
Abstract
Purpose:
This study aimed to analyse the effect of the femoral derotational osteotomy (FDRO) on joint kinematics, kinetics, joint and muscle forces, and muscle moments in patients with idiopathic increased femoral anteversion compared with typically developing children (TDC).
Methods:
In this retrospective study, 17 patients (25 limbs, 13.2 ± 2.2 years, femoral anteversion = 49.0° ± 7.1°) were compared to nine TDC (9 limbs, 12.0 ± 3.0 years, femoral anteversion = 18.7° ± 4.1°). Gait analysis was performed 8.5 ± 7.2 months pre-surgery and 17.3 ± 5.5 months post-surgery. Joint angles, moments and forces as well as muscle forces and muscle contributions to joint moments were analysed using statistical parametric mapping.
Results:
Significant improvements in kinematics (hip rotation, foot progression, knee and hip flexion) were observed pre- to post-FDRO. Joint forces remained unaltered after surgery and did not differ from TDC. Gluteus minimus and deep external rotators muscle forces decreased in mid-stance, while adductor muscle forces increased during stance post-op compared to pre-op. Due to an improved knee extension postoperatively, the rectus femoris muscle force decreased to normal values during mid- and terminal stance. Postoperatively, only the deep external rotator muscle forces differed from TDC.
Conclusions:
This study showed that FDRO can restore muscle forces and muscle contributions to joint moments in addition to normal gait kinematics, while joint contact forces remain within normative ranges. This knowledge might also apply to other conditions in which pathological femoral anteversion is present.
Introduction
Femoral anteversion refers to a twist between the proximal and distal parts of the femur in the transverse plane. 1 The normal degree of anteversion decreases from approximately 40° at birth to 15°–20° during adulthood.2 –4 If increased femoral anteversion does not resolve spontaneously during growth and persists during adolescence, it can be associated with pain or an in-toeing gait pattern and represents a frequent reason for consultation with paediatric orthopaedic clinicians. 5 In detail, increased femoral anteversion has been associated with the severity of hip osteoarthritis, 6 femoroacetabular impingement syndrome,7 –9 the development of overuse injuries, such as patellofemoral pain syndrome,10 –12 and recurrent patellar instability.13,14
From a functional perspective, altered lower-limb kinematics during gait, hip abductor lever arm dysfunction,15,16 as well as high falling frequencies17,18 have been reported. Patients typically present an in-toeing gait pattern with increased hip internal rotation, increased hip flexion and greater anterior pelvic tilt.18 –21 Additionally, some children also present increased knee flexion in mid- and terminal stance.20,22 Modelling different values of femoral anteversion in association with a normal gait pattern has been shown to increase knee contact force (KCF) and hip (HCF) contact forces with increasing femoral anteversion.23,24 By contrast, when patients with increased femoral anteversion walked with their preferred gait pattern, HCFs and KCFs calculated using subject-specific musculoskeletal models did not differ from typically developing children (TDC, i.e. healthy controls with no orthopaedic or neurological medical history). 22 These patients also presented a lower gluteus medius abductive contribution and lower hip-spanning muscle forces compared to TDC. However, walking straight would require higher muscle forces and would lead to larger co-contractions of hip internal and external rotators. 25 In addition, no clinically relevant differences in joint loading were found when patients were stratified according to their gait pattern (i.e. in-toeing, kneeing-in and knee flexed). 22
Most studies suggest surgery as the only possible treatment, and the decision to intervene surgically ultimately depends on the severity of the patient’s symptoms.3,5,26 In addition, several studies recommend 3D gait analysis for surgical planning because of the weak correlations between femoral anteversion measured by imaging methods (CT or MRI) and hip internal rotation during walking.14,18,27 However, only limited studies are available on the effect of femoral derotational osteotomy (FDRO) on gait kinematics and kinetics in children with increased femoral anteversion but without any neurological disorders.28,29 Hamid et al. 29 reported gait improvements in hip rotation and foot progression during gait in patients with increased femoral anteversion after FDRO, as well as in patient-reported outcomes for transfer/basic mobility, sports/physical function, global functioning and satisfaction with symptoms. MacWilliams et al. 28 reported improved gait kinematics and kinetics following FDRO. Post-operative hip rotation was found to be more external in patients than in TDC. The mean foot progression angle during single support improved significantly, while the maximum foot progression during stance remained more inward compared to TDC. 28 Nevertheless, no information is available on how FDRO affects joint loading and muscle functionality.
Therefore, this study aimed to analyse the effect of FDRO on joint kinematics, kinetics and forces, as well as muscle forces and moments, in patients with idiopathic increased femoral anteversion compared to TDC. Based on the improvements reported in the literature, we hypothesised that FDRO would lead to improvements in joint kinematics, kinetics, muscle forces and muscle contributions to joint moments.
Methods
Participants
As part of the standard procedure, in cases of clinically increased femoral anteversion with values >30° in the trochanteric prominence angle test, 30 patients were referred to CT for confirmation and gait analysis to evaluate their gait patterns. Normal femoral anteversion was defined as 15° ± 10°. 31 Patients with CT-confirmed increased femoral anteversion of >30° and who underwent 3D gait analysis pre- and post-FDRO were included in this retrospective study (Level of Evidence III). The exclusion criteria were as follows: age <8 or >18 years, leg length discrepancy >1 cm, any kind of foot deformity, tibiofemoral varus/valgus deformity >5°, adiposity (body mass index >90th percentile), scoliosis, any type of psychomotor or neurological disorder (e.g. cerebral palsy), pathological tibial torsion (<24° or >42° 32 ), and additionally for controls (TDC): pathological femoral anteversion. Frontal plane axis assessment was evaluated by paediatric orthopaedic surgeons during consultation. The use of standing radiographs for further confirmation was at the discretion of the attending paediatric orthopaedist. The cut-off of the mechanical axis deformity of >5° was based on the recommendations of Imhoff et al. 33 The current trial was approved by the regional ethics board (Ethics Committee Northwest Switzerland EKNZ 2021-00015) and written informed consent was obtained from all participants and their legal guardians.
Next, 17 patients were compared to nine TDC functioning as a control group (Table 1). An a priori power analysis (two-tailed, power = 0.95, α = 0.05) 34 revealed a required sample size of 9 and 10 to detect differences within patients based on the pre- to post-operative changes in hip rotation in the data of Hamid et al. 29 and MacWilliams et al., 28 respectively. Therefore, we assumed that the available sample size for this retrospective study was sufficient. It should be noted that some of the included patients were also included in previous work, comparing patients with increased anteversion to TDC.20,22,25 Patients had a pre-operative femoral anteversion of 49.0° ± 7.1° (range: 37°–60°). Normal values of femoral anteversion were confirmed for TDC using existing MRI measurements to limit radiation exposure. Gait analysis was performed at 8.5 ± 7.2 months (range: 0.2–29.7 months) pre-surgery and 17.3 ± 5.5 months (range: 11.1–38.7 months) post-surgery. The age at the time of the FDRO was 13.9 ± 2.0 years (range: 9.8–17.5 years). FDRO was performed at the distal level using an external fixator and at the proximal level using a locking plate for 20 and 5 limbs, respectively. The reported surgical correction was on average 28.1° ± 5.3° (range: 15°–35°). Two wires were inserted perpendicular to the longitudinal bone axis, and the bony segments were rotated. A sterilised ruler was used to control the rotation shown by the angle between the wires. Fixation of the bony segments to the fixing device may result in a tiny rotation to either side. Hence, the intraoperative assessment of rotation is an estimate. All FDROs were performed at the same institute under the lead of the same surgeon.
