
Abstract
Background:
Synthetic calcium sulfate–calcium phosphate bioceramic composite has been developed as a material for bone grafting; however, the literature is limited on outcomes of benign bone tumors treated with bone grafting. This study aims to investigate the outcomes of benign pediatric bone tumors treated with a calcium sulfate–calcium phosphate composite bone graft.
Methods:
A retrospective review at a tertiary pediatric hospital with benign bone tumors treated with curettage and bone grafting with a calcium sulfate–calcium phosphate synthetic bone graft from 2008–2018 was included. Minimum follow-up was 6 months.
Results:
Twenty-seven patients met inclusion criteria with a mean age of 10.3 ± 4.5 years and follow-up was 37.2 ± 22.3 months. Diagnoses were unicameral bone cysts (n = 16) and aneurysmal bone cysts (n = 11). Pathologic fracture was present in 48% (13/27) of patients on admission. All patients were treated using synthetic bone grafts and 37% (10/27) with internal fixation. Following index treatment, 96% (26/27) had resolution of pain and returned to full activity at 13.4 ± 10.7 weeks. Complications occurred in 33% (9/27) of patients; one developed chronic hip pain resulting in decreased physical activity, seven had a tumor recurrence without fracture, and one had tumor recurrence with pathologic fracture. Revision surgery was required in 26% (7/27) of cases. Per the modified Neer outcomes rating system, 52% of patients had a healed bone lesion, 4% had a healing lesion with a bone defect, and 44% had a persistent/recurrent cyst.
Conclusions:
Children with benign bone tumors treated with curettage and bone grafting using a calcium sulfate–calcium phosphate composite had a high incidence of complications and revision surgery.
Level of evidence:
IV.
Introduction
Benign bone tumors in the pediatric population are comprised of heterogeneous etiologies including unicameral bone cysts (UBC), aneurysmal bone cysts (ABC), giant cell tumors, and both ossifying and non-ossifying fibromas.1,2 The disease burden of these benign lesions represents a spectrum of symptom severity from mild to debilitating. Benign bone tumors may be incidental radiographic findings in asymptomatic patients, may cause persistent pain with or without the inability to bear weight, or could result in pathologic fracture. 3 Given the benign characteristic of these lesions and the potential for self-resolution as children approach skeletal maturity, some authors have explored the role of observation in managing benign pediatric bone tumors.4,5 However, widely accepted indications for interventional management include chronic pain and pathologic fracture, which are found in the majority of patients.3 –5
Multiple strategies have been proposed in managing benign primary bone tumors in children, including open curettage and autogenous versus allogenic bone grafting, steroid injection, calcium sulfate grafting, demineralized bone matrix injection, and bone marrow aspirate injection.1,3,6 –8 The purpose of this study was to further and independently investigate the outcomes of benign pediatric bone tumors treated with a calcium sulfate–calcium phosphate composite graft material.
Materials and methods
Approval was obtained from the Institutional Review Board prior to study initiation. A retrospective review was conducted on patients at a tertiary care pediatric hospital from 2008 to 2018. Inclusion criteria were diagnosis of a benign bone tumor, treatment with curettage and grafting using PRO-DENSE, and a minimum of 6 months of follow-up. PRO-DENSE (Wright Medical Group; Memphis, TN, USA) is a synthetic calcium sulfate–calcium phosphate composite material with osteoconductive properties; it has been proposed as a potential bone graft substitute for the treatment of benign bone tumors.7,9 All consecutive patients were included. Exclusion criteria included the use of allograft in combination with calcium sulfate–calcium phosphate composite. Medical charts and radiographs were reviewed for age, diagnosis, presenting symptoms, bone cyst location, pathologic fracture, treatment, time to resolution of presenting symptoms, complications, and revision surgeries. Time to resolution of presenting symptoms was defined as the time from initial presentation to the point at which the patient was both weight-bearing as tolerated and denied any pain or difficulty with motor function of the affected limb.
Outcomes were evaluated using the modified Neer outcomes rating system as originally described by Chang et al. 5 Data were analyzed using descriptive statistics.
