
Abstract
Purpose
To assess the outcome of children with cerebral palsy following reposition of the distal rectus femoris tendon for treatment of stiff knee gait.
Methods
Children with cerebral palsy with stiff knee gait who underwent rectus femoris transfer were studied retrospectively. Inclusion criteria were cerebral palsy of diplegic or quadriplegic type, preoperative and 1 year postoperative three-dimensional motion analysis, and no other surgery except rectus femoris transfer at the time of study. The patients were separated into two groups: in group I, the rectus femoris was transferred to the distal medial hamstring tendons, either the gracilis or the semitendinosus; in group II, the distal tendon of the rectus femoris was transposed laterally and attached to the iliotibial band/intermuscular septum.
Results
Peak knee flexion during swing phase, total dynamic knee range of motion, knee range of motion during swing phase, and time to peak knee flexion during swing phase were all improved in both groups. Hip and pelvic kinematics were not influenced by the surgery. Velocity, stride length, and cadence were all improved following the surgery. There was no difference between the transfer group and the transposition group.
Conclusion
These findings suggest that distal transfer of the rectus femoris is effective in improving swing phase knee function by diminishing the mechanical effect of the dysphasic swing phase activity of the rectus femoris, not by converting the rectus femoris to an active knee flexor.
Introduction
Reduced knee flexion during the swing phase is a common problem in ambulatory children with cerebral palsy. In addition to this diminished peak knee flexion, there is also a reduction in total range of knee motion as well as delayed timing of peak knee flexion. These may cause functional problems, such as poor foot clearance during normal walking with resultant compensatory circumduction of the hip to help achieve foot clearance as well as difficulty ascending and descending stairs or curbs. This problem was first recognized in the 1980s when Perry, Gage and others [1–3] defined the problem and recommended transfer of the distal tendon of the rectus femoris to eliminate its activity as a dysphasic swing phase knee extensor and convert it to a swing phase knee flexor.
Their recommendation was to transfer the distal rectus tendon to the semitendinosus, gracilis, sartorius, or iliotibial band. However, most subsequent studies [4–6] have recommended transfer to the hamstrings medially, as it was thought that this would not only reduce dysphasic extensor activity during swing but also augment swing phase knee flexion by converting the rectus activity to knee flexion. Multiple other studies have documented similar beneficial effects of this operation, an average increase of ten degrees in swing phase knee flexion as well as an improvement in the timing of peak knee flexion [7–10]
In previous studies of this issue, most of the patients under study underwent concommitant procedures, thus making the outcome of the rectus procedure difficult to ascertain. We also limited this study to patients with bilateral involvement, eliminating hemiplegic patients in order to have a more homogeneous study group. We compared the outcomes based on the location of the transfer, medially or laterally, to determine whether improvements were due solely to the removal of the dysphasic swing phase rectus or whether this effect was augmented by the transfer.
Materials and methods
This study was approved by the local IRB and included all ambulatory spastic diplegic or quadriplegic cerebral palsy patients who underwent rectus femoris transfer or transposition for treatment of stiff knee gait between 1993 and 2002 as their only surgical procedure at the time of surgery and underwent no additional surgery within 1 year following the index surgery.
We identified 13 children with 25 affected limbs who met this inclusion criterion. In group I, the transfer group (13 limbs), the distal rectus femoris tendon was attached to the sartorius. In group II (12 limbs), the tendon was reattached to the iliotibial band to remove it as a deforming force and prevent its re-attachment to its natural insertion site. Since this is a retrospective study, patients were not randomized, and the choice of operation was based on the preference of the surgeon, with one of the involved surgeons performing all transfers and the other performing all transpositions.
