
Abstract
Purpose:
Pediatric pelvic fractures are uncommon. This study aimed to investigate the clinical characteristics of pediatric pelvic fractures requiring hospitalization and analyze their correlation with associated injuries and complications.
Methods:
Data from 315 pediatric pelvic fracture patients admitted to our hospital from January 2006 to December 2021 were retrospectively analyzed. Sex, age, modified Torode–Zieg classification, abbreviated injury scale score, injury severity score, mortality, and concomitant injuries were analyzed.
Results:
Of the 285 (90.5%) cases of combined injuries, most injuries occurred in the abdomen (64.8%) and lower extremities (47.6%), followed by the chest (45.4%) and head (34.6%). A total of 78 patients (24.8%) were transferred to the intensive care unit. In total, 94 patients (29.8%) had complications during hospitalization. There were differences based on injury mechanism (p = 0.001), with the highest complication rate in the fall injury group (32 cases (46.4%)). Approximately 51.4% of patients received surgical treatment for problems that were not related to pelvic fractures. Among these, 30.2% necessitated surgical intervention on the lower limbs. Abdominal surgery was necessary in 19.0% of patients.
Conclusions:
Children who have pelvic fractures frequently require hospitalization due to the presence of severe injuries in other areas of their bodies. IIIB pelvic fractures frequently occur in conjunction with more severe abdominal injuries; therefore, the prompt management of cavity and organ injuries is of particular importance. Blood transfusion and injury severity score were associated risk factors for intensive care unit admission.
Introduction
Pediatric pelvic fractures (PPFs) are uncommon, with a reported incidence of 0.3%–4% following injury. 1 High-energy blunt injuries are the primary contributors to pelvic fractures in children caused by motor vehicle accidents or falls. 2 Conversely, bleeding that leads to hemodynamic instability in adult pelvic fractures is rarely seen in PPFs; high-energy trauma resulting in solid organ damage is the main source of bleeding in children.1,3 The level of force required to fracture a pelvis is high; hence, it is likely to be transmitted to other body parts, including the abdomen, genitourinary system, spine, and head. Therefore, mortality rates secondary to pelvic fractures are higher in adults than in pediatric patients attributed to injuries to other body parts, especially the head.1,2,4
Although there are many reports on pelvic fractures in children, no corresponding studies have detailed the associated injuries and complications. In this study, we reviewed 315 pediatric patients with pelvic fractures to analyze the mechanism of injury, concomitant injuries at each site, and the characteristics of complications during hospitalization.
Materials and methods
Data sources
This study was conducted at our hospital, with a retrospective collection of data of patients with age <18 years diagnosed with pelvic fractures based on the International Classification of Diseases (ICD) classification, 9th and 10th editions (808.0–808.9; S30–39) and hospitalized from 1 January 2006 to 31 December 2021. Patients were identified by searching our electronic case query system and medical imaging picture archiving and communication system (PACS) system. This study was approved by the Ethics Committee of our hospital (2021).
Inclusion and exclusion criteria
The inclusion criteria were as follows: (1) initial visit after injury, (2) pelvic imaging available for evaluation from the time of injury, and (3) complete medical records.
The exclusion criteria were as follows: (1) non-accidental injuries and (2) pathological fractures due to bone tumors, metabolic bone disease, and bone developmental disorders.
Methods
A uniform survey form was developed to collect data on the following characteristics: age, sex, cause of injury, modified Torode–Zieg classification of pelvic fractures in children, length of hospitalization, mortality, abbreviated injury scale score (AIS), injury severity score (ISS), associated injuries, and comorbidities during hospitalization. The AIS classified associated injuries to the head, neck, face, chest, abdomen, spine, upper extremity, and lower extremity; the site further detailed them for each site. Complications during hospitalization included shock, acute respiratory failure, acid-base balance disorders, electrolyte disorders, traumatic coagulopathy, and thrombosis.
Pelvic fracture staging was based on the modified Torode–Zieg classification. 5 Two senior orthopedic surgeons and one chief radiologist were responsible for quality control, and any fracture staging errors exceeding 5% were re-read and judged.
Statistical analysis was performed using the Statistical Package for the Social Sciences, version 19.0 (SPSS Inc., Chicago, IL, USA), with measures described as percentages; counts are expressed as rates or composition ratios. The t-test and analysis of variance (ANOVA) were used for measurement data, while the non-parametric rank sum test was used for data that did not conform to a normal distribution. The chi-square test or (T < 5) Fisher’s exact probability method was used for the count data. Yates’ corrected chi-square was also used for categorical variables if the expected cell frequencies were below 5. For skewed continuous data, a non-parametric Mann–Whitney test was performed. A two-tailed p value of <0.05 was considered statistically significant.
Results
Epidemiology
During the 16-year study period (January 2006–December 2021), there were 315 PPF patients, 198 males (62.9%) and 117 females (37.1%). There was no difference between the sexes regarding the mechanism of injury, pelvic injury classification, mortality, and associated injuries.
