
Abstract
Purpose:
Anterior cruciate ligament repair techniques are of growing interest because they allow for minimally invasive surgery that avoids harvesting of the transplant, without risking growth deficiencies in young patients. The aim of this study is to summarize the published evidence about arthroscopic repair of anterior cruciate ligament proximal tears in skeletally immature patients.
Methods:
In total, four studies were included and processed for data extraction after screening for eligibility for this systematic review: one retrospective cohort study and three retrospective case series. Altogether, the four studies included in this review included 61 skeletally immature patients with a mean age of 12.1 years diagnosed with proximal anterior cruciate ligament tear who underwent arthroscopic repair with preservation of the native ligament. The mean follow-up period was 2.8 years.
Results:
The most relevant and objective outcome that we considered was re-rupture rate. One study reports a cumulative incidence of graft failure in the first 3 years after surgery of 48.8% while the others report a 0%, 0% and 21.5% re-rupture rate. No growth disturbances were reported in the included studies.
Conclusion:
Despite growing interest surrounding anterior cruciate ligament repair techniques, the presence of limited quality studies in the literature means repair cannot be strongly supported at present. Some encouraging data regarding the absence of growth disturbance and functional outcomes does exist, but studies with larger samples are required.
Level of evidence:
level IV.
Introduction
Anterior cruciate ligament (ACL) injuries in pediatric and adolescent patients are uncommon but increasing in incidence, accounting for 0.5%–3% of all knee injuries.1 –3 ACL injuries in this population have been rising over the last two decades, a result of improved clinical awareness, diagnostic skills, along with a growing participation of children in high-demand sports and intensive physical training programs.4 –8
Non-operative treatment was traditionally considered to be the management of choice, consisting of activity modification and bracing, largely because of concern regarding physeal damage arising from adopted “adult” reconstructive techniques. Surgery was often delayed until physeal growth plate closure.9 –12
Although surgical treatment is today widely acknowledged to restore joint stability and prevent the above-mentioned sequelae, the timing of surgery, graft choice, and the technique of tunnel placement remain deeply controversial.13 –15
Many different techniques for ACL reconstruction have been proposed, and the skeletal age plays a key role in the selection of a method that may minimize growth disturbance.14,16 –19 Reported growth abnormalities after ACL reconstruction in Tanner 1 and 2 patients range from 2% to 13%.20 –22
The high revision rates following ACL reconstruction in the skeletally immature combined with controversies over technique and graft choice have led to consideration of the option of maintaining the native ACL. The ligamentous tissue of skeletally immature patients is characterized by higher cell density and greater potential for cell migration,23 –25 suggesting the benefits of repair in children may outweigh the risks in comparison to older patients.
A detailed analysis of the specific anatomical location of the tear and of the timing of surgery revealed that proximal tears and early surgical intervention are related with positive outcomes.26 –28 Furthermore, in addition to the less invasive nature of the procedure, a crucial benefit associated with the retention of the native ligament is the preservation of proprioceptors and mechanoreceptors that have a key role in the complex neural network required for the restoration of optimal joint biomechanics.29,30
As a result, there has been a recent increase in the number of arthroscopic ACL repair procedures as a possible response to the unique challenge represented by the surgical management of ACL tears in children and adolescents.
The aim of this study was therefore to summarize the published evidence about arthroscopic repair of ACL proximal tears in skeletally immature patients, with specific interest in proximal tears, which seem to have the most promising results.
Materials and methods
Focused based question
Based on the Preferred Reporting Items for Systematic Review and Meta-Analysis (PRISMA) guidelines, a specific question was constructed. The focus question addressed was “What is the role of arthroscopic repair for ACL proximal tears in skeletally immature patients?”
Eligibility criteria
The following eligibility criteria were required: (1) original English language published articles or articles with English translation; (2) studies based on human skeletally immature patients, with specific documentation of open growth plates at the distal femur and proximal tibia at the time of surgery; (3) studies including patients who sustained proximal ACL tears documented with magnetic resonance imaging (MRI); (4) studies including arthroscopic ACL repair procedure with preservation of the native ligament; (5) studies including a minimum of five patients; and (6) studies including a minimum mean follow-up of 24 months. Exclusion criteria therefore consisted of non-English language articles, literature reviews, letters to the editor, editorial comments, unpublished articles, studies on animals or cadaveric specimens, patients undergoing non-operative management or open surgical treatment, and all those conditions contravening the above inclusion criteria.
