
Abstract
Introduction:
In situ pinning is an accepted treatment for stable slipped capital femoral epiphysis. However, residual deformity of severe slipped capital femoral epiphysis can cause femoroacetabular impingement and forced external rotation.
Purpose/questions:
The aim of this study was to evaluate the (1) hip external rotation and internal rotation in flexion, (2) hip impingement location, and (3) impingement frequency in early flexion in severe slipped capital femoral epiphysis patients after in situ pinning using three-dimensional computed tomography.
Patients and methods:
A retrospective Institutional Review Board-approved study evaluating 22 patients (26 hips) with severe slipped capital femoral epiphysis (slip angle > 60°) using postoperative three-dimensional computed tomography after in situ pinning was performed. Mean age at slipped capital femoral epiphysis diagnosis was 13 ± 2 years (58% male, four patients bilateral, 23% unstable, 85% chronic). Patients were compared to contralateral asymptomatic hips (15 hips) with unilateral slipped capital femoral epiphysis (control group). Pelvic three-dimensional computed tomography after in situ pinning was used to generate three-dimensional models. Specific software was used to determine range of motion and impingement location (equidistant method). And 22 hips (85%) underwent subsequent surgery.
Results:
(1) Severe slipped capital femoral epiphysis patients had significantly (p < 0.001) decreased hip flexion (43 ± 40°) and internal rotation in 90° of flexion (−16 ± 21°, IRF-90°) compared to control group (122 ± 9° and 36 ± 11°). (2) Femoral impingement in maximal flexion was located anterior to anterior–superior (27% on 3 o’clock and 27% on 1 o’clock) of severe slipped capital femoral epiphysis patients and located anterior to anterior–inferior (38% on 3 o’clock and 35% on 4 o’clock) in IRF-90°. (3) However, 21 hips (81%) had flexion < 90° and 22 hips (85%) had < 10° of IRF-90° due to hip impingement and 21 hips (81%) had forced external rotation in 90° of flexion (< 0° of IRF-90°).
Conclusion:
After in situ pinning, patient-specific three-dimensional models showed restricted flexion and IRF-90° and forced external rotation in 90° of flexion due to early hip impingement and residual deformity in most of the severe slipped capital femoral epiphysis patients. This could help to plan subsequent hip preservation surgery, such as hip arthroscopy or femoral (derotation) osteotomy.
Keywords
Article summary
Article focus
Research questions addressed are as follows:
Hip flexion and internal rotation (IR), and forced external rotation (ER);
Impingement location;
Impingement frequency in early flexion in severe SCFE patients after in situ pinning.
Key messages
Restricted flexion and IR in 90° of flexion due to early hip impingement;
Most of the severe SCFE patients had restricted flexion < 90° and had < 10° of IR in 90° of flexion and forced ER in 90° of flexion due to impingement;
Proportion of anterior hip impingement in early flexion was high for severe SCFE patients after in situ pinning.
Strengths and limitations of this study
Strength: 3D-CT scan for 3D models, and standardized and validated method for range of motion and impingement simulation.
Limitation: Bone-to-bone contact for collision detection and small sample size.