Results
Twenty-seven patients were included. The mean age was 10.3 ± 4.5 years and the mean follow-up was 37.2 ± 22.3 months. Fifty-six percent (15/27) of patients were male and 44% (12/27) were female. Diagnoses were UBC (n = 16) and ABC (n = 11). The diagnosis was made based on the radiographic appearance of the lesion and confirmed with biopsy during open curettage. The anatomic location of the tumors was proximal femur (n = 19), pelvis (n = 3), proximal fibula (n = 1), distal humerus (n = 2), distal femur (n = 1), and distal radius (n = 1). Patient characteristics are summarized in Table 1.
Patient characteristics (n = 27).
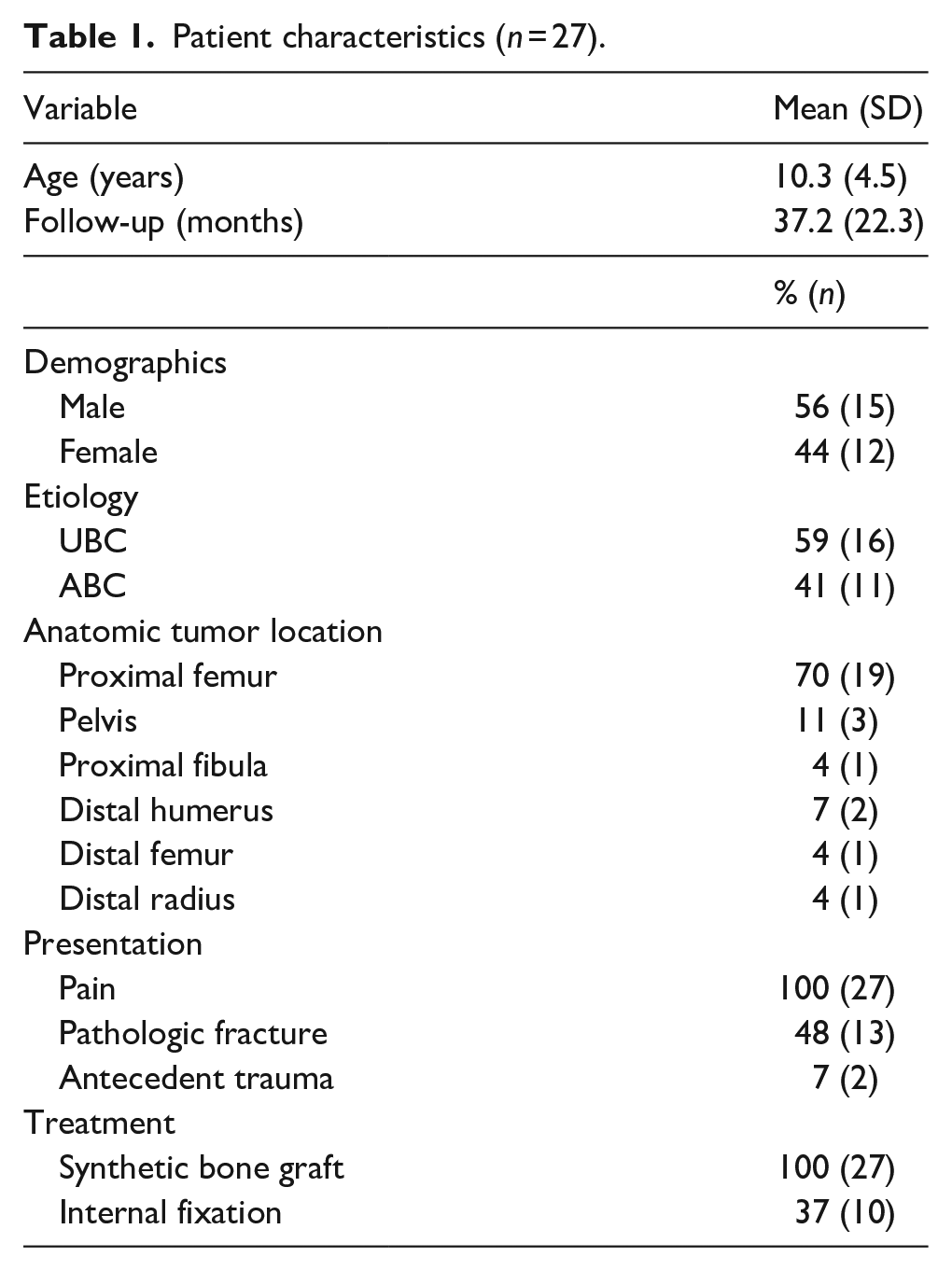
All patients initially presented with pain and 48% (13/27) had a pathologic fracture on admission (Table 1). Antecedent trauma immediately prior to symptom onset was present in 7% (2/27) of patients; no identifiable traumatic event was reported by the other 93% (25/27) of patients. For both patients, the preceding traumatic events were motor vehicle collisions. They both had a proximal femoral UBC, and one also had a pathologic proximal femur fracture while the other did not.
