
Abstract
Purpose:
Hybrid techniques using thoracic sublaminar bands have proved their efficacy in adolescent idiopathic scoliosis posterior fusion, but clinical axial correction sometimes remained disappointing. One solution found was “the frame technique” and the second alternative was the replacement of the convex sublaminar bands by periapical uniplanar screws. The goal of this study was to compare clinical and radiological outcomes of both techniques in a consecutive cohort of adolescent idiopathic scoliosis patients.
Methods:
All patients undergoing primary posterior fusion for thoracic adolescent idiopathic scoliosis between January 2017 and March 2020 were included. Two groups were compared: Group 1 with thoracic sublaminar bands only and Group 2 with periapical uniplanar screws. All patients underwent standing stereoradiographs. The main frontal, sagittal, and axial (apical vertebra rotation) radiological parameters of interest were analyzed. Functional outcomes were assessed using the Scoliosis Research Society 30 score.
Results:
A total of 147 adolescents were included (Group 1, n = 73 and Group 2, n = 74 patients). In the frontal plane, a greater reduction index was observed in Group 2 (68% versus 62%, p < 0.001) as well as a better apical axial correction (67.8% versus 46.6%, p = 0.03). The number of thoracoplasty performed was reduced (6.7% versus 20.5%, p = 0.02) in Group 2, with a significant decrease in the rate of mechanical complication. No significant loss of correction was observed during follow-up in any of the group.
Conclusion:
The adjunction of convex uniplanar screws at the periapical levels improved the three-dimensional surgical correction of thoracic adolescent idiopathic scoliosis treated with hybrid constructs.
Level of evidence:
level III, retrospective comparative study
Keywords
Introduction
Adolescent idiopathic scoliosis (AIS) surgical correction techniques have changed considerably in the last three decades, with the development of stiffer reduction rods (CoCr+, 5.5 or 6 mm diameter), and a wider use of thoracic pedicle screws, often associated with efficient derotation instruments. All-pedicle screw constructs have become the gold standard for AIS posterior fusion, but hybrid techniques using thoracic sublaminar bands have also proved their efficacy for deformity correction, emphasizing the sagittal alignment restoration in hypokyphotic patients.1 –3 Our department has a long experience with the bands, used since 2005, and the constructs have progressively evolved over time. 4 Sublaminar bands are no longer recommended at lumbar levels, except in the very dystrophic pedicles that can be found in some syndromic patients, and they are mainly used now from T5 to T10 in AIS, mostly on the concave side. While frontal correction rates have been for long very satisfactory, ranging from 50% to 70% in the recent literature, the clinical axial correction, observed both intraoperatively and postoperatively with the residual rib hump, sometimes remained disappointing.1 –3,5 –7 One of the solutions found was “the double rod frame technique,” described in 2019, in which the contact of the right rod on the apical convex lamina during the concave translation helped emphasize the axial correction, which reached 42%. 5 The second alternative that gained popularity among some surgeons was the replacement of the convex sublaminar bands by periapical uniplanar screws, to increase the implant density and allow a more direct vertebral derotation from the convex side, after having performed the posteromedial translation on the concave rod. The goal of this study was therefore to compare clinical and radiological outcomes of both techniques in a consecutive cohort of AIS patients.
Materials and methods
Study population
Following institutional review board (IRB) approval (CEER N°2022-621ter), all consecutive AIS patients undergoing primary posterior fusion for thoracic AIS (Lenke 1 to 4) between January 2017 and March 2020 were included. A minimum 2-year follow-up was required. Data were prospectively included but retrospectively analyzed. Patients were evaluated preoperatively, in the early postoperative period (within 4 months), and at latest follow-up.
Surgical procedures
All patients underwent posterior fusion under neuromonitoring using hybrid constructs (5.5 mm CoCr+ diameter rods), combining bilateral pedicle screws (Solera; Medtronic, Minneapolis, USA) below the inflection point (from T11 to L4), concave sublaminar bands (above the inflection point, from T5 to T11) (Jazz; Implanet, Bordeaux, France), and proximal angled supralaminar hooks on the upper instrumented vertebra (UIV), as previously reported. 5 No selective thoracic fusion (no LIV at T12 or above) was performed, and no patient underwent prior anterior release before correction.
Patients from Group 1 (bands group) were instrumented with sublaminar bands on the thoracic convex side and reduced following the “frame” technique principles, while periapical uniplanar screws (4–6) were preferred on the thoracic convex side in Group 2 (uniplanar group) (Figure 1). Patients from Group 1 were operated between January 2017 and December 2018, while patients from Group 2 were operated between January 2019 and December 2020. In the latter, the thoracic curve reduction started first on a single concave rod using sublaminar bands and then additional direct vertebral derotation and in situ frontal correction were added via the convex screws.
