
Abstract
Vertebral osteomyelitis caused by Aspergillus nidulans is rare and usually affects immunocompromised patients. This report presents a case of thoracic vertebral osteomyelitis with epidural abscesses due to A. nidulans in a 40-year-old immunocompetent female who presented with back pain, numbness and weakness of both lower limbs. Magnetic resonance imaging demonstrated osteomyelitis involving the thoracic (T)1–T3 vertebral bodies with epidural abscesses, resulting in spinal compression. The patient underwent a decompression laminectomy of T1–T3 and debridement of the thoracic epidural inflammatory granuloma. Histopathology revealed fungal granulomatous inflammation. The patient received 6 mg/kg voriconazole every 12 h (loading dose on day 1) followed by 4 mg/kg voriconazole twice daily for 1 month, administered intravenously. The patient returned with recurrent back pain 16 months after initial presentation. A. nidulans was identified by fungal culture and polymerase chain reaction. The patient showed no evidence of recurrence 1 year after a 6-month course of oral voriconazole. The key to the effective treatment of Aspergillus osteomyelitis is not to excise the abscess, but to administer systemic antifungal drug therapy.
Keywords
Introduction
Vertebral osteomyelitis is diagnosed with increasing frequency as a result of advances in magnetic resonance imaging (MRI) technology. 1 The prevalence of vertebral Aspergillus osteomyelitis also rises with the increasing population of immunocompromised patients, although it still presents a diagnostic and therapeutic challenge, because the symptoms are nonspecific. 2 It is difficult to distinguish between an Aspergillus infection and bacterial infection, based on imaging studies. 3
Aspergillus nidulans is one of several species of Aspergillus with low pathogenicity, but it can also cause invasive aspergillosis with associated morbidity and mortality. 4 Vertebral osteomyelitis caused by A. nidulans is rare and the majority of reported cases have arisen in immunocompromised patients. 5 This report presents a case of thoracic vertebral osteomyelitis with epidural abscesses due to A. nidulans in an immunocompetent patient; this infection was identified by fungal culture and polymerase chain reaction (PCR) analysis.
Case report
A 40-year-old Chinese woman was admitted to the Department of Neurosurgery, Qilu Hospital, Shandong University, Jinan, Shandong Province, China in March 2010. Her symptoms were back pain, numbness and weakness of both lower limbs. She had a history of lung fungal granuloma and brain cysticercosis. Computed tomography (CT) revealed a space-occupying lesion in the apex of the right lung, first identified over 6 years previously (October 2003). The lesion was resected using a right thoracotomy. The histopathology of the lung lesion was granulomatous inflammation with the presence of Aspergillus. The patient developed neurocysticercosis 3 years later in September 2006, which was removed in the Department of Neurosurgery, Qilu Hospital. Later she complained of persistent back pain without spontaneous relief for 1 year. Approximately 20 days before the second admission to the Department of Neurosurgery, Qilu Hospital, she experienced numbness and weakness in both lower limbs. This numbness and weakness became progressively worse until the patient could not walk without assistance. MRI examinations of the cervicothoracic spine showed osteomyelitis involving the thoracic (T)1–T3 vertebral bodies and associated paravertebral tissues (Figure 1). The lesion showed low signal intensity on T1-weighted images, and high signal intensity on T2-weighted images and T1-weighted images with gadolinium enhancement. Soft-tissue infection was more severe on the left side. There were anterior and posterior epidural abscesses extending from T1 to T3, as well as bilateral pleura, resulting in moderate spinal cord compression.
Magnetic resonance imaging scans of the cervicothoracic spine of a 40-year-old Chinese woman who presented with back pain, numbness and weakness of both lower limbs. The images show osteomyelitis involving the thoracic (T)1–T3 vertebral bodies and associated paravertebral tissues (arrows): A, sagittal T1-weighted image; B, sagittal T2-weighted image; C, gadolinium-enhanced sagittal T1-weighted image.
