
Abstract
Purpose:
Patients of elective orthopedic surgeries often reduce activity levels during postoperative recovery. It is unclear whether these extended periods of modified activities lead to weight changes. The purpose of this study was to evaluate changes in body mass index percentile in pediatric patients over 2.5 years following primary musculoskeletal surgeries.
Methods:
Institutional records for utilized current procedural terminology codes were used to identify patients aged 21 years or younger who underwent elective surgery at a single pediatric orthopedic institution between October 2016 and December 2018. Non-primary surgeries and patients without preoperative body mass index measurements were excluded. Demographic characteristics, height, weight, and body mass index within 30 months of surgery were collected. Body mass index relative to age was calculated. Analysis of body mass index changes at follow-up intervals of 3–7, 9–18, and 24–30 months after surgery was performed for the overall sample, within surgical categories, and within preoperative weight classifications.
Results:
A total of 1566 patients (53.1% female, average age 12.4 years) were included. Over one-third of patients were overweight or obese at presentation. The average change in body mass index percentile relative to baseline was increased at all follow-up intervals. Values reached significance at 9–18 months (p = .002) and 24–30 months (p = .001). While underweight and normal-weight patients had increased body mass index at all three timepoints, overweight or obese patients decreased.
Conclusions:
Patients undergoing elective orthopedic procedures may experience significant changes in body mass index percentile postoperatively. At extremes of weight, patients experience improvement toward the mean, but most patients may undergo body mass index increases beyond what would be expected during normal growth.
Level of evidence:
Retrospective level III.
Introduction
High body mass index (BMI) is directly implicated in a broad swath of negative health outcomes, including cardiovascular disease, stroke, respiratory disease, and cancer.1 –4 In addition, overweight status and obesity are associated with increased risk of musculoskeletal injuries, as well as postoperative complications and poorer outcomes following orthopedic surgeries in children and adolescents.5 –10
Many musculoskeletal surgeries necessitate extended periods of activity restriction during postoperative recovery.11 –13 Given that higher levels of exercise in children are associated with lower childhood BMI, reduced activity levels after surgery may lead to increased weight or BMI. 14 However, it is not known whether orthopedic surgeries performed in the pediatric population commonly result in weight gain secondary to postoperative activity restrictions. Particularly, in athletic populations accustomed to significant amounts of exercise, it is possible that patients may experience undesired weight gain. However, limited literature exists on the association between orthopedic surgeries and postoperative changes in weight or BMI, particularly in youth. While a small number of studies have demonstrated a correlation between anterior cruciate ligament (ACL) rupture and increases in body fat percentage or BMI status in both youth and adult populations, to the best of our knowledge, no studies have explored an association between other common orthopedic procedures and postoperative weight gain in a pediatric population.15 –17 The purpose of this study was to explore changes in BMI percentile following primary elective orthopedic surgeries in children and adolescents.
Materials and methods
After institutional review board approval was obtained, institutional records for utilized current procedural terminology codes were used to identify patients 21 years of age or younger who underwent elective surgery at a single pediatric orthopedic institution between October 2016 and December 2018. 18 These codes identified the procedures listed in Supplemental Appendix 1. The electronic medical record was utilized to compile the following data on patients undergoing the procedures corresponding to the codes of interest. Exclusion criteria were non-primary surgery, other surgical procedures performed concurrent to the procedure code of interest, spine procedures that were not anterior or posterior spinal fusions of less than 13 levels, lack of preoperative height and weight measurements, or lack of follow-up visits with height, weight, or BMI measurements available within any of the three prescribed postoperative intervals (Figure 1). The initial query identified 2585 patients undergoing procedures of interest, with 1566 patients remaining following the application of exclusion criteria. Follow-up intervals of 3–7, 9–18, and 24–30 months were determined based on standard follow-up protocols. For participants who underwent spine surgery for scoliosis, preoperative BMI was calculated using postoperative height within 6 weeks of surgery to adjust for the shortening effect of spinal deformities on height in these patients. To account for natural changes in height and weight with physical maturation, BMI percentiles were calculated from BMI z-scores, which were determined using a formula based on the Centers for Disease Control (CDC) BMI-for-age percentiles growth charts.19,20 Average change in BMI percentile at each follow-up interval compared with preoperative BMI percentile was calculated for each observation.