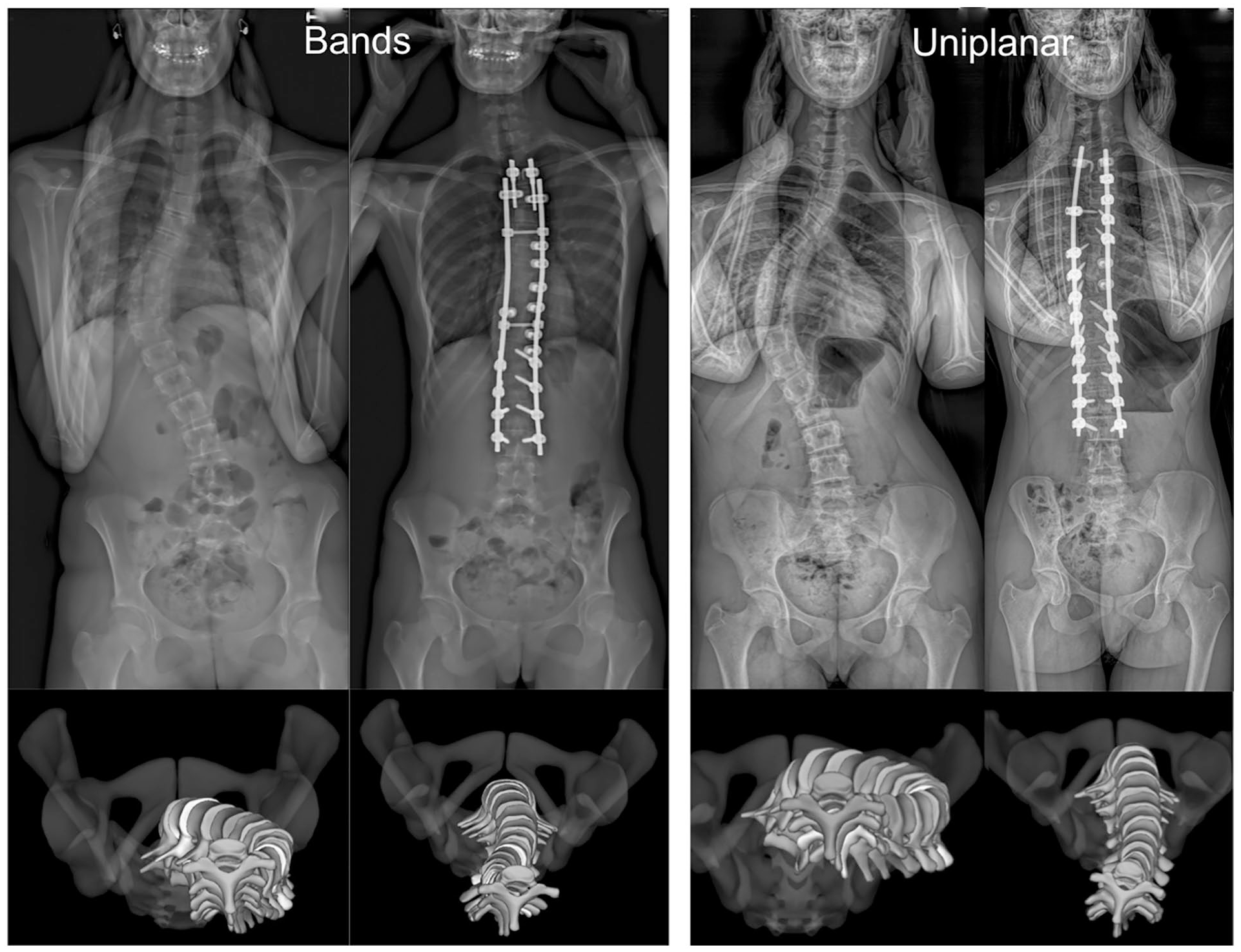
Frontal and 3D apical preoperative and postoperative views of both types of constructs.
Facetectomies were performed at every level, and 3–4 periapical posterior column osteotomies (PCOs) were systematically added in both groups. No additional 3-column osteotomy was used. After decortication, a combination of local autograft (from spinous processes) and allograft (50 cc) was used in all cases, and two subfascial 8 mm drains (opened 6 h after closure) were placed for 48 h. According to the patient’s request, the need for a thoracoplasty was mainly decided preoperatively. It was usually explained that a 30%–50% residual rib hump would exist after posterior fusion, and if the patient expressed high cosmetic concern, and accepted the idea of wearing a full-time brace for 3 months postoperatively, it was decided with the family. However, if the surgeon observed a significant rib hump reduction after the deformity correction, the thoracoplasty (even if requested) was not performed.
The “patient blood management” strategy was standardized during the entire study period. Preoperatively, iron and vitamin B9 implementation were started 6 weeks prior to surgery. Erythropoietin injections (600 UI/kg/week, maximum four injections) were performed on a weekly basis, until the hemoglobin rate reached 15 g/dL. Tranexamic acid was used intraoperatively, with a loading dose of 10 mg/kg, followed by a continuous infusion (5 mg/kg/h) until the end of the procedure. Cell saver was installed in all cases and blood was reinfused if the quantity was above 3 mL/kg. Postoperative multimodal analgesia included morphine (patient-controlled analgesia, PCA), paracetamol, non-steroidal anti-inflammatory drugs (NSAIDs), gabapentin, and nefopam. All patients benefited from enhanced recovery after surgery (ERAS) protocols, as previously described.8,9 Surgical data and perioperative blood loss were reported, and all intraoperative events and/or complications requiring revision were analyzed. 10
Radiological measurements and functional outcomes
All patients underwent standing low-dose stereoradiographs (EOS Edge, EOS imaging, Paris, France) preoperatively, at 4-month postoperative and at latest follow-up. Independent three-dimensional (3D) reconstructions were performed (EOS 3D service, Montreal, Canada), and the main frontal, sagittal, and axial (apical vertebra rotation, AVR) radiological parameters of interest were analyzed. 11 The AVR limit values proposed by Upasani et al. 12 were used to define the grades of axial rotation (i.e. 0° to 8° for Grade 0, 9° to 12° for Grade 1, and >12° for Grade 2).
The Cincinnati reduction index was also used. The index formula is preoperative flexibility index/postoperative correction index. The preoperative flexibility index (%) is defined by preoperative [(main curve Cobb angle while standing − main curve Cobb angle while bending)/main curve Cobb angle on standing] × 100. The correction index (%) is defined by [(preoperative main curve Cobb angle while standing − postoperative main curve Cobb angle while standing)/preoperative main curve Cobb angle while standing] × 100.
Functional outcomes were assessed at follow-up using the Scoliosis Research Society 30 (SRS 30) score.