Introduction
Slipped capital femoral epiphysis (SCFE) is a frequent hip disorder in adolescent patients with a high risk of disability. 1 In situ pinning is the conventional treatment for a stable SCFE. 2 In situ pinning provides stabilization of the growth plate followed by epiphysiodesis, and this treatment was associated with good Iowa hip outcome scores at long-term follow-up.3,4 However, this is different for hips with severe SCFE and the long-term hip outcome scores are lower, and radiographic progression to osteoarthritis is more prevalent than those with mild deformity.4 –6 Although the deformity of the proximal femur may remodel after SCFE, the remodeling process occurs through impingement of the femur against the acetabular rim.7 –9 SCFE-related femoroacetabular impingement (FAI) due to post-slip deformity can lead to acetabular cartilage defect, hip pain, limited motion, and ultimately to hip osteoarthritis.5,10 –16
The concept of SCFE-related FAI is not new.17,18 In 1999, Rab 18 used a computerized 3D volume/surface model to describe the FAI secondary to SCFE as two different mechanisms: impaction and inclusion. On the one hand, impaction refers to metaphyseal impingement of the metaphysis against the acetabular labrum limiting the range of hip motion and leading to erosion of the acetabular labrum. On the other hand, inclusion happens once the remodeled metaphyseal bump falls into the acetabulum and is associated with a high potential for erosion of the acetabular cartilage. Rab 18 showed that relevant alterations in hip motion were necessary to compensate for the SCFE deformity. 18 While little external rotation (ER) was needed to avoid metaphyseal impingement for a mild slip, more ER was needed with moderate and severe slips. A previous study of 23 patients simulated hip osteotomy and reported that the limitation of range of motion (ROM) was associated with the severity of the SCFE using computed tomography (CT). 19 In addition, mild SCFE exhibited inclusion impingement, but for severe cases, the impaction impingement was the dominant mechanism due to the abutment of the prominent metaphysis on the acetabular rim. Another study using a 3D geometric model of acute SCFE deformity of one normal adolescent hip found that impingement occurred in all moderate and severe deformities, and it was noted anterosuperiorly on the acetabular rim. 20 Recently, patient-specific CT-based bony 3D models were used for dynamic simulation of hip ROM and were applied to patients with FAI, 21 abnormal femoral torsion, 22 and Legg–Calve–Perthes disease. 23
In this study, we sought to improve our understanding about the mechanism of FAI in severe SCFE patients treated with in situ pinning with a single cannulated screw. The specific aims of our study were (1) to determine postoperative hip ROM in external and internal rotation (IR) in flexion, (2) to identify the specific areas of femoral and acetabular impingement, and (3) to calculate the proportion of hips with impingement in early flexion using the patient-specific 3D-CT models after treatment with in situ pinning and comparing them to the contralateral uninvolved hip as controls.
Patients and methods
Study design and population
This is a retrospective Institutional Review Board (IRB)-approved study. We searched our tertiary pediatric hospital database to identify patients treated for SCFE between 2000 and 2018. Patients between 8 and 15 years of age who had a postoperative CT scan (Figure 1) of the pelvis that included the femoral condyles after in situ pinning were included. The indications for acquiring a CT during the study period included an assessment of the residual symptomatic deformity, planning for the surgical treatment, and deciding whether to conduct a subcapital realignment or other procedures, such as osteoplasty or intertrochanteric osteotomy. The epiphysis-diaphysis angle, according to Southwick, 24 was measured on the preoperative lateral radiographs to classify SCFE as mild (<30°), moderate (30°–60°), or severe (>60°). We excluded patients with mild (slip angle < 30°) and moderate SCFE (slip angle 30°–60°), patients with only preoperative CT available (no previous treatment performed), and inadequate CT images (e.g. CT of unilateral hip joint or missing femoral condyles). Of 123 patients with SCFE and CT imaging available, 101 patients were excluded, yielding the final cohort of 22 patients with severe SCFE treated with in situ pinning with postoperative pelvic CT image that included the femoral condyles. There were 15 male patients (58%), with a mean age of 13 ± 2 years at the time of SCFE diagnosis and 14 ± 3 years at the CT scan (Table 1). Four patients (15%) had bilateral SCFE, yielding 26 hips included in the analysis. Out of the 26 hips with severe SCFE, 22 (85%) were chronic, and 20 (67%) were stable. Surgery was performed for 22 hips (85%) after the CT scan. The contralateral hips of 15 patients with unilateral SCFE of a previous study 25 were used as a control group.
