
Abstract
Background:
Congenital scoliosis is often associated with costal deformities, of which a bilateral bifid intrathoracic rib is very rare. The aim of this study was to retrospectively summarize the clinical manifestations, imaging characteristics, treatment strategies, and postoperative outcomes of five patients with bilateral bifid intrathoracic rib.
Methods:
We retrospectively reviewed the imaging findings and medical records of five pediatric patients (two girls, three boys) with bilateral bifid intrathoracic rib who were surgically treated for congenital kyphoscoliosis (mean age = 8 years). The clinical manifestations, imaging characteristics, treatment strategies, and postoperative outcome were summarized.
Results:
Four of five patients showed abnormalities from birth. All five patients presented with kyphoscoliosis and a fused vertebral body or lamina. The bilateral bifid intrathoracic rib was located at T2–3 in three patients, T7 in one patient, and T10 in one patient. Various congenital spinal deformities and multiple system malformations were present in all five patients. Three patients had preoperative neurological deficits. For corrective surgery, one patient received a traditional growing rod implantation, one patient underwent resection of a bony septum, and three patients underwent spinal osteotomy. One patient suffered complete paralysis of the lower limbs after surgery.
Conclusion:
Bilateral bifid intrathoracic rib is a rare anomaly that typically occurs in patients with serious kyphoscoliosis. Bilateral bifid intrathoracic rib patients show similar clinical and radiological characteristics and are likely to exhibit neurological deficits before or following corrective surgery. Spinal surgeons should be aware of the high risk of permanent neurological complications related to surgery in these patients.
Level of evidence:
level IV.
Keywords