Statistical analysis
Statistical analyses were performed using XLSTAT 2022.4 (Addinsoft, Paris, France). A Shapiro–Wilk test was performed to assess data distribution. Continuous numeric data was expressed as mean ± standard deviation (SD) using absolute values. Group comparisons were performed with a two-tailed Student t-test for the data with normal distribution, a two-sample Wilcoxon test for the non-parametric data, and a two-tailed Fisher’s exact test for nominal variables. A p < 0.05 was considered significant.
Results
Patients’ demographics and radiological parameters
A total of 147 adolescents were included, 74 patients in the uniplanar group and 73 in the bands group. Patients in Group 2 (uniplanar) were significantly older (1.5 years on average). Curves distribution (Lenke type) and the proportion of Lenke (-) sagittal modifier (i.e. T4T12 < 10°) were similar between groups. A significant difference was found for the length of follow-up (27 months versus 31 months, p < 0.001), explained by the fact that the use of uniplanar screws was a more recent technique (Table 1). Preoperative radiological measurements are summarized in Table 2. Curves were comparable preoperatively, but patients in the bands group were significantly more coronally imbalanced (3 mm on average, p = 0.04). No difference was found between groups regarding operative time and blood loss.
Patient demographics and surgical data.
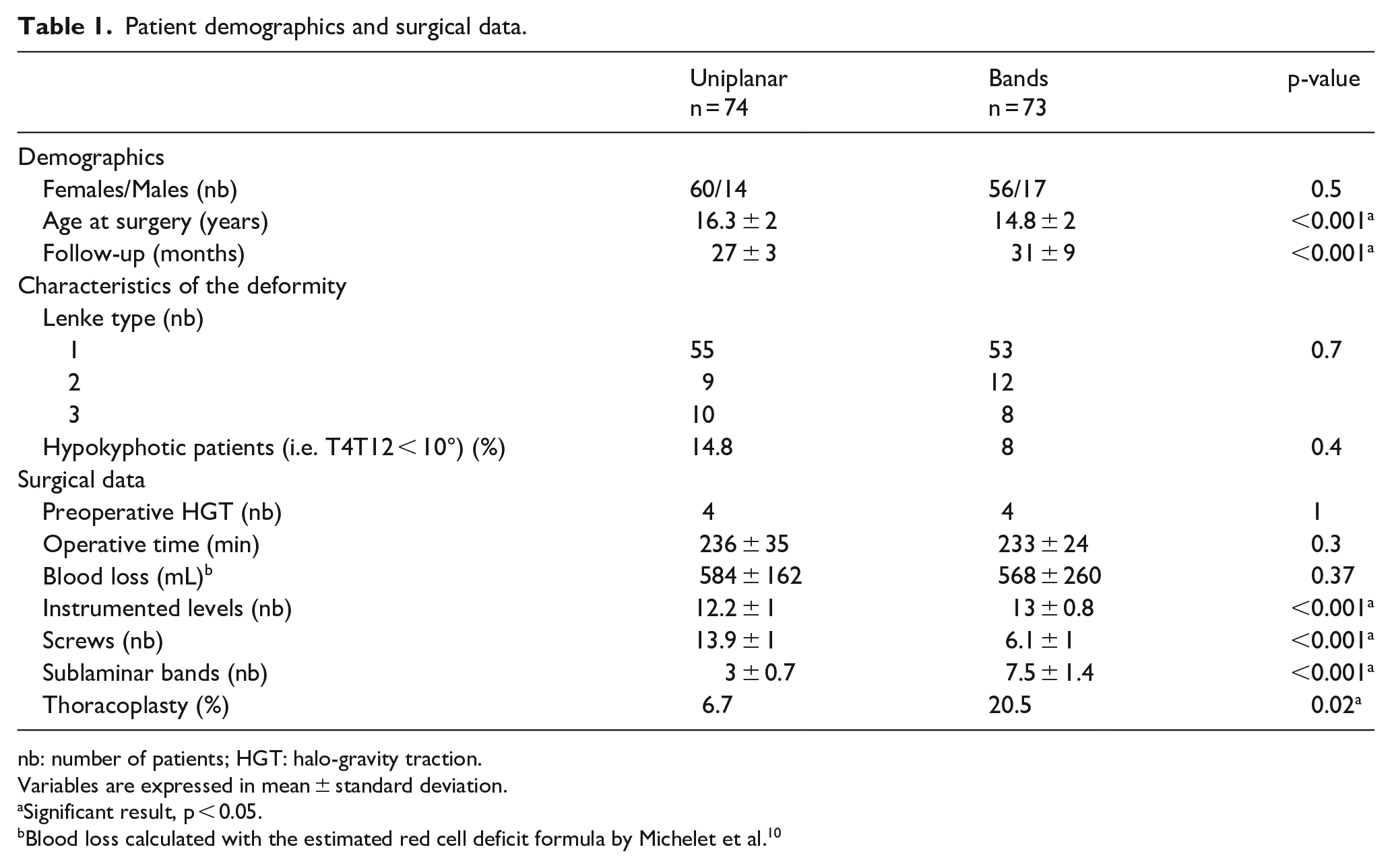
nb: number of patients; HGT: halo-gravity traction.
Variables are expressed in mean ± standard deviation.
Significant result, p < 0.05.
Blood loss calculated with the estimated red cell deficit formula by Michelet et al. 10
Preoperative radiological measurements.