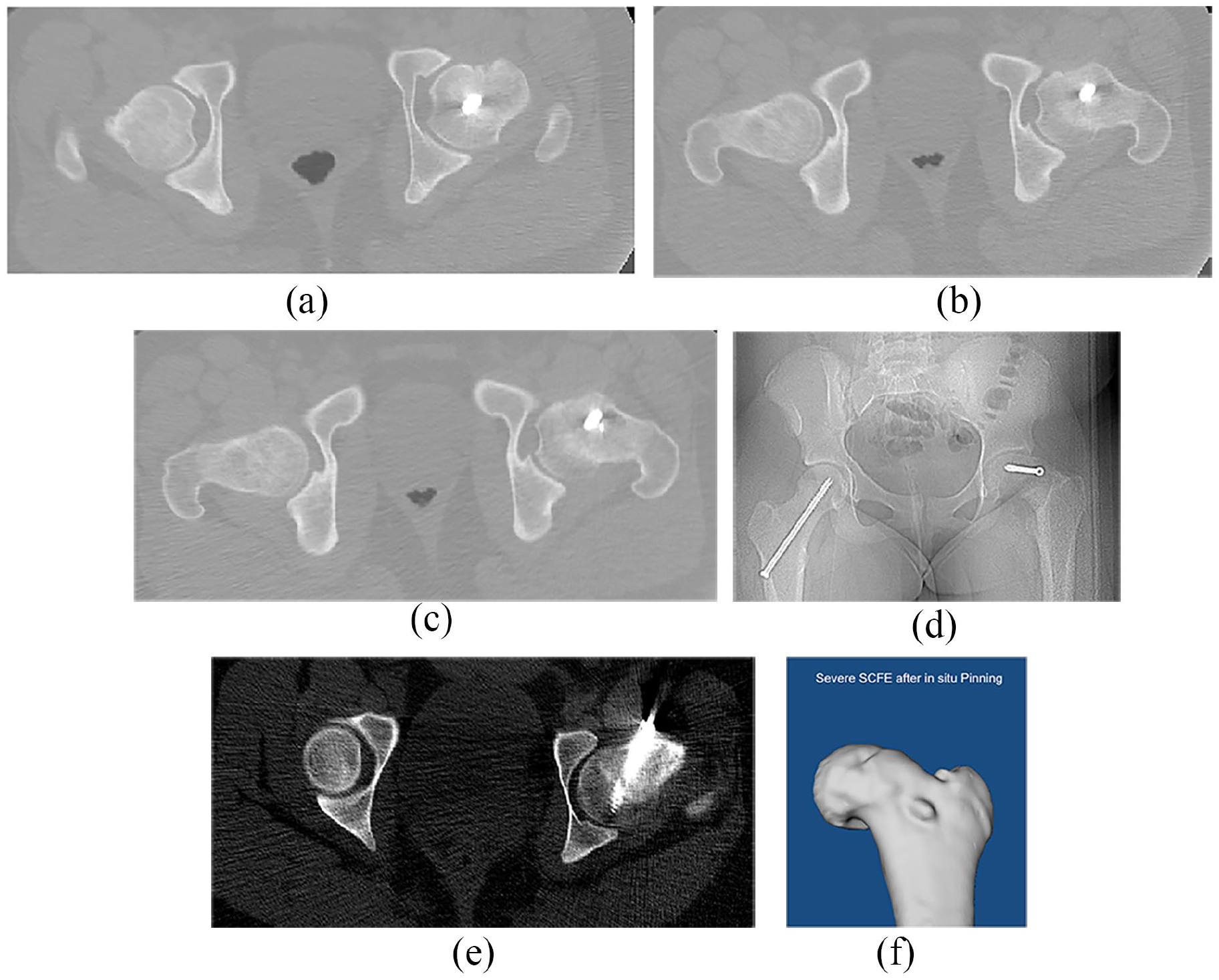
(a–f) Pelvic CT scan of a patient with severe SCFE treated with in situ pinning (a-c). Anteroposterior (AP) pelvis radiograph (d) and corresponding pelvic CT scan (e) of a second patient with severe SCFE treated with in situ pinning. Femoral CT-based 3D model of another patient with severe SCFE after previous in situ pinning (f).
Demographic information of the patient series.