Mean ± standard deviation (range) anthropometric data and walking speed for patients and typically developing children (TDC).
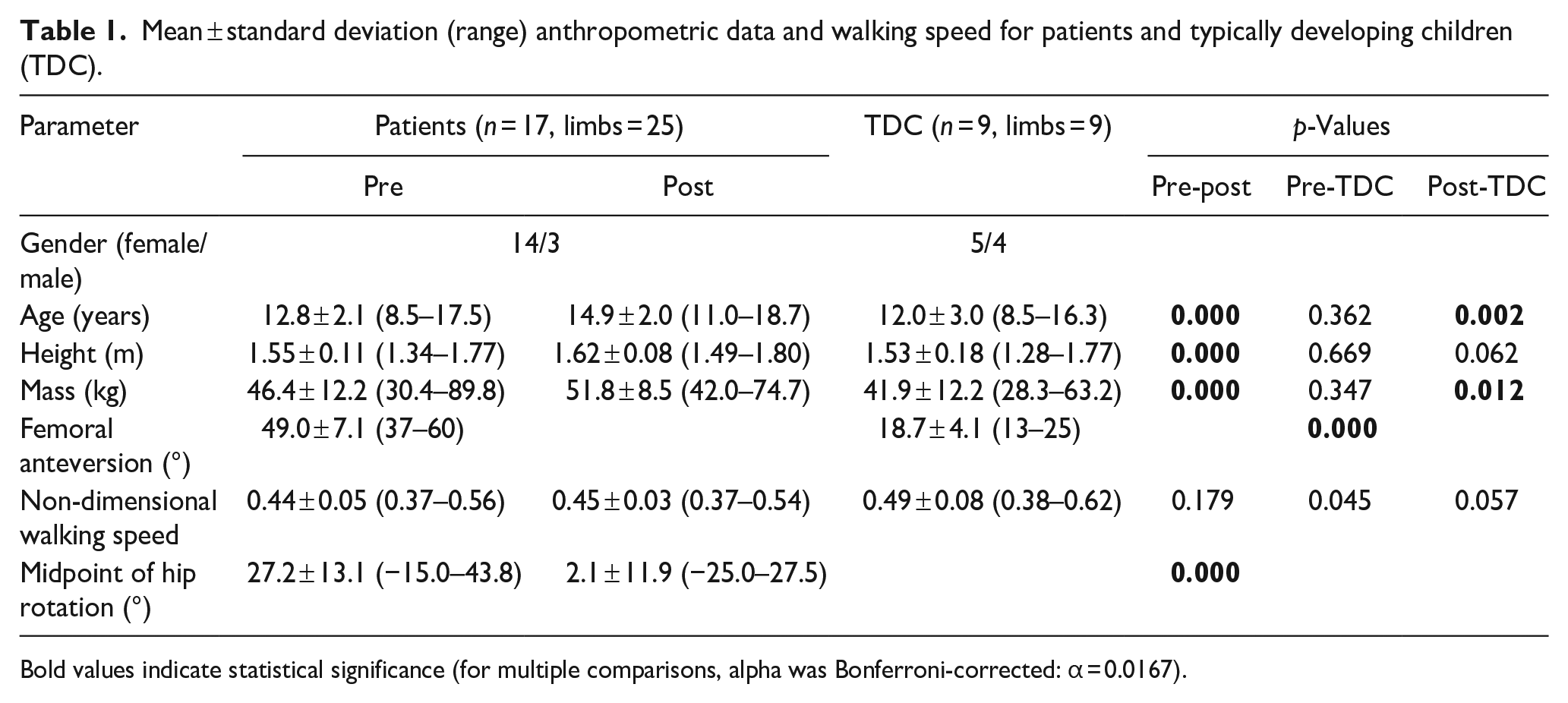
Bold values indicate statistical significance (for multiple comparisons, alpha was Bonferroni-corrected: α = 0.0167).
Data collection
Sixteen self-reflective markers were attached to the lower limbs according to the Plug-in Gait model. 35 The participants walked barefoot at a self-selected speed. Lower limb kinematics and kinetics were collected during gait using a 3D motion capture system (Vicon Motion Systems Ltd., Oxford, UK, 200 Hz) and two force plates (patients: AMTI, Advanced Mechanical Technology Inc., Watertown, Massachusetts, USA; TDC: Kistler Instrumente AG, Winterthur, Switzerland, 1000 Hz). A minimum of three valid gait cycles (GCs) were recorded.
From the clinical examination data collected following gait analysis for patients, the evaluation of passive hip range of motion was used in the current study. Clinical hip rotation is presented as the midpoint of the hip rotational range of motion, which is the midpoint between maximal internal and external hip rotation. 36 If the midpoint is positive, hip internal rotation predominates, whereas for negative values, hip external rotation predominates.
Musculoskeletal modelling
Marker trajectories and ground reaction forces were filtered using a second-order low-pass Butterworth filter with cut-off frequencies of 5 Hz and 12 Hz, respectively, and used as input for an inverse dynamics analysis in the AnyBody Modelling System (AnyBody Technology A/S, Aalborg, Denmark). 37 Personalised models for each subject were created from a detailed generic model of the lower limb, 38 which was based on a cadaveric dataset. 39 The model contains 55 muscle actuators in each leg, discretised into 169 fascicles. The models were scaled to match the overall anthropometric and marker data collected during the static standing reference trial. 40 Muscle strength was scaled according to the mass of each participant. The muscle elements were modelled as constant-strength actuators. The geometry of the femur was morphed to include a transverse rotation between the proximal and distal sections, matching the subject’s femoral anteversion value obtained from the imaging data. 41 No post-operative imaging data were available. Post-operative femoral anteversion was assumed to be the pre-operative anteversion subtracted by the amount of planned surgical correction, which was set according to pre-operative pathological CT anteversion values, clinical findings and gait analysis data.