Search strategy and study selection
We conducted a comprehensive literature search using PubMed/Medline (National Library of Medicine, Washington, DC, USA) and EMBASE (Elsevier API) from 1 January 1976 up to and including 1 April 2023, since the first reports of pediatric arthroscopic procedures date back to the mid-1970s.31,32 The following string was used to perform the literature search: “ACL” AND “repair” AND (“pediatric” OR “pediatric” OR “adolescent” OR “skeletally immature”).
Titles and abstracts of studies identified using the above-described protocol were screened by two different authors (“Turati” and “Anghilieri”) and checked for agreement. Disagreement was solved through debate, involving the other authors. The studies included during the screening phase were read in full and evaluated based on the stated eligibility criteria. Reference lists of potentially relevant original articles were hand-searched to identify any studies not captured using the initial search terms. 33 Research of “similar article” was additionally done for the papers selected. Once again, the articles were checked for disagreement via discussion among the authors following a structured algorithm (Figure 1).
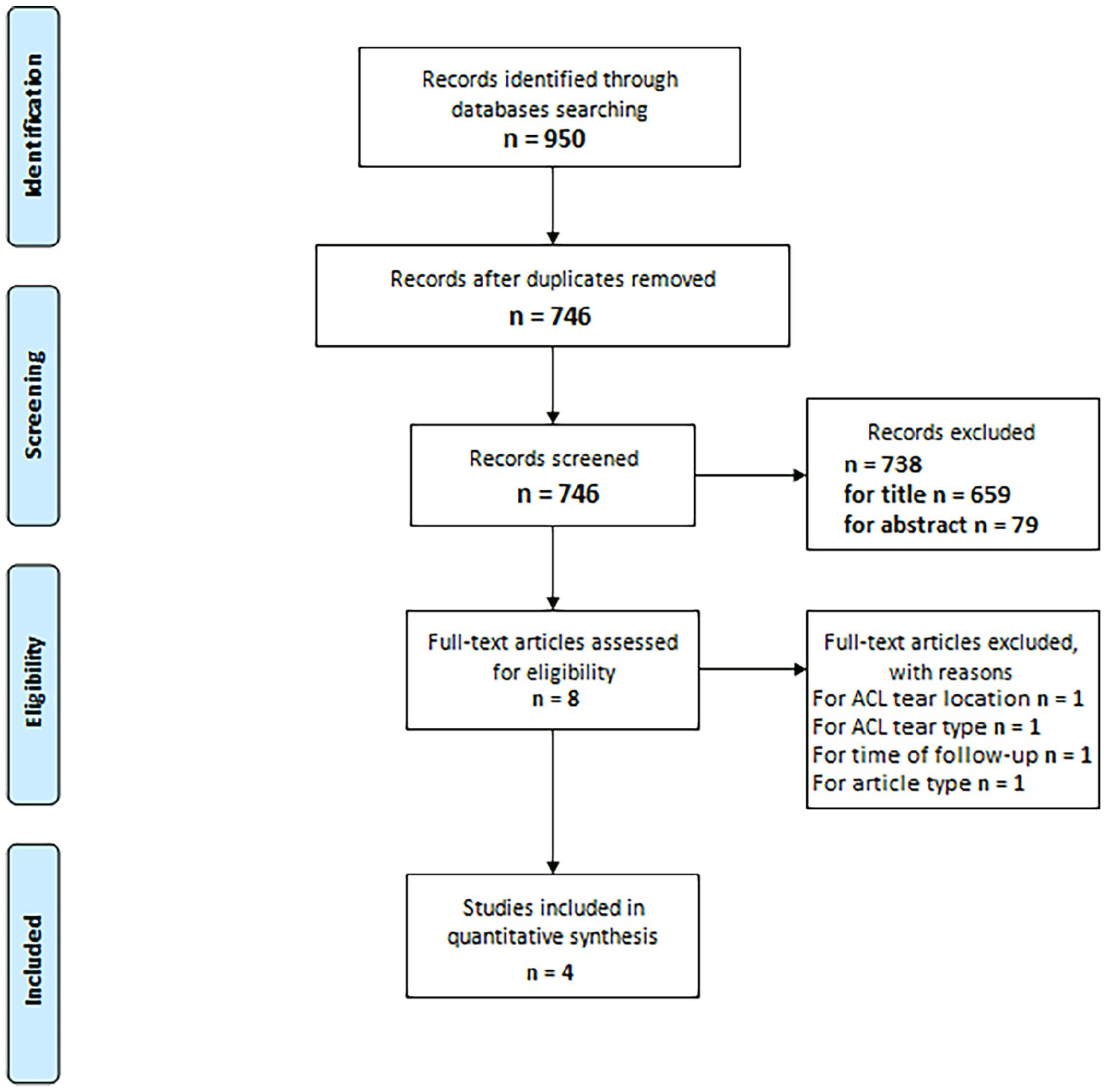
Structured algorithm for study selection.