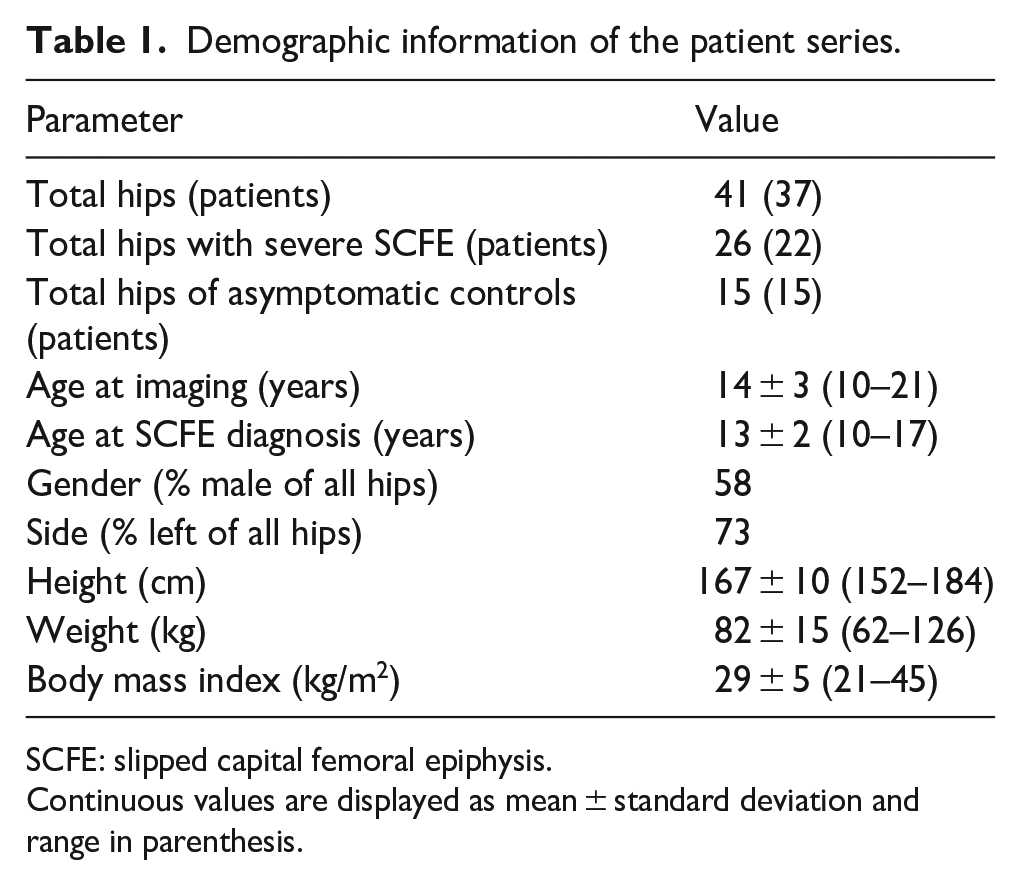
SCFE: slipped capital femoral epiphysis.
Continuous values are displayed as mean ± standard deviation and range in parenthesis.
Imaging and 3D impingement simulation
All patients underwent standardized anteroposterior (AP) and frog-leg or cross-table lateral radiographs and CT of the pelvis (Figure 1), including the distal femoral condyles. Mean femoral anteversion was −7°, minimal femoral anteversion was −36° (femoral retroversion), and maximum was 61°. Femoral anteversion was measured according to the Murphy method. Overall, 11 (42%) hips had absolute femoral retroversion < 0°. An osseous 3D model of the proximal femur and the pelvis (Figure 1(f)) of every patient was generated using the software Amira (Visage Imaging Inc, Carlsbad, CA, USA). Threshold-based bone segmentation was performed by two independent observers (TDL and AB). The two observers were independent and were not the treating physicians of the patients. The acetabular reference coordinate system was the modified anterior pelvic plane (APP), a virtual plane formed by the pubic tubercles and the inferior iliac spines (Supplemental Table 1) and a tilt angle of 20° as previously described. 21 The femoral reference coordinate system was defined by the knee center, both femoral condyles and the center of the femoral head. 26
Specific collision detection software was used for 3D impingement simulation to determine the degree of impingement-free hip flexion (Figure 2(a)) and IR with the hip in 90° of flexion (Figure 2(b)) in severe SCFE hips after in situ pinning and control hips. The amount of necessary ER in 90° of flexion (Figure 2(c)) was calculated for severe SCFE patients. The details and algorithms of the used software were described in previous studies and are based on the equidistant method and are listed in Supplemental Table 1. The impingement location was analyzed for every patient individually. The impingement location was assessed in a standardized manner with a clockface system that was also used intraoperatively: inferior was defined 6 o’clock and represents the acetabular notch on the acetabular side; 3 o’clock represents anterior (for both right and left hips), as per Tannast et al.’s study. 23 To calculate the proportion of hips with impingement in pure flexion without rotation, impingement was recorded in 10° increments between 60° and 90° of flexion. The proportion of hips with impingement at each given hip flexion was recorded and compared to control group. All patients were evaluated with the equidistant method using personalized CT-based 3D bone models and validated collision detection software. 27 Based on a cadaveric investigation, the impingement collision can be detected with a mean accuracy of 2.6° ± 2.5°. 27 The intra- and interobserver measurements for this software for IR in 90° of flexion and for flexion were excellent (> 0.9) 21 in a validation study.