The hip joint was modelled with 3 degrees of freedom (DoF), while the knee and talocrural joints had 1-DoF. In this model, the subtalar joint was locked because of the limited number of markers on the foot segment. The laboratory reference frame was defined based on the direction of gait, which was defined as the line connecting the positions of the heel marker in two consecutive ipsilateral heel strikes (first axis, anterior–posterior). The second axis (vertical) was perpendicular to the floor, and the third axis (medio-lateral) was perpendicular to the other two axes. Joint kinematics were computed from the measured marker trajectories. The pelvis 39 and foot progression angle (i.e. the orientation of the foot was identified through an axis connecting the heel and the second metatarsal marker) were calculated relative to the laboratory reference frame. 22 Inverse dynamics were performed, and a third-order polynomial muscle recruitment criterion was used to calculate the required muscle forces, resulting joint moments, and contact forces. The hip moments and hip contact forces (HCFs) were calculated in a proximal (pelvis-based) coordinate system. Knee moments and KCFs were computed in an anatomical tibia-based coordinate system. The contribution of each hip-spanning muscle to the net sagittal, frontal, and transversal moments was computed as the product of the force exerted by the muscle times the distance of its instantaneous line of action from the centre of rotation of the joint projected in the plane of interest. 25
Data analysis
Non-dimensional walking speed 42 was calculated. Joint and muscle forces were normalised to body weight (BW), whereas joint moments and muscle moment contributions were normalised to body mass. The reported muscle forces are defined as the sum of the forces generated by all fascicles constituting each muscle. The following muscles were included in the analysis: gluteus maximus, gluteus medius posterior and anterior, gluteus minimus, hamstrings (sum of semimembranosus, semitendinosus and biceps femoris long head), adductors (sum of adductor magnus, longus, and brevis, as well as pectineus and gracilis), iliopsoas, rectus femoris, tensor fasciae latae and deep external rotators (sum of obturator internus, obturator externus, gemellus superior, gemellus inferior, quadratus femoris and piriformis). All waveforms were time-normalised to the duration of the GC from heel strike (0%) to heel strike (100%) of the ipsilateral leg. The first foot strike was on the first plate and was defined when the ground reaction force exceeded 20 N. The second heel strike was detected using the Zeni-algorithm 43 and visually checked using videos. The average trajectories per participant were calculated based on the recorded walking trials.
Statistical analysis
Patient anthropometric data, midpoint of hip rotation, and walking speed were compared before and after FDRO using paired t-tests, and compared against TDC using two-sample t-tests. Temporal profiles were analysed using statistical parametric mapping (SPM; www.spm1D.org, v0.43). 44 Patient data were compared before and after FDRO using the SPM paired t-tests and compared against TDC using SPM two-tailed, two-sample t-tests. The level of significance was set at α = 0.0167 (Bonferroni-corrected α for multiple comparisons) for all statistical tests. For clarity, only statistically significant differences in intervals longer than 3% of the GC duration and those with differences greater than the minimal detectable change were reported. The minimal detectable change was defined based on the standard error of measurement (SEM) using the following equation:

For each interval with significant differences, the mean absolute maximum difference (MaxDiff) is reported. For within-group comparisons, MaxDiff was calculated as the absolute maximum difference between the pre- and post-operative trajectories during this period. For group comparisons (patients versus TDC), MaxDiff was calculated as the absolute maximum difference between the trajectory of each patient and the mean trajectory of all TDC in the significant period. Subsequently, the mean MaxDiff ± standard deviation was calculated for all participants.
Results
The clinically assessed midpoint of the hip rotational range of motion decreased significantly after FDRO. Non-dimensional walking speed did not differ between the pre- and post-operative gait analyses or TDC (Table 1).
Post-operative anterior pelvic tilt (0–9% GC, MaxDiff: 4.8 ± 3.0°; 44%–62% GC, MaxDiff: 5.3 ± 3.0°; 90%–100% GC, MaxDiff: 4.9 ± 3.0°), hip flexion (0%–69% GC, MaxDiff: 9.9 ± 5.7°; 93%–100% GC, MaxDiff: 5.6 ± 3.3°), knee flexion (22%–59% GC, MaxDiff: 8.1 ± 3.9°), hip internal rotation (0%–73% GC, MaxDiff: 10.9 ± 4.9°) and internal foot progression (0%–72% GC, MaxDiff: 9.1 ± 3.8°; 94%–100% GC, MaxDiff: 5.7 ± 3.5°) decreased significantly in comparison to pre-operative values. In comparison to TDC, significant differences in hip flexion (64%–79% GC, MaxDiff: 9.6 ± 4.8°), pelvic obliquity (22%–31% GC, MaxDiff: 4.0 ± 2.4°), hip adduction (23%–34% GC, MaxDiff: 4.5 ± 2.2°) and foot progression (52%–63% GC, MaxDiff: 7.6 ± 3.7°) were found post-FDRO (Figure 1).
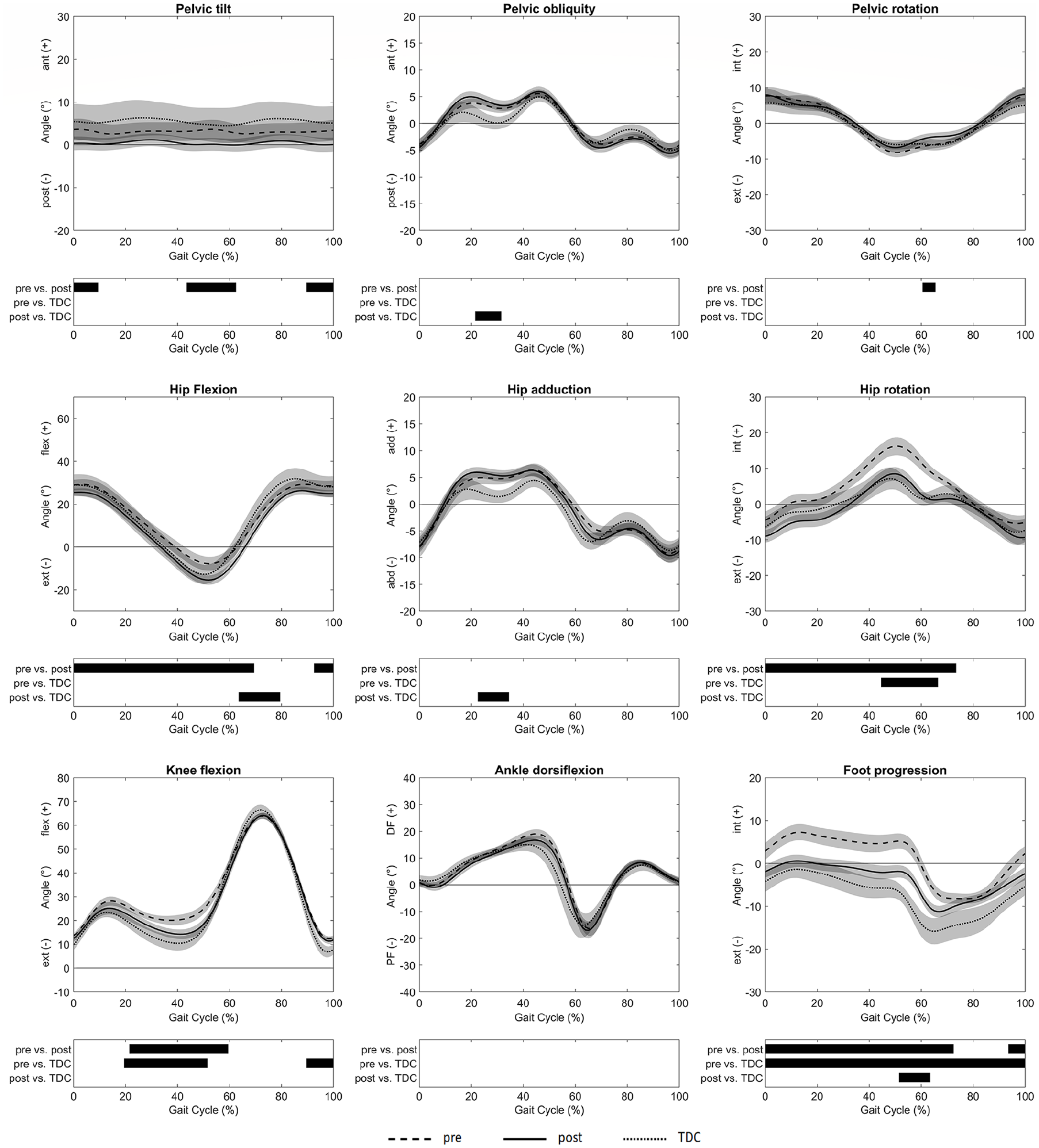
Joint kinematics were reported as mean values and 95% confidence intervals as dashed lines for patients pre-FDRO, solid lines for patients post-FDRO and dotted lines for TDC. The phases of the GC for which a statistically significant difference was found are indicated by black bars for each comparison.