Ages ranged from 0.4 to 15.7 years, with a mean age of 6.39 ± 3.66 years, and differed across pelvic injury classifications and mechanisms of injury. Among the pelvic injury classifications, the mean age for type I injuries was 11.01 ± 6.17 years, while the mean age for type II injuries was 5.14 ± 2.45 years. The remaining three injury types showed ages similar to the overall mean (Table 1). Regarding injury mechanism, patients injured in pedestrian–motor vehicle traffic accidents were significantly younger (mean age, 5.05 ± 2.87 years). In addition, the mean age of patients gradually increased across the five groups, with the youngest mean age found in pedestrian–motor vehicle traffic accidents and the oldest mean age in simple falls (Table 2).
Comparison of clinical presentations and outcomes of PPFs based on the Torode fracture classification.
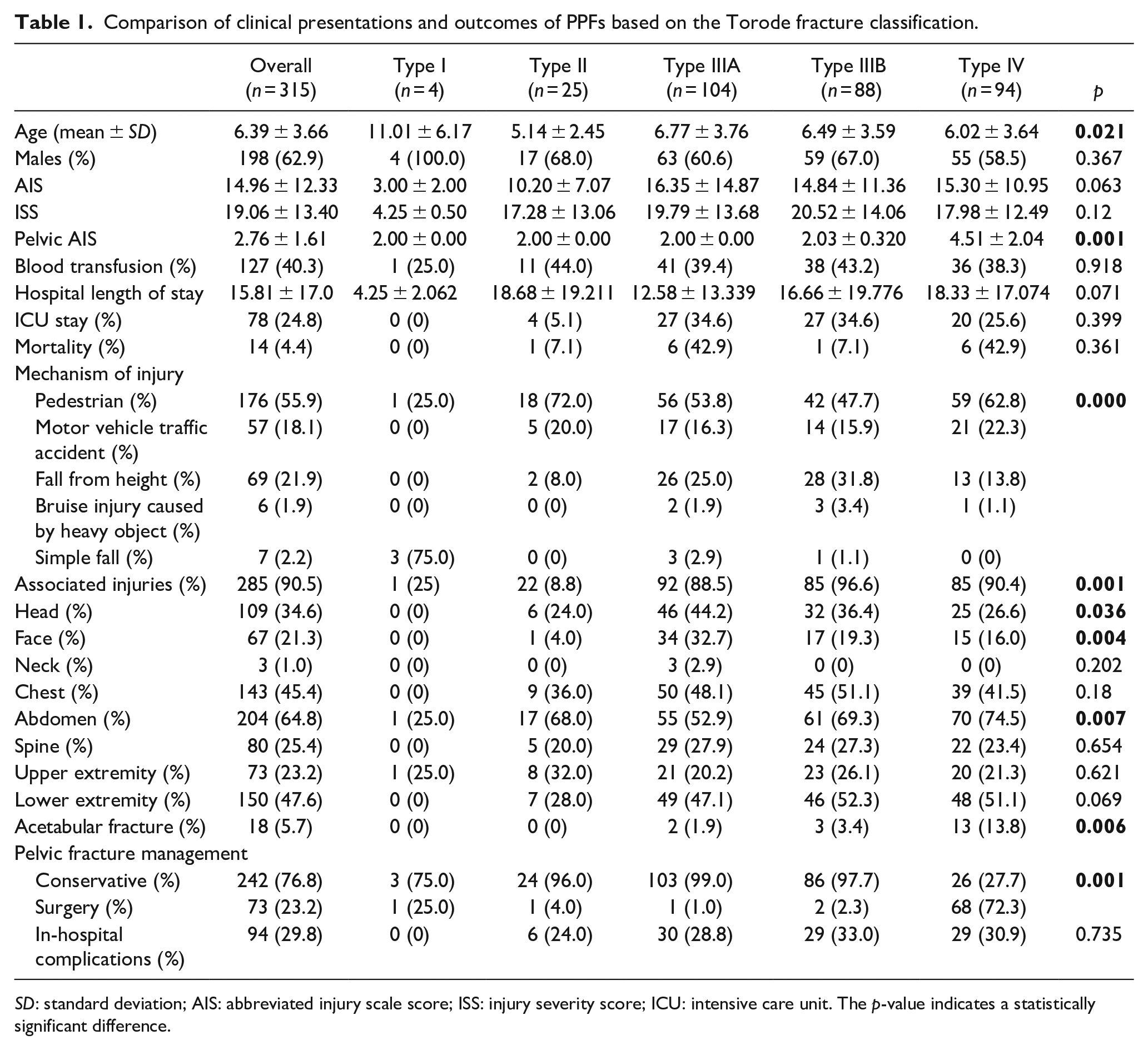
SD: standard deviation; AIS: abbreviated injury scale score; ISS: injury severity score; ICU: intensive care unit. The p-value indicates a statistically significant difference.
Comparison of clinical presentations and outcomes of PPFs based on the cause of injury.