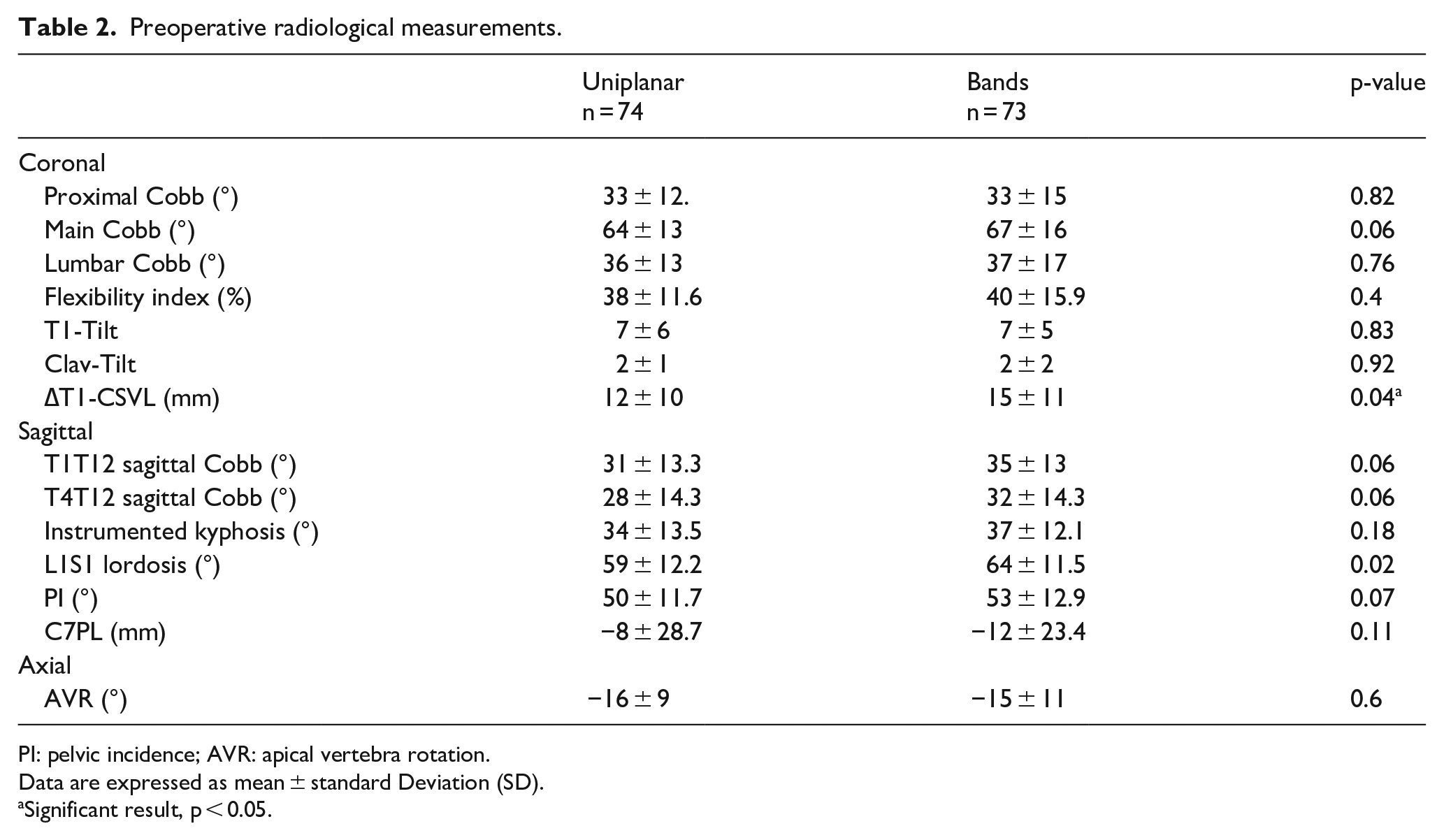
PI: pelvic incidence; AVR: apical vertebra rotation.
Data are expressed as mean ± standard Deviation (SD).
Significant result, p < 0.05.
3D radiological outcomes
Postoperative radiological measurements are reported in Table 3. In the frontal plane, a significantly greater correction index was observed in the uniplanar group (68% versus 62%, p < 0.001), but no difference was found regarding Cincinnati reduction indices (2 versus 1.8, p = 0.15). Both types of constructs maintained or restored efficiently the thoracic sagittal alignment, with a significant increase in the instrumented thoracic kyphosis in both groups (7° on average with bands versus 5° with uniplanar screws) (Figures 2 and 3). No patient remained hypokyphotic at latest follow-up according to Lenke sagittal modifier classification (i.e. T4T12 < 10°), and the mean gain in the instrumented zone of that subgroup even reached 11° in the uniplanar group and 12° in the bands group (p = 0.6). A significantly better apical axial correction (AVR mean gain 10.5 ± 7° versus 7 ± 6°, p = 0.03) was observed in the uniplanar group (67.8% versus 46.6%, p = 0.03). Number of thoracoplasty performed was also significantly reduced (6.7% versus 20.5%, p = 0.02) (Figure 4). Using the AVR grades proposed by Upasani et al., 54% of the uniplanar group were Grade 0 postoperatively, while 32.5% were Grade 1 and 13.5% remained Grade 2.
Postoperative radiological outcomes.