The internal knee flexor moment (40%–49% GC, MaxDiff: 0.18 ± 0.11 Nm/kg) increased significantly post-operatively. Furthermore, the quadriceps force on the patella (37%–51% GC, MaxDiff: 0.69 ± 0.39 BW) decreased post-operatively. No differences between pre- and post-FDRO were found for HCFs and KCFs. After FDRO, joint moments and absolute HCFs and KCFs were comparable between the patients and TDC (Figure 2).
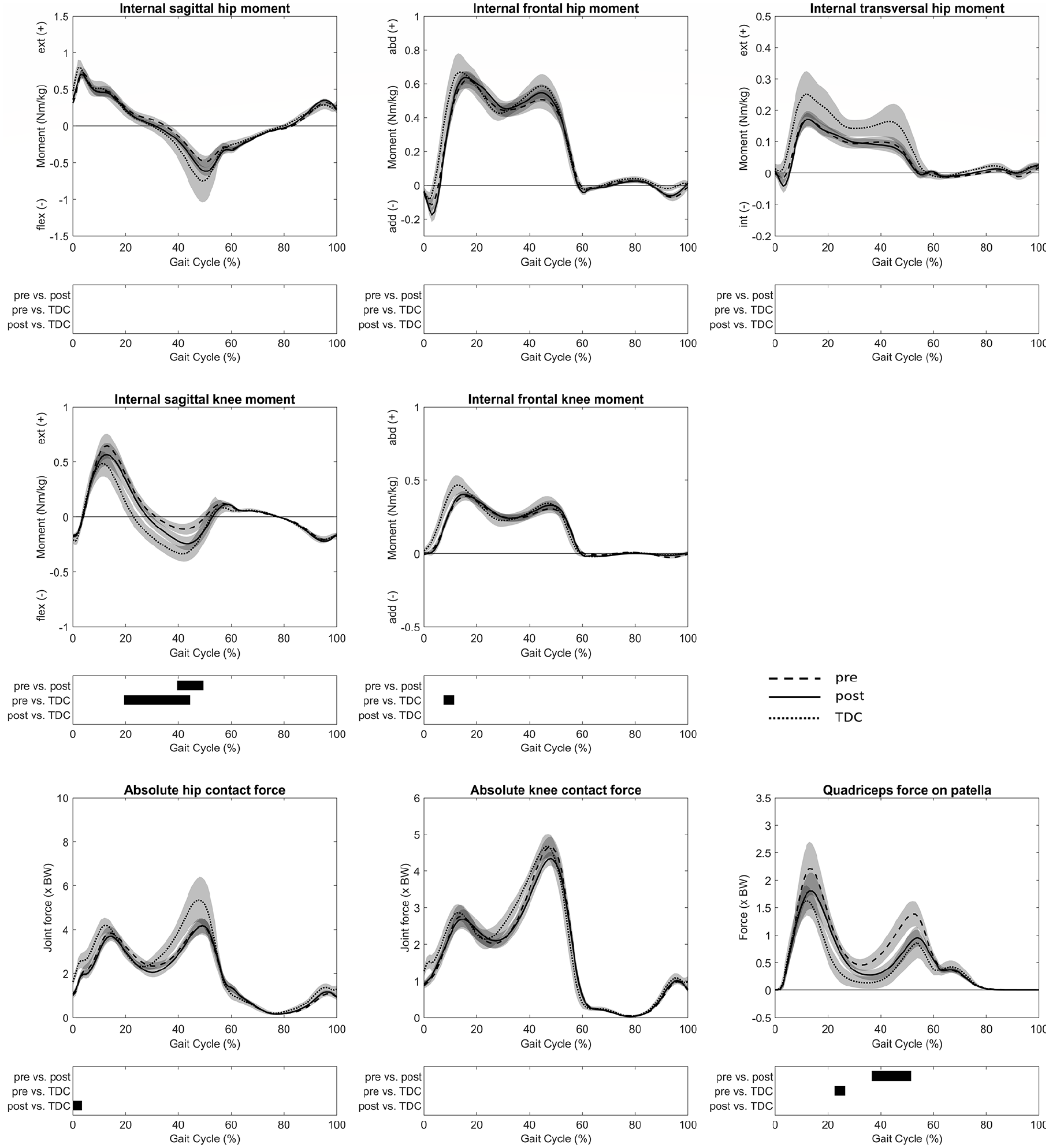
Joint moments and forces were reported as mean values and 95% confidence intervals as dashed lines for patients pre-FDRO, solid lines for patients post-FDRO and dotted lines for TDC. The phases of the GC for which a statistically significant difference was found are indicated by black bars for each comparison.
After FDRO, the gluteus minimus muscle forces decreased in stance (4%–11% GC, MaxDiff: 0.09 ± 0.06 BW; 15%–20% GC, MaxDiff: 0.12 ± 0.06 BW) but increased in swing (61%–69% GC, MaxDiff: 0.08 ± 0.05 BW; 95%–99% GC, MaxDiff: 0.05 ± 0.03 BW) compared to pre-operative values. Adductor muscle forces (10%–18% GC, MaxDiff: 0.13 ± 0.07 BW; 39%–49% GC, MaxDiff: 0.19 ± 0.10 BW) increased, whereas the rectus femoris (12%–32% GC, MaxDiff: 0.25 ± 0.14 BW) and deep external rotator muscle forces (3%–14% GC, MaxDiff: 0.19 ± 0.11 BW; 26%–31% GC, MaxDiff: 0.13 ± 0.08 BW) decreased after surgery. Thus, the deep external rotator muscle forces were significantly lower (27%–44% GC, MaxDiff: 0.40 ± 0.16 BW) post-operatively compared to TDC (Figure 3).