Methodological study quality assessment and data extraction
The Methodological Index for Non-randomized Studies (MINORS) scoring system was chosen to assess the quality of each study included in the present review. 34
The revised and validated version of MINORS provides eight methodological items for non-comparative studies: (1) clearly stated aim, (2) inclusion of consecutive patients, (3) prospective collection of data, (4) endpoints appropriate to the aim of the study, (5) unbiased assessment of the study endpoint, (6) follow-up period appropriate to the study aim, (7) loss to follow-up <5%, and (8) prospective calculation of the study size.
Moreover, to score comparative studies, the MINORS system includes four additional items; however, no comparative study was included in the present review. The items are scored as follows: 0 if not reported, 1 if reported but inadequate and 2 if reported and adequate. The global ideal score adds up to 16 for non-comparative studies and 24 for comparative studies. According to MINORS, the study quality is considered high only when an article reached full scores (16/16 for non-comparative studies and 24/24 for comparative ones) and low in all other cases.
From the included articles, the following data were considered relevant to this review: article type, journal, year of publication, presence of a control group, number of patients included, sex, mean age, follow-up period, surgical techniques, and peri-operative and post-operative complications.
Results
Literature search and quality assessment
The initial search yielded 950 studies. After duplicate removal, 746 articles were screened for eligibility and 742 studies which did not fulfill the eligibility criteria were excluded (Figure 1). In total, four studies were included and processed for data extraction.35 –39
For the three case series included, the mean MINORS score was 11 out of 16, ranging from 9 to 12. The one cohort study 37 included was scored 19 out of 24 (Table 1).
References, MINORS score, and type of study for each article included.
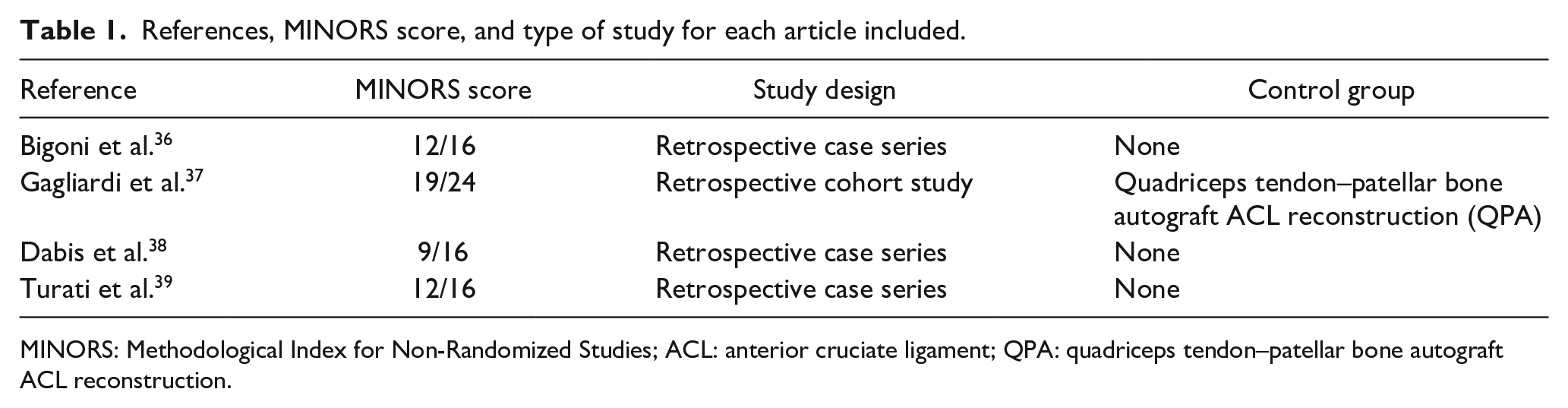
MINORS: Methodological Index for Non-Randomized Studies; ACL: anterior cruciate ligament; QPA: quadriceps tendon–patellar bone autograft ACL reconstruction.
Concerning the adequacy of follow-up in the present review, 1 point was assigned for follow-up between 2 and 5 years, while 2 points were assigned for follow-up ≥5 years. This decision was based on the fact that we considered fully appropriate follow-up that reached the period of physeal closure and thus were able to detect any growth disturbances. Unfortunately, not a single study was scored 2/2 for the follow-up period and prospective calculation of the sample size was absent in all of the included studies. According to MINORS score, the quality of all included studies was overall low.