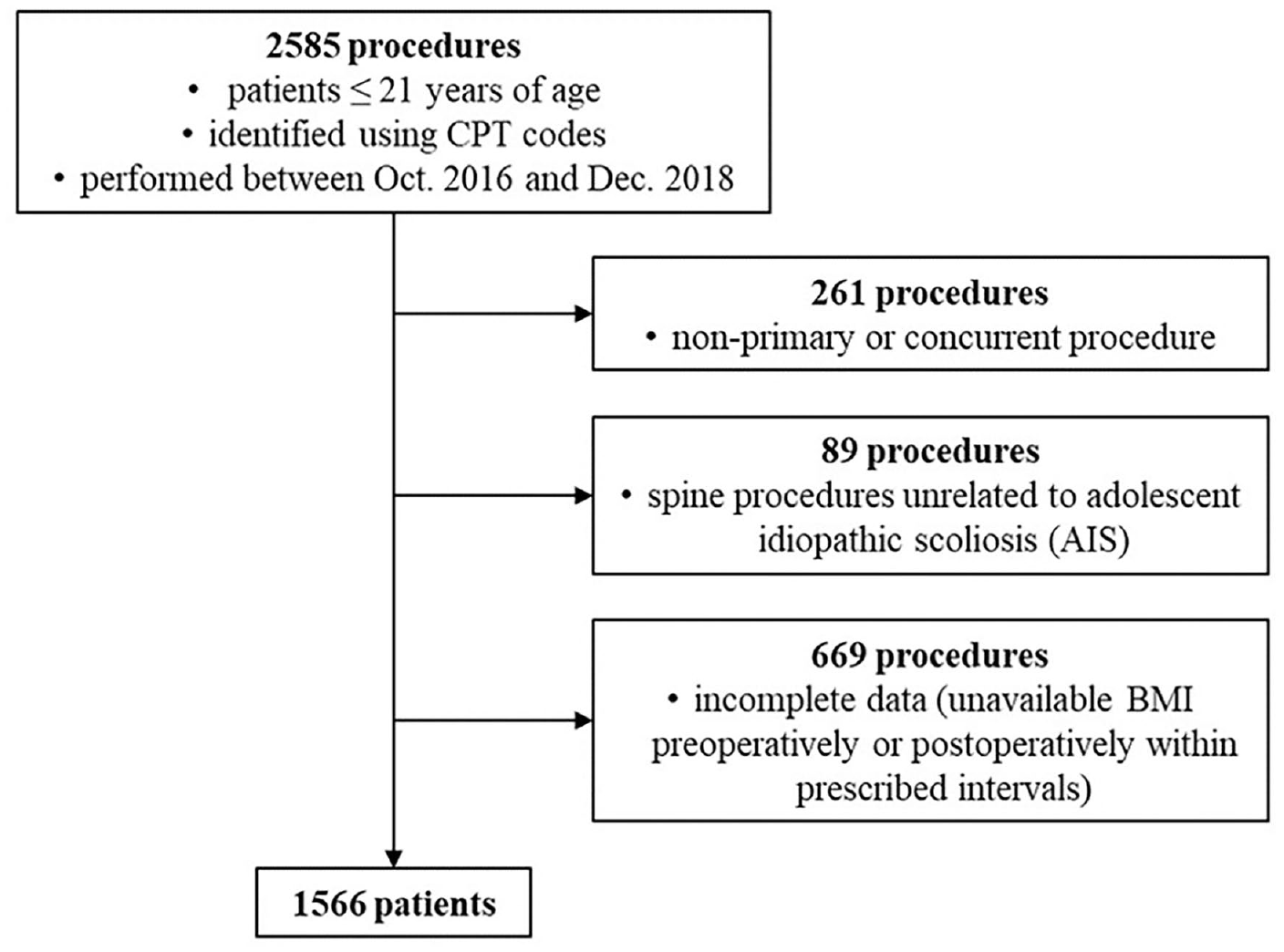
Patient selection and exclusion criteria.
Statistical analysis of changes in BMI percentile was performed for the overall sample, within surgical categories, and within preoperative weight classifications per the CDC delineations of these categories for children, which define underweight as BMI less than 5th percentile for age, normal weight from 5th up to 85th percentile, overweight from 85th up to 95th percentile, and obese as 95th percentile or greater. 21 Within the cohort of patients who underwent sports-related procedures, a Mann–Whitney U test was used to compare differences between upper extremity and lower extremity surgeries. One-way analysis of variance and nonparametric Kruskal–Wallis tests were used to compare changes in BMI percentile between BMI category cohorts. The Tukey–Kramer method and Dwass-Steel-Critchlow-Fligner procedure were also used for multiple comparisons. To compare changes in BMI percentile between follow-up intervals, a paired Student’s t-test and nonparametric Wilcoxon signed-rank test were used. All analyses were performed using Statistical Package for the Social Sciences.
Results
A total of 1566 patients (53.3% female) were available for study (Table 1). The average age at surgery was 12.4 years (range 5–20). The most common surgical category was sports, followed by spine; foot and ankle; lower extremity epiphysiodesis; lower