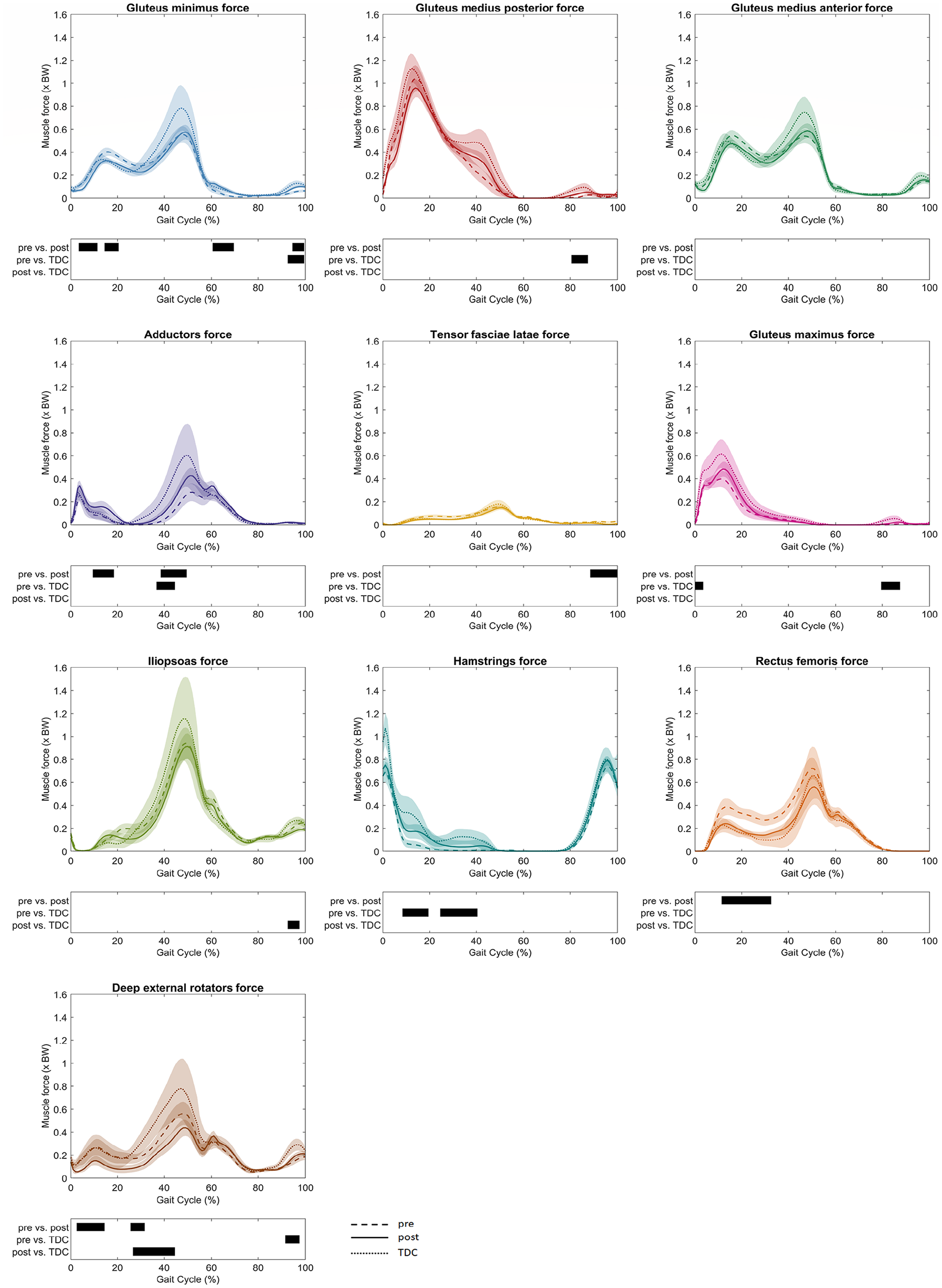
Muscle forces were reported as mean values and 95% confidence intervals as dashed lines for patients pre-FDRO, solid lines for patients post-FDRO and dotted lines for TDC. The phases of the GC for which a statistically significant difference was found are indicated by black bars for each comparison.
Before FDRO, the gluteus medius posterior part provided a significantly larger hip extension moment (2–31% GC, MaxDiff: 0.12 ± 0.04 Nm/kg) than post-FDRO. The patients also presented a significantly lower flexing contribution by the rectus femoris (13%–31% GC, MaxDiff: 0.06 ± 0.04 Nm/kg; 36%–43% GC, MaxDiff: 0.05 ± 0.03 Nm/kg) after FDRO. Furthermore, the adductors’ extending (10%–18% GC, MaxDiff: 0.06 ± 0.04 Nm/kg) and flexing (39%–51% GC, MaxDiff: 0.07 ± 0.03 Nm/kg) contributions increased post-operatively (Figure 4). In the frontal plane, the gluteus medius posterior part (9%–31% GC, MaxDiff: 0.11 ± 0.05 Nm/kg; 40%–44% GC, MaxDiff: 0.09 ± 0.07 Nm/kg) and anterior part (48%–53% GC, MaxDff: 0.08 ± 0.04 Nm/kg; 94%–100% GC, MaxDiff: 0.03 ± 0.02 Nm/kg) abductive contributions to the net frontal moment increased after surgery. At the same time, the adductive contribution by the hip adductors (39%–51% GC, MaxDiff: 0.12 ± 0.06 Nm/kg) increased (Figure 5). The externally rotating contribution to the net transversal moment by the gluteus medius posterior part (8%–44% GC, MaxDiff: 0.05 ± 0.02 Nm/kg) increased, while the externally rotating contribution by the deep external rotators (2%–54% GC, MaxDiff: 0.07 ± 0.03 Nm/kg) decreased after surgery. Furthermore, the internally rotating contributions of the gluteus medius anterior part (4%–48% GC, MaxDiff: 0.03 ± 0.01 Nm/kg) and gluteus minimus (13%–49% GC, MaxDiff: 0.01 ± 0.01 Nm/kg) decreased significantly (Figure 6). After FDRO, significant differences between patients and TDC were found for the gluteus minimus (26%–36% GC, MaxDiff: 0.01 ± 0.00 Nm/kg) contributions to the transversal net moment, while limited differences were observed in the sagittal and frontal planes.
