
Abstract
Background:
The COVID-19 pandemic has affected healthcare worldwide since December 2019. We aimed to identify the effect of the COVID-19 pandemic on outpatient clinic and surgical volumes and peri-operative complications for pediatric spinal deformities patients.
Methods:
In this multi-center retrospective study, outpatient visits (in-person and virtual care) and pediatric spine surgeries volumes in four high-volume pediatric spine centers were compared between March and December 2019 and the same period in 2020. Peri-operative complications were collected and compared in the same periods. Descriptive statistics were calculated, and comparative analyses were performed.
Results:
During the 2020 study period, the outpatient visit (in-person and virtual care) volume decreased during local lockdown periods by 71% for new patients (p < 0.001) and 53% for returning patients (p = 0.03). Overall, for 2020, there was a 20% reduction in new patients (p = 0.001) and 21% decrease in returning patients (p < 0.001). During the pandemic, there was also 20% less overall surgical volume of adolescent idiopathic scoliosis (AIS) patients undergoing primary posterior spinal fusion, with a 70% reduction during lockdown times (p < 0.001). Complication rate and profile were similar between periods.
Conclusion:
There was a significant decrease in outpatient pediatric spine outpatient visits, particularly new patients, which may increase the proportion of pediatric patients with spinal deformities that present late, meeting surgical indication. This, in combination with the reduction in surgical volume of AIS over the first year of the pandemic, could result in an extended waitlist for surgeries during years to come. Complication rate was similar for both periods, suggesting it is safe to continue elective pediatric spine surgery even in a time of a pandemic.
Level of evidence:
level IV.
Introduction
In December 2019, a novel coronavirus disease 2019 (COVID-19) caused by severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), emerged from Wuhan, China. Declared a pandemic by the World Health Organization on March 2020, as of May 2022, there were over 500 million reported cases and over 6 million mortalities. 1
Children account for about 19% of patients diagnosed with COVID-19, usually experience milder disease, and have a better prognosis than adults. However, a proportion of children require hospitalization and a small number needs ventilatory support for respiratory failure. There are well-described clusters of patients who require critical care support due to pediatric inflammatory multi-system syndrome temporally associated with SARS-CoV-2 (PIMS-TS).2,3 –7
COVID-19 has impacted many aspects of healthcare worldwide, in the field of pediatric orthopedics, it has created challenges regarding patients’ safety and the balance between their safety, the staff’s safety, and a timely surgical treatment of orthopedic conditions. Several studies regarding orthopedic pediatric care during the pandemic demonstrated decreased volume of elective surgery and clinic visits.8 –12 These studies focus on short timeframes and mainly compare the lockdown period in 2020 to the corresponding period in 2019. In addition, mortality or morbidity of spine deformity pediatric patients during the COVID-19 pandemic was not adequately studied. Finally, the published literature captured local practices leaving some concern about the generalizability of their conclusions.
We aimed to identify the global effect of the COVID-19 pandemic on surgical and outpatient volumes in four medical centers across different countries. Furthermore, we sought to describe possible impact on surgical complications for pediatric patients with spinal deformity during the pandemic.
Materials and methods
This is a retrospective multi-centric chart review study. The study was approved by the institutional review board and ethics committees of each center (REB #1000076612, EKNZ #2021-02042, IRB #2021-0124, Helsinki #0130-21), with informed consent waivered due to the retrospective observational design of the study. Four high-volume pediatric spine centers, from different countries, participated.
At all four centers, the first national lockdown and suspension of elective surgery were at approximately the same time—mid-March 2020. Due to this, the timeframe of the study was chosen as March to December 2019 and the same period in 2020.
We recorded the number of outpatient visits (new and returning patients, in-person and virtual care) at the pediatric spine clinic between the dates 1 March 2019 and 31 December 2020. Patients above 21 years of age were excluded.
From the pediatric spinal deformity surgical database of each center (representing the practice of nine pediatric spine surgeons), we collected patient demographic data, including—diagnosis, surgical volume, technique, and complications. We included patients younger than 21 years of age that underwent primary spinal surgery. Exclusion criteria consisted of age above 21 years and other procedures performed in the operating room (namely, Risser casts, halo gravity traction application, and revision surgeries). The data included were anonymized, with the centers designated henceforth in a randomly selected alphabetical order (A–D).