Body temperature was normal at admission. A physical examination revealed percussion pain in the central back at the T1–T3 levels. However, no redness or swelling was observed on her back. Muscle strength was grade 3, which was evaluated using the British Medical Research Council grading system. 6 Pain sensations in her skin were reduced below the xiphoid process. The Chaddock reflex was bilaterally positive. Laboratory analyses revealed the following: White blood cell count, 9.98 × 109 cells/l (differential count: Neutrophils, 70.06%; lymphocytes, 20.96%; monocytes, 6.24%; eosinophils, 2.26%; basophils, 0.48%); red blood cell count, 4.43 × 1012 cells/l; haemoglobin, 88.9 g/l; platelets, 458 × 109 platelets/l; alanine aminotransferase, 15 U/l; erythrocyte sedimentation rate (ESR), 48 mm/h; immunoglobulin G, 25.7 g/l; complement C3, 0.62 g/l; C-reactive protein, 21.8 mg/l; CD4+T cell proportion, 50.44%; CD8+ T cell proportion, 23.16%; CD4+/CD8+ ratio, 2.18. The absolute CD4+ and CD8+ T cell counts and their ratio were normal. The patient was HIV negative.
The persistent back pain and worsening neurological symptoms, especially the progressive paraparesis, led to the decision to perform a decompressive surgery. The patient underwent a T1–T3 laminectomy and surgical exploration. This revealed thickened dura mater and an extensive epidural inflammatory granuloma around the spinal cord at the T1–T3 levels. The lesion infiltrated into the paravertebral tissues through the intervertebral foramina, causing narrowing of the left T1–T3 intervertebral foramina and scarring of the associated roots. A decompression laminectomy of T1–T3 and debridement of the epidural inflammatory granuloma were performed. The intraoperative frozen-section analysis showed hyperplastic fibrous connective tissue with chronic inflammatory cell infiltration. Removal of the epidural lesion was performed. After the operation, the patient’s numbness and disability in both lower limbs were relieved, but the back pain remained. Postoperative MRI showed almost-complete resolution of the epidural lesion.
As the intraoperative frozen section analysis did not indicate the likelihood of fungal infection, no fungal culture of the surgical tissue was performed. However, histopathology revealed fungal granulomatous inflammation, with multifocal fungal spores and mycelia (Figure 2). Periodic acid-Schiff staining of fungal cell walls, which stain magenta, was positive. The patient received antifungal therapy (6 mg/kg voriconazole every 12 h as a loading dose on day 1, followed by 4 mg/kg voriconazole twice daily) administered intravenously. The back pain had disappeared when the patient was discharged from hospital on day 18 of the antifungal therapy. The patient was then asked to continue 4 mg/kg voriconazole twice daily, administered intravenously at Yucheng Hospital, Dezhou, Shandong Province, China for ≥3 months.
Light photomicrographs of frozen sections of an epidural lesion that was removed during decompressive surgery of the spine; the lesion showed an inflammatory granuloma with uniform septated hyphae, branching at 45°, which were morphologically consistent with Aspergillus infection. A, Haematoxylin and eosin staining (original magnification × 400); B, Periodic Acid-Schiff staining of fungal cell walls, which appear magenta under light microscopy (original magnification × 400).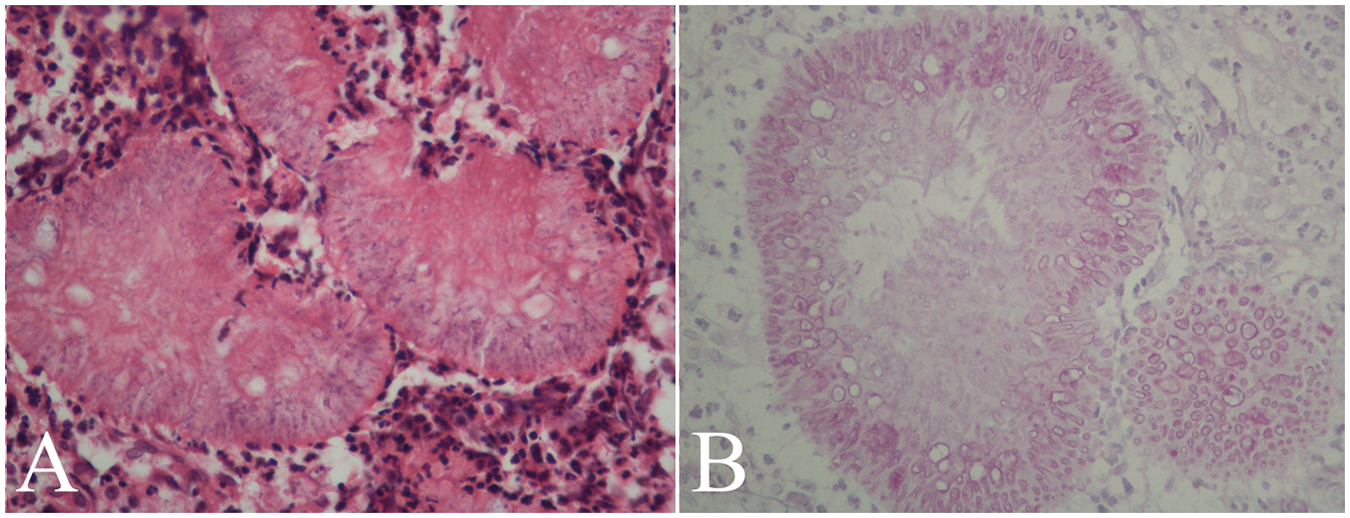