General characteristics of included studies
No randomized controlled trials were found to be included in this review. We included one retrospective cohort study and three retrospective case series (Table 1). Altogether, the four studies in this review included 61 skeletally immature patients diagnosed with proximal ACL tear who underwent arthroscopic repair with preservation of the native ligament (Table 2). The mean age in the population of the current review, weighted among the four studies, was 12.1 years old. Although female patients have a higher risk of ACL injury, even in school-aged children and adolescents, 4 male sex was prevalent, representing 57.4% of the total. The cumulative mean period of follow-up was 33.66 months (2.8 years).
General patient characteristics of included studies.
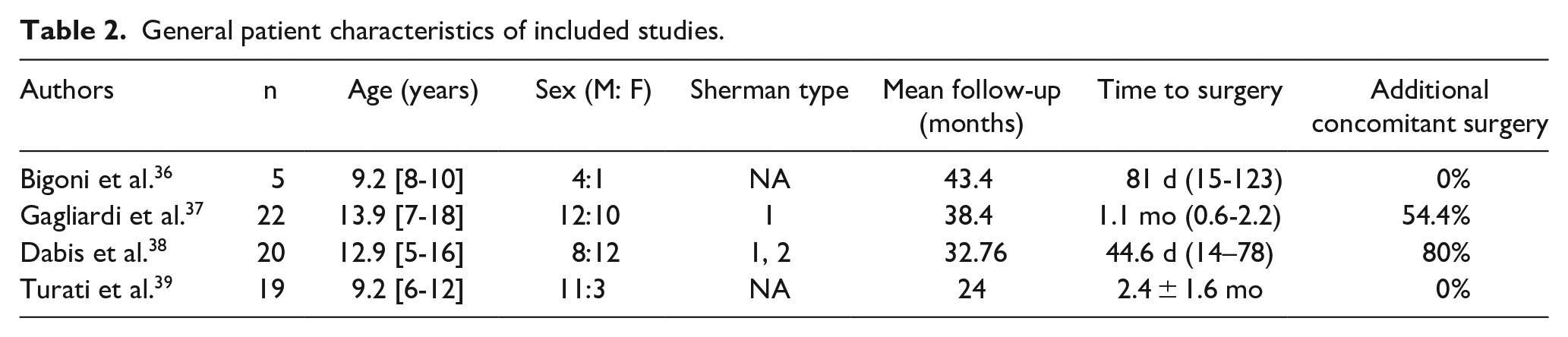
In two studies, more than half of the population required additional concomitant surgery during ACL repair. These cases included both meniscal repairs and meniscectomies, while cases of additional ligamentous surgery were not included, as multiligamentous injuries were excluded from the beginning. This is because surgery on structures other than the ACL could have been confounding on the outcome of knee stability after ACL repair. The mean time from injury to surgery was recorded in three papers out of four, with a mean weighted value of 59.1 days.
Surgical techniques
Different surgical techniques for ACL repair were used in the considered studies (Figure 2). Bigoni et al. 36 and Turati et al. 39 performed an arthroscopic ligament repair through anteromedial (AM) and transpatellar (TP) portals. The ACL stump was captured through a polydioxanone (PDS) 2-0 suture (Ethicon, Somerville, NJ, USA) as a shuttle and transfixed at the native proximal femoral footprint after appropriate drilling. The re-fixation was performed with a single suture anchor (Panalok 3.5 mm, DePuy Mitek, Raynham, MA, USA) with microfracture performed at the femoral footprint to promote bleeding.