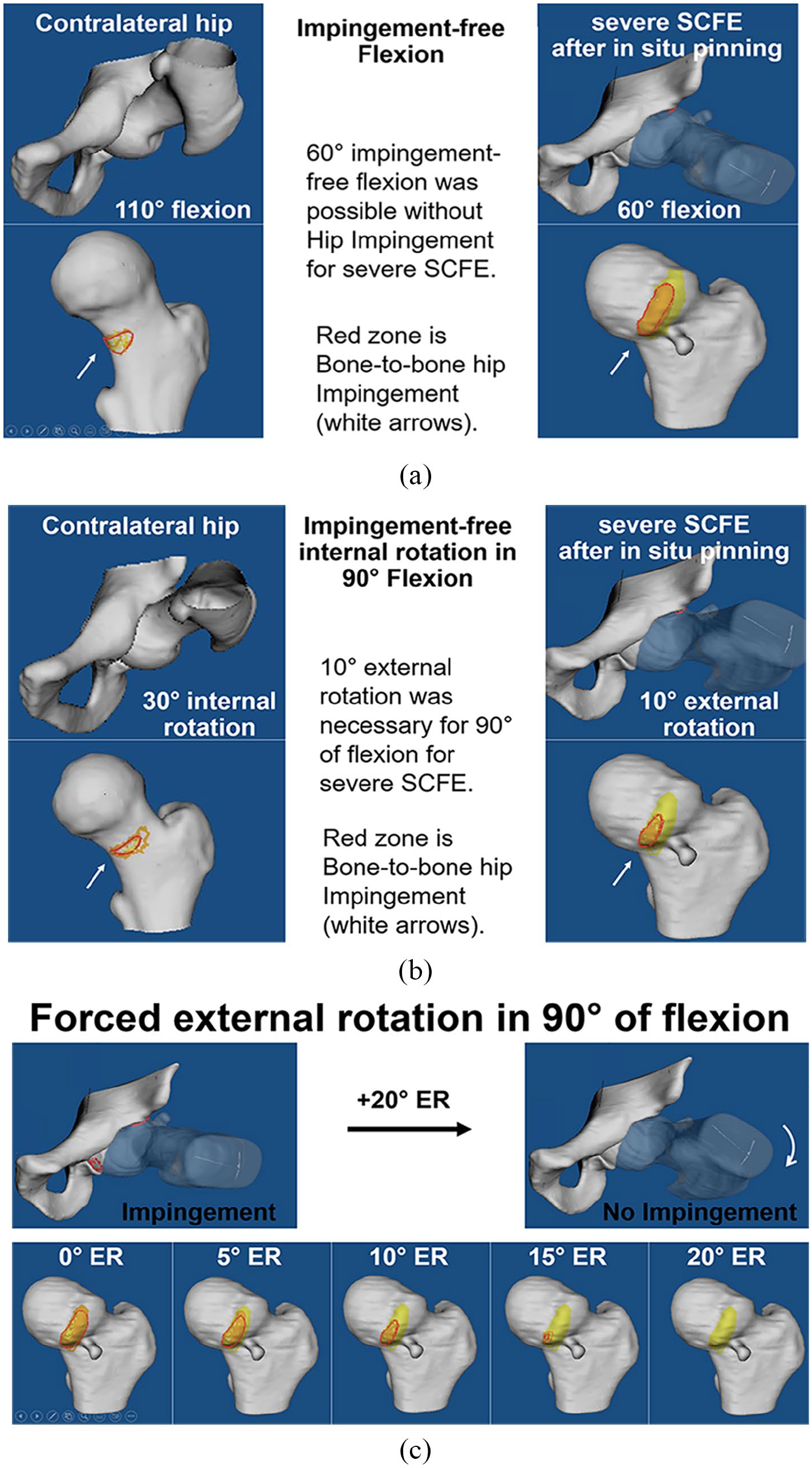
(a) CT-based 3D models of a patient with severe SCFE after previous in situ pinning is shown in impingement-free flexion. (b) Impingement-free simulation of 90° flexion was performed and (c) impingement-free 90° of flexion was achieved with 16° of external rotation.
Statistical analysis
Statistical analysis was performed using Winstat software (R. Fitch Software, Bad Krozingen, Germany). The data were assessed for normal distribution with the Kolmogorov–Smirnov test. Because not all the parameters were normally distributed, we used nonparametric tests for comparison. To compare demographic and radiographic data, ROM, or location of impingement, we used the Mann–Whitney U test. The chi-square test was used to compare the frequency of impingement at different degrees of hip flexion.