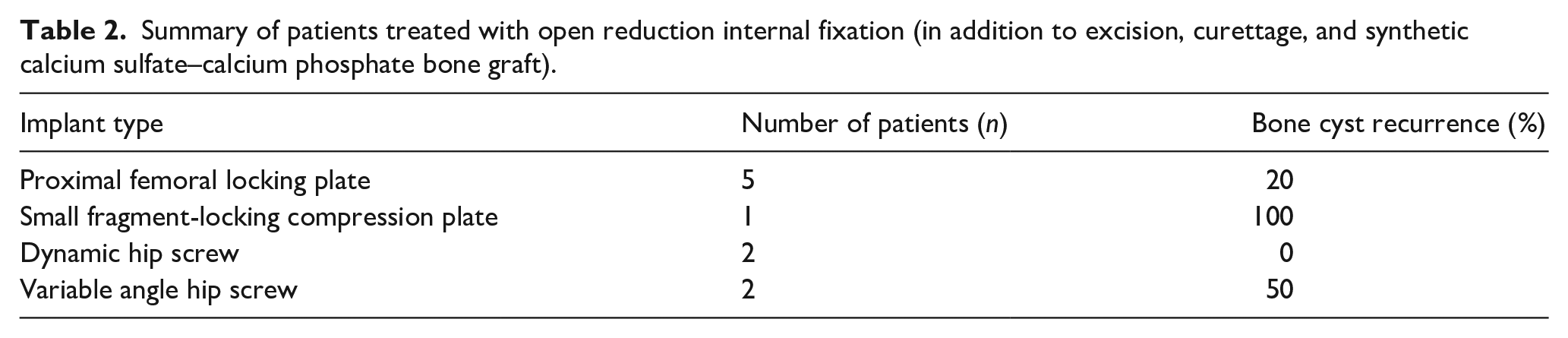
All patients were treated using calcium sulfate–calcium phosphate bone grafting, and 37% (10/27) were also treated with internal fixation (Table 1). All 10 patients treated with internal fixation had proximal femoral involvement, 70% (7/10) of these patients had a pathologic fracture on presentation, and 30% (3/10) of these patients eventually experienced recurrence. Choice of internal fixation was at the discretion of the treating surgeon, and the implants used were proximal femoral locking plate (n = 5), dynamic hip screw (n = 4), and small fragment locking compression plate (n = 1) (Table 2). Twenty-five of the 27 (93%) patients were treated by a single pediatric orthopedic surgeon. The remaining two patients were treated by separate pediatric orthopedic surgeons.
Summary of patients treated with open reduction internal fixation (in addition to excision, curettage, and synthetic calcium sulfate–calcium phosphate bone graft).