extremity osteotomy; non-sports hip; and tendon lengthening or release. Overall, 120 patients (7.7%) were classified as underweight at the time of surgery, 869 (55.5%) normal weight, 224 (14.3%) overweight, and 353 (22.5%) obese.
Patient demographics.
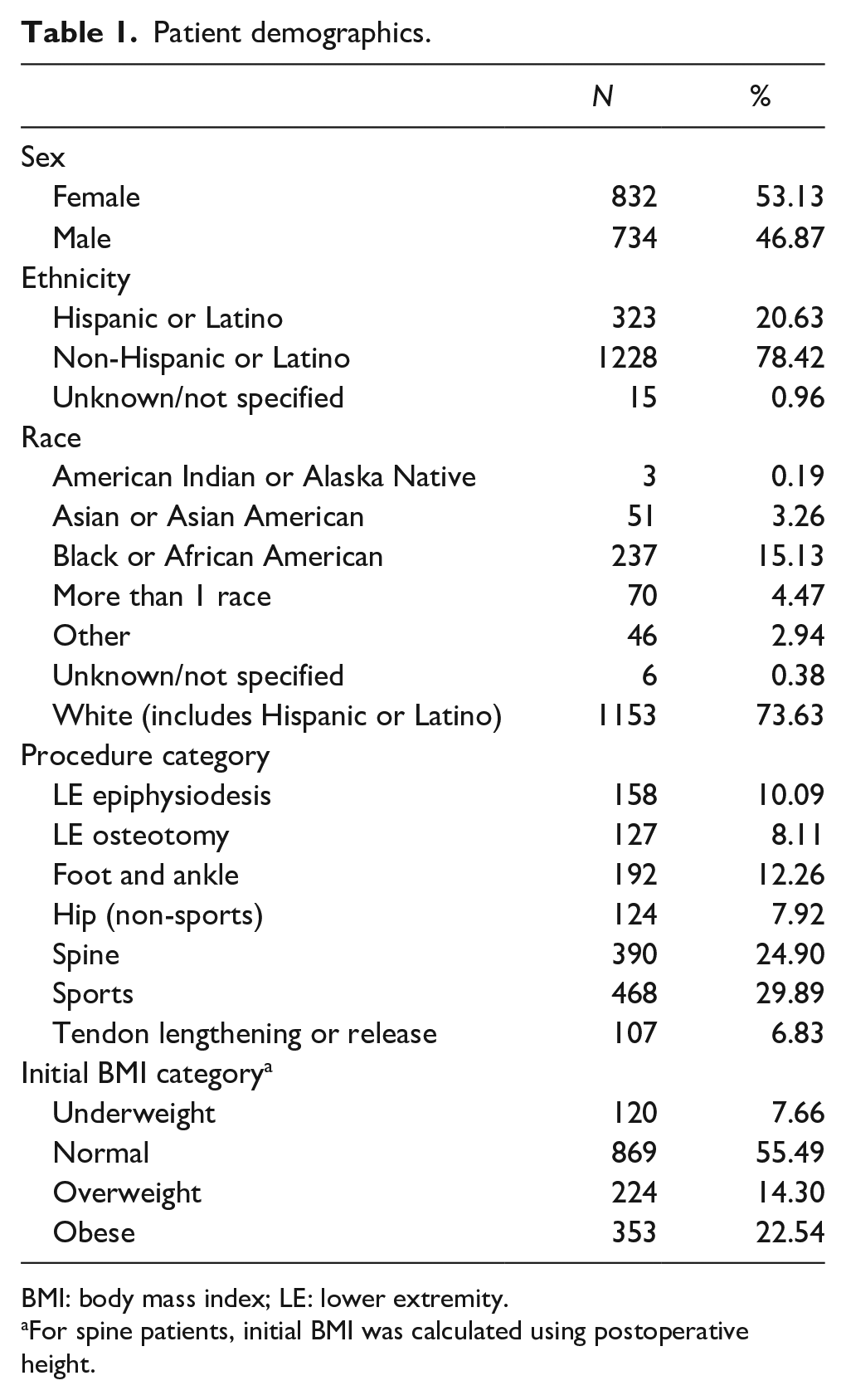
BMI: body mass index; LE: lower extremity.
For spine patients, initial BMI was calculated using postoperative height.
For the overall cohort, the average change in BMI percentile relative to baseline was increased at all 3 follow-up timepoints, with values reaching significance at 9–18 and 24–30 months (Table 2). Moreover, the magnitude of the increase trended upward over the course of the follow-up period. The same trend of increased BMI percentile held true after the cohort was divided into categories based on surgical procedure; however, the difference at 24- to 30-month follow-up was significant only for spine procedures and tendon lengthening or release procedures (Table 3). Notably, at nearly 2 years following pediatric spine procedures, the average BMI percentile increase approached 10 points (p = .032). In contrast, patients undergoing sports procedures experienced BMI percentile changes of less than 1 point through the first 1.5 postoperative years.
Average change in BMI percentile—overall.
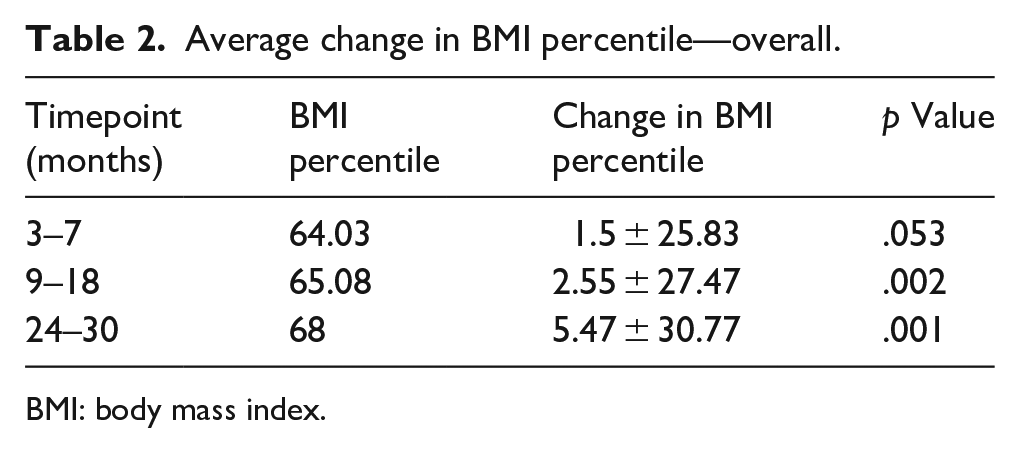
BMI: body mass index.
Average change in BMI percentile by procedure category.