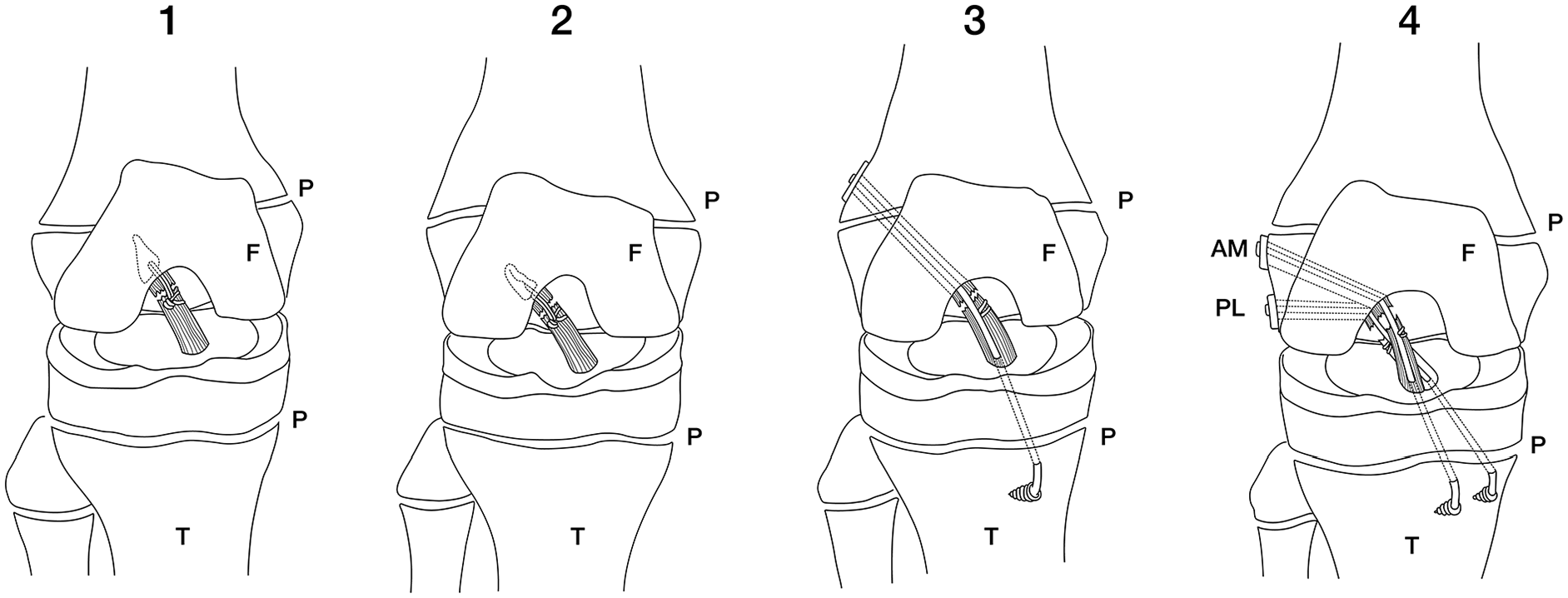
Different techniques for proximal ACL repair in the skeletally immature. Suture anchor repair with bioabsorbable anchor (1), suture anchor repair with all-suture anchor (2), suture repair with a suture tape augmentation (3), and suture repair with suture tape augmentation and double all epiphyseal tunnels (4).
Gagliardi et al. 37 proposed a surgical repair with suture ligament augmentation (SLA). A single suture (No. 2 FiberWire; Arthrex, Inc., Munich, Germany) was passed into the ACL stump in either a modified Bunnell suture pattern or a luggage tag-type suture. Osteochondral microfracture was performed in order to stimulate the healing of the reinsertion zone at the native femoral footprint.
For the tunnel, the authors described two independent femoral drill tunnels and one or two independent tibial tunnels. For patients with open physes, the tunnels were all epiphyseal.
Finally, Dabis et al. 38 proposed a transphyseal approach with small-diameter tunnels. Through AM portal, two high tensile braided composite looped sutures were passed around the proximal ACL stump, as a luggage tag-type stitch, to bring the remnant closer to the lateral wall of the femoral condyle. Moreover, the author routinely augmented the repair, consisting of a metal cortical suspension button and non-biodegradable suture tape. This technique requires subsequent removal, performed in a second procedure 3 months after the index surgery.
Post-operative management
The post-operative management was not homogeneous among the included studies. Gagliardi et al. and Dabis et al. allowed immediate weight-bearing as tolerated for patients without meniscal tears. Dabis et al. permitted full range of motion (ROM), while Gagliardi et al. applied immobilization at full extension until the patients were able to perform 75 straight leg raises in 1 day without extensor lag. For patients who underwent meniscal repair, weight-bearing, and ROM were limited for 4–6 weeks depending on tear pattern. Standard ACL post-operative rehabilitation was performed with knee motion exercises, isometric quadriceps activation, reinforcement training of the hamstrings, hydrotherapy, and proprioception exercises under physiotherapist guidance.
Bigoni et al. and Turati et al. applied a much more cautious post-operative protocol using a constant long leg non-weight-bearing splint for 4 weeks. After removal of the splint, weight-bearing was allowed using a hinged knee brace for 8 weeks with a gradual increase of ROM and standard ACL rehabilitation was started. Straight line jogging was allowed after 3–4 months, while cutting sports after 6–7 months.