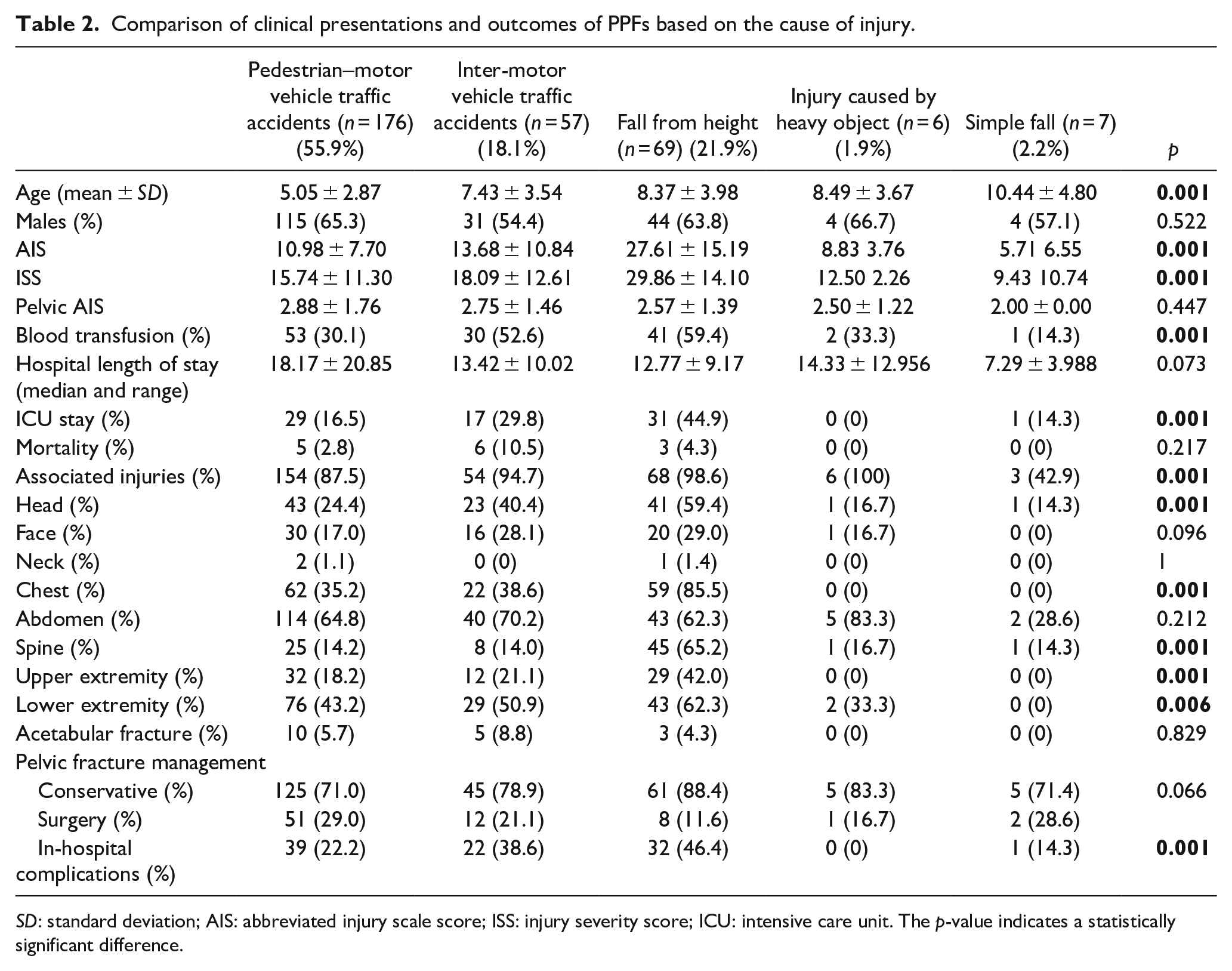
SD: standard deviation; AIS: abbreviated injury scale score; ISS: injury severity score; ICU: intensive care unit. The p-value indicates a statistically significant difference.
Hospital stay
The mean hospital stay was 15.81 ± 17.0 days (range, 1–159 days), and the median hospital stay was 11 days; there was no difference in hospital stay according to injury type or pelvic fracture type. In total, 78 (24.8%) patients were admitted to the intensive care unit (ICU), and there were no differences between the fracture subtypes (p = 0.399). However, AIS and ISS were significantly higher in patients admitted to the ICU (AIS: 26.94 ± 14.17 versus 11.01 ± 8.58, p < 0.001; ISS: 31.65 ± 13.81 versus 14.91 ± 10.35, p < 0.001).
Cause of injury and pelvic classification
The most common cause of injury was pedestrian–motor vehicle traffic accidents in 176 cases (55.9%), followed by falls from height in 69 cases (21.9%), inter-motor vehicle traffic accidents in 57 cases (18.1%), injuries from heavy objects in 6 cases (1.9%), and simple falls in 7 cases (2.2%). In addition, there was a significant difference based on fracture subtype and cause of injury (p < 0.001); type I fractures occurred mostly in simple falls, while most types II–IV were seen in pedestrian–motor vehicle traffic accidents.