Introduction
Congenital scoliosis is caused by abnormal vertebral development in utero (at 4–6 weeks of gestation), leading to curvature of the spine. 1 Although the presence of anomalous ribs is common in patients with congenital scoliosis, a bifid intrathoracic rib is a very rare condition.2 –4 Intrathoracic ribs typically occur singly and unilaterally. 5 To our knowledge, surgical treatment for congenital kyphoscoliosis with a bilateral bifid intrathoracic rib (BBIR) has not been reported. BBIR is a rare type of rib that runs through the thorax, formed by a congenital bony fusion anterior to the spine. This fusion frequently results in kyphosis, spine subluxation, and accompanying neurological symptoms. Herein, we describe five cases of congenital kyphoscoliosis with BBIR. We also review the clinical characteristics and surgical outcomes of this syndrome and discuss practical considerations for treating this deformity.
Materials and methods
We included five children with BBIR, which collected over time by the senior author, and who underwent consecutive surgical treatment of spinal deformities between 2010 and 2020. The required information was collected from each patient’s clinical and hospital chart, including preoperative plain radiographs, computed tomography (CT) scans with three-dimensional reconstructions, and magnetic resonance images (MRI) of the whole spine. Medical records and imaging studies for these patients were reviewed.
Imaging features of the patients were characterized according to the type of spinal deformity, scoliosis Cobb angle, kyphotic Cobb angle, bifid rib location, and intraspinal deformities. Therapeutic measures, surgical outcomes, and complications were reviewed. Clinical and radiological data are summarized in Table 1.
Demographic, medical, and surgical characteristics of five patients with a bilateral bifid intrathoracic rib.