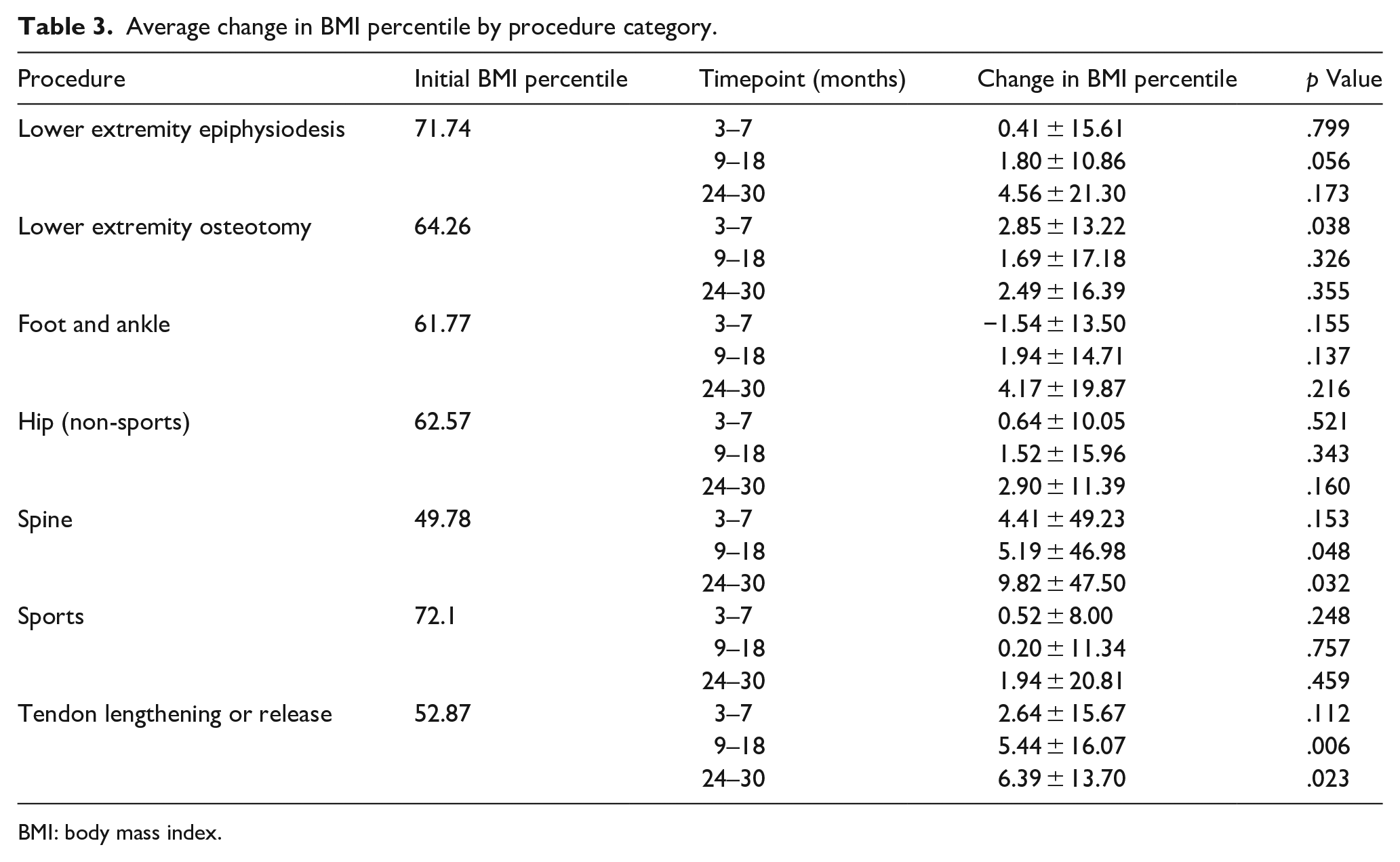
BMI: body mass index.
Sports surgeries were subdivided into upper extremity and lower extremity groups. At 24- to 30-month follow-up, the upper extremity cohort demonstrated an average increase in BMI percentile of 13.3 points, while the lower extremity cohort decreased by 0.42 points (p = .015). Differences at earlier timepoints did not reach significance (Table 4).
Average change in BMI percentile by upper or lower extremity—sports only.

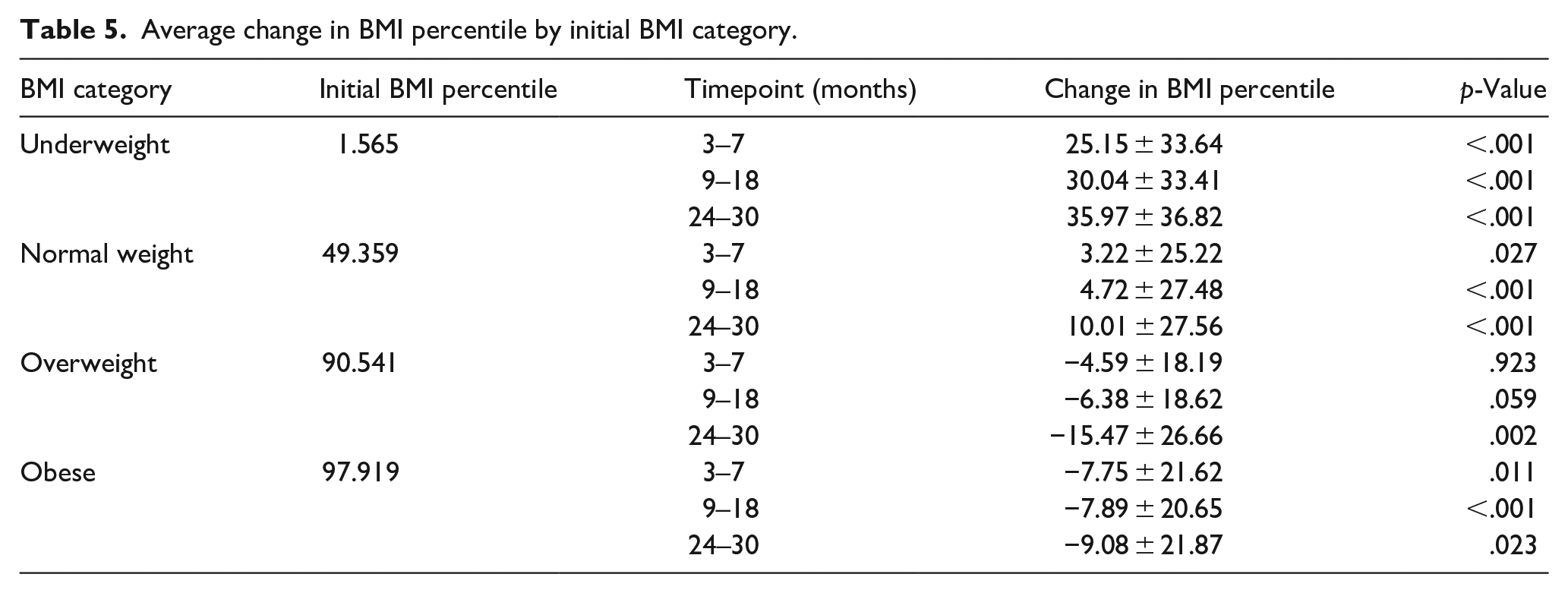
Significant differences were noted in comparisons across preoperative BMI categories (Table 5, Figure 2). At all three timepoints, patients who were underweight or normal weight at the time of surgery were more likely to have significant increases in BMI percentile, with particularly large changes noted in the underweight population. While normal-weight patients also increased BMI percentile at all three timepoints, they did so to a lesser degree. In contrast, patients who were overweight or obese at the time of surgery tended to experience significant decreases.