Treatment
In total, 127 patients (40.3%) required blood transfusions, and there were no differences in the types of pelvic fractures. One patient with open fracture had pelvic packing, 12 patients with hemodynamic instability underwent angiography, and two patients underwent vascular embolization. However, there were differences based on injury mechanisms, with significantly more patients with fall from height injuries (41 (59.4%)) and inter-motor vehicle accidents (30 (52.6%)) needing a blood transfusion. In terms of the degree of injury, AIS and ISS were significantly higher in transfused patients than in non-transfused patients (AIS: 23.22 ± 13.70 versus 9.37 ± 7.14, p < 0.001; ISS: 28.02 ± 13.43 versus 13.00 ± 9.41, p < 0.001). Blood transfusion and ISS were associated risk factors for ICU admission. Pelvic fractures were treated conservatively in 242 cases (76.8%) and surgically in 73 cases (23.2%). Of 73 surgical patients, 71 were treated with external fixation and 2 were treated with plates and iliosacral screw fixation. Furthermore, combined acetabular fractures were found in 18 cases (5.7%) and 12 cases (66.7%) in males, with the highest percentage of patients (13 (13.8%)) classified as type IV fractures (p = 0.006). There were no differences in acetabular fractures based on injury mechanism or pelvic injury classification. Approximately 51.4% of patients received surgical treatment for problems that were not related to pelvic fractures. Among these, 30.2% necessitated surgical intervention on the lower limbs. Abdominal surgery was necessary in 19.0% of patients.
Associated injuries
In terms of associated injuries, there were 285 injuries (90.5%) associated with pelvic fractures, with most injuries occurring in the abdomen (64.8%) and lower extremities (47.6%), followed by the chest (45.4%) and head (34.6%) (Table 1); associated injuries required surgical treatment in 178 cases (56.5%). There were differences in associated injuries according to pelvic injury classification (p = 0.001), with type IIIB having the highest rate of associated injuries at 96.6%. Head (p = 0.036) and facial (p = 0.004) injuries were more common in type IIIA, while abdominal injuries (p = 0.007) were more common in type IIIB. Furthermore, we analyzed the injury sites and types and found that injuries to the head, chest, spine, and upper and lower extremities were significantly higher in falls from height compared with other causes (Table 2). In terms of specific sites, most injuries occurred in the lungs in 128 cases (40.6%), followed by the cranium in 69 cases (21.9%), which was also the most severe injury, and then the liver in 50 cases (15.9%). Finally, the highest number of extremity fractures was of the femur (61 (19.4%)), tibia (40 (12.7%)), and femoral neck (32 (10.2%)) (Table 5). After conducting statistical analysis on the number of injury sites, we discovered a significant increase in the rates of ICU admission (p < 0.001), blood transfusion (p < 0.001), and complications (p < 0.001) as the number of injury sites increased. However, we did not find any correlation between the mortality rate and the number of surgical sites (Table 3).
Specific injury situations and different injury mechanisms of each part.
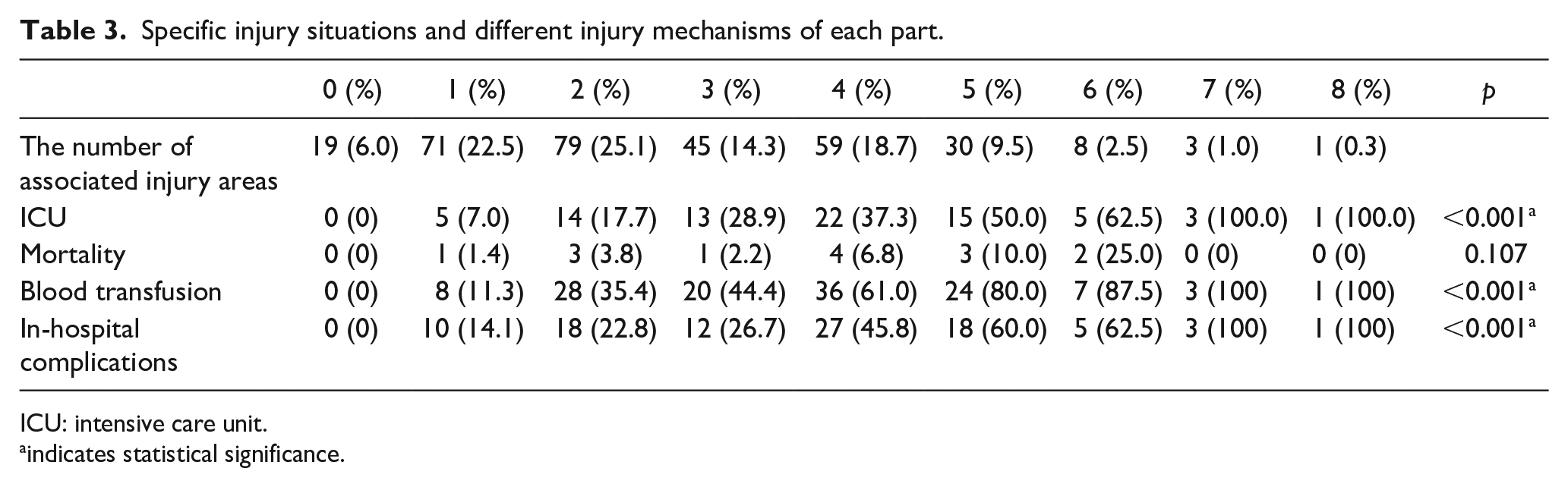
ICU: intensive care unit.
indicates statistical significance.