Statistical analysis was blinded to the origin of the data and was performed using SPSS 22.0 software (IBM Corp., Armonk, NY, USA). Negative binominal and linear equations using GEE models were applied. All statistical tests were two-sided, and p < 0.05 was considered statistically significant.
Results
The first COVID-positive case was diagnosed between January and February 2020 in all four countries. Timing of the first quarantine was similar, mid-March 2020, with cessation of elective surgeries also implemented at that time. Only one center (B) had complete cessation of pediatric spinal deformity surgeries for a 1-month period (April 2020). There were different policies regarding return to previous surgical volume—center C resumed near normal operations in May 2020, centers A and B in June 2020, and center D had a more regulated return, beginning also in June 2020, but not achieving the pre-COVID surgical volume even by the end of 2020. Regarding outpatient clinics, during mandatory state-imposed quarantines, the outpatient clinics were closed in all four centers. In between lockdown periods, centers A and C returned to routine outpatient clinic operation, whereas centers B and D limited substantially the number of patients arriving at the clinic, at the initial phase of the pandemic, with a gradual increase in volume over the year. All centers implemented COVID-19 precautions that included mandatory mask wearing, eyewear protection, hand hygiene, and mandatory pre-operative COVID-19 tests for patients.
Outpatient volume
When comparing 2019 (pre-COVID) and 2020 (during COVID), there was a 14% reduction in the number of patients visiting the four outpatient clinics. This includes both in-person and telehealth visits. Between March 2019 and December 2020, 15,979 patients visited the four clinics, of these, 54% (8608 patients) were examined between March and December 2019, and 46% (7371 patients) in the corresponding months in 2020. Two centers (B, D) experienced a substantial reduction (−22%, −22.5%, respectively), while two centers (A, C) maintained roughly the same volume as pre-COVID (−5%, +7%, respectively) (see Figure 1).
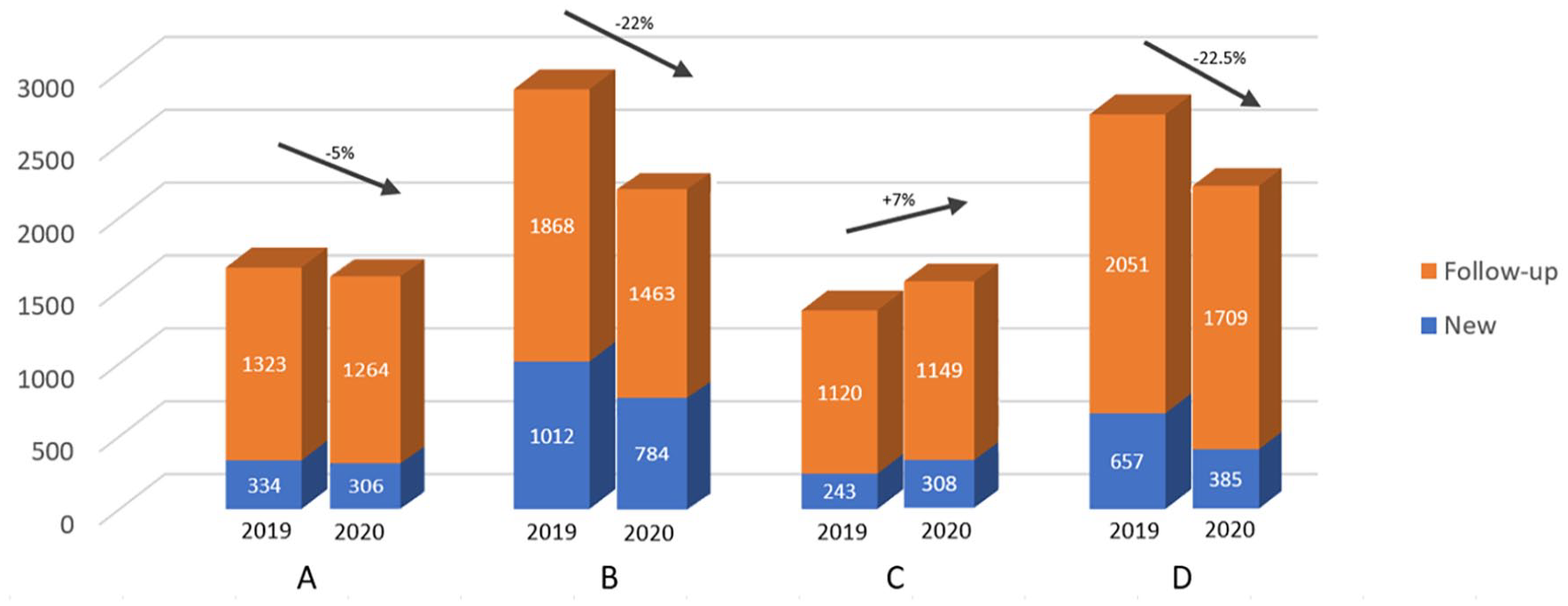
Outpatient clinic volume—2019 versus 2020—by center.