Average change in BMI percentile by initial BMI category.
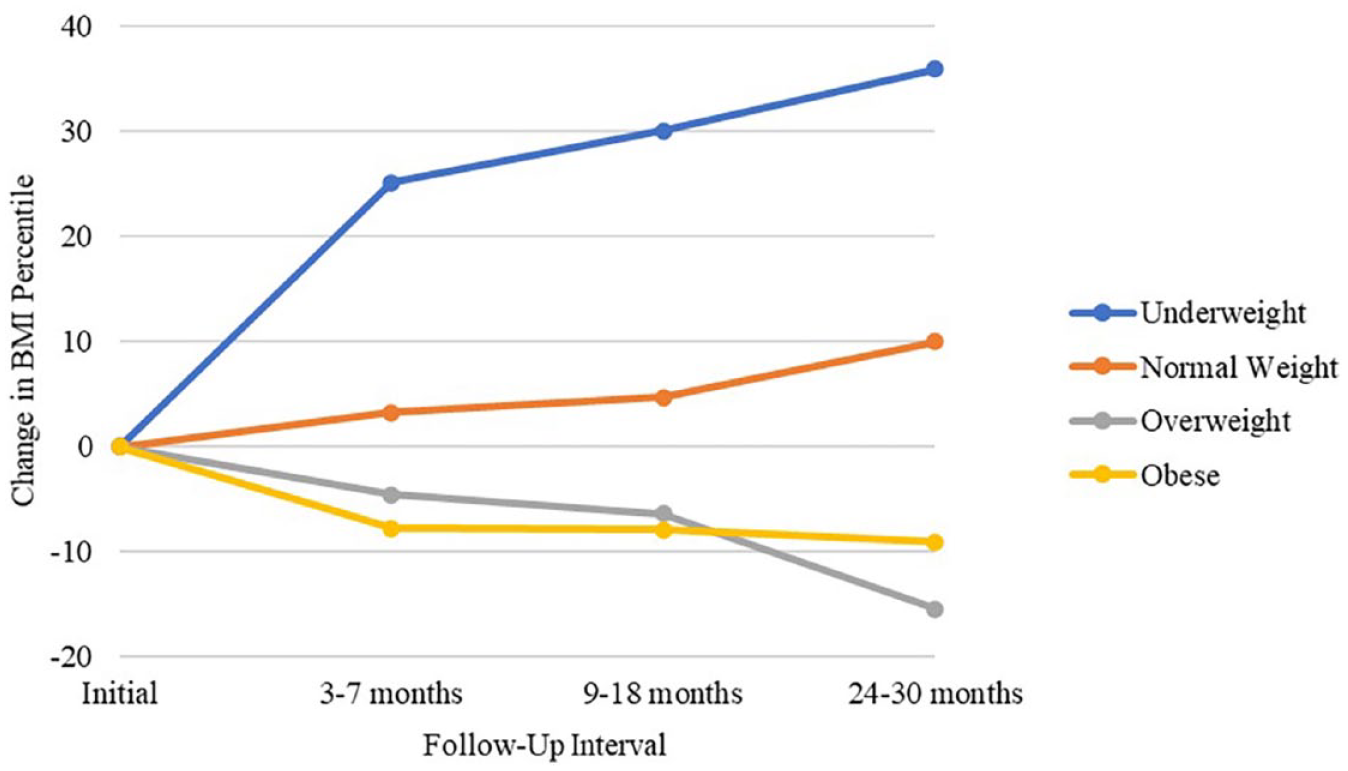
Change in BMI percentile by initial BMI category.