Results
Mean flexion was significantly (p < 0.001) decreased in hips with severe SCFE after in situ pinning (43° ± 40°, range −20° to 120°) compared with uninvolved contralateral hips (122° ± 9°, range 107° to 138°, Figure 2(a)). Similarly, mean IR with the hip in 90° of flexion was significantly (p < 0.001) decreased in severe SCFE patients treated with in situ pinning (−16° ± 21°, range −55° to 35°) compared to the control group (36° ± 11°, range 21°–55°, Figure 2(b)). The −16° of IR with the hip in 90° flexion represent the forced ER in 90° of flexion (Figure 2(c)).
In maximum hip flexion, the impingement zones on the femur were located more anterosuperior (between the 1 and 3 o’clock) in the hips with severe SCFE after in situ pinning compared (p < 0.001) to the uninvolved contralateral group (5 o’clock). (Figure 3(a)) Impingement in maximum hip flexion was similarly concentrated on the acetabular 2 o’clock zone for hips with severe SCFE after in situ pinning (69%) and the control hips (93%) (Figure 3(b)).
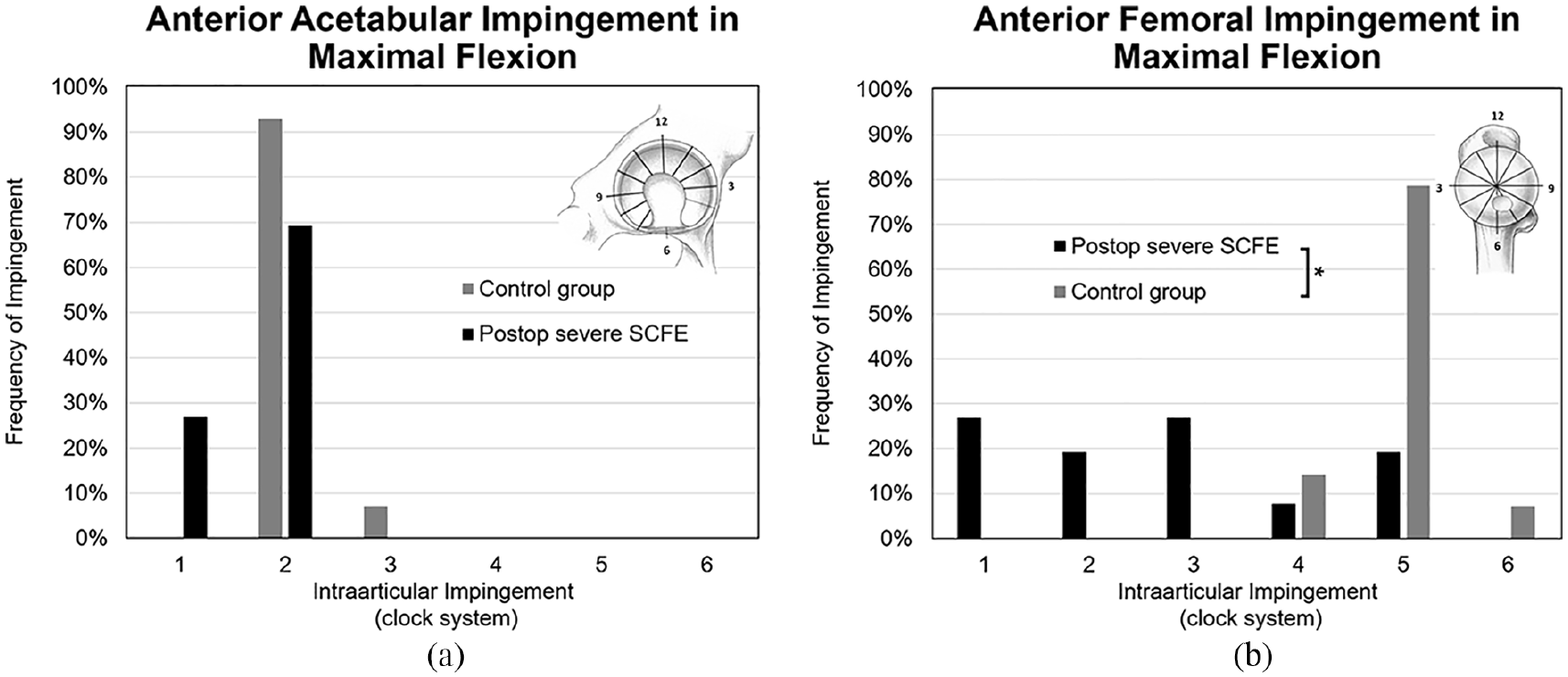
(a) Acetabular and (b) femoral impingement location is shown in maximal flexion using a patient-specific osseous CT-based 3D model of a patient with severe SCFE after previous in situ pinning.