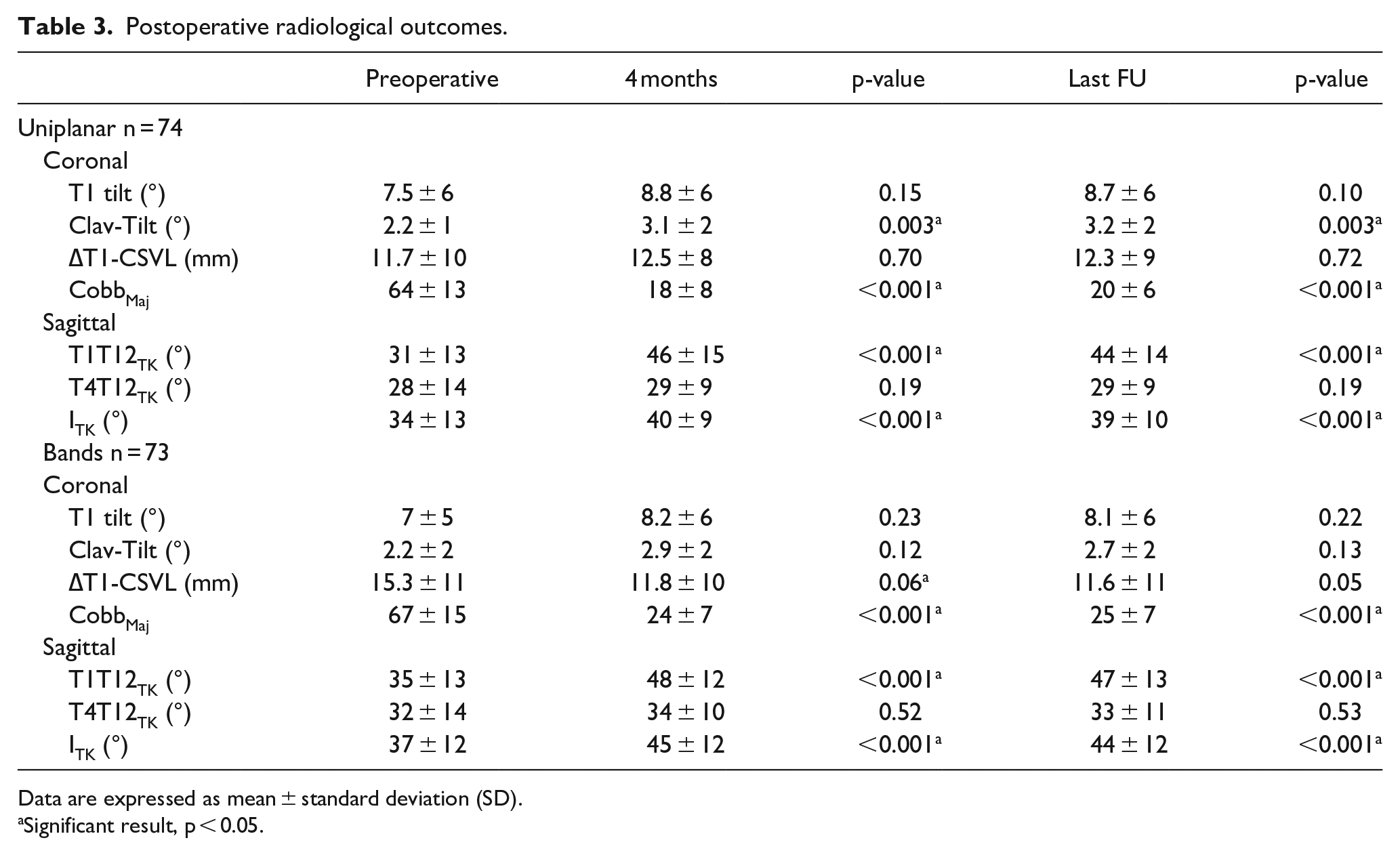
Data are expressed as mean ± standard deviation (SD).
Significant result, p < 0.05.
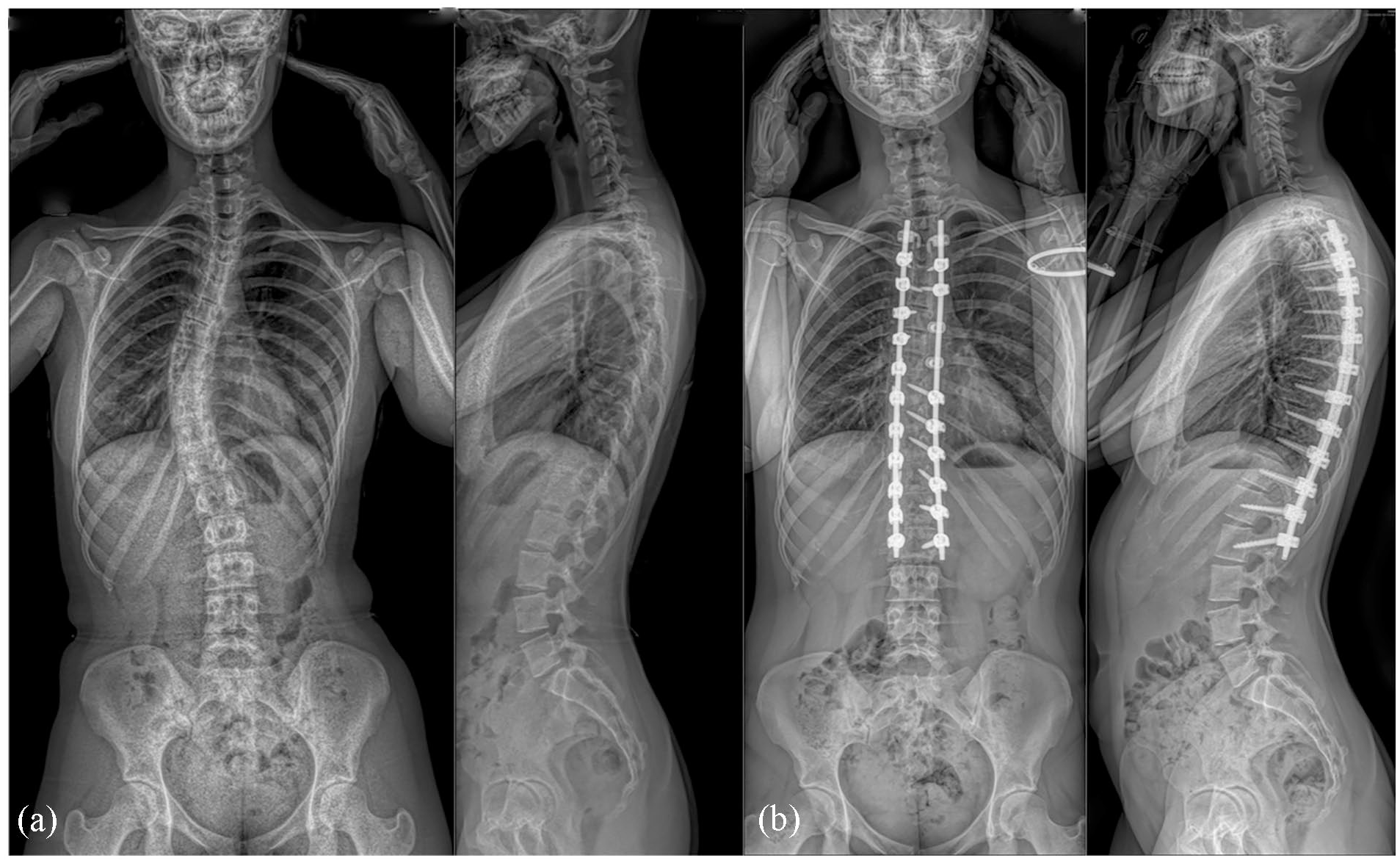
A 16-year-old patient with a Lenke 1 AN deformity operated with the most recent uniplanar/bands hybrid technique (a). Two years postoperatively, thoracic kyphosis was maintained with a well-balanced global sagittal and coronal alignment (b).