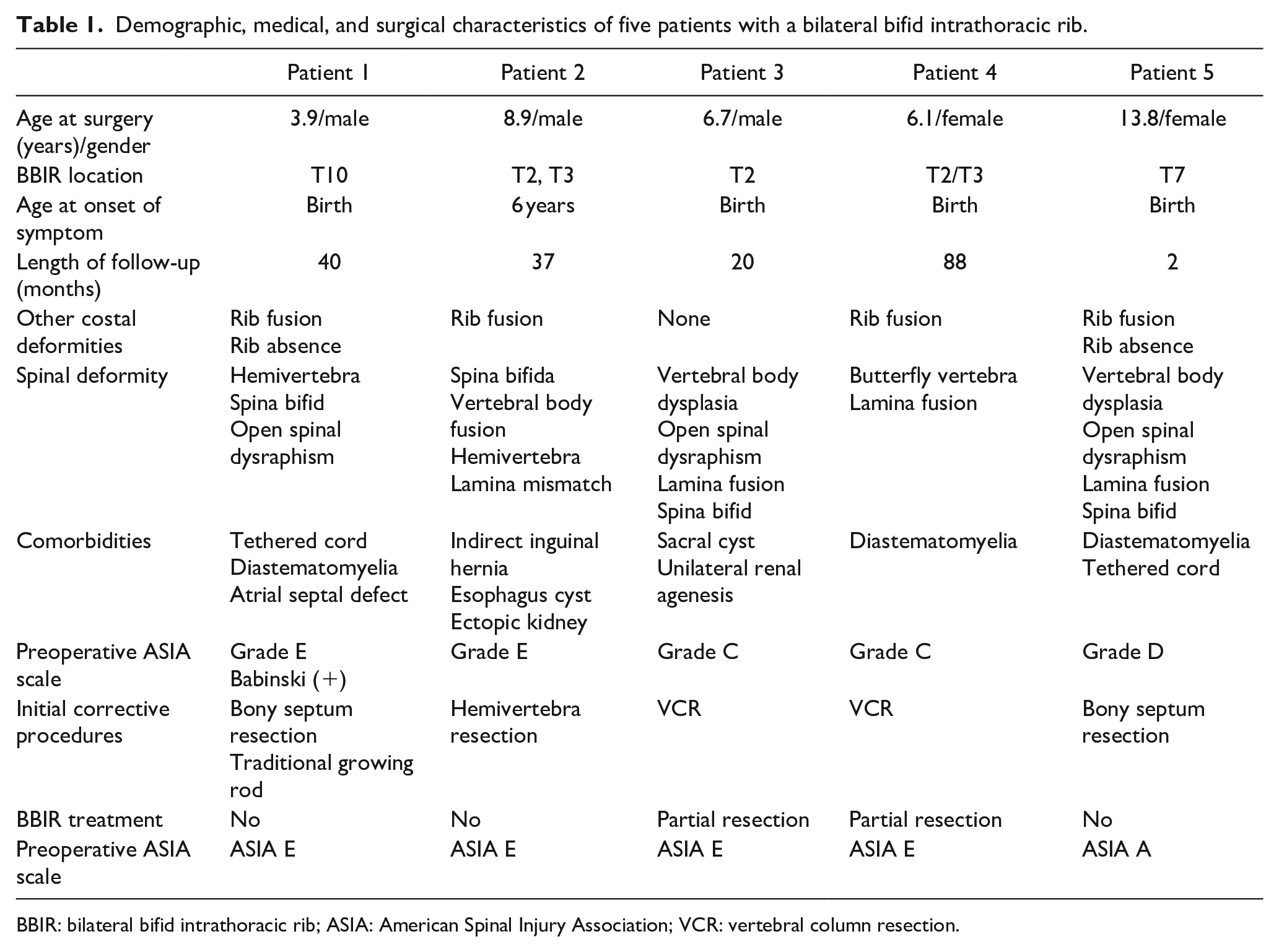
BBIR: bilateral bifid intrathoracic rib; ASIA: American Spinal Injury Association; VCR: vertebral column resection.
Source of funding
There was no external funding for this project.
Results
Patient 1
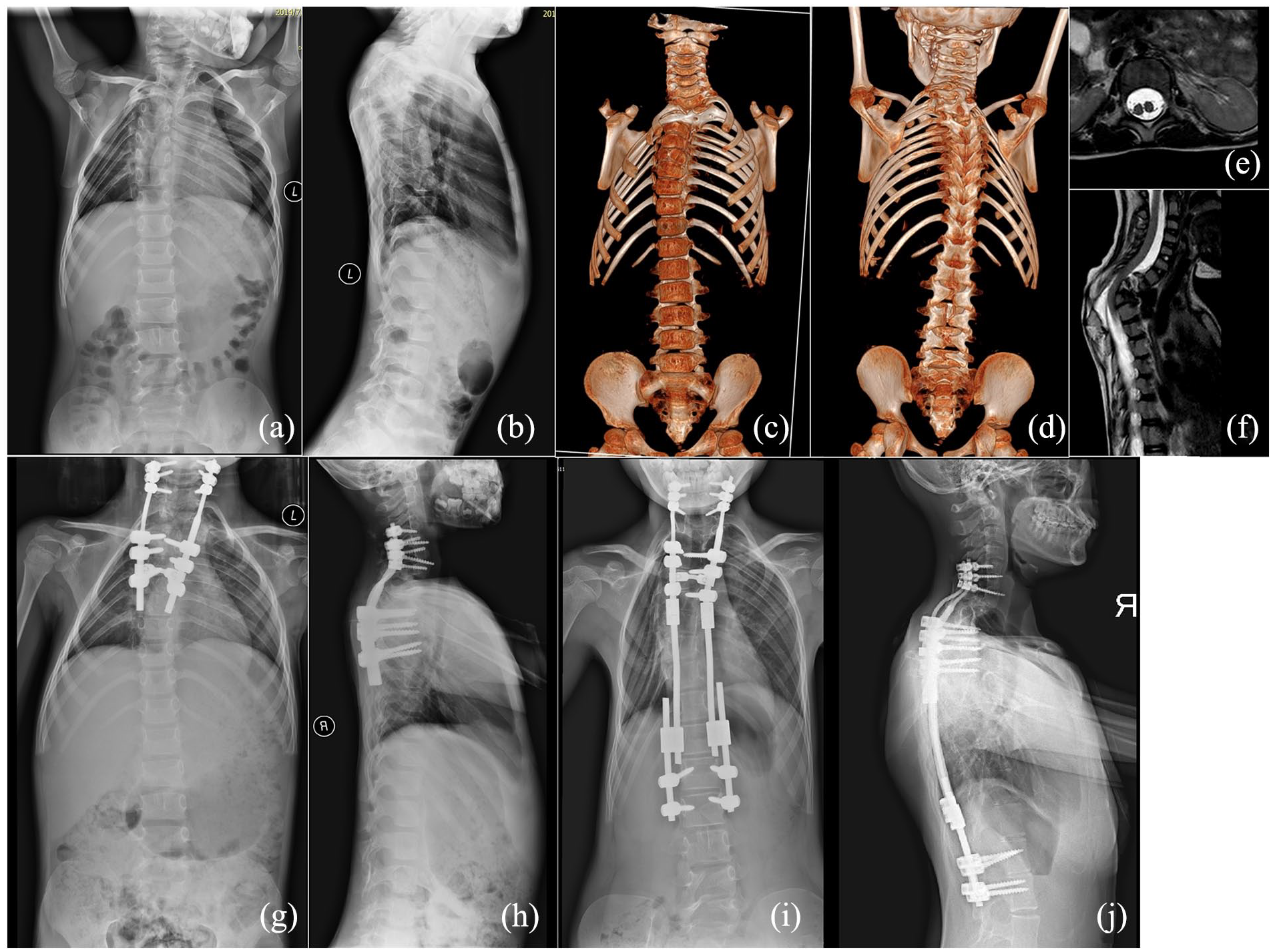
A 4-year-old boy presented with an uneven back since birth, which gradually worsened over time. He received interventional closure for an atrial septal defect at 2 years old, after which he was referred to our hospital. His plain spinal radiographs showed a thoracolumbar scoliosis Cobb angle of 57° and a kyphosis Cobb angle of 70° (Figure 1), indicating the requirement for surgical correction. CT revealed multiple costal and spinal deformities, including fusion of the right 6th and 7th rib, BBIR of the 10th rib, absence of the bilateral 12th rib, left T11 hemivertebra, open spinal dysraphism from the thoracic to the sacral vertebra, and bony diastematomyelia from T12 to L2. MRI showed a tethered cord and diastematomyelia from T12 to L2. Upon physical examination, in addition to a positive Babinski sign, no other positive neurological findings were noted. Furthermore, no abnormalities in pulmonary function were observed.
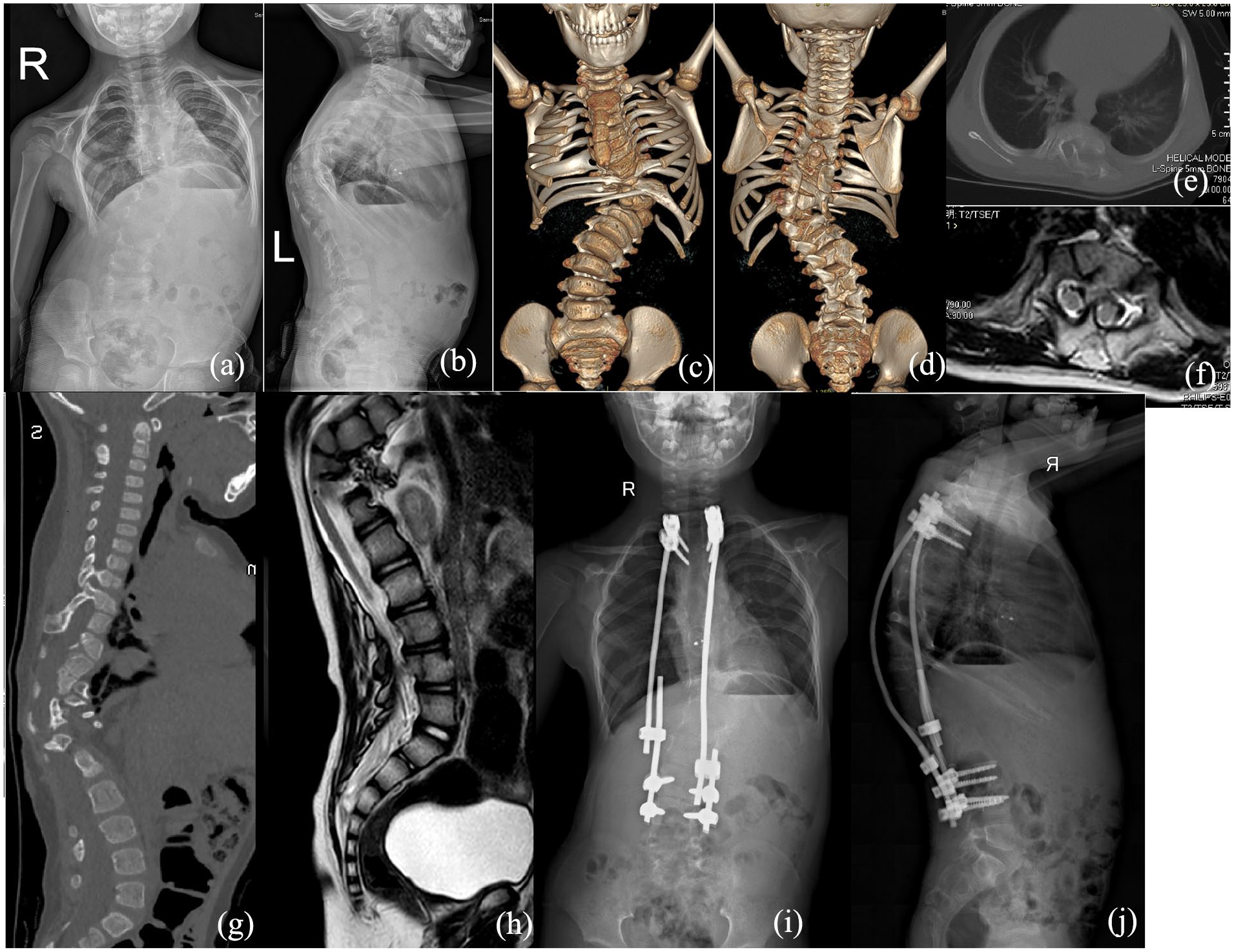
Findings in patient 1. (a) and (b) Preoperative anteroposterior and lateral spinal radiographs showing thoracolumbar scoliosis and kyphosis. (c) and (d) Anterior and posterior views of three-dimensional computed tomography showing a bifurcated 10th rib and various other costal and spinal deformities. (e) and (f) Computed tomography scan and magnetic resonance imaging showing T6–T7 diastematomyelia with a bony septum. (g) and (h) Sagittal CT and MR image at the site of pathology. (i) and (j) Postoperative anteroposterior and lateral spinal radiographs showing partial correction of the thoracolumbar scoliosis and kyphosis.