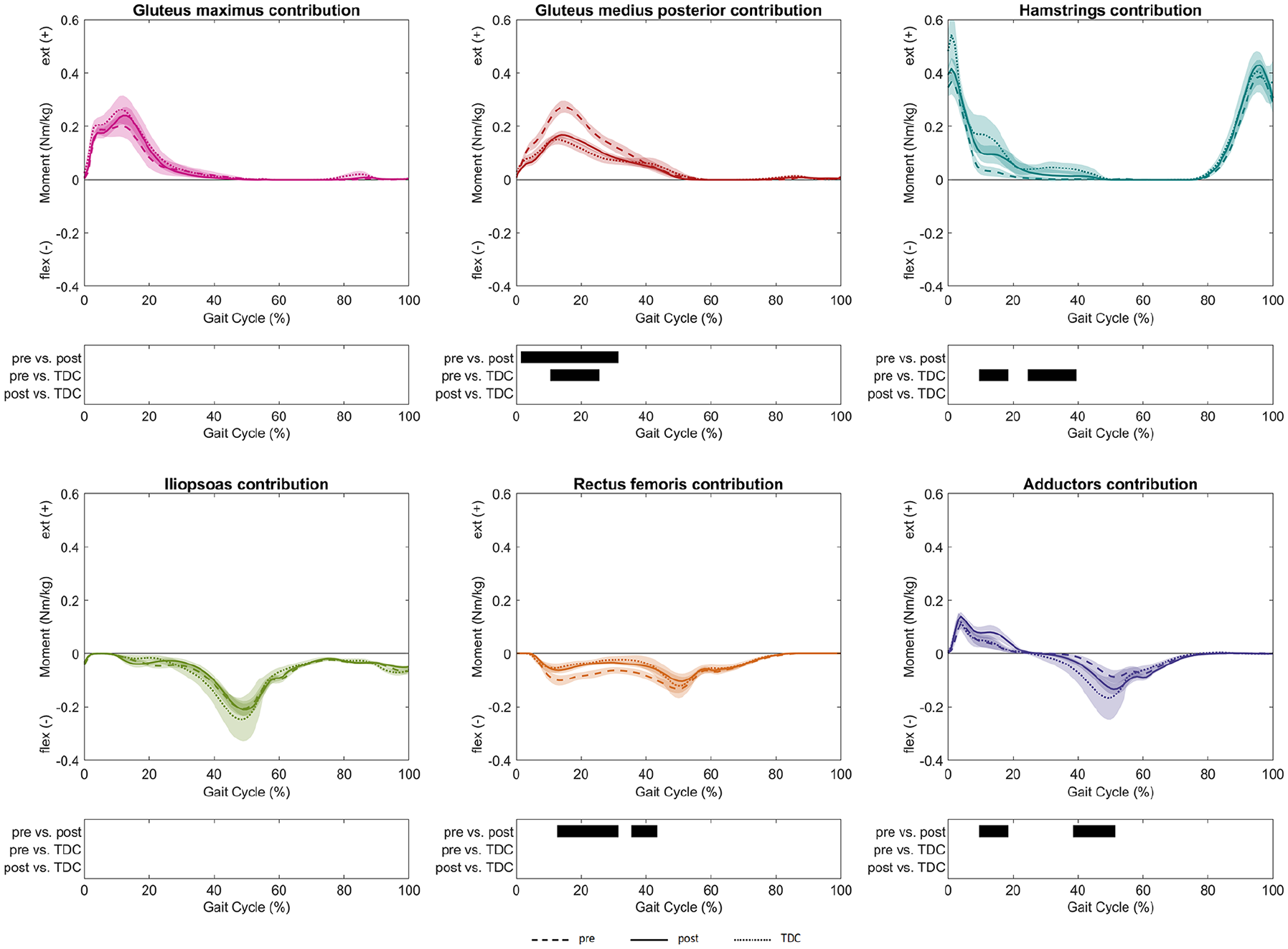
Muscle moment contributions to hip net sagittal moment were reported as mean values and 95% confidence intervals as dashed lines for patients pre-FDRO, solid lines for patients post-FDRO and dotted lines for TDC. The phases of the GC for which a statistically significant difference was found are indicated by black bars for each comparison.
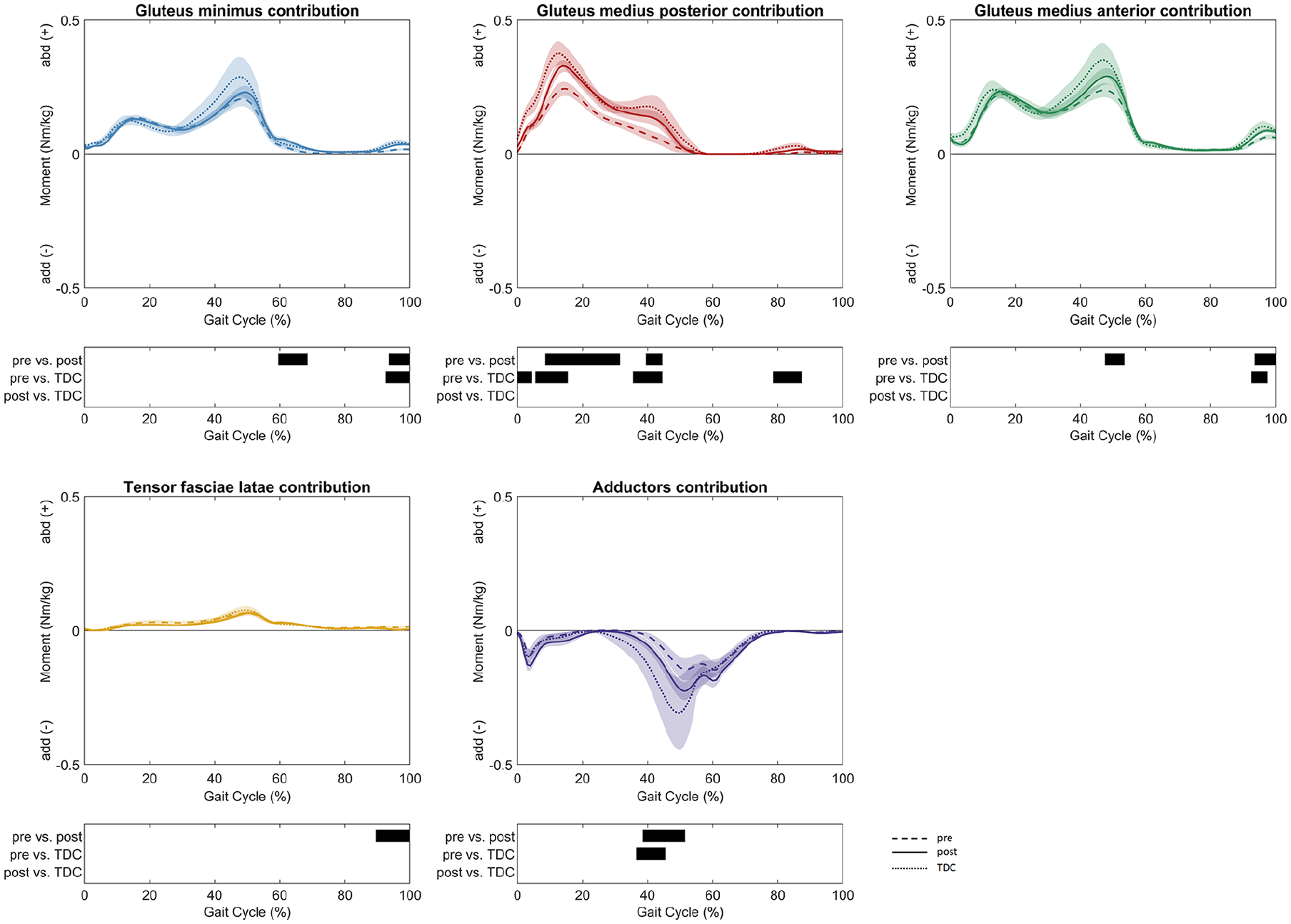
Muscle moment contributions to hip net frontal moment were reported as mean values and 95% confidence intervals as dashed lines for patients pre-FDRO, solid lines for patients post-FDRO and dotted lines for TDC. The phases of the GC for which a statistically significant difference was found are indicated by black bars for each comparison.