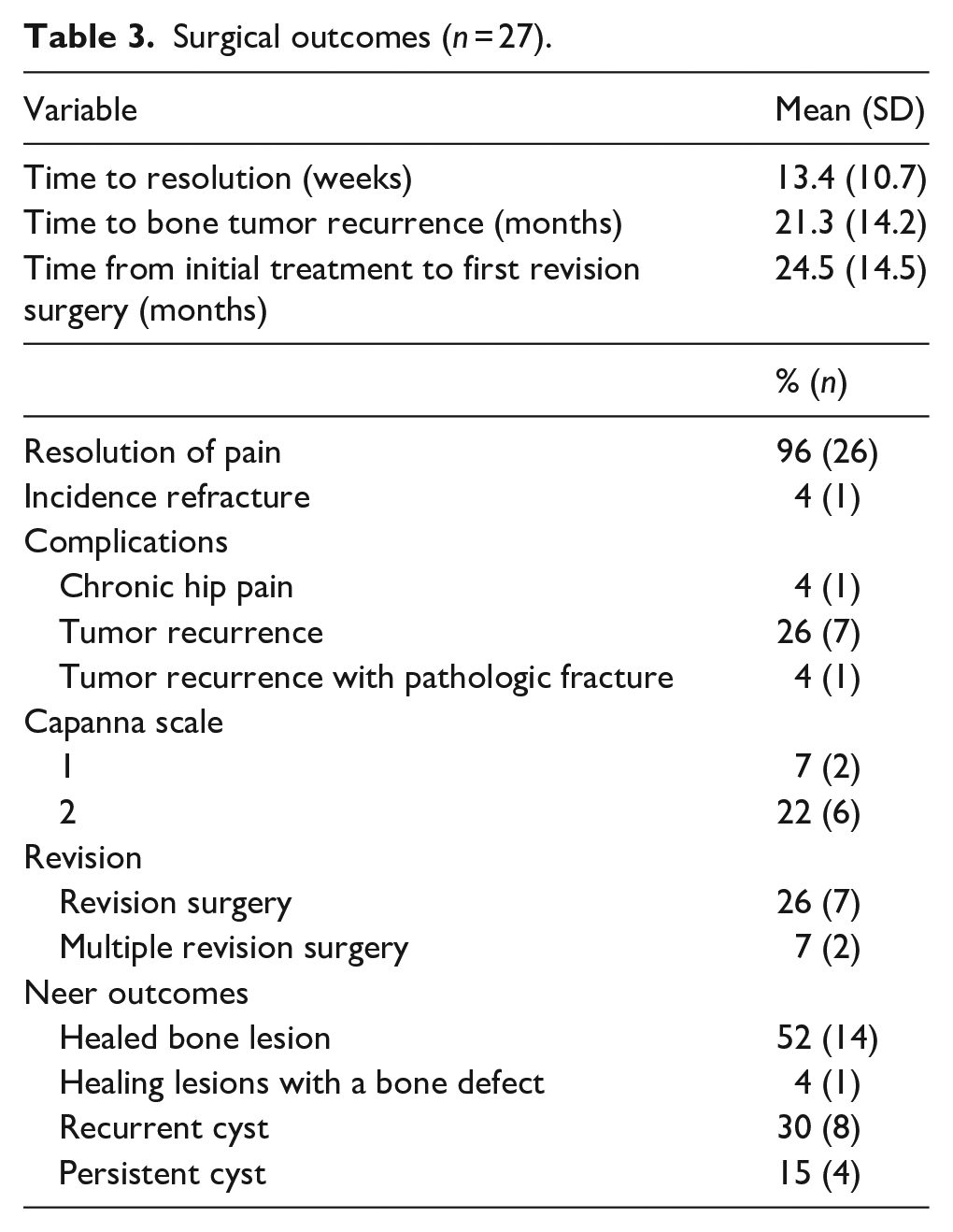
Following treatment, 96% (26/27) of patients had a resolution of pain and returned to full activities. The mean time to resolution of symptoms was 13.4 ± 10.7 weeks. Complications occurred in 33% (9/27) of patients; one patient developed chronic hip pain resulting in decreased physical activity, seven had a tumor recurrence without fracture, and one had a tumor recurrence with pathologic fracture. The incidence of bone tumor recurrence among all patients was 30% (8/27). The mean time to tumor recurrence was 21.3 ± 14.2 months and the incidence of refracture was 4% (1/27). Of the eight patients with recurrence, two were a one on the Capanna scale and six were a two on the Capanna scale when recurrence was first identified.
Revision surgery was required in 26% (7/27) of patients, and multiple revision surgeries were required in 7% (2/27) of patients. The mean time from initial treatment to first revision surgery was 24.5 ± 14.5 months. Per the modified Neer outcomes rating system at final follow-up or prior to revision surgery, 52% (14/27) of patients had a healed bone lesion, 4% (1/27) had a healing lesion with a bone defect, 30% (8/27) had a recurrent cyst, and 15% (4/27) had a persistent cyst. Fifty-six percent (15/27) of patients had a healed or healing lesion, while 44% (12/27) of patients had either a recurrent or persistent cyst. Surgical outcomes are summarized in Table 3.