Resection of the bony septum and insertion of a traditional dual growing rod were performed. T2–T3 and L2–L3 were used as the proximal and distal anchors, respectively. The scoliosis and kyphosis Cobb angles improved to 33° and 38°, respectively. Growing rod distractions were performed at approximately 6-month intervals. The patient had no neurological or instrumentation-related complications.
Patient 2
A 9-year-old boy was admitted to our department for a shoulder imbalance that developed when he was 6 years old. His medical history was remarkable in that he underwent esophageal cyst resection and high ligation of the hernia sac for an oblique inguinal hernia and had a right ectopic kidney. The physical examination indicated normal limb muscle strength and tone in this patient, with no significant respiratory abnormalities. Limited cervical spine motion, approximately 50% of normal, was observed, alongside an absence of neurological symptoms. Spinal radiographs during initial assessment in our clinic revealed left upper thoracic scoliosis and kyphosis Cobb angles of 44° and 42°, respectively (Figure 2). CT showed BBIR of the second and third ribs, fusion of the left third and fourth ribs, left T3 hemivertebra, T4–T5 block vertebrae, and multiple lamina mismatches. His spinal MRI showed no spinal cord abnormality.
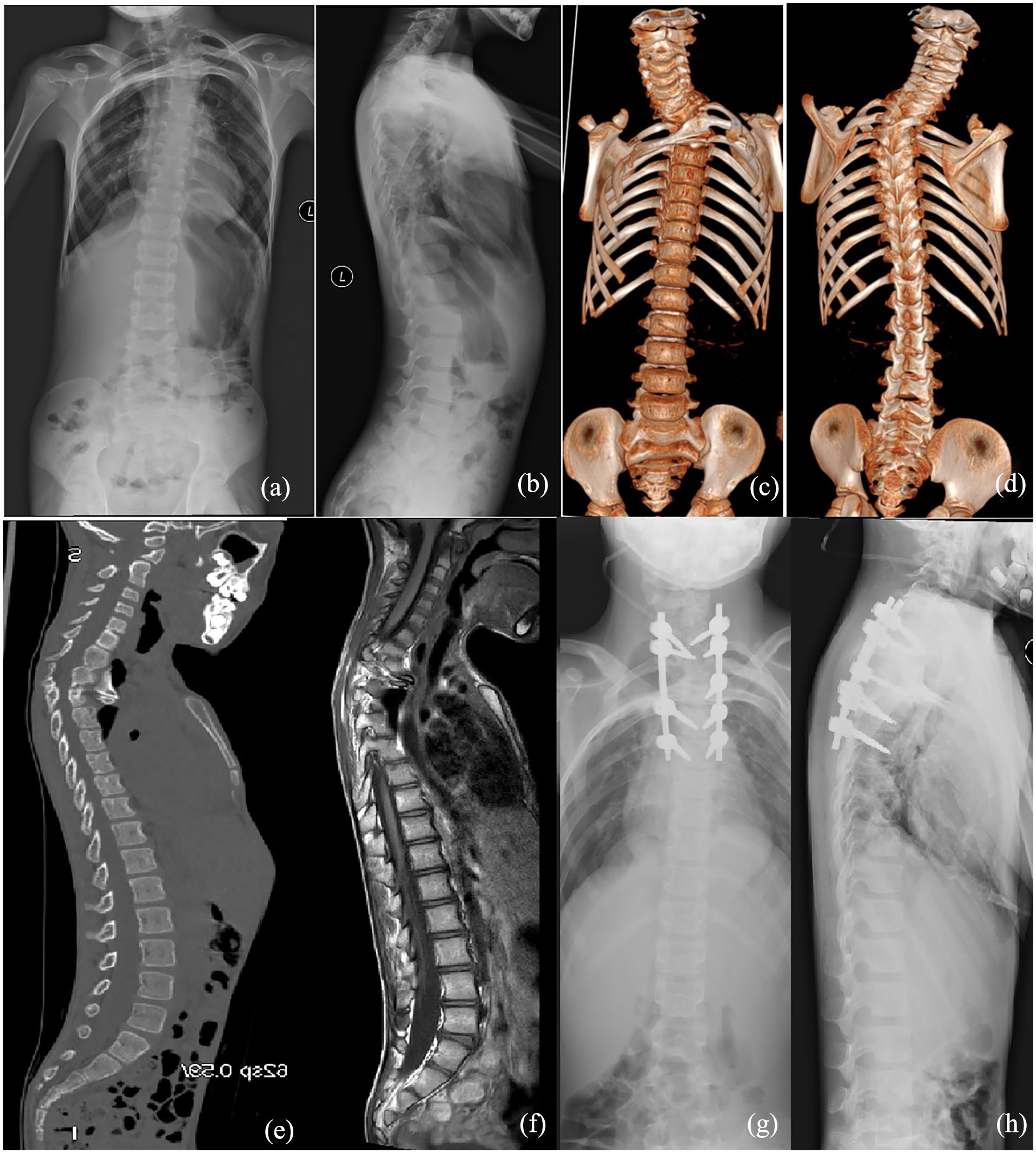
Findings in patient 2. (a) and (b) Preoperative anteroposterior and lateral spinal radiographs showing upper thoracic kyphoscoliosis. (c) and (d) Anterior and posterior views of computed tomography reconstruction showing bilateral bifid intrathoracic ribs (second and third ribs), left T3 hemivertebra, rib fusion, and other spinal deformities. (e) and (f) Sagittal CT and MR image at the site of pathology. (g) and (h) Postoperative anteroposterior and lateral spinal radiographs showing partial correction of the thoracic kyphoscoliosis.