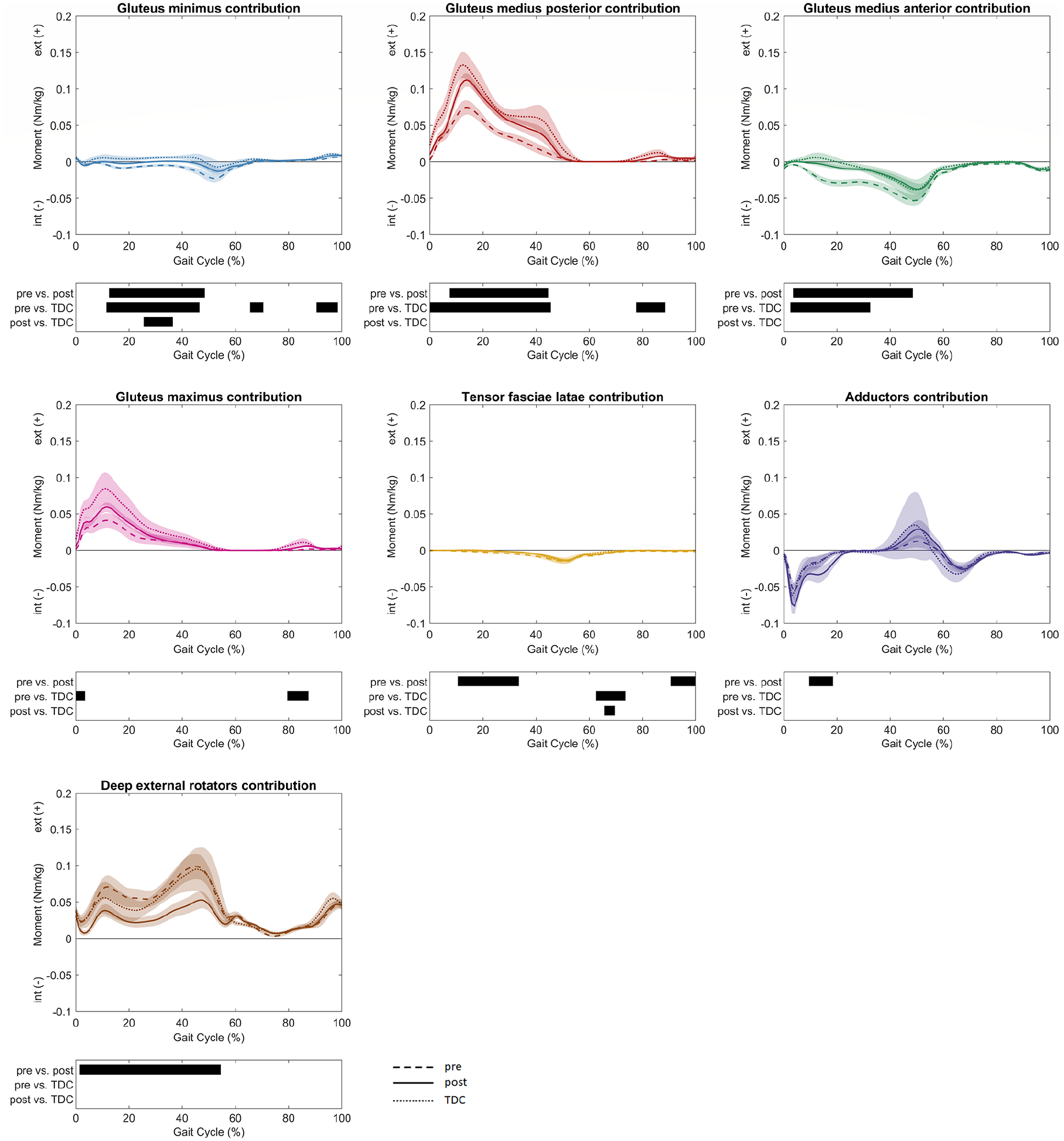
Muscle moment contributions to hip net transversal moment were reported as mean values and 95% confidence intervals as dashed lines for patients pre-FDRO, solid lines for patients post-FDRO and dotted lines for TDC. The phases of the GC for which a statistically significant difference was found are indicated by black bars for each comparison.
Discussion
This study investigated changes in joint kinematics, joint moments, joint forces, muscle contributions to hip joint moments and muscle forces in patients with increased femoral anteversion who underwent FDRO. Post-operative results were compared to pre-operative values as well as TDC. Differences between patients before FDRO and TDC are presented but are not the focus of the current study. We aimed to explore the effect of FDRO by comparing pre- and post-intervention values and to understand whether gait patterns, joint loading and muscle functionality are restored to normative values after surgery. This study could show that FDRO can restore normal gait kinematics, quadriceps force on the patella, as well as muscle forces (except deep external rotators) and muscle contributions to joint moments, while HCFs and KCFs remained within normative ranges. Thus, most of our hypotheses were accepted.
A similar cohort of 42 patients with increased femoral anteversion was previously compared with TDC20,22,25 and presented gait kinematics and kinetics similar to the pre-operative data of the 17 patients investigated in this study. The post-operative kinematic improvements observed in the current study are comparable to those reported in the literature.28,29 We found improvements in the foot progression angle, as previously reported,28,29 but it remained slightly more inward compared to TDC, post-FDRO. Similar to the findings of MacWilliams et al., 28 the clinical relevance of the post-operative differences might be low. After FDRO, patients’ hip internal rotation decreased to normative values. MacWilliams et al. 28 reported an ‘overcorrection’ to increased external hip rotation compared to TDC after FDRO, while Hamid et al. 29 did not show differences in hip rotation post-operatively. A decrease in anterior pelvic tilt was found after surgery, which is in agreement with the findings of MacWilliams et al. 28 By contrast, Hamid et al. 29 did not report changes in pelvic tilt.