Mortality
A mortality rate of 4.4% was observed, with 14 deaths out of 315 patients. In injury mechanism, five cases were pedestrian–motor vehicle traffic accidents, six were inter-motor vehicle traffic accidents, and three were falls from height; there were no differences in mortality rates based on injury type or pelvic subtype. The causes of death were severe head trauma (seven patients), ruptured iliac vessels and severe pelvic fracture (one patient), blunt abdominal trauma (one patient), multiple organ failure (four patients), and pulmonary complications (one patient). The AIS and ISS were significantly higher in the patients who died (AIS: 29.50 ± 18.94 versus 14.28 ± 11.54, p < 0.001; ISS: 34.43 ± 11.86 versus 18.34 ± 13.05, p < 0.001).
Complications
In total, 94 patients (29.8%) had complications during hospitalization: 40 cases (12.7%) of shock, 37 cases (11.7%) of myocardial damage, 36 cases (11.4%) of electrolyte disturbance, 35 cases (11.1%) of hepatic impairment, and 33 cases (10.5%) of acute respiratory failure. Among the 40 patients with shock, 27 were of hemorrhagic shock, 11 were of traumatic shock, and 2 were of neurogenic shock. Among the 33 cases of acute respiratory failure, 15 were of central respiratory failure and 2 were of acute respiratory distress syndrome (Table 1). Regarding complications during hospitalization, there were differences based on injury mechanism (p = 0.001), with the highest complication rate in the fall injury group (32 cases (46.4%)). Respiratory failure (p < 0.001), electrolyte disorders (p = 0.044), traumatic coagulopathy (p = 0.021), and hyperuricemia (p = 0.042), which were all mostly observed with fall from height injuries, were mainly related to the degree of injury (Table 4). There were no differences in complications according to age, and its occurrence was mainly related to the severity of the injury. Of the 33 complications observed, 16 (53.3%) differed according to AIS, and 17 (56.7%) differed according to ISS; the rate of complications was significantly higher when AIS and ISS were higher. In 13 patients with complications (43.3%), there was a difference in the length of hospital stay, resulting in a significantly increased length of hospital stay in the study population.
Association between AIS and ISS with complications.
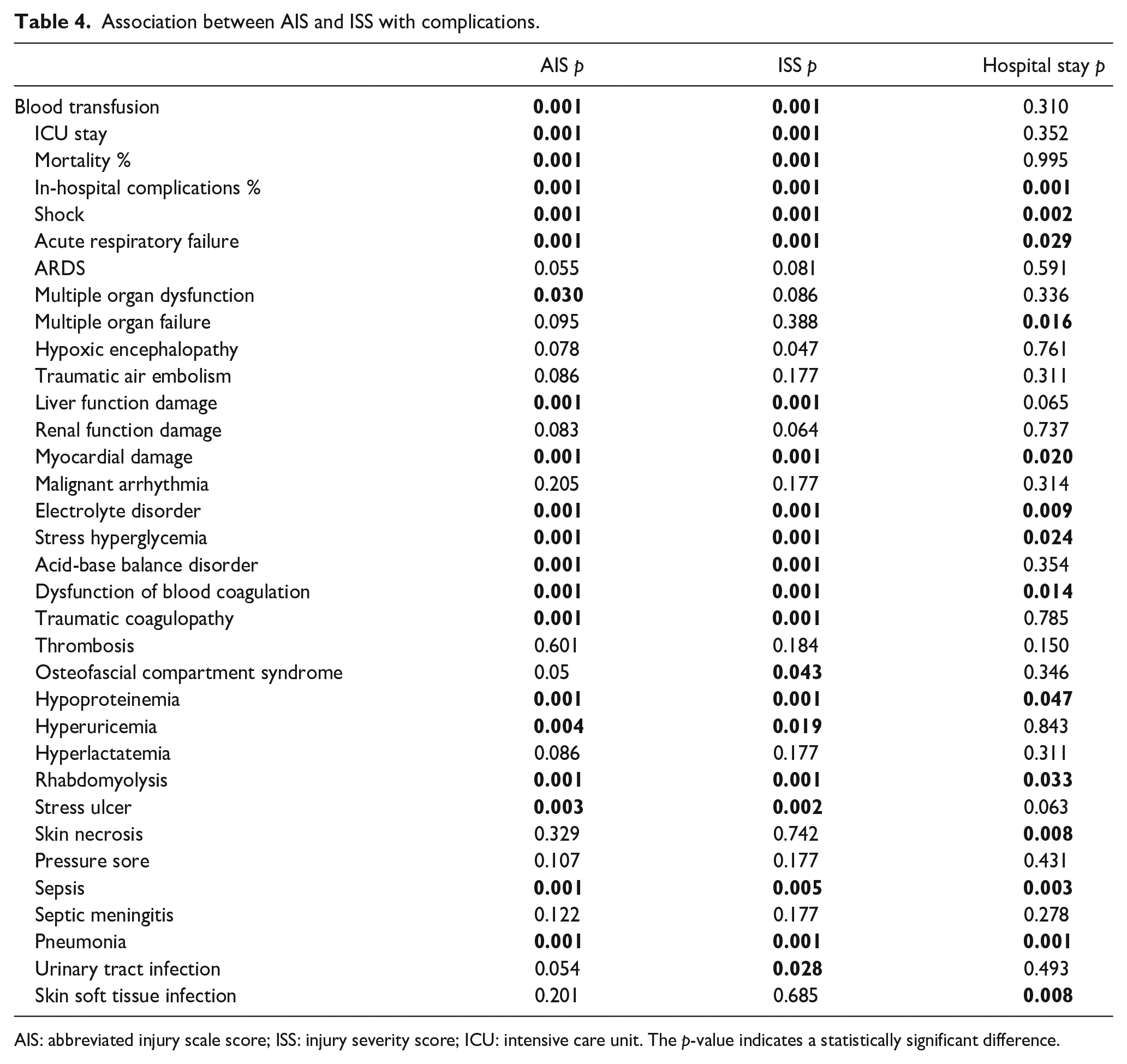
AIS: abbreviated injury scale score; ISS: injury severity score; ICU: intensive care unit. The p-value indicates a statistically significant difference.