A 14-year-old patient with a severe Lenke 1 AN deformity and proeminent rib hump operated with the uniplanar screws techniques (a). Results at the last follow-up (b) showed a well-balanced global sagittal and coronal alignment and a significant reduction of the rib hump without thoracoplasty. Axial apical correction was improved by 65%.
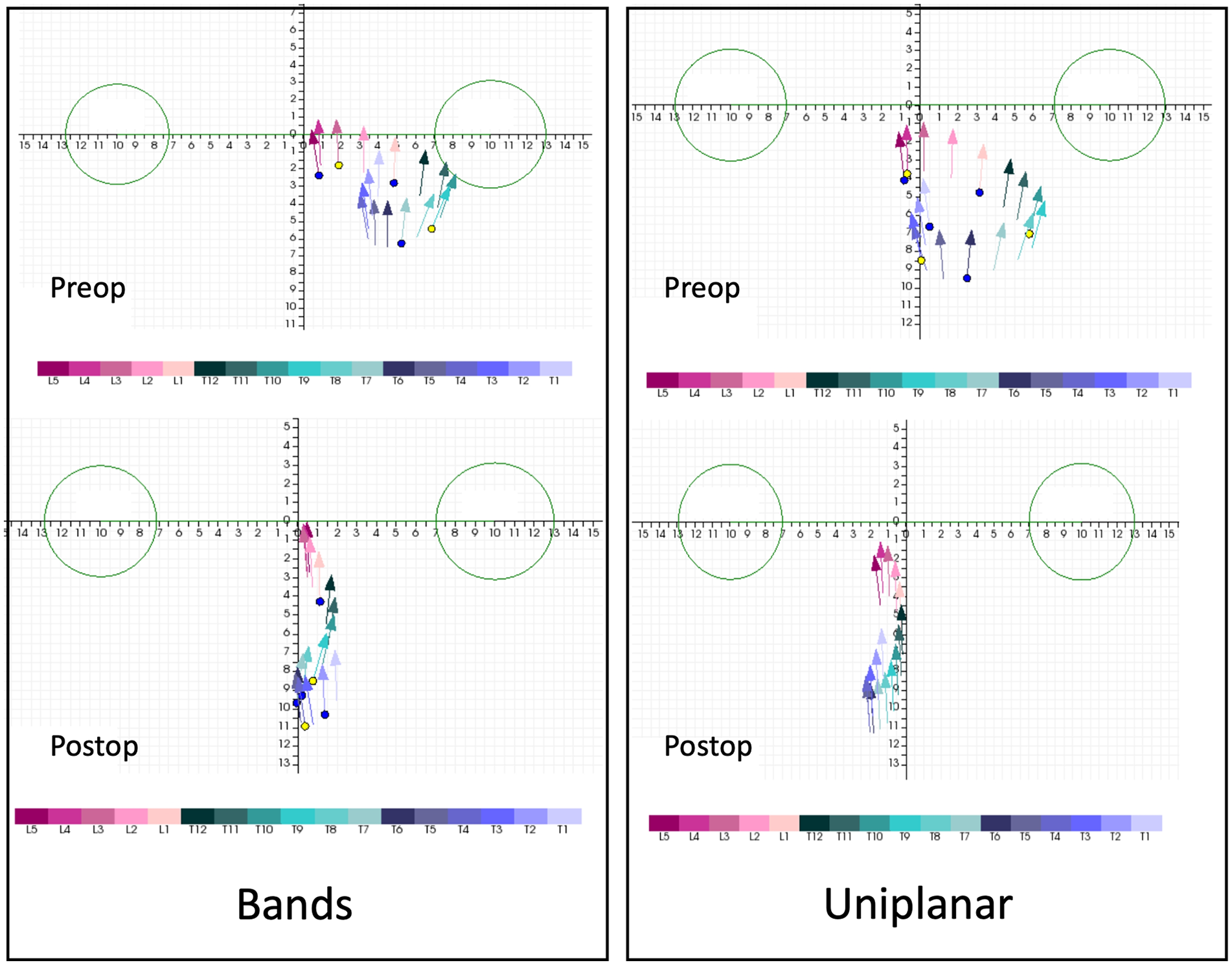
Comparison of axial correction illustrated by vertebral vectors in both groups showing a significant correction in the axial plane with both techniques. The figure corresponds to a top view vector representation of the deformity, in which each vector represents the location and the rotation of a single vertebra. The two circles correspond to the femoral heads. On postoperative representations, the reader can appreciate the posteromedial translation obtained at the apex, with all vectors more centered between the femoral heads, and the direction of the vectors became more anteroposterior, corresponding to less residual axial rotation.