T3 hemivertebra resection with fixation from T1 to T7 was performed. His scoliosis and kyphosis Cobb angles improved to 18° and 22°, respectively. There were no neurological or other complications within his 3-year follow-up.
Patient 3
A 7-year-old boy presented with an uneven back since birth and claudication of the left lower limb for 1 month. Physical examination showed grade 3 muscle strength in the left lower limb, weakened abdominal reflexes and testicle raising reflex, and a bilateral Babinski sign (+), with a resulting American Spinal Injury Association (ASIA) impairment scale grade of C. Abdominal ultrasound showed congenital absence of the right kidney.
Spinal radiographs showed left upper thoracic scoliosis and kyphosis Cobb angles of 30° and 55°, respectively (Figure 3). CT showed BBIR of the second rib, dysplasia of the T2 and T3 vertebra, T2–T4 block lamina, and open spinal dysraphism from the lumbar to the sacral vertebra. Spinal MRI revealed spinal cord compression at the kyphotic apex.
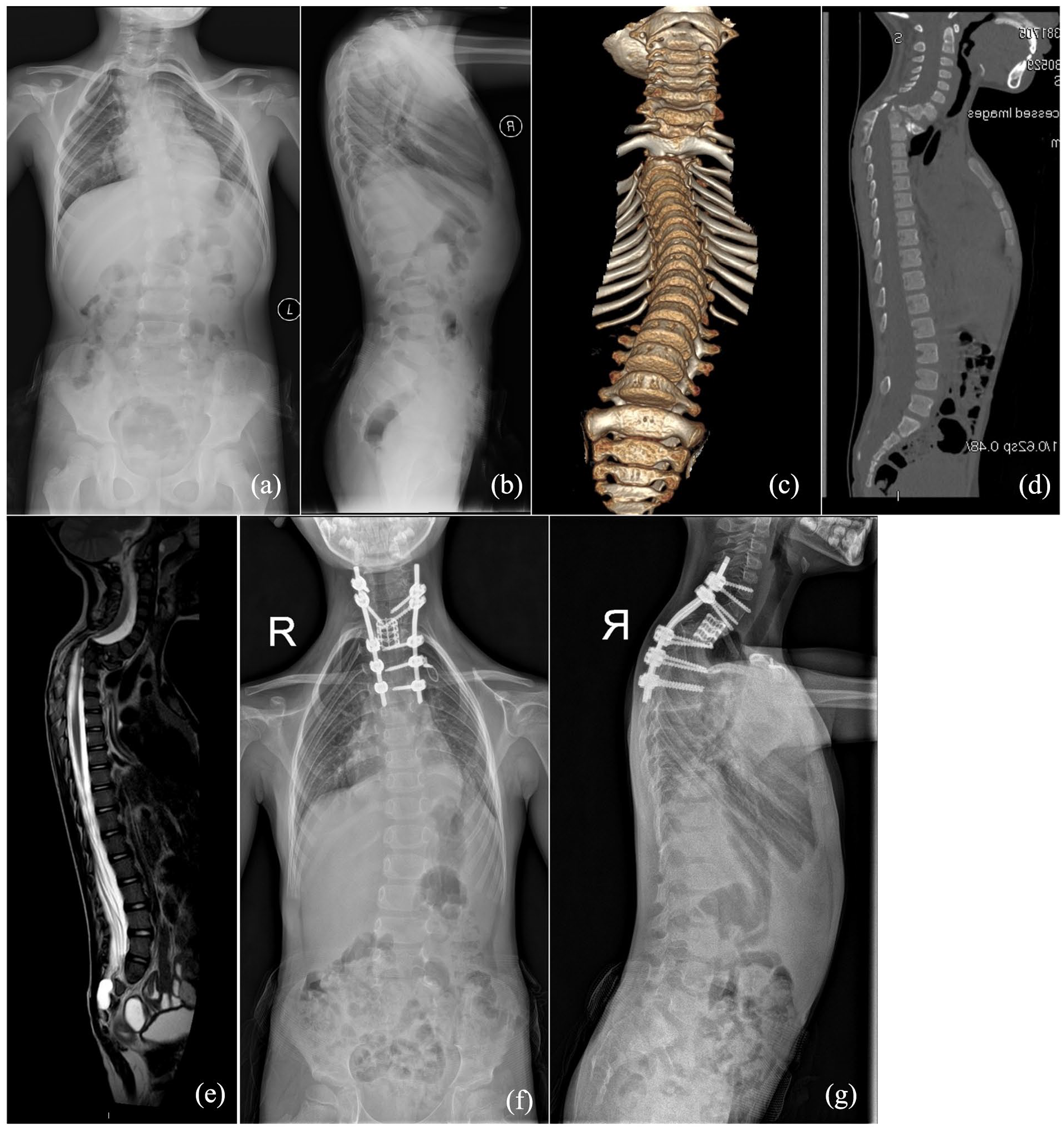
Findings in patient 3. (a) and (b) Preoperative anteroposterior and lateral spinal radiographs showing upper thoracic kyphoscoliosis. (c) and (d) Anteroinferior view and median sagittal plane of computed tomography reconstruction showing a bilateral bifid intrathoracic rib (second rib) and local angular kyphosis. (e) Magnetic resonance imaging showing spinal cord compression at the kyphotic apex and a sacral canal cyst. (f) and (g) Postoperative anteroposterior and lateral spinal radiographs showing satisfactory correction of kyphoscoliosis after vertebral column resection.