Specific injuries at each site.
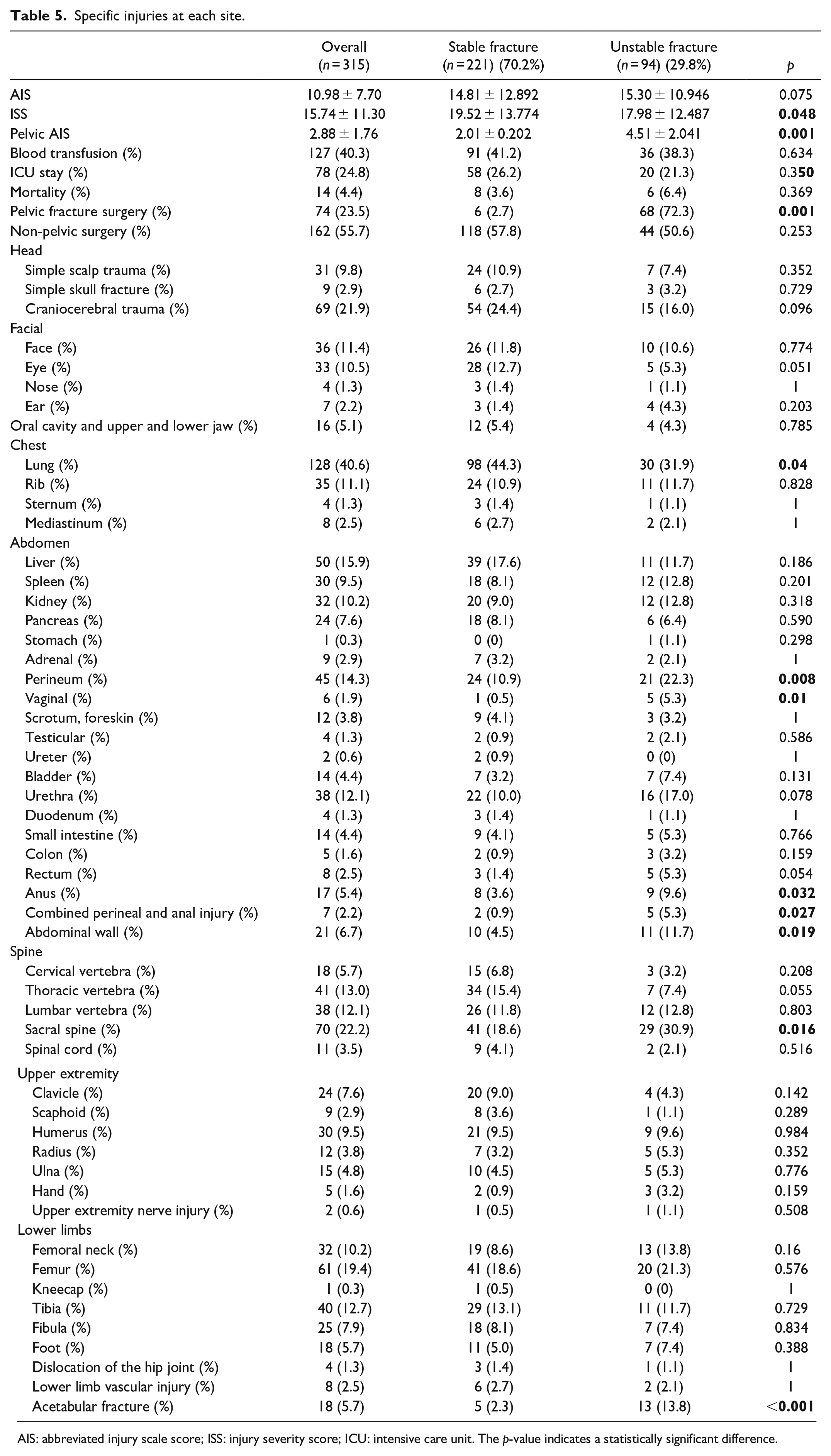
AIS: abbreviated injury scale score; ISS: injury severity score; ICU: intensive care unit. The p-value indicates a statistically significant difference.