Complications and functional outcomes
A significant decrease in the rate of mechanical complication (proximal junctional failure and pseudarthrosis) was observed in Group 2 (Table 4), and the use of additional uniplanar screws did not lead to an increase in surgical site infections (SSIs). All those complications required revision. No significant loss of correction was observed during follow-up in any of the group.
Complications reported during follow-up requiring revision and latest functional outcomes.
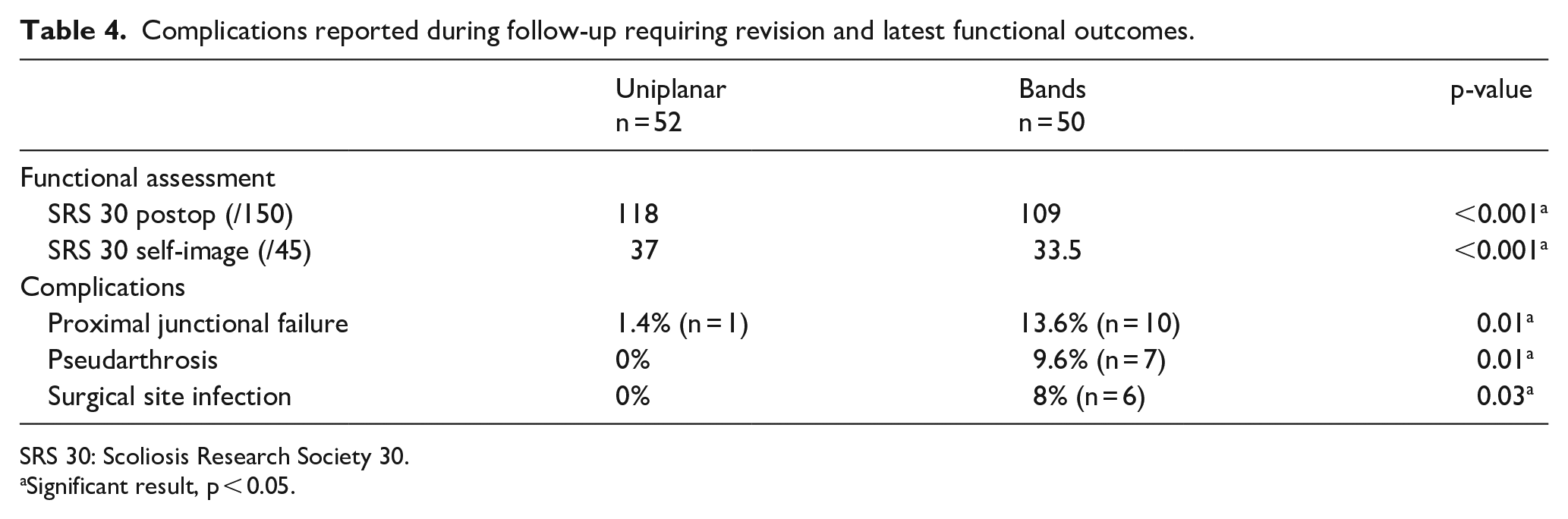
SRS 30: Scoliosis Research Society 30.
Significant result, p < 0.05.
Functional outcomes were assessed in 103 patients (70% responders, same rate in each group). The scores reported at latest follow-up were significantly better in the uniplanar group regarding the mental health and the self-image items (Table 4).
Discussion
This is the first study to report axial analysis of convex thoracic uniplanar screws based on stereoradiographic 3D reconstructions in AIS surgery. The addition of apical convex uniplanar screw improved axial correction and the sublaminar bands used on the other side enhanced thoracic sagittal alignment without increasing the perioperative morbidity.
Uniplanar screws in AIS
Despite a growing popularity in spinal deformity surgery in the last decade, few studies have reported the radiological and/or clinical outcomes of AIS patients treated with uniplanar screws. These screws are particularly interesting at thoracic levels, in order to provide the reduction potential of a monoaxial screw in the coronal plane, while avoiding the sagittal deleterious flattening effect frequently reported in all-screw constructs.13,14 As a matter of fact, the 20°–25° modularity available in the sagittal plane helps respect and maintain the rod sagittal contour, while in situ frontal maneuvers or derotation remain possible. The main expected advantage of these screws is therefore the apical axial correction, which can be assessed clinically by the residual rib hump, or radiologically by the rib height difference or the validated grading system (0–2) developed by Upasani et al. 12 Another option is postoperative CT, but this examination is performed in supine position and is associated with high and unnecessary radiation exposure.
In 2011, Dalal et al. 15 first showed radiologically that uniplanar screws (used in all-screw constructs) were superior to polyaxial ones for axial apical correction of thoracic curves, due to an increased rotational leverage during intraoperative bilateral direct vertebral derotation maneuvers. The same team later reported that a high degree of coronal correction could be achieved in association with vertebral derotation, without sacrificing sagittal alignment, if uniplanar screws were used with high-strength rods, aggressively bent (overcorrection) in the sagittal plane. 16 This finding was later confirmed by Badve et al., 17 who observed a greater long-lasting correction of the sagittal thoracic alignment with uniplanar screws compared to fixed ones. Hu et al. 18 also confirmed the superiority of uniplanar screws in Lenke 5C curves, which should definitely be considered now in AIS correction.