Including both in-person and telehealth visits, there were a 20% reduction in new patients (p = 0.001) and 21% in returning patients (p < 0.001) in 2020. When comparing periods with and without quarantine in 2020, there were a 71% reduction in new patients and 53% in returning patients (p < 0.001 and p = 0.03, respectively).
Telehealth visits were not utilized in any substantial way pre-COVID by the four centers. During 2020, only two centers (B and D) used telehealth significantly (595 patients: 92% returning and 8% new) (see Figure 2). Even with the substantial increase in telehealth services in these two centers, the significant decline in patients (new and returning) during 2020, and specifically during quarantine periods, was maintained.
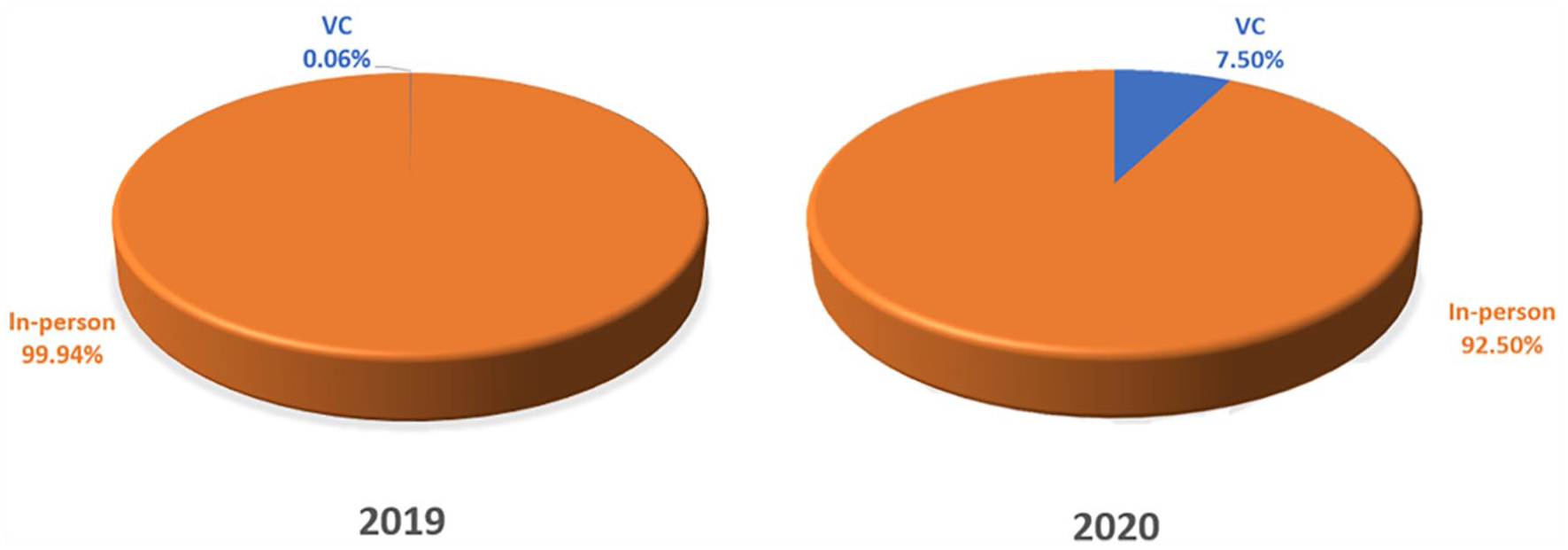
In-person versus virtual care volume—2019 versus 2020.
Surgical volume
Comparing total surgical volume between 2019 and 2020 demonstrated an increase in volume by 6%–12% in three centers (A–C) and a 36% reduction in one center (D). In the subgroup of adolescent idiopathic scoliosis (AIS) patients undergoing primary posterior spinal fusion, there was a 20% volume reduction in all four centers (p = 0.001), with a 70% reduction during periods of full quarantine (p < 0.001) (see Figure 3).