Vertebral column resection (VCR) of T2 and T3, anterior reconstruction with titanium mesh, and fixation from C7 to T6 were performed. His scoliosis and kyphosis Cobb angles improved to 6° and 32°, respectively. There were no neurological or other complications within his 2-year follow-up.
Patient 4
A 6-year-old girl presented with an uneven back since birth and lower limbs weakness for half month. Physical examination showed grade 3 muscle strength of both lower limbs, weakened abdominal reflexes, and a bilateral Babinski sign (+), with a resulting ASIA scale grade of C.
Spinal radiographs showed left upper thoracic scoliosis and kyphosis Cobb angles of 30° and 62°, respectively (Figure 4). CT showed BBIR of the second and third ribs, dysplasia of the T2 and T3 vertebra, T7 butterfly vertebra, T2–T4 block lamina, and open spinal dysraphism from the lumbar to the sacral vertebra. Spinal MRI revealed spinal cord compression at the kyphotic apex and diastematomyelia at the middle thoracic level.
Findings in patient 4. (a) and (b) Preoperative anteroposterior and lateral spinal radiographs showing upper thoracic kyphoscoliosis. (c) and (d) Anterior and posterior views of computed tomography reconstruction showing bilateral bifid intrathoracic ribs (second and third rib) and other spinal deformities. (e) and (f) Axial and sagittal magnetic resonance imaging showing diastematomyelia at the lower thoracic level and spinal cord compression at the kyphotic apex. (g) and (h) Postoperative anteroposterior and lateral spinal radiographs showing partial correction of the kyphoscoliosis. (i) and (j) Anteroposterior radiograph after revision.
VCR of T2 and fixation from C5 to T7 were performed. The scoliosis and kyphosis Cobb angles improved to 4° and 22°, respectively. Her ASIA scale improved to grade E at 3 months after surgery. At 2-year follow-up, a distal adding-on phenomenon occurred, and the growing rod technique was used to correct the distal curve, with connection of the primary rods by serial connectors and fixation of L1–L2. Yearly growing rod distractions were performed. No neurological or other complications occurred within the 2 years after revision surgery.
Patient 5
A 14-year-old girl presented with dermal sinus tracts (posterior midline, about L2-L3) and an uneven back since birth. Neurological examination revealed decreased perianal sensation and a bilateral Babinski sign (+), with a resulting ASIA scale grade of D. Spinal radiographs revealed a left long curve and kyphosis, with Cobb angles of 45° and 100°, respectively (Figure 5). CT showed BBIR of the seventh rib, absence of multiple left ribs, dysplasia of multiple lower thoracic vertebra, lamina block from T4–L1, bony diastematomyelia from T10–T11, and open spinal dysraphism from the lumbar to the sacral vertebra. Spinal MRI revealed spinal cord compression at the kyphotic apex and diastematomyelia below the apex.