Discussion
This single-center study described the clinical characteristics, injury patterns, associated injuries, and complications of 315 pediatric pelvic injury cases at a children’s hospital. The pediatric population rarely experiences pelvic fractures often caused by high-energy trauma, including those resulting from pedestrian–motor vehicle traffic accidents, inter-motor vehicle traffic accidents, and falls from heights. In this study, we observed that pedestrian–motor vehicle traffic accidents were the most common mechanism of injury, similar to pelvic fracture in adult patients, 6 in line with previous findings.7,8 Although the mechanisms of injury that cause pelvic fractures in adults are similar, pediatric patients appear to have a more stable fracture pattern. In particular, among our patients, there were 69 cases of injuries caused by falling from a height, which was less reported in the previous medical records. The overall injuries of these patients were serious, but most of them were stable pelvic fractures, which means that children’s pelvis can absorb more energy than adults when suffering from high-energy injuries. Notably, 70.2% of our patients had stable fractures and a much lower percentage of pelvic fractures requiring surgery.
Rapid fatal blood loss from pelvic fractures in children is extremely rare, but it remains a major and common cause of early death in adult patients with multiple injuries. This discrepancy may be attributed to the vasoactive nature of children’s blood vessels, which are more prone to constriction than the more vulnerable atherosclerotic adult vessels. Blood transfusion was required by 127 (40.3%) of our patients, similar to the 17%–46% reported in previous studies. The indication for blood transfusion is not primarily to resuscitate life-threatening hypovolemia but restore the red blood cell count. 9 However, from our medical records, shock occurred in 40 cases (12.7%); there was a correlation between blood transfusion and shock (p < 0.001), meaning that a proportion of patients underwent transfusion because of shock. Regarding the degree of injury, AIS and ISS were significantly higher in transfused patients than in non-transfused patients. There was no difference between whether the pelvic fracture was operated on and the need for a blood transfusion. However, for non-pelvic fracture surgeries, there was a correlation with blood transfusion. Ismail et al. 2 concluded that the source of hemodynamic instability in the pediatric population is more from visceral rather than pelvic vascular system disruption. The degree of patient’s injury was significantly associated with the blood transfusion, while AIS and ISS did not differ between different pelvic fracture subtypes, suggesting that pelvic fractures are not a major contributor to blood loss and death in children.2,10
In our patients, 308 cases (95.9%) were caused by high-energy injuries, and 285 cases (90.5%) had associated injuries, indicating that high-energy injuries often result in a higher number of associated injuries in children with pelvic fractures.11 –13 In our medical records, abdominal and lower extremity injuries were the most common, followed by chest and head injuries. The incidence of associated injuries reported by others ranges between 60% and 80.8%, while the rates previously reported were slightly higher.5,7,13 The most common abdominal injury locations were the liver (50 (15.9%)), kidney (32 (10.2%)), and spleen (30 (9.5%)). Although the spleen was the third most common abdominal parenchymal organ injury, eight patients were treated surgically for splenic rupture: one was repaired, while the remaining seven were resected. This indicates that the abdominal parenchymal organ is the most common injury site and one of the main causes of bleeding. Small bowel injury occurred in 14 cases (4.4%); although the incidence was not high, there were six cases of intestinal perforation and five cases of intestinal rupture treated surgically, with a high morbidity and mortality rate, and a high postoperative complication rate, which also occurred in traffic accident injuries. Therefore, the risk of abdominal cavity organ injury in traffic accident injuries should also be considered. Although the overall incidence is low, it can lead to serious abdominal complications and must be diagnosed and treated early. As previously suggested,12,14 patients with intra-abdominal injuries, especially visceral cavity perforations, are sometimes missed. It is difficult to interpret the signs in traumatized children, as seen in patients with small bowel injuries in this study. Our findings indicate that all patients with significant abdominal organ injury had stable fractures. Children’s skeletal development was incomplete, with a higher proportion of cartilage components present. Consequently, when children experience higher levels of violence, their pelvis tends to resemble a structure known as the “energy absorption box.” This often results in more frequent injuries, with the abdominal organs absorbing a greater amount of damaging energy. In addition, this can also lead to tiny fractures in the pelvic region. Hence, it was crucial to prioritize the assessment of abdominal parenchyma and organ damage in patients with stable pelvic fractures. In addition, thorough examination of the abdomen was necessary in patients with pelvic fractures to detect potential signs of perforated peritonitis such as high fever and severe abdominal pain, to prevent misdiagnosis. In children with pelvic fractures, perineal to anal injuries were the most frequent injuries, with 58 cases (18.4%), 47 (81.0%) that occurred due to pedestrian–motor vehicle traffic accidents, indicating that these patients were more likely to have perineal injuries. Combined perineal, anal, and rectal injuries occurred in seven cases (2.2%). Furthermore, unstable pelvic fractures were more likely to have perineal trauma, vaginal trauma, anal trauma, and combined perineal-anal injuries. Female patients were more likely to have perineal injuries due to their anatomical peculiarities. However, the incidence of urethral injuries was higher in male patients, with 32 cases (84.2%), 27 (71.1%) of which were due to pedestrian and motor vehicle traffic accidents, a result reported in previous literature. 15
Femoral and tibial fractures are the most common fractures of the extremities. Spinal fractures, mainly of the thoracic spine, are the most commonly associated fractures of the axial skeleton,8,9,16,17 of which 32 cases (78.0%) occurred in fall injuries, followed by the lumbar spine with 28 cases (73.7%) associated with falls from height. These findings are similar to our findings. Furthermore, scaphoid fractures were more common in falls from height injuries (seven cases (77.8%)). Mediastinal injuries were most common in falls from height (six cases (75.0%)). The acetabular fracture incidence was 5.7%, higher in unstable pelvic fractures. In our patients, no acetabular fracture occurred in isolation—all were combined with other pelvic fractures, unlike in previous reports.9,18 This was probably due to the overall young age of our patients and the fact that acetabular fractures rarely occur alone in younger children due to anatomical peculiarities. It could also be that acetabular fractures in children tend to occur after triradiate cartilage closure. Lu et al. 19 reported that children with skeletal immaturity were less likely to have acetabular fractures compared with skeletally mature patients (12% versus 37.5%), and no acetabular fractures were found in our skeletally mature patients, which may be related to both the age of the child and the type of injury. For stable and unstable fractures, we found higher ISSs for stable fractures, meaning that stable fractures may be more likely to be combined with other injuries; for unstable fractures, owing to partial energy absorption, the associated injuries are less severe. The combined injury required surgical treatment in 78 cases (56.5%). This indicates that the severity of the combined injury is relatively high, and the diagnosis and treatment of associated injuries, especially internal organs such as the head and abdomen, need more attention in the early stages compared with pelvic fractures.