Surgical outcomes (n = 27).
Discussion
Our study is the largest published series on children with primary benign bone tumors treated using a synthetic calcium sulfate–calcium phosphate bone graft material. Our results found that a significant proportion of pediatric patients treated with this type of calcium sulfate–calcium phosphate bone graft material had recurrent or persistent bone tumors and required revision surgery.
Like other commercially available calcium sulfate–calcium phosphate bone graft substitutes, this particular product is a composite of both calcium sulfate and calcium phosphate that possesses osteoconductive properties and has been shown to have a much slower resorption rate than that of calcium sulfate alone.3,6,7 In theory, the increased time until resorption maximizes the osteoconductive potential of the synthetic material and facilitates both osteogenesis and the healing of cavitary bone defects. 6 Thus, the chemical properties have made it an appealing potential treatment for benign primary bone tumors. Multani et al. studied 14 patients (9 adults and 5 children) who received PRO-DENSE grafting for a benign bone tumor; they reported that only 7% had recurrence requiring reoperation. 7 Fillingham et al. reviewed 56 adult and pediatric patients and also reported a 7% incidence of recurrence. 2 Gentile et al. published a review of 16 cases of pediatric benign bone tumors treated with PRO-DENSE, and they reported a 6% incidence of tumor persistence, and is the only prior study that investigated this treatment solely in the pediatric population. 3
Our study is the largest series of pediatric patients with benign bone tumors treated with open curettage and calcium sulfate–calcium phosphate bone grafting, and the results of our study differ from those in the literature. Our results showed that 30% of patients had a recurrent tumor, 15% had a persistent tumor, and only 52% had complete healing. Twenty-six percent of patients required revision surgery. One patient developed right hip pain with ambulation 1.5 months post-op, radiographs did not reveal an obvious recurrence or other cause for the hip pain. MRIs of the right proximal femur and right hip were obtained, and upon review, a right labral tear was discovered, which was consistent with the symptoms she had developed. Aside from this patient, more than one-third in this series had a clinical course that was complicated by recurrence. These outcomes are less promising than those previously published. The difference in outcomes between our study and the literature may be related to differences in study design, sample size, and length of follow-up. Gentile et al. included only 16 patients in their review—compared to 27 in our study—and this may have rendered their study underpowered. 3 Also, the mean follow-up in the Gentile et al. study was 16 months compared to 37 months in our study; the longer follow-up in our study may have facilitated more accurate reporting of tumor recurrence and need for revision surgery. The studies of Multani et al. and Fillingham et al. included a mix of both adult and pediatric patients while our study was solely comprised of pediatric patients; the mean age was 28 and 18 years in their studies, respectively, compared to 10 years in our study.2,7 The differences in the physiology of children versus adults may have influenced the bone remodeling seen after grafting.
While the prolonged resorption of synthetic calcium sulfate–calcium phosphate bone graft is promoted as advantageous to facilitate osteogenesis, it may make radiographic interpretation more challenging and may potentially mask the beginning of recurrence. Perhaps the more rapidly absorbing alternatives are in fact more advantageous from this perspective. In fact, we feel that the more pessimistic results we are presenting may be due to the longer follow-up which ultimately identified these issues. By contrast, the papers with a higher success rate often had relatively short follow-ups at which point identifying recurrence may have been limited by the lack of resorption of synthetic calcium sulfate–calcium phosphate bone graft at that point.