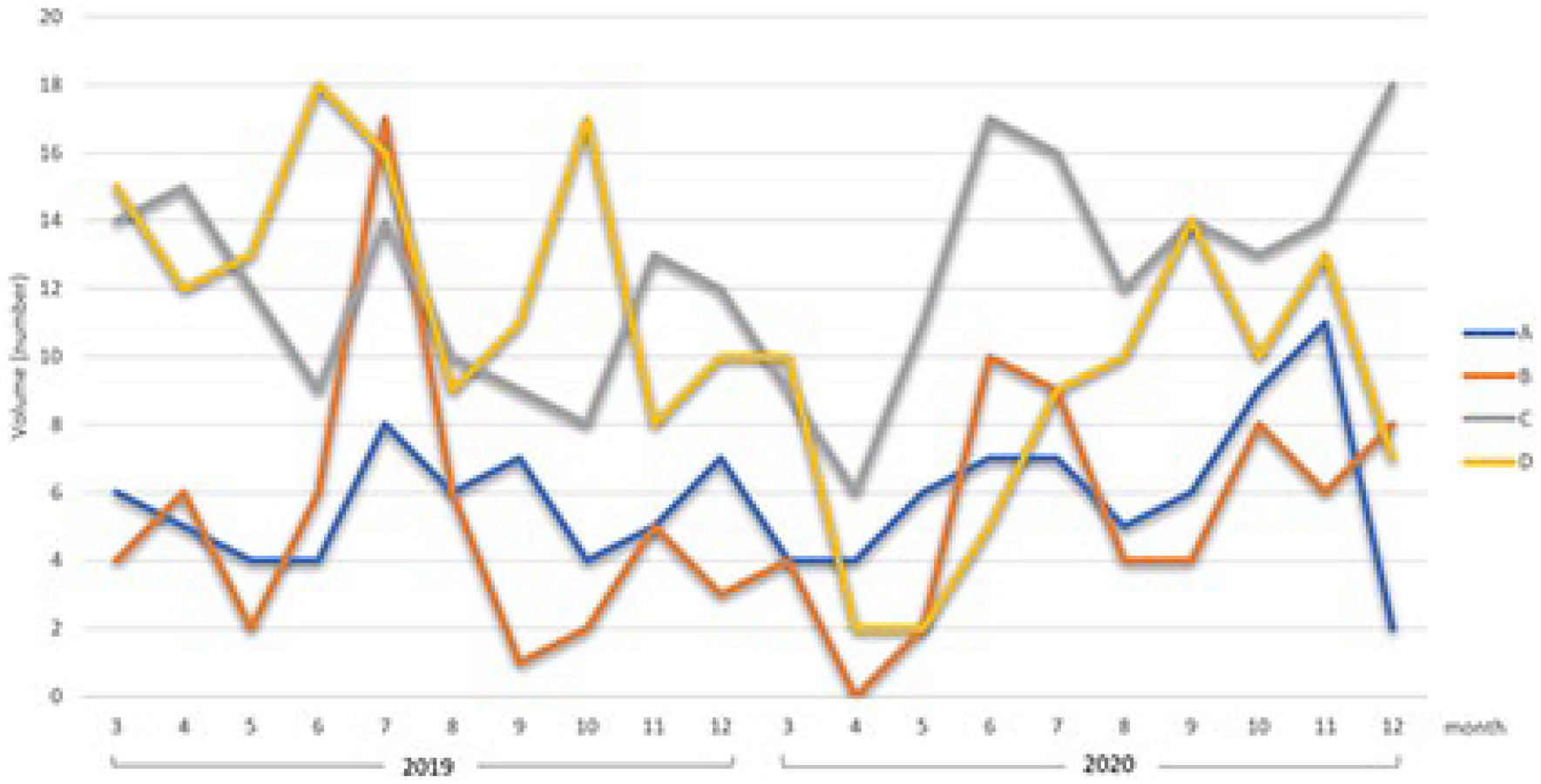
Surgical volume 2019 versus 2020—by center.