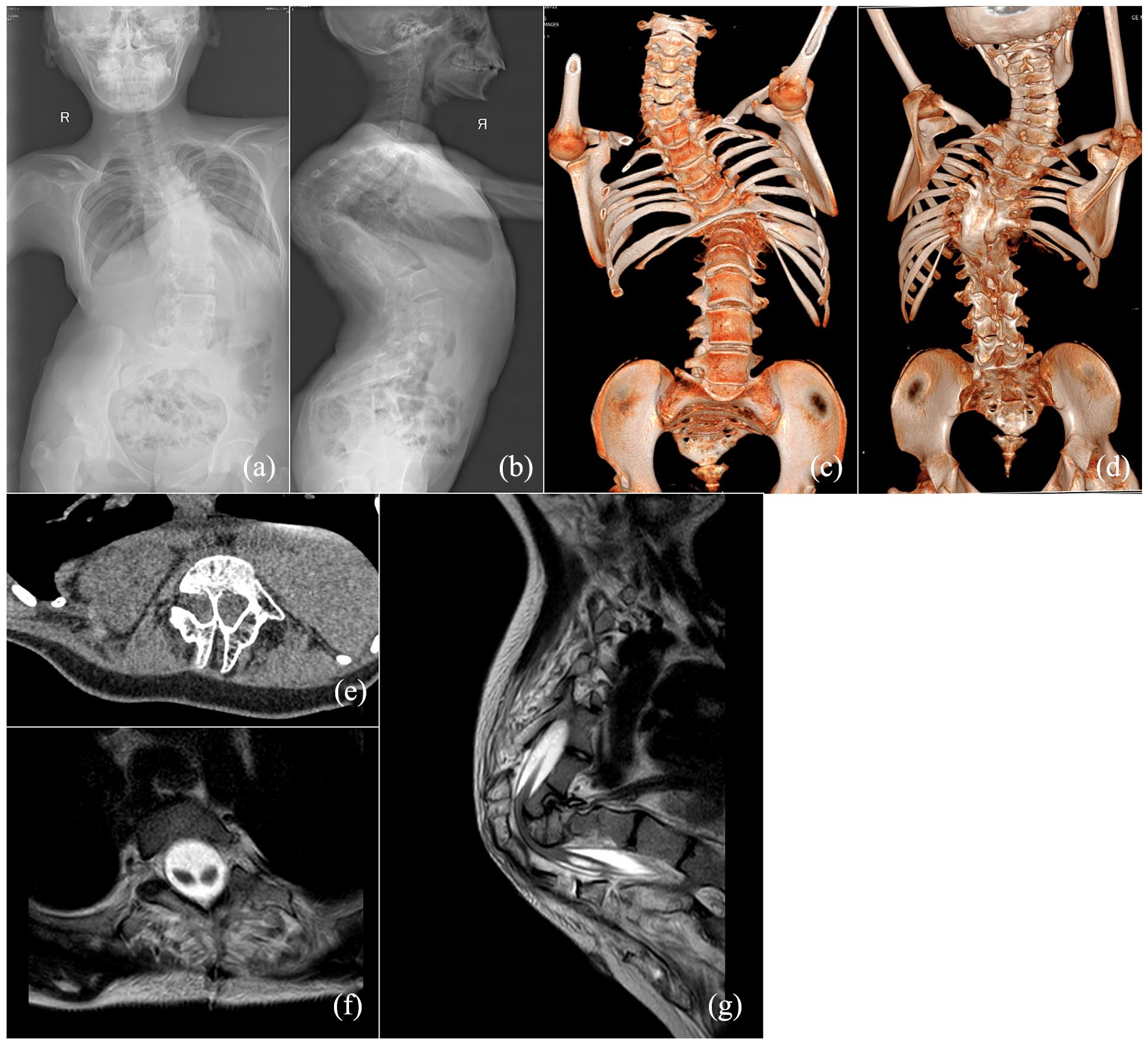
Findings in patient 5. (a) and (b) Preoperative anteroposterior and lateral spinal radiographs showing thoracic scoliosis and severe kyphosis. (c) and (d) Anterior and posterior views of computed tomography reconstruction showing a bilateral bifid intrathoracic rib (seventh rib) and other spinal deformities. (e) and (f) Axial computed tomography and magnetic resonance imaging showing bony diastematomyelia below the kyphotic apex. (g) Sagittal magnetic resonance imaging showing spinal cord compression at the kyphotic apex.
We planned a two-stage surgery, with bony septum resection in the first stage, a period of halo-gravity traction, and then VCR of the kyphotic apex in the second stage. However, the bony septum resection was associated with approximately 50% loss of the transcranial motor-evoked potential amplitude. After she regained consciousness from anesthesia, there was no voluntary movement of her left lower limb, and complete paralysis of both lower limbs occurred within 48 h after returning to the ward. Thus, she did not receive the corrective spinal surgery.
Discussion
Congenital malformation of the ribs and chest wall are often found in association with congenital spine deformities. 6 In 2005, Tsirikos et al. 6 reported 119 patients (19.2%) with rib anomalies from 620 patients with congenital spine deformities. In that study, the most common simple rib anomaly was a localized fusion of two or three ribs, and the most common complex rib anomaly was an extensive fusion of multiple ribs associated with a large adjacent chest wall defect. In 2013, Xue et al. 3 reported an incidence of rib anomalies of 50.3% in surgical patients with congenital scoliosis, in whom rib absence was the most common numerical abnormality and a fused rib was the most common structural abnormality. In 2015, Ghandhari et al. 4 reported an incidence of rib anomalies of 57.4% in surgical Caucasians with congenital scoliosis, and the majority of rib changes were of simple type. Note that the bifid ribs reported in these studies were all unilateral, and BBIR was rarely reported.
An intrathoracic rib is a rare anomaly and is usually an incidental finding, while intervention is seldom necessary because it is normally benign and asymptomatic.5,7,8 Intrathoracic ribs typically occur singly and unilaterally. In 2006, Kamano et al. 5 reported a case with a unilateral bifid intrathoracic rib found by CT, and after a review of 41 reported cases of intrathoracic supernumerary rib, they provided a classification for this condition. Note that all cases in their classification only had a unilateral intrathoracic rib. In 2020, Xue and Zhao 8 presented a case with a bifurcated intrathoracic rib articulated with the anterior aspect of T5, and they performed posterior spinal fusion to correct the concurrent kyphoscoliosis. To date, this study contains the largest number of reported BBIR cases.