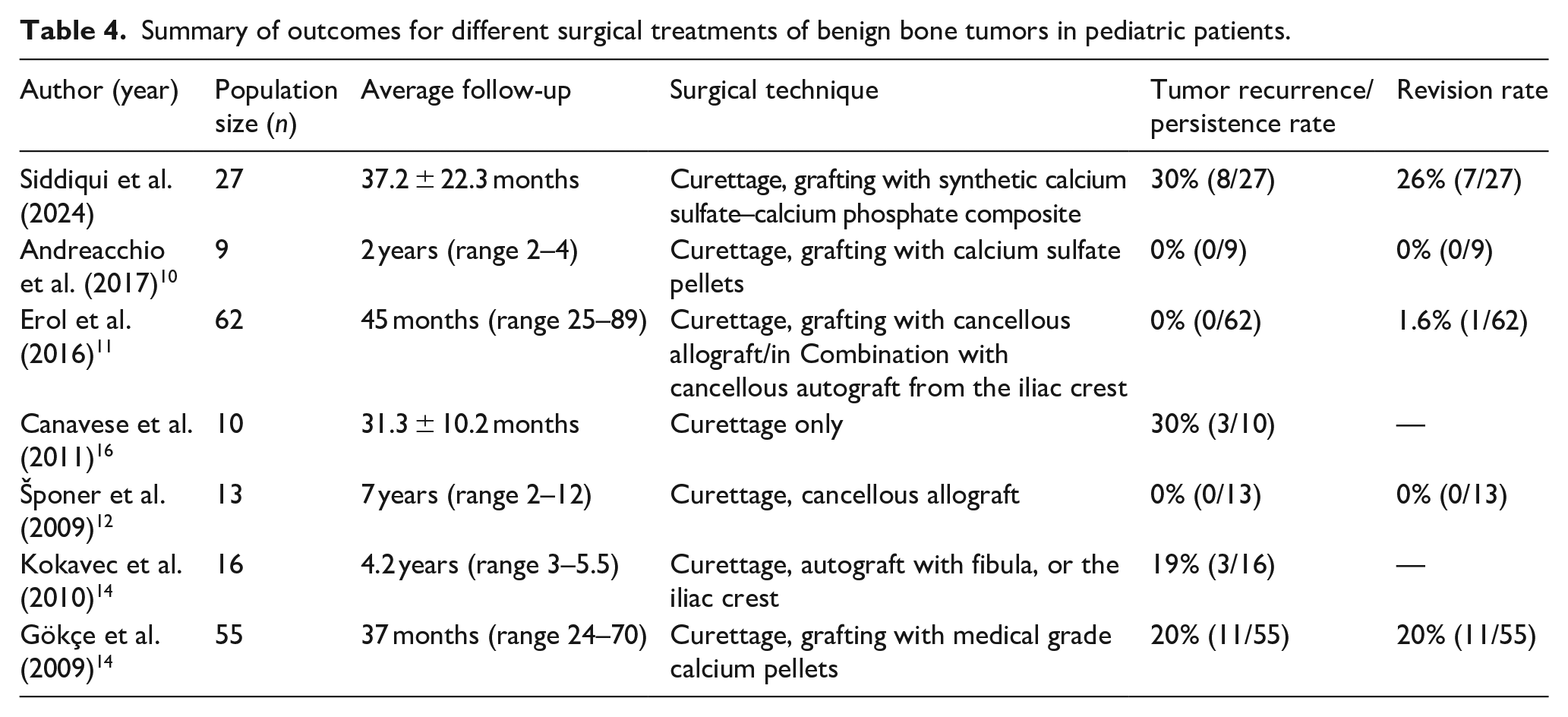
One of the challenges is determining whether recurrence is attributable to the tumor or the treatment. Particularly in the setting of a slow-absorbing synthetic graft, it may be difficult or impossible to determine if the tumor is resolved or if recurrence occurs. We believe that this may be one of the factors that is contributing to the variability in the literature. Andreacchio et al. reviewed pediatric patients treated for symptomatic non-ossifying fibromas with calcium sulfate pellet grafting. Although they found no recurrence, persistence, or other complications, their review only included nine patients with a mean follow-up of 2 years. 10 Erol et al. retrospectively reviewed 62 pediatric patients with proximal femoral benign bone lesions treated with biopsy, curettage, and bone grafting consisting of cancellous allograft cubes alone or in combination with morselized cancellous autograft from the iliac crest. They reported complete clinical recovery in 90.3% of patients between 4–8 months post-op, and median follow-up was 45 months. 11 Šponer et al. who reviewed 13 patients treated with curettage and cancellous allograft had a similarly successful tumor recurrence rate of 0%. 12 By contrast, studies that reviewed the techniques of curettage only, curettage with autograft, and curettage with calcium pellets found tumor recurrence rates more similar to our own with 30%, 19%, and 20%, respectively.13 –15 These studies suggest a markedly different incidence of recurrence based on treatment type, while our series with longer follow-up suggests that it is in fact detection of recurrence that is influenced more than its occurrence (Table 4).