Complications
All four centers required patients to have a pre-operative COVID test prior to admission. Of the 328 pediatric patients who underwent spinal surgery during 2020, all were COVID-negative prior to surgery. A post-operative test was not mandatory, and only performed if COVID-19 infection was suspected. Only 29 patients (9%) underwent COVID-19 test post-operatively—all were negative. There was no meaningful difference in the complication profile between the years 2019 and 2020. In 2019, there were 11 cases of deep wound infections, with 5 cases in 2020. There were three pulmonary complications in 2019 (atelectasis, viral upper respiratory tract infection, and pulmonary embolism) and six in 2020 (atelectasis, pneumothorax, and four cases of COVID-negative pneumonia). There were no mortalities in either year. Of note, using existing precautions, none of the attending surgeons in the four centers tested positive for COVID-19 during the study period (see Table 1).
Complications by center—2019 versus 2020.
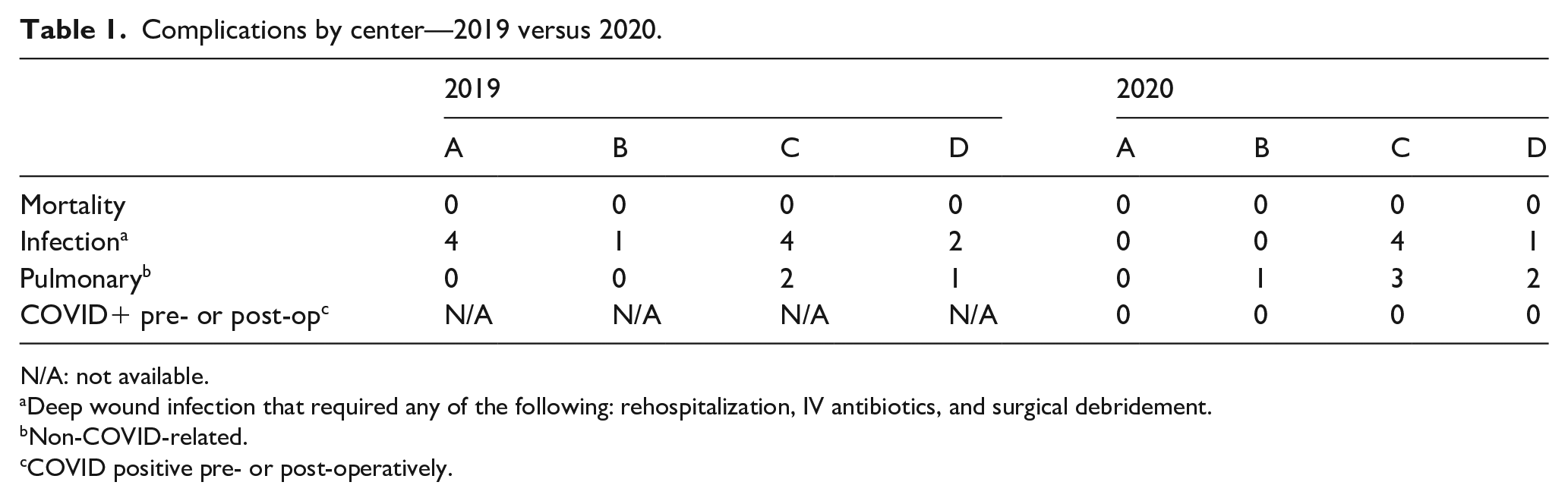
N/A: not available.
Deep wound infection that required any of the following: rehospitalization, IV antibiotics, and surgical debridement.
Non-COVID-related.
COVID positive pre- or post-operatively.
Discussion
The COVID-19 pandemic has been affecting healthcare worldwide since December 2019. In the initial phase, aside from the challenging number of patients infected with a new and unknown virus, the medical field was also adapting to new circumstances—quarantines, travel limitations, periodic suspension of elective procedures, and different, rapidly changing, precaution measurements. Adding to this was a well-documented shift in the public’s health-seeking behavior, as less people sought medical care for non-related COVID-19 health concerns.3,13
An inverse relationship between pediatric neurosurgical operative volumes and the incidence of COVID-19 in the United States has been documented. 9 Specific to the orthopedic pediatric population, studies have demonstrated a significant decrease in emergency department presentations (30%–70%), hospital admissions (5%–45%), and outpatient clinic volumes (20%–80%) early in pandemic.8,11,12 With fewer people accessing primary care, fewer specialty-care referrals were made. A 76% reduction in referral rates of pediatric idiopathic scoliosis to a high-volume spine center indicates that, in that region at least, the majority of new scoliosis patients went undiagnosed early in the pandemic. 10
We examined the impact of COVID-19 on four pediatric spine centers. Focusing on clinic volume and surgical volume and complications of pediatric spinal deformity patients, we compared a 10-month period (March to December) encompassing the first year of COVID-19 (2020) with the same months a year prior to the COVID-19 outbreak (2019).