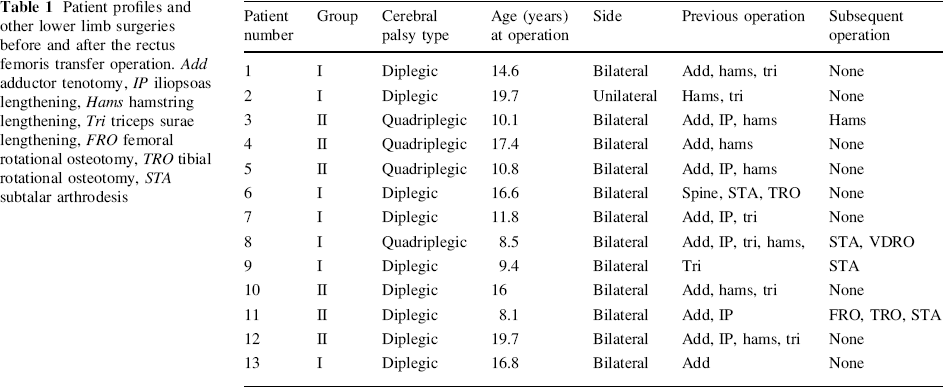
The patients groups included 9 with a diagnosis of spastic diplegia and 4 with spastic quadriplegia. Patients were classified according to functional levels as described by Hoffer, as well as by the gross motor function classification system for cerebral palsy (GMFCS). The use of walking aids such as walkers and crutches as well as orthotic use was also recorded. Four of these children were community ambulators, GMFCS I and II, nine used walking aids and were GMFCS III. The average age at surgery was 13.8 years. Ten of the children used ankle foot orthoses for ambulation and three used no orthotic. The Duncan-Ely Test was positive in all cases prior to surgery. Twelve of the patients underwent bilateral rectus femoris surgery and one had unilateral surgery; for each patient the same surgical technique was used for both sides. All patients were managed similarly postoperatively with an initial period in knee immobilizers. Ambulation commenced with full weight bearing and knee range of motion as soon as they were comfortable, usually within 1–2 days after surgery. Knee immobilizers were used for only 2–3 days on average. During the period of the study, no other surgical intervention was performed, though all of the patients in the study had prior surgery as documented in Table 1.
Patient profiles and other lower limb surgeries before and after the rectus femoris transfer operation. Add adductor tenotomy, IP iliopsoas lengthening, Hams hamstring lengthening, Tri triceps surae lengthening, FRO femoral rotational osteotomy, TRO tibial rotational osteotomy, STA subtalar arthrodesis
All children underwent physical examination including passive range of motion using a standard goniometric technique conducted by Motion Analysis staff, as well as testing for the presence or absence of a positive Duncan-Ely test. A gait analysis was performed using a Vicon 370 Motion Analysis System with six cameras. Patients were studied at their usual walking speed. The kinematic parameters assessed were maximum hip extension in stance, maximum knee extension in stance, maximum knee flexion in swing, total range of knee motion, and time to maximum knee flexion in swing. Temporal spatial parameters of stride length, cadence, and walking speed were measured. Statistics were analyzed using SPSS, and the difference between the transfer group and the transposition group was assessed using one-way repeated-measures of analysis of variance (ANOVA).
Results
The GMFCS level did not change in any patient following the surgery. One of the patients no longer needed an ankle foot orthosis (AFO) during ambulation. Following the surgery the Duncan-Ely test became negative in 11 of the patients, and was still mildly positive in two patients, both of whom with rectus femoris transposition to the iliotibial band.
Pre- and postoperative kinematics are shown in Table 2. There were no significant kinematic changes at the hip or pelvis in either group. Peak knee flexion during the swing phase significantly improved in all patients from a mean of 33° preoperatively to 45° postoperatively, and the group that underwent the operation involving transposition to the iliotibial band showed a greater degree of improvement than the group that underwent transfer to the medial hamstring. Total range of knee motion improved significantly from 31° to 36°, and ROM during swing increased from 10° to 19° with no difference between the groups. The timing of peak knee flexion improved from 54% of swing phase preoperatively to 39% postoperatively with no difference between the two groups (Fig. 1).
Changes in knee kinematics pre- and postoperatively. Pkf peak knee flexion
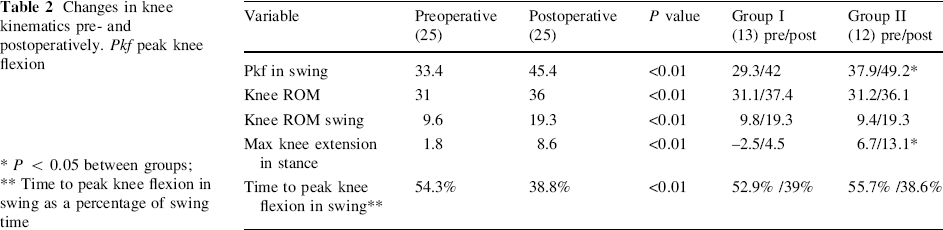
P < 0.05 between groups;
Time to peak knee flexion in swing as a percentage of swing time
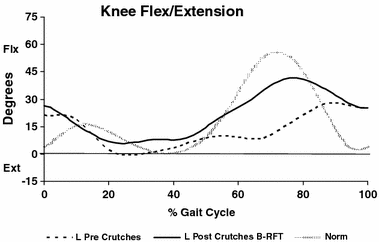
Representative case number 10. Kinematics of sagittal knee motion pre- and postoperative
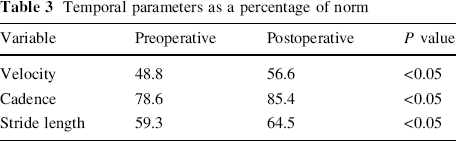
The linear parameters of velocity, cadence, and stride length all improved significantly at 1 year following surgery, with no difference between the two groups (Table 3).