In July 2011, 16 months after initial presentation, the patient returned with recurrent back pain. The patient had not followed the doctor's advice and had only continued intravenous voriconazole for 1 month after hospital discharge. The MRI with gadolinium enhancement showed recurrent T1–T3 vertebral osteomyelitis and epidural abscess. A CT-guided needle biopsy of the paravertebral lesion, fungal culture and PCR analysis were performed. Genome sequencing results identified A. nidulans. According to drug susceptibility test results, the patient subsequently recommenced 4 mg/kg voriconazole every 12 h, administered intravenously. Her back pain had disappeared by the time she was discharged (August 2011). She continued 200 mg voriconazole every 12 h administered orally for 6 months. One year after systemic antifungal therapy was completed, she is well with no sign of recurrence.
Discussion
Aspergillus is a ubiquitous opportunistic fungus that only develops hyphae in the pathogenic phase. It is seldom pathogenic in healthy hosts who have fully functioning immune systems. The annual incidence rate of invasive Aspergillus infection is ∼12 per 1,000,000. 7 Only 20 of the recognized species of Aspergillus have been verified to cause infections in humans and animals.8,9 One of the most import fungi is A. fumiguatus, which accounts for more than 90% of human infections. 8 The other Aspergillus fungi that infect humans include A. flavus, A. nidulans, A. versicolor, A. niger, A. terreus and A. flaviparus.8,9 A. nidulans is uncommon in indoor environments, but it has been frequently encountered in soil.10,11 The patient described in the present case report had reared cattle and sheep outdoors for a long time, so she was at a high risk of becoming infected with A. nidulans.

AmB, amphotericin B; AML, acute myeloid leukaemia; C, cervical; F, female; L, lumbar; M, male; T, thoracic.
There are three possible origins of the spinal epidural abscess associated with vertebral osteomyelitis: Haematogenous spread from a distant organ, contiguous spread from an adjacent involved organ; iatrogenic inoculation.18,36 Aspergillus infection more commonly results from haematogenous spread of invasive pulmonary aspergillosis in immunocompromised patients, which occurs in 6–14% of patients after transplantation. 31 In addition, Aspergillus involvement of the vertebral body can also occur by contiguous spread from neighbouring tissues such as the skin, liver, kidney, thyroid, brain and most commonly lungs. 8 In the present case, the patient had a history of pulmonary Aspergillus granulomatous inflammation but she had never received a lumbar puncture. In our opinion, the vertebral osteomyelitis possibly spread from the adjacent lung tissues, although the lung fungal granuloma had already been resected over 6 years previously.
The key to effective treatment for Aspergillus osteomyelitis is not the excision of the abscess, but systemic antifungal drug therapy. 17 In consideration of the widespread nature of the disease, surgery is unlikely to clear all involved tissues. Bridwell et al. 37 argued that surgical intervention should be limited to cases that fail systemic drug treatment. In the present case, the patient received a surgical decompression on her first admission, but relapsed soon after unauthorized withdrawal of antifungal drug therapy. As the clinical response to antifungal therapy predicts long-term survival in patients with vertebral Aspergillus osteomyelitis, 9 the standardized application of antifungal agents is very important. However, in our opinion, emergency surgery is usually necessary in cases of spinal cord compression, as was observed in the present case.
Footnotes
Declaration of conflicting interest
The Authors declare that there are no conflicts of interest.
Funding
This work was supported by grants from the National Natural Science Foundation of China (No. 30901536) and the Natural Science Foundation of Shandong (Nos ZR2009CM113 and ZR2010HQ026). This study was also supported by grants from the Promotive Research Fund for Excellent Young and Middle-aged Scientists of Shandong Province (No. BS2011SW015) and the Independent Innovation Foundation of Shandong University (No. 2010TS103).