Furthermore, the pre-operative increased knee flexion in the terminal stance significantly decreased after FDRO, and no differences to TDC were found post-operatively. This leads to improvements in the knee flexor moment (i.e. increase pre-to-post), as well as the quadriceps force acting on the patella (i.e. decrease pre-to-post), with no difference present post-operatively compared to TDC. In adults, anterior knee pain was associated with increased anteversion but without changes in trochlear morphology or patellar orientation to the femur. 45 For adolescents with symptomatic increased femoral anteversion, FDRO improved both function and pain scales. 46 With increasing knee flexion angles, the patellofemoral compression forces increase47,48 and greater quadriceps forces contribute to larger tibiofemoral and patellofemoral joint loadings. 49 Therefore, the anterior knee pain reported in patients with increased femoral anteversion45,46 as well as its improvements 46 might be related to the knee flexion angles in these patients. Given the retrospective nature of this study, we could not obtain patient-reported outcome measures (PROMs), as done by Stambough et al. 46 Future studies should focus on analysing PROMs in combination with the methods presented in this study to better understand whether the improved gait biomechanics also correlates with PROMs. In such a prospective study, the rehabilitation process may also be thoroughly documented to allow for further conclusions.
It has been reported that FDRO restores the hip abductor moment arm. 50 In the frontal plane, muscle moment contributions became normal or showed a trend towards normal values after surgery, which might indicate that the hip abductor moment arm was restored after surgery. The greatest post-operative differences compared to TDC for muscles were found for deep external rotators. The deep external rotator muscle force decreased significantly from before to after surgery, resulting in lower post-operative values in the terminal stance compared to TDC. The hip net transversal moment remained similar to pre-operative values and was lower, even though only partly significant, compared to TDC. This, in turn, can influence the functional role of the deep external rotators. MacWilliams et al. 28 assumed that the increased hip external rotation after FDRO was due to lingering compensations. The unaltered transversal net moment and resulting deep external rotator deviations found in the current study might also be due to persistent compensations.
As previously reported, patients’ pre-operative KCFs and HCFs were similar to – or at most slightly lower than – TDC. 22 The KCFs and HCFs were not affected by the surgery and remained similar to or lower than TDC. Therefore, altered femoral morphology by itself may not necessarily lead to an increased risk of joint overloading in terms of joint contact forces 22 ; however, the concomitant presence of other morphological deformities (e.g. impingement syndrome7 –9 or altered patellar morphology13,14) and their interplay with increased femoral anteversion may explain some of the clinically observed orthopaedic complications and should therefore be kept in mind in the clinical management of these patients.
The following limitations of this study should be considered. Personalised musculoskeletal models accounting for radiographically measured femoral anteversion values were created for all the participants. Therefore, imaging data must also be available for TDC. No post-operative imaging data of femoral anteversion were available due to the retrospective design of the current study. Therefore, personalised anteversion in the musculoskeletal model had to be estimated based on pre-operative anteversion values and planned surgical correction. Furthermore, the timing between pre-operative gait analysis and FDRO was heterogeneous. This is due to the retrospective design and daily clinical practice, with different amounts of time needed by individual patients and families for decision-making. Overall, we believe that this effect was minimal. An analysis of a larger sample of patients with more homogeneous procedures and TDC is warranted to confirm these findings further. The current study included patients with distal and proximal FDROs. Nelitz et al. 51 performed virtual torsional osteotomies with a 3D computer model, created from CT data of a human cadaver femur and reported that proximal and distal external derotational osteotomies tended to increase varus and valgus angulation, respectively. Nevertheless, Nelitz 52 stated in 2018 that the literature provides no evidence of whether a proximal, mid-shaft or distal osteotomy location is preferable. Furthermore, Niklasch et al. 53 showed that there was no difference in static and short-term gait kinematic outcomes in children with cerebral palsy comparing proximal and distal derotations. With only five limbs corrected at the proximal level, a comparison of the two subgroups was not possible in this study; however, future studies should evaluate this further. An additional limitation lies in the potential impact of frontal plane axis deformation on both kinematic and kinetic parameters. Consequently, individuals with tibiofemoral varus or valgus deformities >5° were excluded from the study. Assessment of frontal leg axis alignment was conducted by paediatric orthopaedic surgeons during clinical consultations, with the option for further confirmation through standing radiographs. However, it is important to note that radiological measurements were not obtainable for every participant in the study cohort. This is due to the retrospective design of the study and the following patients were only exposed to X-rays if there existed clinical suspicion of tibiofemoral varus or valgus deformities. While musculoskeletal modelling predictions have been validated in the past,38,54 further validation regarding femoral anteversion and referring gait patterns is advisable. However, major difficulties in measuring the activity of the deep hip muscles using surface electromyography techniques make further validation of the presented findings challenging. Therefore, the modelling assumptions must be thoroughly discussed. A more extensive discussion of musculoskeletal modelling limitations and assumptions specific to the analysis of patients with increased femoral anteversion and altered gait patterns can be found in Alexander et al. 22 and De Pieri et al. 25
In conclusion, in line with previous studies, we showed that FDRO seems to be a good option for normalising most gait pathologies in patients with increased femoral anteversion. Muscle contributions at the hip level changed to almost normal values by FDRO. When conservative approaches fail, and severe symptoms persist, the altered morphology can be surgically corrected through FDRO. An important result is the improvement of knee extension and the knee flexor moment in terminal stance as well as the rectus femoris muscle force as knee pain is a common issue linked to femoral malrotation. This study aimed to provide information on muscle functionality and how it might be affected by surgery. These results are not only of interest in patients with isolated increased femoral anteversion but might also provide valuable information in other patient groups presenting increased femoral anteversion.
Supplemental Material
sj-pdf-1-cho-10.1177_18632521241269339 – Supplemental material for Effect of femoral derotational osteotomy in patients with idiopathic increased femoral anteversion on joint loading and muscular demands
Supplemental material, sj-pdf-1-cho-10.1177_18632521241269339 for Effect of femoral derotational osteotomy in patients with idiopathic increased femoral anteversion on joint loading and muscular demands by Nathalie Alexander, Johannes Cip, Reinald GH Brunner and Enrico De Pieri in Journal of Children’s Orthopaedics
Footnotes
Acknowledgements
None of the authors has any financial or personal conflicts of interest with regard to this study.
Author contribution
Nathalie Alexander and Enrico De Pieri contributed to study conceptualisation, project administration, ethics, study design, methodology, data curation, data analysis, data interpretation and writing. Reinald Brunner and Johannes Cip contributed to study conceptualisation, study design, data interpretation and writing. All authors have contributed to the manuscript and approved the submitted version.
Data availability statement
The datasets presented in this article are not readily available because of privacy restrictions. Requests to access the datasets should be directed to Nathalie Alexander.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship and/or publication of this article: EDP was funded by the University of Basel Research Fund for Excellent Junior Researchers.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.