible. The patient had no complaints related to the deformed femoral head since this is the paralytic side. No further treatment was recommended for the femoral head deformity. The patient could still walk with a KAFO and spinopelvic instrumentation did not negatively affect walking capacity.

Discussion
Although similar clinical entities have been reported previously, SCIWORA was first defined with its acronym by Pang and Wilberger in 1982 as “objective signs of myelopathy as a result of trauma, whose plain films of the spine, tomography, and occasionally myelography carried out at the time of admission showed no evidence of skeletal injury or subluxation” [7]. SCIWORA is often caused by severe trauma such as a motor vehicle accident, a significant fall, a sports injury, or child abuse. Differential stretch, vascular injury and concussion are some of the theories that have been proposed to account for the etiology [8, 9]. Normal radiographic findings make the diagnosis challenging [10, 11]. There are some unique characteristics in pediatric patients that have been proposed to explain the higher incidence of SCIWORA in this age group. Horizontal orientation of the facet joints (especially in the upper cervical spine), anterior wedging of the superior aspects of the vertebral bodies, weakness of the paravertebral muscles, and the elasticity of ligaments and joint capsules are some of the features of the pediatric spinal column that predispose to SCIWORA [7, 8, 11, 12]. During trauma, the cord cannot bear forces like the bone and soft tissue. Also, the larger head–body proportions render younger children vulnerable to stretch injuries [9].
With the expanded use of MRI in neurologically injured patients with normal radiography and CT, the term SCIWORA became more uncertain. Pang [9] included spinal cord injuries with extra- and intraneural pathologies detected on MRI as SCIWORA. Extraneural abnormalities include injuries to the ligaments, muscles and the disk. Intraneural abnormalities include injuries to the cord and can be classified into 5 groups: complete disruption of the spinal cord, major cord hemorrhage involving more than 50% of the diameter of the cord, minor cord hemorrhage involving less than 50% of the axial diameter of the cord, edema only, and no abnormality (35% of all cases). In Pang's series, the cases with no intraneural abnormality on the MRI scans demonstrated excellent prognosis, with full recovery of neurological function.
The prognosis depends on initial clinical instability, neurologic features, the age of the child at injury, and MRI findings. Patients who present with complete neurological injury have a poor prognosis. Children younger than 8 years of age experience greater neurologic trauma and consequently a worse prognosis when compared to older children. Normal MRI findings predicate a better outcome. If SCIWORA is diagnosed early, the prognosis can be improved. Launay et al. reported on their meta-analysis that 44% of the patients did not recover and 39% showed a complete recovery [13].
Deformities after vertebral column injuries with or without spinal cord injuries in the pediatric patient population have been well defined [14, 15]. However, questions regarding the incidence and progression of post-SCIWORA deformities have not been studied. Long-term follow-up reports of SCIWORA patients are scarce. Yngve et al. [2] reported that 5 of 7 patients with complete spinal cord injuries without an osseous spine fracture developed late spinal deformity. They did not report the time from injury to the development of the spinal deformity, but noted that 2 of these patients required surgery to correct the deformity. In patients with incomplete neurological injuries, they did not observe any spinal deformity at a mean 3.7 years, but these children were not followed up until skeletal maturity. They noted that spinal cord injury without osseous disruption occurred in younger patients when compared to patients with vertebral fractures, and warned against the development of spinal deformity requiring orthopedic intervention in all immature patients with spinal cord injuries.
In our series of 4 SCIWORA patients, we noticed that the patients were predisposed to developing spinal deformities with long thoracolumbar curves extending to the pelvis. All deformities were greater than 50° preoperatively and associated with pelvic obliquity. All patients were less than 8 years old, and although there was no clinical instability, the neurological status of two patients partially improved while the other two patients remained unchanged. The patients who did not show any improvement both had a neurological level of T5. The 6-month-old male patient had a total lesion which improved significantly during clinical follow-up. The other patient who showed improvement (case 4) had an incomplete lesion which improved partially during the follow-up. The spinal deformities were not rigid and could be easily treated utilizing pedicle screws. When necessary, additional chevron osteotomies were performed to increase flexibility. The correction was maintained during follow-up in all of the patients, and none demonstrated the crankshaft phenomenon. We did not encounter any complications. None of the patients needed extra care preoperatively, perioperatively and postoperatively, which can commonly be the case in other neuromuscular scoliosis patients. These late surgeries did not affect the functional level and walking ability of the patients. After the surgeries, we did not observe any worsening in the patients’ ambulatory capacities, which is in concordance with a previous report on cerebral palsy patients [16]. However, this series consists of only 4 patients, and with the current data it is not possible to reach firm conclusions, but the level of injury and age at injury may be factors related to the prognosis.
Pelvic obliquity may result in secondary hip joint incongruity, and even subluxation. In all cases we observed hip deformity—one with complete dislocation, and three with subluxation. If the hip deformity and subluxation were not advanced, the spinal surgery improved the pelvic balance and hip containment.
PSF and SSI of an immature spine may potentially result in a crankshaft phenomenon, but we believe that correction with pedicle screw fixation minimized this potential risk [17, 18]. We were not able to provide information on the incidence of spinal deformities in SCIWORA patients. We also cannot comment on spinal deformity occurrence in neurologically recovered SCIWORA patients. However, from our limited case series, it appears that once commenced, spinal deformities in neurologically impaired SCIWORA patients tend to progress quickly and require surgical intervention. The high occurrence of pelvic obliquity and hip problems draws attention to early extensive corrective spinal surgery before pelvic deformity develops.
Despite the small number of patients in this series, we believe that the following conclusions can be made. Complete or incomplete neurological deficit following SCIWORA causes deformity in children of 7 years of age or less. Clinically apparent spinal deformity develops within 2 years post-injury. The deformity is generally a large, collapsing thoracolumbar curve that includes the pelvis. Secondary hip subluxation may ensue because of the pelvic obliquity. Unless there is specific pelvic muscle imbalance, leveling of the pelvis resolves the hip subluxation issue. Spinal deformities are not rigid. Posterior facet osteotomies along with the new SSI systems are enough to achieve a full three-dimensional correction, obviating the need for posterior column resection or anterior surgery. In patients with incomplete deficits who can walk with crutches, extending the instrumentation to the pelvis does not impair walking ability. Corrective spinal surgery does not require extra care perioperatively or postoperatively, other than that of general pediatric spinal deformity interventions.
In conclusion, spinal deformities with pelvic obliquity should be expected when following up SCIWORA patients. Early detection of pelvic and hip abnormalities may prevent the occurrence of advanced deformities requiring multiple surgeries. Correction of post-SCIWORA spinal deformities is satisfactory, with modern SSI techniques employing pedicle screws. Surgery for deformity correction does not adversely affect the walking ability and functional level of these patients. SCIWORA patients with neurologic deficits should be followed up closely to check for the development of a potential spinal deformity, and those with spinal deformities should be managed early to avoid curve progression and hip joint subluxation.