Our study demonstrates a large reduction in the outpatient clinic volume during quarantine periods in 2020, with a 71% reduction of new patients, and 53% of returning patients. When comparing the entire study period, the overall reduction averaged to about 20%. Evaluating the four centers separately, this volume decrease is consistent across centers during mandatory state-imposed quarantine times but does vary by center when comparing over the full timeframe of the study.
Compared to pre-COVID volumes, centers B and D experienced the greatest reduction (−22%, −22.5%, respectively), and centers A and C maintained roughly the same volume (−5%, +7%, respectively). This shows that although state mandatory lockdown compliance was similar between countries (as evident by the similar volume decrease during lockdown periods), times between lockdowns were affected by the different policies of the four sites. While centers A and C, in between quarantines, resumed near normal outpatient clinic operations, centers B and D limited the number of visits (to allow for physical distancing). This is further explained by the initial difference in outpatient volumes between the sites. Looking at the pre-COVID year outpatient volumes—centers B and D had a higher monthly and yearly outpatient volume (3405 and 3171 yearly patients, respectively) than centers A and C (2058 and 1683 yearly patients, respectively), and so to facilitate physical distancing centers B and D had to substantially limit the number of patients visiting the outpatient clinic. Center C stands out as the only center with a slight increase (+7%) in outpatient volume, representing an outlier within the four centers (and countries) and their reaction to the COVID pandemic. Of note, there was a large percentage of patients in all the centers whose visits to the clinic were canceled during the lockdown periods. We do not know nor was it within the scope of this study to ascertain whether these patients were eventually examined.
The role of virtual care during the pandemic has been discussed in the literature. Several studies have shown the utility of telemedicine in limiting in-person exposure while still enabling medical care.14,15 Interestingly, in our study, the two centers that maintained their overall clinic volume did not use virtual care, whereas the two centers with the greater reduction did.
It is perhaps too early to predict the true impact of the first year of the COVID pandemic on the long-term management of pediatric spinal deformities. The overall decrease in clinic volume, specifically during quarantine periods, might potentially cause late presentation of pediatric patients with spinal deformities. This may result in new patients presenting with a greater deformity, more likely to be referred to surgery than non-operative measures (bracing, for instance). This could have a cumulative effect with longer waitlist to surgery, larger deformities, and the potential of more complex surgeries with increased risk of complications.
To the best of our knowledge, this is the first study presenting the effect of COVID-19 on the surgical volume and complication profile of pediatric spine deformity. In our study, the total spine-related surgical volume was increased in centers A, B and C (+9%, +5.8%, +12%, respectively), with a reduction in center D (−36.5%). The increased surgical volume in centers A, B and C can have several explanations. During the pandemic, most educational establishments were closed with some gradually implementing distance/remote learning, this added to the COVID travel limitations (whether self-imposed avoidance or due to government regulations) possibly made it easier for the patients and families to schedule their surgeries during that year. Moreover, regarding the surgeons and surgical teams, in addition to the national COVID travel limitation, there were also specific travel restrictions concerning medical teams during the first year of the pandemic. The combination of the two resulted in less vacations, and so possibly enabling more surgeries to be performed. Center D is the only center in our study with a decrease in surgical volume. This can be explained by the more state regulated return to surgery, not achieving the pre-COVID surgical volume even by the end of the timeframe of the study (December 2020).
Although most centers saw an increase in surgical volume, when considering only AIS patients undergoing primary posterior spinal fusion, there was a 20% reduction in operative volume, in all centers, implying that this population was triaged as lower priority, relative to other etiologies. This was even more prominent in periods of quarantine (AIS −70%).
This disproportionate decrease in AIS surgeries reflects the focus of the spine centers on patients with medical comorbidities or greater spinal deformity. Maybe not wanting to delay their surgeries to avoid the known complications of untreated spinal deformity in this high-risk group, especially with the uncertainty of the initial phase of the pandemic, and not knowing when hospitals would return to regular operations. It could also be that at a time when hospital managements were concerned about ensuring available ventilator machines and intensive care units for COVID-19 patients, it was more justifiable to operate on these patients (rather than the usually healthy AIS population). Of note, the deferral of surgeries by patients themselves, seen commonly in the adult population during the COVID pandemic,16,17 was not apparent in our pediatric cohort.