Outcomes
The outcomes measured in the four included studies were not homogeneous. Several scores were used in the included studies in order to evaluate the outcomes of ACL repair techniques, usually collected pre-operatively and post-operatively at 1 or 2 years follow-up. These included the pedi-International Knee Documentation Committee (IKDC), used in three out of four studies, which is specific for knee function measurement in pediatric patients: the score ranges from 0 (poor function) to 100 (excellent function). 40
The Lysholm survey was utilized in all four studies and has been proved to be an adequate instrument to evaluate the functional status of the knee in young patients, with the maximum score of 100 representing optimal knee function. 41
Although originally developed for an adult population, the Tegner Activity scale, which evaluates the level of pre- versus post-operative work and sport activities (a higher score corresponds to more demanding performance), was also considered in three studies. Only Dabis et al. performed the KOOS-child score to measure the patients’ perspective on their knee pain and disability 42 (Table 3).
Re-rupture rates and outcome scores considered in included studies.
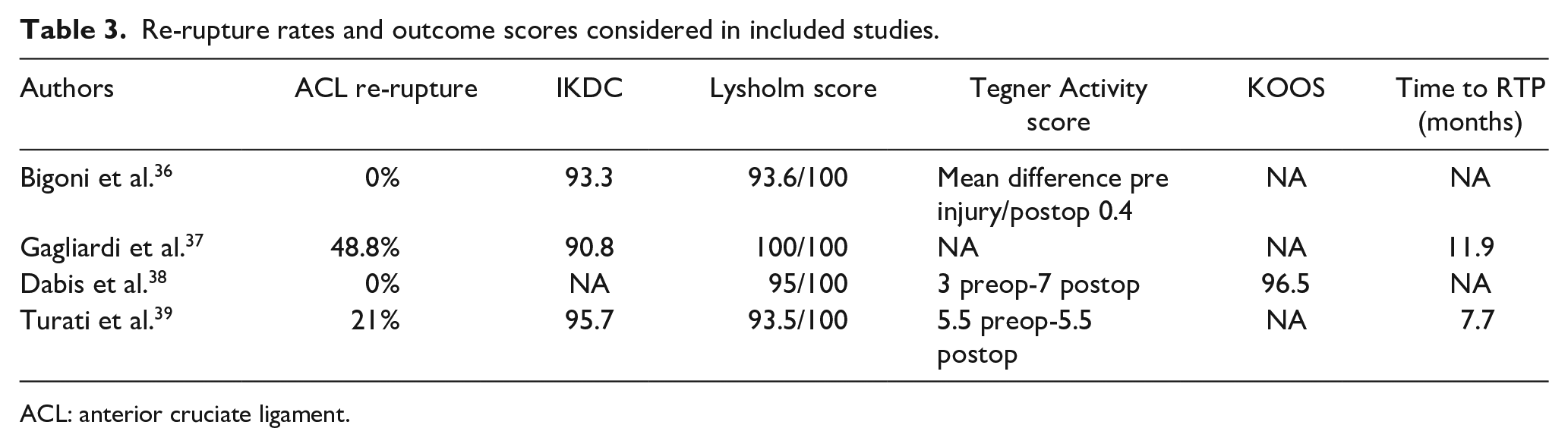
ACL: anterior cruciate ligament.
Most patients were clinically evaluated via the Lachman test, pivot-shift test, and ROM measurements. Turati et al. and Bigoni et al. also performed the One-leg Hop for distance test, in which subjects were instructed to jump as far as possible with a controlled leading at first with the nonsurgical limb followed by the surgical limb in order to calculate the Limb Symmetry Index (LSI) (surgical limb hop distance/non-surgical limb hop distance) × 100. This test allows evaluation of differences in jumping performance between the operated limb and the non-operated limb.
All authors except Dabis et al. evaluated the post-operative stability using a KT-1000™ knee arthrometer estimating side-to-side differences in millimeters of anterior tibial translation at 30° of knee flexion (SSD) by applying 134 N of force (MEDmetric Corporation, San Diego, CA, USA) (Table 4).
Clinical outcomes considered in included studies.