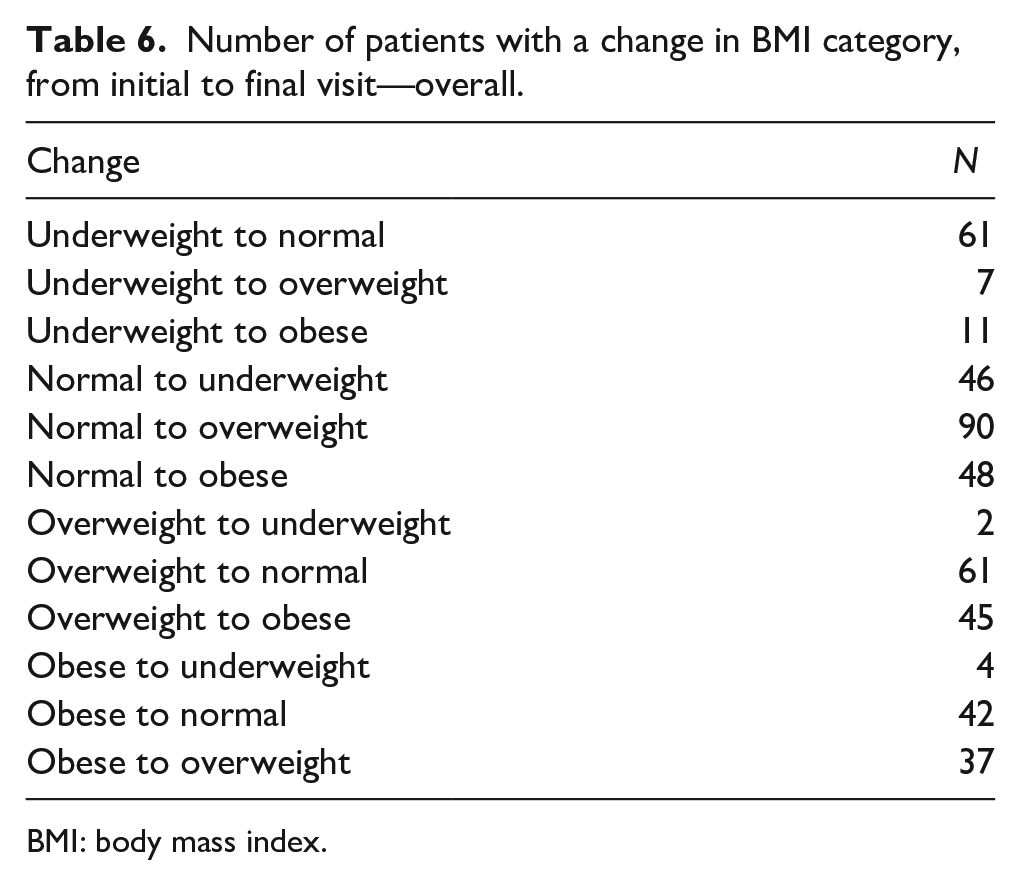
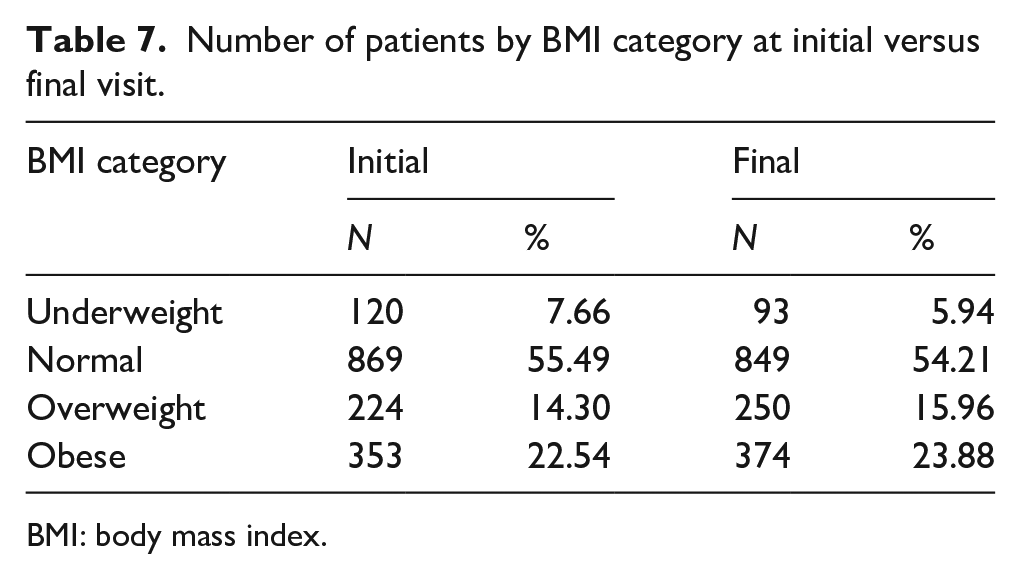
Many patients changed BMI categories over the course of the study (Table 6). Of 120 patients who were underweight at presentation, over half had become normal weight by the final follow-up. Of patients who were initially obese, 22.4% had decreased to overweight or normal weight by final follow-up, and among overweight patients, 27.2% became normal weight. However, overall, the proportion of patients who were overweight or obese had grown by the end of the study, with the greatest contribution coming from initially normal-weight patients who became overweight or obese, reflecting the general pattern of increased BMI percentile (Table 7).
Number of patients with a change in BMI category, from initial to final visit—overall.
BMI: body mass index.
Number of patients by BMI category at initial versus final visit.
BMI: body mass index.