Axial correction in AIS hybrid constructs
Hybrid constructs with thoracic sublaminar bands have also been adopted in the last 15 years by many surgeons who wanted to avoid the risks of periapical concave thoracic pedicle screw placement, while emphasizing sagittal alignment restoration.6,19 –21 The efficiency and safety of the technique has been demonstrated. The use of sublaminar bands is indeed much safer than periapical pedicle screws in the concave side, especially in thin pedicles. The only drawback is the necessity to resect the ligamentum flavum at periapical levels for bands insertion. However, the intervertebral canalar approach can also be facilitated by wide PCOs, especially in hypokyphotic patients with overlapping laminae that are also helpful to optimize deformity correction.
While frontal and sagittal correction rates have always been satisfying, several technical modifications have been proposed to enhance the apical axial correction, which sometimes remained disappointing intraoperatively. Zaher et al. 22 proposed to place the polyester bands under the transverse processes to increase the rotational leverage on the concave rod, while the “frame technique” relied on a double rod simultaneous correction. 5 In 2018, La Maida et al. 23 described the apical vertebral derotation and translation (AVDT) technique, combining concave sublaminar bands and convex monoaxial pedicle screws in low-density constructs, and found better sagittal thoracic and cervical alignments compared to all-screw constructs, with reduced operative time and blood loss. The current series therefore followed the same philosophy for reduction while using exclusively uniplanar screws in higher density constructs.
3D postoperative analysis of hybrid constructs
To date, only two studies have investigated the 3D postoperative axial correction provided by sublaminar bands in thoracic curves.5,6 Both were based on standing EOS 3D reconstructions, which have proved their accuracy and reliability, and found comparable apical axial correction (42.2% and 47.7%, respectively). 24 The current series is the first to compare the 3D postoperative radiological outcomes between classical bands hybrid constructs (with bands on both sides of the curves) and a newer generation uniplanar-bands hybrid construct (Figure 1). The 3D AVR decreased by 46.6% postoperatively in the bands only group, which is in accordance with previous literature, but the adjunction of convex uniplanar screws significantly improved axial correction (67.8%, p = 0.03), without sacrificing the sagittal alignment. Interestingly, the postoperative distribution of the uniplanar group based on Upasani’s grade was very similar to the one described in the original study with all-uniplanar screw constructs, showing that convex uniplanar pedicle screws might be sufficient to obtain the expected derotation effect, while the concave bands (or the reduction concave screws) are more useful for the posteromedial translation of the spine. 12
Both operative time and blood loss were not significantly affected by the change of the surgical technique, despite a higher implant density, but the rate of complication during follow-up was significantly reduced, probably due to a greater initial stability. Indications of thoracoplasty were dramatically reduced (20.5%–6.7%), and patients reported a significantly higher self-image score (37 versus 33.5, p < 0.001).
Limitations
This study presents several limitations. First, it was not randomized, and the surgical technique was only based on the surgeon’s preference and technical improvements of the hybrid construct over the years. Second, the influence of implant density on postoperative correction was not investigated here, as more implants (but different) were used in the uniplanar group. The latter might also be an explanation for the differences in complication rates (mechanical failure). Nonetheless, the decrease in SSIs was rather attributable in a change of perioperative protocols and not due to the surgical technique. 25 In addition, the accuracy of postoperative EOS reconstructions can be questioned, as implants may hide some key anatomical landmarks, but the method has been previously validated. 24 The inter-observer (and intra) reproducibility was also not assessed, but all 3D measurements were made by independent senior observers from EOS 3D services. Finally, 30% of the functional scores were not available at follow-up, which remained relatively short. The differences between groups regarding the different SRS domains still need to be further studied in bigger cohorts.
In conclusion, results of the current series confirmed that the adjunction of convex uniplanar screws at the periapical levels improved the 3D surgical correction of thoracic AIS treated with hybrid constructs, without any increase in perioperative morbidity.
Supplemental Material
sj-pdf-1-cho-10.1177_18632521231220388 – Supplemental material for Does the addition of convex uniplanar screws in hybrid constructs improve 3D surgical correction in thoracic adolescent idiopathic scoliosis posterior fusion?
Supplemental material, sj-pdf-1-cho-10.1177_18632521231220388 for Does the addition of convex uniplanar screws in hybrid constructs improve 3D surgical correction in thoracic adolescent idiopathic scoliosis posterior fusion? by Laurie Simon, Mikael Finoco, Florence Julien-Marsollier, Adèle Happiette, Anne-Laure Simon and Brice Ilharreborde in Journal of Children’s Orthopaedics
Footnotes
Author contributions
Conception and design: Brice Ilharreborde.
Administrative support: Anne-Laure Simon.
Provision of study material and patients: Brice Ilharreborde, Adèle Happiette, Florence Julien-Marsollier.
Collection and assembly of data: Laurie Simon, Mikael Finoco.
Data analysis and interpretation: Laurie Simon, Mikael Finoco, Anne-Laure Simon.
Manuscript writing: All authors.
Final approval of manuscript: All authors.
Declaration of conflicting interests
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: All authors except Brice Ilharreborde declared. . . Brice Ilharreborde report to be consultant for Zimmer Biomet, Medtronic and Implanet.
Ethical statement
The study was conducted in accordance with the Declaration of Helsinki and was approved by the Ethics Committee of Robert Debré (Comité d’évaluation de l’éthique des projets de recherche de Robert Debré, CEER-RD) (no 2022-621ter) on 18 July 2023 with an exemption from informed consent. No specific consent is needed for statistical analyses of aggregated deidentified data. For this study, the raw data were first extracted from HIS, and patients’ identities, including names, screening IDs, patient IDs, and mobile phone numbers, were de-identified.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Availability of data and materials
The datasets generated during and/or analyzed during the current study are available from the corresponding author on reasonable request.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.