
Abstract

We are glad that our paper 1 raised such interest in the correspondent to push him to write this “Letter to the editor.” We would like to respond to every point raised in the letter, some of which are really hard to understand.
First, the correspondent starts denying the milestone concept of “stress shielding.” We are aware that fragment fixation with single LAG screw is not the main clinical setting in which “stress shielding” is a concern, but it exists and it is actually relevant with bigger implants; we believe that research is also about taking little steps forward to solve bigger problems. Moreover, the correspondent shows also a lack knowledge in basic science mixing up biomechanical issues related to the stress shielding and biochemical processes causing the temporary bone resorption around magnesium (Mg) implants. We and many other authors have demonstrated that this process is circumscribed and self-limiting and that it does not interfere with fracture healing.2 –6
Biocompatible does not mean inert. Interactions between interfaces are possible at various levels. Different alloying methods have the purpose to optimize these interactions. This may not be the perfect alloying proportion, but it has demonstrated his safety and efficacy since years.
Talking about imaging appearance I wonder if the correspondent has ever seen other metal screws or even polymeric resorbable screws on MRI, and what does he think about. In fact, previous research has confirmed that magnetic resonance imaging (MRI) distortion is inferior with Mg implants than with standard ones. 7
Moreover, we cannot express on bone quality with MRI images. Those images have the only purpose to show that the area of altered signal is really circumscribed, without any sign of bone resorption around implant.
We previously reported on a case of breakage of the head of a screw that was overhanging from the bone. We clearly reported that it was an incidental finding during routinary follow-up. While the previous was a pilot study, in which recording all aspects of the follow-up, this is a comparative study, with recording of outcomes and adverse reactions. Given that the patient was completely asymptomatic, this is not included in the complications report.