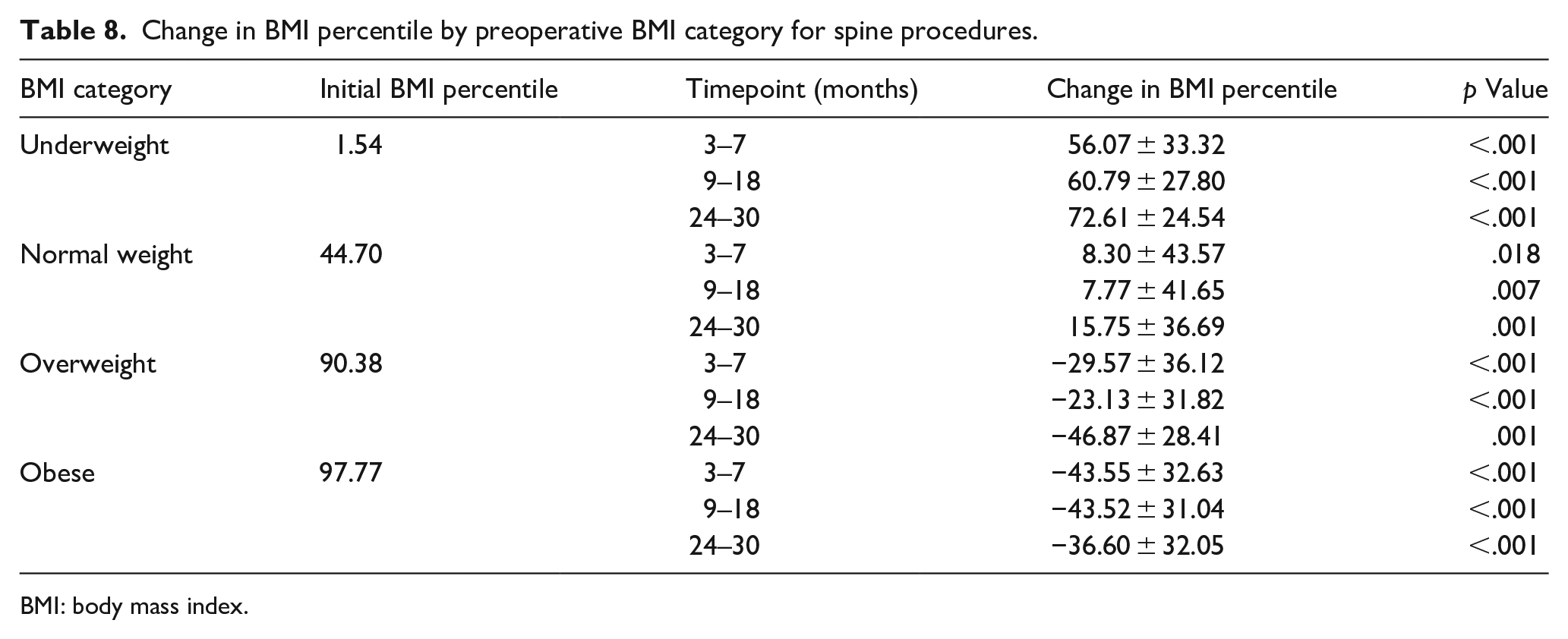
The association between preoperative BMI category and change in BMI percentile was especially significant for patients undergoing spine surgery, who experienced the largest changes, particularly at the extremes of weight (Table 8). Underweight spine patients had progressively increased BMI percentile over the course of the study; at the final follow-up, in fact, the proportion of spine patients who were underweight had decreased from 13.8% to 9.23%. Normal-weight spine patients demonstrated the same pattern of increased BMI percentile, though with changes of smaller magnitude. Mirroring the overall cohort, both overweight and obese spine patients tended to experience reductions in BMI percentile at all three timepoints, with larger decreases among the obese group. In fact, of 34 spine patients who were overweight at surgery, 20 improved to normal weight by final follow-up; similarly, 40 of 52 initially obese spine patients decreased to overweight or normal weight. However, despite these downward trends, the proportion of both overweight and obese patients among the spine cohort had increased by the final follow-up, reflecting the number of underweight and normal-weight spine patients who had become overweight or obese by the end of the study period.
Change in BMI percentile by preoperative BMI category for spine procedures.
BMI: body mass index.
Discussion
The purpose of this study was to evaluate changes in BMI percentile after orthopedic surgery in children and adolescents and, consequently, elucidate any effects that orthopedic surgeries may have on BMI in a pediatric population. To the best of our knowledge, no study has yet examined patterns of postoperative weight or BMI changes across a variety of orthopedic surgeries in this population. Of note, over one-third of patients in this cohort were overweight or obese when presenting for elective musculoskeletal surgery. We demonstrated that pediatric patients undergoing orthopedic surgery are likely to experience increases in BMI percentile postoperatively, particularly if their initial BMI is in the normal range; these changes may persist for up to 2.5 years after surgery. In addition, we observed that many patients who are overweight or obese may improve their weight category after surgery; as a group, these patients demonstrated a health-positive response with decreases in BMI percentile. While no studies thus far have explored weight gain across a broad spectrum of surgeries, a number have explored postoperative BMI percentile changes following specific orthopedic procedures or surgical categories, most notably ACL reconstruction (ACL-R) and spine surgeries.
In this study, though we found an overall upward trend in postoperative BMI percentile for patients undergoing a variety of sports-related procedures, the difference in BMI percentile between baseline and 24–30 months after surgery did not reach significance. In a retrospective review of 666 pediatric patients who underwent ACL-R, MacAlpine et al. discovered that patients experienced significantly increased BMI percentile that reached its apex at 6–9 months postoperatively; while BMI percentile on average had declined toward baseline by maximum follow-up of 2 years after surgery, it never returned to its preoperative level. 15 This pattern was consistent across normal, overweight, and obese weight categorizations, though obese patients showed the smallest increases in BMI percentile across almost all follow-up timepoints. While MacAlpine et al.’s observation of elevated BMI percentile in normal-weight patients is consistent with our study, the findings diverge for the overweight and obese subgroups, who we found had decreased BMI percentile at 24–30 months. Our observation that normal-weight sports patients are likely to have significantly increased BMI percentile 2 or more years after surgery, while overweight (but not obese) patients tend to decrease, raises interesting questions. One possible explanation is that normal-weight sports patients were accustomed to a higher level of physical activity preoperatively, and therefore the surgery resulted in a greater reduction in activity than for their overweight or obese counterparts, who may have experienced a relatively smaller impact on their activity levels. In addition, the MacAlpine study examined only patients undergoing ACL-R; the broader scope of sports patients in our study makes a direct comparison difficult. A significant limitation of both studies is a lack of data regarding preoperative and postoperative activity levels, leaving us to merely hypothesize that postoperative increases in BMI percentile may be due to reduced activity levels. However, many studies have documented persistent symptomatology and reduced rates of sports participation following injury.22,23
The finding that underweight patients with scoliosis tend to increase the weight percentile or BMI percentile following spinal fusion is consistent with the existing literature. In a retrospective study that followed 50 cerebral palsy (CP) patients with neuromuscular scoliosis (NMS) for 2 years postoperatively, DeFrancesco et al. found that those under the 50th percentile for weight relative to other CP patients tended to increase weight percentile significantly in the first year after posterior spinal fusion. 24 Similarly, a retrospective review by Baldwin et al. that followed patients with CP who underwent spinal fusion for NMS for up to 5 years postoperatively discovered that those of below-average preoperative weight increased weight percentile significantly, while those weighing above average decreased weight percentile, though the latter value did not reach significance. 25 The same trend has been demonstrated after other scoliosis procedures as well.26 –28 However, our study included only primary spinal fusions while excluding patients with NMS; to the best of our knowledge, no prior study has examined weight trends following spinal fusion in this population. In patients with adolescent idiopathic scoliosis (AIS) specifically, low BMI has been associated with poor body image and the development of eating disorders. 29 Therefore, the benefits of spinal surgery for these patients may not be limited to correction of the physical defect and enhancement of nutritional status, but may also include improvements in mental health during a critical developmental period when patients may be especially vulnerable to poor body image and low self-esteem. In addition, our observation that overweight or obese children and adolescents decrease their BMI percentile following spinal fusion has not been previously illustrated. Overall, we found a tendency for postoperative BMI percentile to trend toward normal in both underweight and overweight or obese AIS patients. While there are theoretical benefits to respiratory function and exercise capacity associated with surgical correction of scoliosis which may contribute to decreased BMI percentile in these patients, the cause of these changes remains to be elucidated.