Summary of outcomes for different surgical treatments of benign bone tumors in pediatric patients.
Neer et al. studied multiple approaches to manage proximal humeral UBCs and reported that, following open curettage and allogenic bone grafting, 48% of lesions healed, 21% had a residual defect, and 31% required reoperation. 17 Our results were similar to those of Neer et al.; 52% of primary bone tumors in our study healed completely while 26% required reoperation. Furthermore, Spence et al. reviewed 177 UBC patients also treated with allografting and reported that 55% healed completely and 36% had recurrence with revision surgery. 18 Our results—52% completely healed, 30% recurrence, and 26% reoperation—again mirror those of patients treated using allograft. The similarities in outcomes between calcium sulfate–calcium phosphate bone grafting and allografting in the literature suggest that this novel calcium sulfate–calcium phosphate compound may not be superior to established prior treatments. A future meta-analysis or comparative study would be worthwhile to further investigate the effectiveness of calcium sulfate–calcium phosphate bone grafting substitutes.
Limitations of this study include our sample size (n = 27). However, this is the largest series to date on the use of calcium sulfate–calcium phosphate bone grafting for the treatment of benign pediatric bone tumors, and thus our results significantly contribute to the existing literature. A further limitation is that 93% of our patients were treated by a single surgeon. The results of our study may have been heavily dependent on the individual treating surgeon and may not accurately reflect the true effect of calcium sulfate–calcium phosphate on the management of benign bone tumors in children. There was also no institutional protocol to determine whether a tumor was treated with calcium sulfate–calcium phosphate bone grafting versus other treatments such as allograft, autograft, or steroid injection. There may have been selection bias that led to a certain subset of patients being treated using calcium sulfate–calcium phosphate bone grafting. In addition, most patients had a proximal femoral lesion (n = 19), and given the small sample, we were unable to perform a subgroup analysis. Of the seven patients who required revision surgery, six of them involved the proximal femur.
Our study is the largest series to date to investigate the outcomes of benign pediatric bone tumors managed with open curettage and grafting using a synthetic, osteoconductive calcium sulfate–calcium phosphate composite. Our results contradict prior findings in the literature and suggest that using a calcium sulfate–calcium phosphate bone graft composite yields significant rates of tumor persistence and reoperation that are comparable to those of historical treatments. Orthopedic surgeons should be cognizant of these findings when considering this novel technology, and further research is warranted to optimize the treatment of primary bone tumors in children and determine the optimal role of bone graft substitutes.
Supplemental Material
sj-pdf-1-cho-10.1177_18632521241310049 – Supplemental material for Low rate of healing and high incidence of complications in benign pediatric bone tumors treated with synthetic calcium sulfate–calcium phosphate bone graft
Supplemental material, sj-pdf-1-cho-10.1177_18632521241310049 for Low rate of healing and high incidence of complications in benign pediatric bone tumors treated with synthetic calcium sulfate–calcium phosphate bone graft by Ali A Siddiqui, Lindsay M Andras, Annika Y Myers, Bensen B Fan, James Bennett, Kenneth D Illingworth, David L Skaggs and Vernon T Tolo in Journal of Children's Orthopaedics
Footnotes
Author contributions
A.A.S.: data curation, formal analysis, investigation, resources, and manuscript preparation. L.M.A.: conceptualization/design, methodology, investigation, formal analysis, supervision/oversight, resources, and manuscript preparation. A.Y.M.: data curation, formal analysis, investigation, resources, and manuscript preparation. B.B.F.: data curation, formal analysis, and manuscript preparation. J.B.: data curation, formal analysis, and manuscript preparation. L.K.D.I.: conceptualization/design, methodology, investigation, formal analysis, supervision/oversight, resources, and manuscript preparation. D.L.S.: conceptualization/design, methodology, investigation, formal analysis, supervision/oversight, resources, and manuscript preparation. V.T.T.: conceptualization/design, methodology, investigation, formal analysis, supervision/oversight, resources, and manuscript preparation.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
This study has been carried out with approval from the Institutional Review Board at Children’s Hospital Los Angeles and Boston Children’s Hospital.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.