The mortality rate was 4.4%, including seven deaths (50%) from craniocerebral trauma and four (28.6%) from multiple organ failure; children with pelvic fractures died from associated injuries, similar to previous reports.2,13,20 –22 No relationship was found between the Torode–Zieg classification and mortality, which is consistent with previous studies. 8 The AIS and ISS differed between deceased and surviving patients, with significantly higher AIS and ISS in deceased patients; this validates the concept that more extensive patient injury is associated with increased mortality, as previously reported. 10
Based on medical records, head injury was one of the main causes of death in patients, and nine patients (13.0%) had severe or very severe craniosynostosis, which correlated with death. However, in patients with severe craniosynostosis, the pelvic fractures were types IIIA and IIIB, which are often stable fractures, indicating that pelvic fractures are not the main cause of death in children.
Previous studies have reported few complications during hospitalization for pelvic fractures21,23,24; however, children with combined pelvic fractures are at an increased risk of complications, such as infection, neurological injury, and acute respiratory failure during hospitalization. Zwingmann et al. 23 noted that postoperative complications, such as acute respiratory distress syndrome, venous thromboembolism, and multiorgan failure, are less common in children than adults, and severe complications often affect survival in children. We demonstrated a relatively high rate of complications during hospitalization at 29.8%, which were mainly related to the severity of the injury and not to the pelvic fracture itself. Meanwhile, serious complications were associated with death and a significant length of hospital stay. Mulder et al. 21 reviewed 163 pediatric pelvic patients and showed a mean ISS of 23 and a 21% incidence of shock. In this study, the incidence of shock was 12.7%, which may be related to the relatively low mean ISS of 19. Askegard-Giesmann et al. 25 showed that pelvic fractures were associated with an increased risk of venous thromboembolism. In our results, there was no correlation between pelvic fracture and risk of thrombosis, which may be related to the overall young age of our patients and the low incidence of thrombosis. Venous thromboembolism does not appear to cause significant morbidity or mortality in the pediatric population and may not require the regular use of thromboprophylaxis, especially in younger children. 26
Limitations
This study has some limitations. First, because it was a retrospective design, our study was subject to selection bias and confounding factors. Pelvic fractures of the types I were frequently treated in the outpatient department. However, because the majority of our patients were inpatients, there was a bias in the results due to the small number of type 1 patients. In addition, all data were from a single care center in one city and may not represent all institutions. Second, our study on complications was limited only to the inpatient period and lacked a study on complications in long-term follow-up of pelvic fractures. In addition, long-term morbidity and quality of life scores were not studied, which are certainly useful to the analysis and should ideally be collected prospectively to reduce bias.
Conclusion
This study showed that high-energy impact injuries often cause pelvic fractures in children, the majority of which are stable. Children who have pelvic fractures frequently require hospitalization due to the presence of severe injuries in other areas of their bodies. While the fall damage may be severe, it frequently results in a stable pelvic fracture. The treatment of other combined injuries should receive greater attention in the context of hospitalized stable pelvic fractures. IIIB pelvic fractures frequently occur in conjunction with more severe abdominal injuries; therefore, the prompt management of cavity and organ injuries is of particular importance. Blood transfusion and ISS were associated risk factors for ICU admission.
Supplemental Material
sj-pdf-1-cho-10.1177_18632521241237933 – Supplemental material for Associated injuries and complications in pediatric pelvic fractures requiring hospitalization: A series of 315 cases
Supplemental material, sj-pdf-1-cho-10.1177_18632521241237933 for Associated injuries and complications in pediatric pelvic fractures requiring hospitalization: A series of 315 cases by Baojian Song, Qiang Wang, Wei Feng, Danjiang Zhu, Ziming Yao and Xuejun Zhang in Journal of Children’s Orthopaedics
Footnotes
Author contributions
B.S. contributed to article preparation, study design, and collection and analysis of data. Q.W. contributed to study design and article preparation. W.F. contributed to study design and article preparation. D.Z. contributed to study design and article preparation. Z.Y. contributed to study design and article preparation. X.Z. contributed to article preparation, study design, and analysis of data.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.