Despite some improvements in BMI among the overweight and obese cohorts in this study, the overall pattern of increased BMI percentile is concerning considering the significant upward trend in obesity prevalence among both youth and adults in the United States over the last several decades. It is projected that, by 2030, nearly half of all American adults will be obese, with almost a quarter classified as having severe obesity.30,31 Along with the increased prevalence of childhood obesity, there has been a dramatic rise in health complications associated with excess adiposity in youth, which is likely to persist into adulthood.32,33
In recent years, many different interventions targeted toward reducing excess weight among youth have been implemented at local and national levels, with varying degrees of success.34,35 Given that this study is the first, to the best of our knowledge, to demonstrate an association between pediatric orthopedic surgery and increased postoperative BMI percentile across a broad variety of procedures, it may be premature to recommend postoperative dietary modifications to counteract unfavorable changes in weight. Nevertheless, considering that elective musculoskeletal procedures are among the most common surgeries in children, the postoperative changes we have observed illuminate yet another facet of childhood overweight and obesity that should be taken into consideration. Moreover, the finding that over one-third of patients were overweight or obese at presentation suggests that above-normal-weight classification is a risk factor for musculoskeletal pathology requiring operative correction and is another observation that warrants exploration.
This study has several limitations, including the inherent disadvantages of a retrospective design. The lack of specificity in the subject sample in reference to the procedure performed and patient pathology understandably adds a degree of heterogeneity to the study. In addition, many patients at follow-up visits did not have their height measured, precluding BMI calculation at these observations, and limiting our sample size. The shortcomings of using BMI as a proxy for body composition are well known, as BMI cannot differentiate between adiposity and muscle mass; it is possible that some patients’ elevated BMI percentile was a result of increased muscle as opposed to fat. 36 Given the complexity of caring for a patient population varying significantly in BMI, a multidisciplinary team could have been employed to offer additional insight into treatment and postoperative weight management protocols. Finally, a lack of data regarding pre- and postoperative activity levels makes it difficult to attribute the postoperative BMI percentile changes to differences in activity level versus other causes.
Overall, we demonstrate that children and adolescents undergoing orthopedic surgery may experience changes in weight or BMI postoperatively. While many patients at the extremes of weight experience improvement toward the mean, a majority may undergo BMI increases beyond what would be expected during normal growth. These findings suggest the opportunity for individualized messaging based on preoperative BMI status to assist with weight management following elective musculoskeletal surgery.
Supplemental Material
sj-docx-2-cho-10.1177_18632521231198250 – Supplemental material for Elective musculoskeletal surgery is associated with postoperative weight changes in pediatric and adolescent patients
Supplemental material, sj-docx-2-cho-10.1177_18632521231198250 for Elective musculoskeletal surgery is associated with postoperative weight changes in pediatric and adolescent patients by Sharon G Huang, Philip L Wilson, Hannah M Worrall, Brandon A Ramo, Ami Kapadia and Henry B Ellis in Journal of Children’s Orthopaedics
Supplemental Material
sj-pdf-1-cho-10.1177_18632521231198250 – Supplemental material for Elective musculoskeletal surgery is associated with postoperative weight changes in pediatric and adolescent patients
Supplemental material, sj-pdf-1-cho-10.1177_18632521231198250 for Elective musculoskeletal surgery is associated with postoperative weight changes in pediatric and adolescent patients by Sharon G Huang, Philip L Wilson, Hannah M Worrall, Brandon A Ramo, Ami Kapadia and Henry B Ellis in Journal of Children’s Orthopaedics
Footnotes
Author contributions
Sharon G. Huang, MD (Data curation; Investigation; Methodology; Visualization; Writing—original draft; Writing—review and editing)
Philip L. Wilson, MD (Conceptualization; Resources; Supervision; Writing—review and editing)
Hannah M. Worrall, MPH (Data curation; Project administration)
Brandon A. Ramo, MD (Conceptualization; Writing—review and editing)
Ami Kapadia, MD (Writing—review and editing)
Henry B. Ellis, Jr., MD (Conceptualization; Project administration; Resources; Supervision; Writing—review and editing)
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical statement
UT Southwestern Medical Center Human Research Protection Program Approval number: 2020-0531. As this was a retrospective review, informed consent is not applicable. There are no applicable grants to report.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.