BBIR has distinct morphological characteristics. A bifurcated intrathoracic rib can occur in any thoracic segment, from the upper to the lower thoracic vertebra. Bilateral ribs are fused with each other and have an osseous or cartilaginous connection with the anterior part of the corresponding vertebra. This connection may impact normal spinal column growth, resulting in a local kyphosis. As well as BBIR, the radiological findings of these patients are diverse and include involvement of several spinal segments, especially in the thoracic region, which present as butterfly-like vertebrae, lamina anomaly, hemivertebrae or block vertebrae, and diverse alterations to rib morphology. These rib alterations include rib enlargement, fusion, bifurcation, or even agenesis, causing asymmetries with incorrect rib alignment and often with a reduction in the total number of ribs.
Patients with BBIR show a range of marked clinical features. An uneven back is usually observed from birth and can continue to deteriorate with age. As well as the appearance deformity caused by kyphoscoliosis, multisystem disorders including congenital heart disease, urological malformations, digestive malformations, and neurological abnormalities can manifest. Speculatively, these congenital multisystem malformations may be caused by a single syndrome that has not yet been recognized. Before surgery, neurological symptoms occurred in 80% of the present cases. These neurological symptoms were caused by cord compression due to severe kyphosis or cord distraction due to a tether or bony septum.
The aim of surgery in patients with congenital kyphoscoliosis is to achieve partial correction of the spinal deformity and prevent further progression of kyphoscoliosis.9,10 Because apical vertebra deformation is the main cause of kyphoscoliosis, it is impossible to sufficiently correct the curve without an apical osteotomy. In this study, except for patient 5 who did not receive an apical osteotomy because of paralysis, three patients received three-column osteotomy, and one patient who received growing rod treatment had a planned osteotomy at definitive fusion surgery. Note that resection of the middle part of the bifurcated rib is not necessary in all cases. When the BBIR is fused with the anterior part of the apical vertebra, resection of the middle part of the BBIR is recommended to achieve satisfactory kyphotic correction. However, if the BBIR is not located at the planned osteotomy level or not fused with the anterior part of the apical vertebra, kyphotic correction can be performed without BBIR treatment.
The risk of permanent neurological deficits following surgery is very high in BBIR patients. In this study, patient 5 suffered lower extremity paralysis after bony septum resection, which indicated that her spinal cord was compressed by the angular kyphosis and bony septum. Intraoperative traction may have also contributed to the residual spinal cord dysfunction and resulting neurological complications. Thus, although most patients with progressive neurological deficits will benefit from surgery, some will suffer permanent paralysis, and the risk should be recognized by both patients and surgeons.
The limited number of patients in this study and the numerous types of surgical interventions, including growing rod treatment and fusion with osteotomy, made it difficult to determine the optimal surgical option for BBIR. Another limitation of our study is that no genetic tests were performed to verify the genetic etiology.
Conclusion
In conclusion, BBIR is a very rare costal deformity found in congenital kyphoscoliosis patients, and it is commonly associated with multiple system malformations. Patients with this rare anomaly are likely to experience neurological deficits before or following surgery. Spinal surgeons should be aware of the high risk of permanent neurological complications related to surgery in these patients.
Supplemental Material
sj-pdf-1-cho-10.1177_18632521241232304 – Supplemental material for Surgical treatment for congenital vertebral anomalies with bilateral bifid intrathoracic rib in association: A series of five cases
Supplemental material, sj-pdf-1-cho-10.1177_18632521241232304 for Surgical treatment for congenital vertebral anomalies with bilateral bifid intrathoracic rib in association: A series of five cases by Hanwen Zhang, Lining Zhu, Jiahao Jiao, Dong Guo, Xuejun Zhang and Ziming Yao in Journal of Children's Orthopaedics
Footnotes
Author contributions
H.Z. and L.Z. contributed equally to this work. All authors contributed to the conception and design of the study. Material preparation data collection and analysis were performed by Z.Y., L.Z., H.Z. and D.G. The first draft of the manuscript was written by Z.Y., and all authors commented on subsequent versions of the manuscript. All authors read and approved the final manuscript.
Availability of data and material
The data used during this study are available from the corresponding author on reasonable request.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The partial financial support was received from the Beijing Natural Science Foundation (code: L222095) and the National High Level Hospital Clinical Research Funding (code: 2022-PUMCHD-004). The Partial financial support was received from the Beijing Hospitals Authority Youth Programme (code: QML20211204) and the BeiJing Talents Fund (code: 2018000021469G275).
Ethical approval
Ethical approval was waived by the local ethics committee of Beijing Children’s Hospital at Capital Medical University given the retrospective nature of the study and because all procedures were performed as part of routine care.
Consent to participate
Informed consent was obtained from the parents/guardians of all participants included in the study.
Consent to publish
The parents/guardians of participants consented to the submission of the original article to the journal.
Previous communication
The present case series was submitted to the Journal of Bone and Joint Surgery. Nevertheless, it was rejected due to the insufficient number of cases.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.