Temporal parameters as a percentage of norm
Discussion
Perry [2] originally proposed rectus femoris transfer based on electromyographic analysis of gait in patients with cerebral palsy with reduced knee flexion during swing phase. She found four electromyographic patterns of rectus femoris activity in cerebral palsy. The most common was activity only during the swing phase. In such cases, she recommended transferring the rectus in order to move its contractile force behind the knee. This transfer of the distal tendon would eliminate its deforming force as a persistent undesirable knee extensor during the swing phase and provide knee flexion power by virtue of the transferred location posterior to the axis of knee rotation. All patients in our study met this criterion with demonstrated dysphasic activity of the rectus femoris throughout the swing phase when it is normally inactive.
Ounpuu et al. [9], in their study on the effect of rectus femoris transfer site on knee motion, found no differences among the four transfer sites, including three medial and the iliotibial band laterally, and recommended that the choice of transfer site can be dictated by surgeon preference or by the nature of other simultaneous procedures. However, most clinicians favor the medial site—where the tendon is attached to the distal stump of the gracilis or semitendinosus when done simultaneously with medial hamstring lengthening, or to the intact sartorius when done as an independent procedure—and feel that this transfer will provide augmented swing phase knee flexion.
However, recent evidence has shown that the transfer does not provide knee flexion power during swing.
Riewald and Delp [11] tested the moments generated by rectus femoris transfer by directly stimulating the transferred rectus femoris in two groups; one who underwent transfer to semitendinosus and the second who had transfer to the iliotibial band. In both groups, they found that rectus femoris transfer generated a weak knee extension moment and not flexion, as was assumed. Their conclusion was that the rectus femoris transfer does not convert this muscle from a knee extensor to knee flexor, but rather it is effective by removing a deforming force.
Asakawa et al. [12] also studied this issue by means of dynamic magnetic resonance imaging (cine-phase—contrast MRI). They demonstrated in patients after rectus transfer that the rectus femoris is displaced in the direction of knee extensors and not the knee flexors (hamstrings), although less so than in controls. They concluded that rectus transfer probably does not convert the rectus femoris to a knee flexor but diminishes the muscle's capacity for knee extension. In a static MRI study of patients following rectus femoris transfer, Asakawa et al. [13] showed kinking of the muscle in the thigh, which led them to conclude that this kinked muscle was unlikely to provide an effective mechanical force.
However, if the rectus femoris is simply released and the distal tendon left in-situ, kinematics of the knee during the swing phase at 1 year postoperatively are not significantly different from the preoperative status [3]. The likely reason for this is that the tendon scars down and reattaches to its normal anatomic site.
The objective of our study was to determine whether RF distal transfer as an isolated procedure improves stiff knee gait in children with cerebral palsy, and to determine if there was any difference in outcome dependent on the transfer attachment site. Patients in our study had undergone no other surgery during the study period, which allowed us to isolate the effect of the rectus transfer alone. We evaluated two different operative techniques: the classical transfer as described by Perry [2] to the sartorius and the simple transposition of the mobilized tendon to the intermuscular septum. In each group, we found similar improvement of peak knee flexion, normalization in the timing to peak knee flexion, and an increase in the total arc of knee motion during swing.
However, we found an increase in minimum knee flexion during stance (maximum knee extension). Ounpuu et al. [10] found no such increase; however, in their study, 119 of 136 patients underwent concomitant hamstring release at the time of rectus surgery. One possible explanation for the increased crouch in our series may be the tendency of crouch to increase over time in cerebral palsy patients, rather than a weakening of extensor strength during stance. We found more patients with crouch in group II, perhaps because they had more crouch gait preoperatively that became worse with time combined with the fact that in this group of patients no hamstring release was done at the time of the study period (Table 2).
When we compared the two operative techniques, there were no differences in outcomes with regard to knee kinematics. Our results demonstrate that the rectus surgery has its primary effect by eliminating a deforming force, rather than by functioning as an active transfer to augment swing phase knee flexion. The rectus transposition is an alternative to the transfer as it can be performed through either a single incision or the same lateral incision used for distal femoral rotational osteotomy, either at the time of the initial osteotomy or at the time of plate removal. With no obvious superiority of transfer or transposition, the data support the findings of Ounpuu et al. that site location for the rectus re-attachment can be based on surgeon preference and what other concomitant procedures are performed.
Footnotes
Acknowledgment
The authors thank Kaye Wilkins for the friendly assistance.