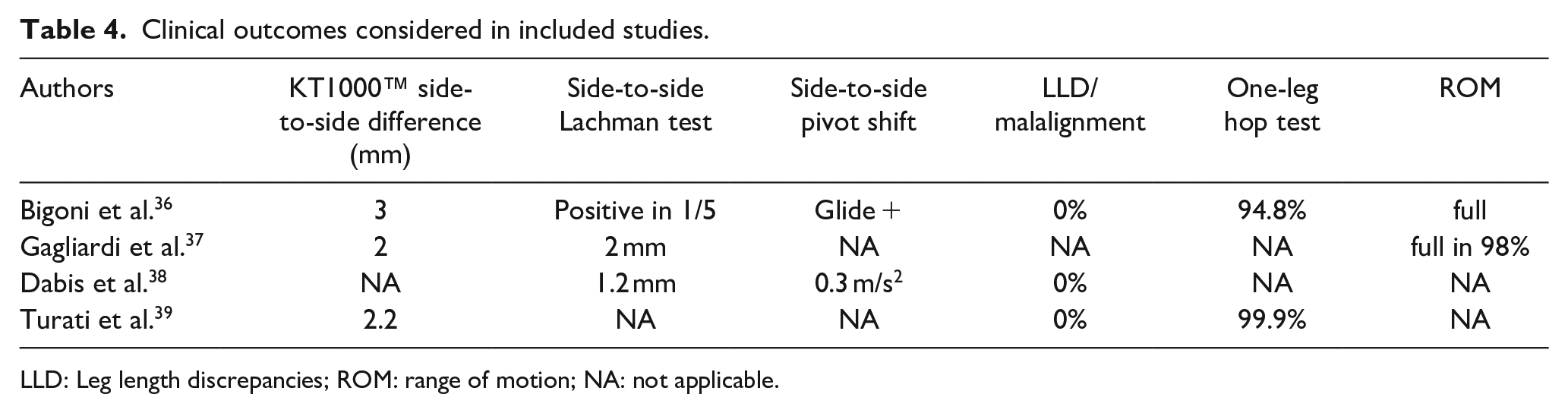
LLD: Leg length discrepancies; ROM: range of motion; NA: not applicable.
Possible leg length discrepancies (LLDs) and malalignment were clinically assessed in most patients via manual goniometer and with tape measurement of the distance from the anterior superior iliac spine and the medial malleolus. No growth disturbances were reported in the included studies.
The re-rupture rate certainly represents the most objective and significant outcome among those considered (Table 3). Among the case series included in this systematic review, Gagliardi et al. reports a cumulative incidence of graft failure in the first 3 years after surgery of 48.8%. This result differs considerably from what is reported in the other three articles (0% for Bigoni et al. and Dabis et al., and 21% for Turati et al.).
Turati et al. reported a median time of 3.9 years (range = 8–93 months) between surgery and re-rupture.
Discussion
ACL repair procedures, especially in skeletally immature patients, have potential benefits that has led to renewed clinical and research interest over the last decade. 43
To the best of our knowledge, current evidence identifies non-homogeneous populations, techniques, and results. For this reason, we decided to focus our investigation on a specific ligament injury location: proximal ACL tears.
Even restricting the investigation to proximal ACL tears, some differences emerged from the populations present in the included studies. Based on the classification of Sherman et al. 44 of the precise anatomical location of the ACL tear, Gagliardi et al. only included patients with a type I lesion, where the ACL avulses directly from the femoral footprint. Dabis et al. included both type I and II injuries, the latter consisting of tears through the upper 1/3 of the ligament. Bigoni et al. and Turati et al. merely report that the lesions occurred within the proximal portion of the ACL, without referring to Sherman’s classification.
Some discrepancies also emerge when considering the age of the patients in these studies. Bigoni et al. and Turati et al. enrolled patients with a mean age of 9.2 years, Dabis et al. 12.9 years, whereas in Gagliardi et al., this value was significantly higher, with a mean age of 13.9 years old. This finding may be relevant when interpreting the high rate of re-ruptures recorded in Gagliardi’s study of almost 50%. A key concept on which ACL repair is based is the notion that skeletally immature individuals have better healing capacity when compared to a skeletally mature population.24,45 In this context, the reparative, rather than reconstructive, surgical option in Gagliardi’s paper might be questionable in a cohort approaching skeletal maturity. This does also take in to account the likelihood that younger age may be associated with higher failure rates after surgery for ACL injuries due to movement patterns, greater growth remaining, and difficulties in rehabilitation. Another crucial factor that may account for the high re-rupture rate is the surgical technique. Gagliardi described a double-bundle repair technique with two independent femoral drill tunnels and one or two independent tibial tunnels that would likely sacrifice native ACL fibers and footprint. The tunnels were 4 mm in diameter; therefore, the cumulative damage to the underlying footprint could be a concern. Remnant ligamentous preservation is in fact still a hot topic in adult ACL reconstructive procedures, and although there is no specific evidence regarding skeletally immature patients, we can extend to this population some of the findings of the adult population. Remnant-preserving ACL reconstruction is reported to have higher potential for early healing, superior functional and proprioceptive recovery, and lower occurrence of reinjury.46,47 For this reason, sacrificing the ligamentous footprint in an ACL repair procedure may not be indicated. It is also important to note that the femoral footprint is a relatively avascular area, most of the blood supply of the ACL ascending in the interval between the cruciate ligaments, although a hematoma produced by bone microfracture will potentially increase the biological healing potential. 48
No case of re-rupture was reported by Bigoni and Dabis, while a rate of 21.5% was registered by Turati. Post-operative protocols were heterogeneous among the included studies. Dabis et al. and Gagliardi et al. allowed for immediate post-operative weight-bearing (Gagliardi with limited ROMs and Dabis with full ROM), while Bigoni et al. and Turati et al. applied a more cautious management with full-time long leg non-weight-bearing splint for 4 weeks followed by gradual increase of flexion using a hinged knee brace.