There is no way a “stress fracture” can happen on the lateral column (the opposite one in relation to screw insertion), considerably far away from the zone of bone resorption, moreover during 4 weeks of continuous casting. Subtle bone impaction at time of trauma is frequent in this setting; it can lead to a periosteal reaction and may be by far the straighter explanation to an unbiased observer.
Return to preinjury level has not been investigated simply because all the patients were not high-level players; thus, differences would have been subtle and non-significant. While I agree this information could have been somehow implemented, its absence clearly does not undermine in any way the rest of the research.
Regarding the importance of anatomical fragment reduction, we are a bit confused on the correspondent’s opinion. First, he debates that the measurement made on anteroposterior (AP) and lateral (LAT) X-rays would have been inaccurate, and then he disputes the anatomical reduction of the epicondyle adopting the landmarks identified according to Klatt and Aoki, 8 that, as long as we can remember, rely on AP and LAT X-rays. Finally, he questioned the usefulness of surgical treatment “per-se,” stating that we should “expand the indications for non-operative management.”
In the end, it is impossible to understand whether a perfect anatomical reduction of the epicondyle is mandatory or not, in the correspondent opinion, given that in two different sentences, he stated opposite things, taking both of them for granted. We are glad to include images with measurement according to Klatt and Aoki, showing the precise AP anatomical reduction and the 2–3 mm displaced medial epicondyle on lateral views to which the correspondent probably refers (Figures 1–3).
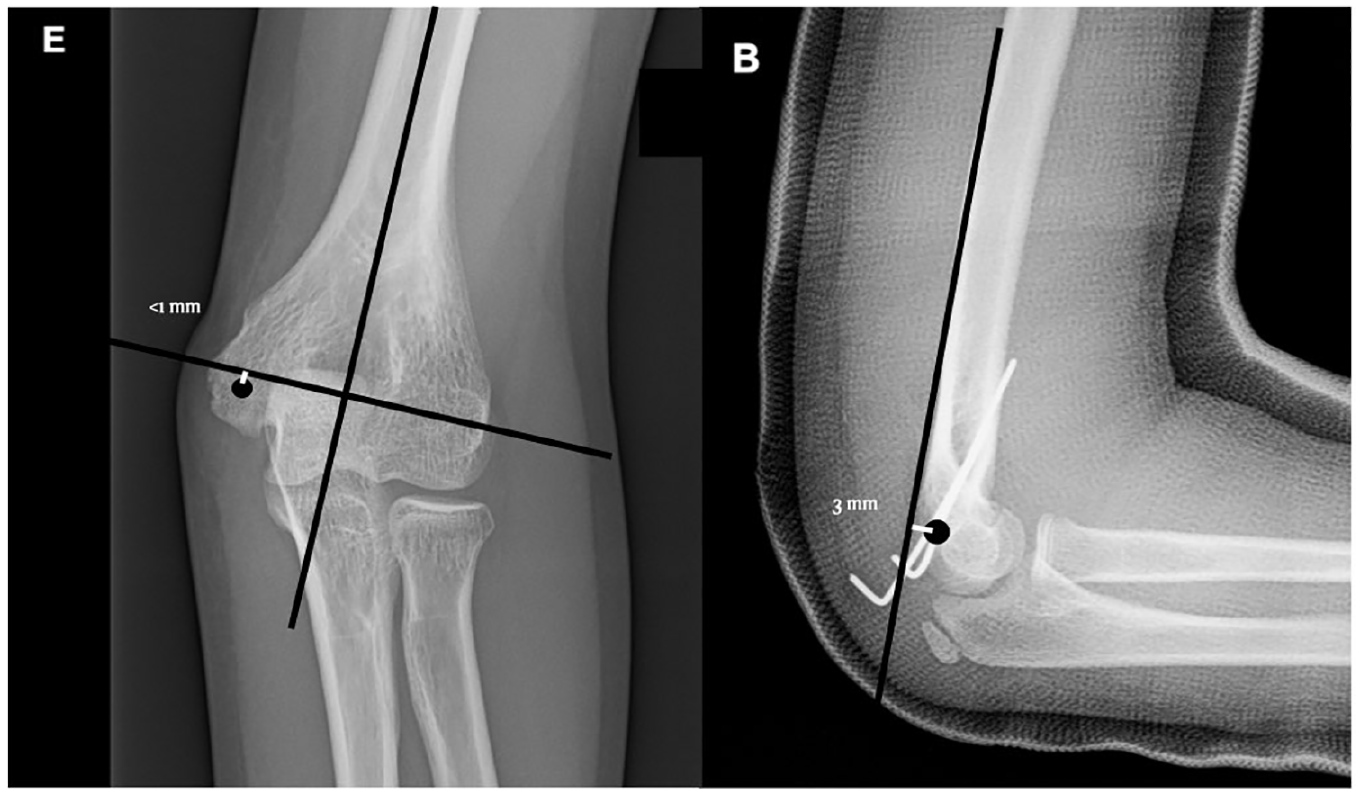
Neglectable anteroposterior and lateral displacement from reference point in the reference case of k-wire ORIF, according to Klatt and Aoki. 8
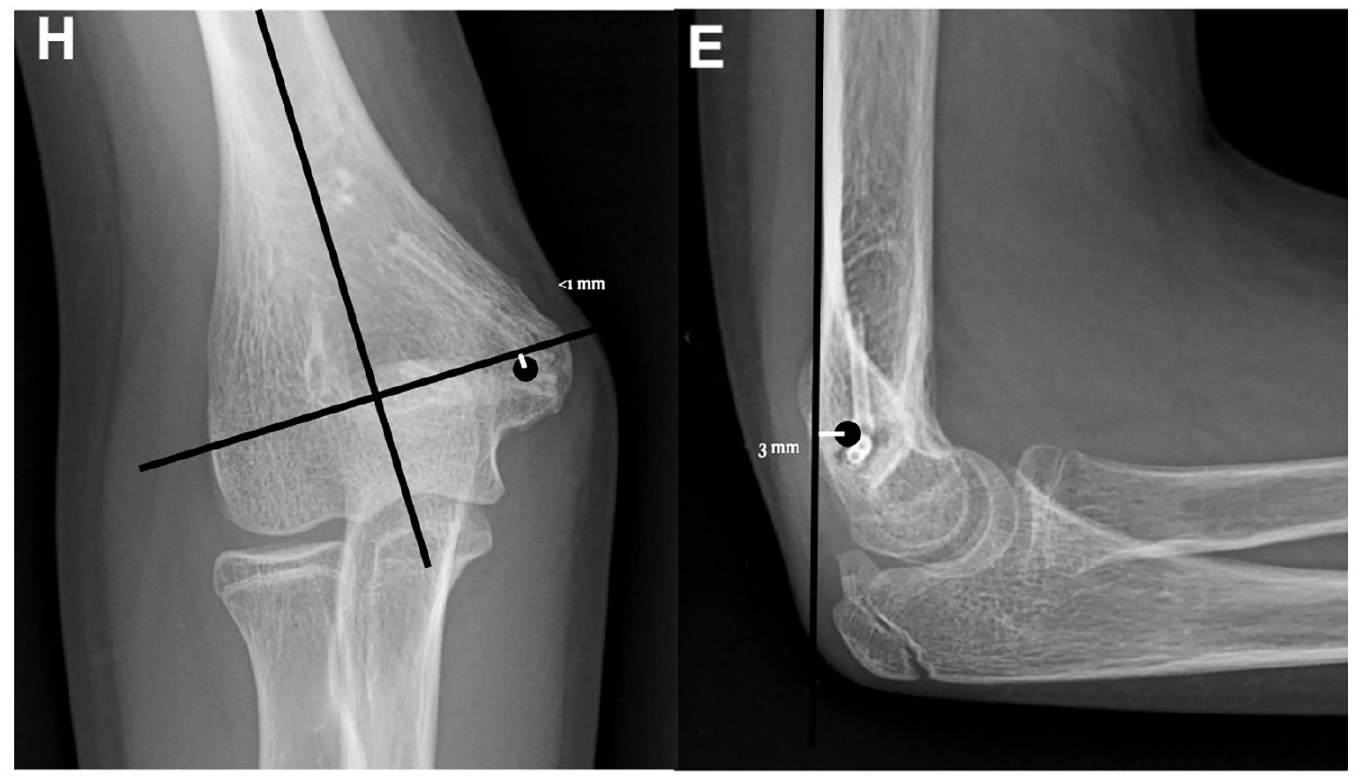
Neglectable anteroposterior and lateral displacement from reference point in the reference case of Mg screws ORIF, according to Klatt and Aoki. 8