In the adult population, post-operative pulmonary complications occurred in half of those with a peri-operative positive COVID-19 tests, with an associated mortality as high as 24%. 18 Studies about surgical morbidity and mortality in COVID-positive pediatric patients demonstrate fewer pulmonary complications (7%–14%) and a significantly lower mortality rate (0%–1%).19,20 In this study, all the patients (328) performed a COVID-19 test prior to surgery in 2020, and all were negative. A post-operative test was not routine and performed only in cases of suspected COVID-19 infection (29 patients, 9%), all these patients were COVID-negative also. The complication profile and volume were not significantly different between the study years. There were no COVID-related pulmonary or inflammatory complications in our cohort. Since all the patients in our study were COVID-negative peri-operatively, we cannot comment on the peri-operative complications related to surgery with a COVID-positive status. It is important to note that the patients did not have an added risk of infection by COVID-19, which was a concern both for families and healthcare providers during this period.
There are limitations to our study. First, our analysis included data from hospital sites in four different countries and the effect of differing health regulations and public reaction was not controlled for. However, this allowed us to explore the regional variation, while making our compiled data more generalizable. Second, the novelty of the COVID-19 virus means that it is too early to fully understand or predict the future ramifications of lockdown, delayed treatment, and complications. Finally, we do not have any long-term follow-up data regarding the status of post-op patients. It has been shown that spine surgery increases the risk of peri-operative pulmonary issues, and it could be possible that COVID-19 may increase the post-operative risk for these patients.
To conclude, over the first year of the COVID-19 pandemic, there was a substantial decrease in the pediatric spinal deformity outpatient volume, specifically during lockdown periods, potentially causing in the years to come an increase in late presentation of pediatric spinal deformity patients. More patients presenting with greater deformity increase the likelihood of surgery, extending waitlists and resulting in more complex surgeries with added complications. In addition, the decrease in surgical volume of AIS could cause an extended waitlist for surgeries that were delayed, further compounding surgical demand. And finally, although in some countries, COVID-19 seems now to be as much a part of daily life as the common cold, new variants are likely, with unpredictable infection and morbidity rates. Learning from the experience of four high-volume pediatric spine centers during the first year of the pandemic shows that continued elective pediatric spine surgery with the existing precautions measures is safe, with no added risk of COVID infection or other COVID-related complications, neither for patients nor for medical staff.
Supplemental Material
sj-pdf-1-cho-10.1177_18632521231210356 – Supplemental material for The global impact of the COVID-19 pandemic on pediatric spinal care: A multi-centric study
Supplemental material, sj-pdf-1-cho-10.1177_18632521231210356 for The global impact of the COVID-19 pandemic on pediatric spinal care: A multi-centric study by Hila Otremski, Jennifer Dermott, Kira Page, Lisa S Ipp, John S Blanco, Daniel Studer, Amit Sigal, Dorothy Kim, Carol C Hasler, David E Lebel, Roger F Widmann and Dror Ovadia in Journal of Children’s Orthopaedics
Footnotes
Author contributions
H.O. contributed to the study design; data collection and statistical analysis; and manuscript preparation. J.D. contributed to the data collection; manuscript preparation; and manuscript revision. K.P. contributed to the data collection; manuscript preparation; and manuscript revision. L.S.I. contributed to the data collection; interpretation of data; and manuscript revision. J.S.B. contributed to the study design; interpretation of data; and manuscript revision. D.S. contributed to the data collection; interpretation of data; and manuscript revision. A.S. contributed to the data collection; interpretation of data; and manuscript revision. D.K. contributed to the data collection and manuscript revision. C.C.H. contributed to the study design; interpretation of data; and manuscript revision. D.E.L. contributed to the study design; interpretation of data; and manuscript revision. R.F.W. contributed to the study design; interpretation of data; and manuscript revision. D.O. contributed to the study design; interpretation of data; and manuscript revision.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
This study was approved by: Tel-Aviv Medical Center ethic committee (approval no. 0130-21-TLV) on 24 August 2021, Hospital for Sick Children Research Ethics Board (approval no. 1000076612) on 26 August 2021, University of Basel Ethics Commission Nordwest (approval no. 2021-02042) on 18 August 2021 and Hospital for Special Surgery Institutional review board (approval no. 2021-0124) on 24 August 2021, with informed consent waivered due to the retrospective observational design of the study.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.