The differences in terms of re-rupture rate are therefore not attributable to the post-operative management, as Gagliardi, who reported a re-rupture rate of almost 50%, applied the same protocol as Dabis, who reported a 0% re-rupture rate. The main determinants of the failure of proximal ACL repair may therefore be the surgical technique and patient selection (skeletal immaturity). Each surgical technique requires larger numbers to be reproducible and to be evaluated with few confounding factors. Regarding patient selection, age and tear anatomical location were homogeneous and ambiguous as stated above.
Since the present review included few studies with low quality, the speculations raised should be intended as hints for the design of high-quality multicentric studies and not as strong conclusions. Where failure did not occur, overall excellent functional recovery was obtained in the operated knees (evaluated via functional scores pedi-IKDC, Lysholm survey, Tegner Activity scale, and KOOS-child score) showing that, if successful, reparative techniques in proximal ACL tears are a valid surgical option that warrant further investigation.
There are now trials emerging on treatment of proximal tears, such as the ACL-STARR trial (NIHR157938), currently funded in both the United Kingdom and Australia, a non-inferiority single blind randomized controlled trial of ACL repair for proximal ruptures versus ACL reconstruction. This trial will include patients from 14 years of age, but a trial specifically looking at the skeletally immature population, who are so different, is needed.
Conclusions
It is difficult to draw conclusions on ACL repair based on the limited studies available. This suggests further research is needed to identify if repair of proximal ruptures in the skeletally immature, where there is better healing potential, balances against the increased risk of re-rupture seen in ACL reconstruction. ACL repair techniques are of growing interest because they allow for less invasive surgery, avoid the need for graft harvesting, and minimize the risk of growth disturbance in young patients.
Careful patient selection is required: males <12 years and females <10 years have higher risk of developing growth disturbance as they are still far from reaching skeletal maturity.49,50 These patients are candidates for physeal-sparing techniques such as repair or physeal-sparing reconstruction. The skeletal age at which a transphyseal reconstruction can be safely performed has yet to be determined, but all techniques still have the potential to cause growth disturbance. At present, there is no universal accepted way to monitor for and assess for post-operative growth plate damage with significant heterogeneity in reporting. 51
Remnant-preserving ACL reparative surgery may be preferable when considering the different surgical techniques for ligamentous repair as footprint preservation seems to be associated with better outcomes in the adult population, although it may affect ROM by causing impingement in the femoral notch.
Therefore, what emerges from this systematic review is that remnant-preserving reparative techniques in proximal ACL tears may be a surgical option in skeletally immature patients but, being backed by studies of limited quality, warrants careful further investigation due to high failure rates seen in some of the published small case series.
Supplemental Material
sj-pdf-1-cho-10.1177_18632521241244626 – Supplemental material for Arthroscopic repair of proximal anterior cruciate ligament tears in children and adolescents: A systematic review
Supplemental material, sj-pdf-1-cho-10.1177_18632521241244626 for Arthroscopic repair of proximal anterior cruciate ligament tears in children and adolescents: A systematic review by Marco Turati, Filippo Maria Anghilieri, Simone Daniel Gatti, Aurelien Courvoisier, Luca Rigamonti, Giovanni Zatti, Nicolas Nicolaou and Marco Bigoni in Journal of Children’s Orthopaedics
Footnotes
Author contributions
M.T., F.M.A., L.R., G.Z., A.C., N.N., and M.B. contributed to the study conception and design. Material preparation and data collection and analysis were performed by F.M.A., S.D.G., N.N., A.C., and M.T. The first draft was written by M.T., F.M.A., A.C., G.Z., and S.D.G. Review, editing, and formal analysis were performed by M.T., S.D.G., L.R., N.N., and M.B. Project administration was conducted by M.T., N.N., and M.B. Statistical analysis was conducted by F.M.A., A.C., and L.R. All authors read and approved the final manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
Not required.
Submission declaration
This manuscript has not been published previously and is not under consideration for publication elsewhere. The publication of this article has been approved by all authors and by the responsible authorities where the work was carried out. We declare that, if accepted, this manuscript will not be published elsewhere, including electronically in the same form, in English or in any other language, without the written consent of the copyright-holder.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.