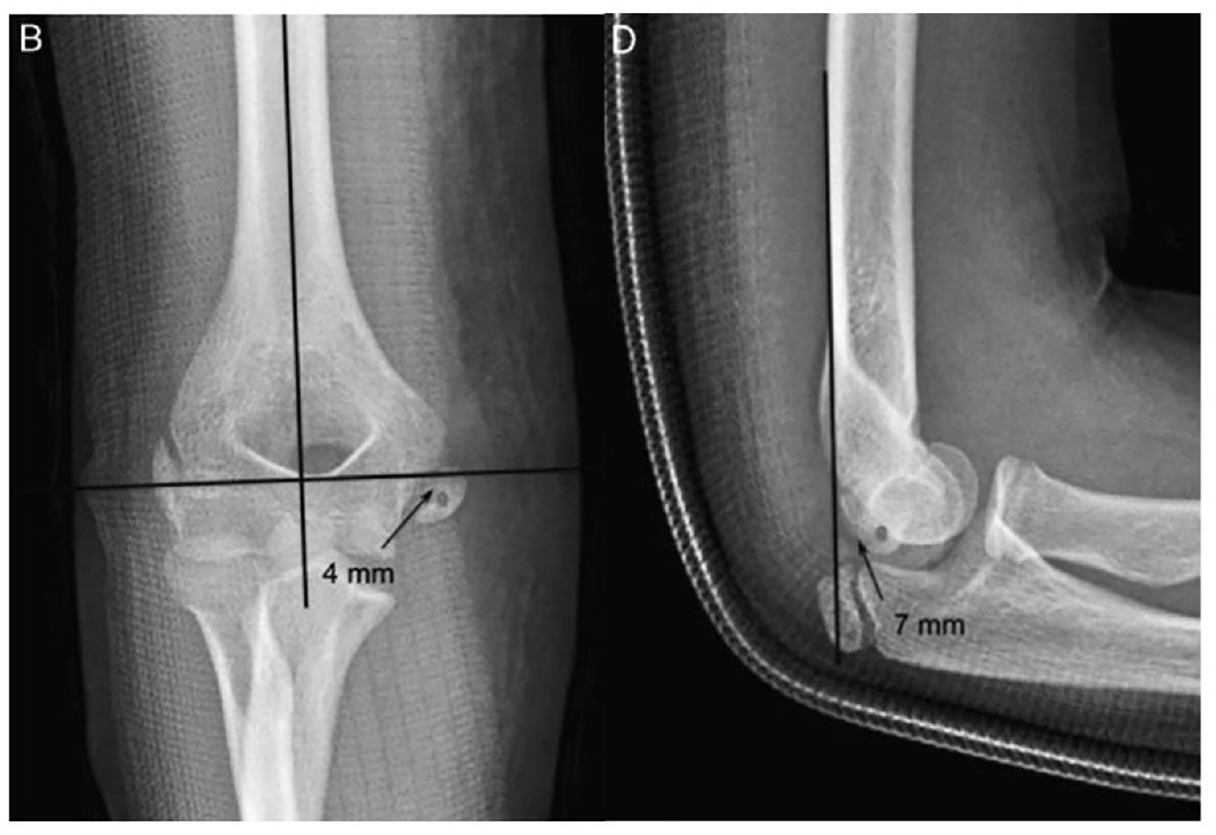
Original image from Klatt and Aoki 8 showing a case with moderate anterior displacement, on lateral view, and mild inferior displacement, on anteroposterior view.
According to Klatt and Aoki, 8 the center of the epicondyle is between 0 and 3 mm anterior from the posterior cortical reference line, in 94% of normal elbows in children. Admitting that such a small displacement from anatomic position would worsen outcomes and at the same time stating that we should overcome the “5-mm displacement rule” to expand conservative treatment is pure sophism, revealing at least the hint of bad faith of the correspondent in his pursuit against our paper. Noteworthy, Klatt and Aoki reported an interobserver disagreement rate of 54% and intraobserver disagreement of 26% when considering a 2-mm difference in measurement, thus questioning the reliability and reproducibility itself of the method.
Finally, the cherry on top: “Stainless steel screws do not need to be removed unless they cause localized symptoms or in young patients to preserve physeal growth.” Implant removal due to patient complaint reaches rates higher than 40% in medial epicondyle open reduction and internal fixation (ORIF) with screws. 9
Moreover, I would like to acknowledge the correspondent that this paper is actually talking about “young patients” if this was not clear enough. Thus, we are grateful to the correspondent that, with this sentence, clearly endorses the rationale of our research. Our group has no conflict of interest at all, and we have no prejudice on one treatment over another.
Preclinical evidence, our previous published systematic review, 2 and our clinical practice have persuaded us that this may represent a valid tool in our box, in specific situation. This knowledge is worth sharing with the scientific community. We are committed to respond to criticism on methodological issues and we know that our paper has its limitations, but we hardly understand the prejudicial livor of some colleagues against this potentially helpful new technology. 10
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.