In maximum IR with the hip in 90° of flexion, the femoral location of impingement differed significantly (p < 0.001) between hips with severe SCFE after in situ pinning and uninvolved contralateral hips. (Figure 4(a)) The impingement location on the acetabulum was more superior (between 12 and 2 o’clock) in hips with severe SCFE after in situ pinning compared (p < 0.001) to the control group (2 o’clock) (Figure 4(b)).
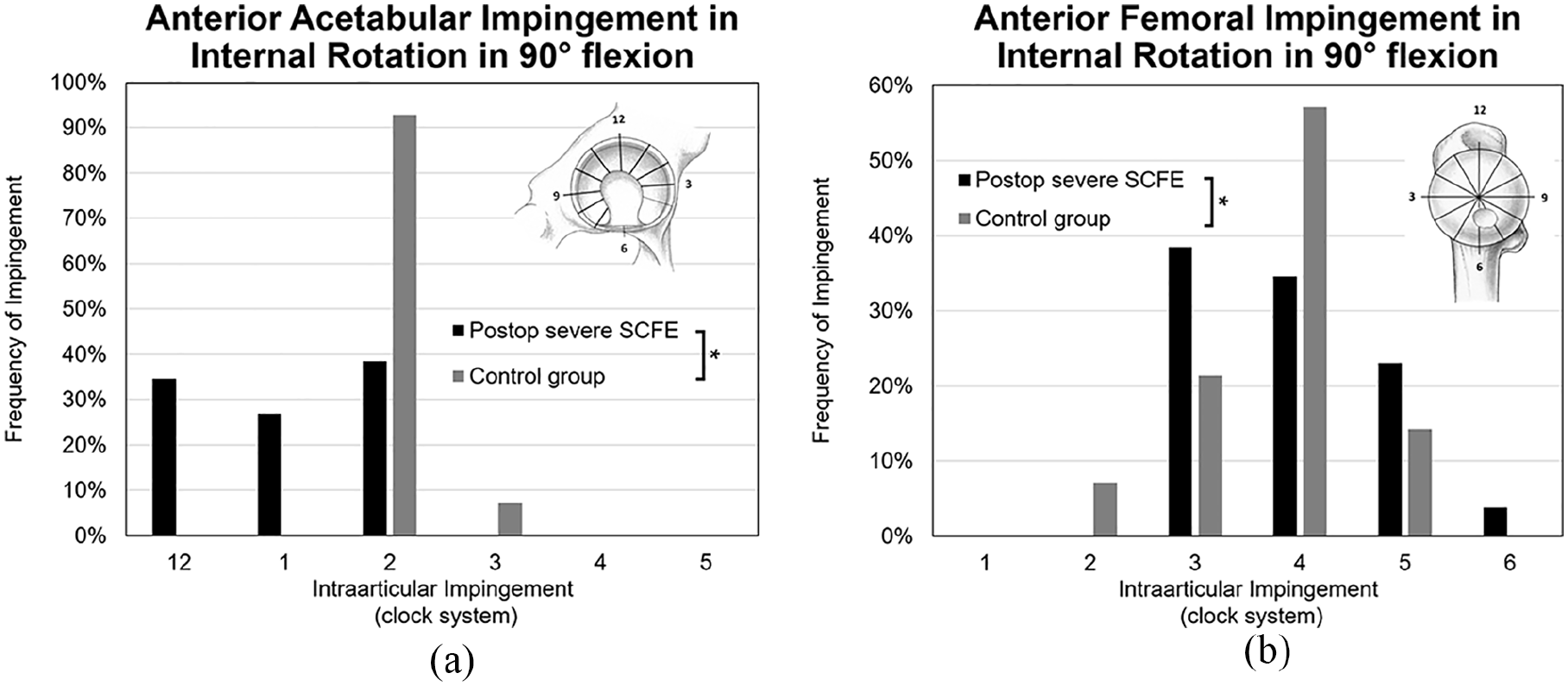
Acetabular (a) and femoral (b) impingement location is shown in maximal internal rotation with the hip in 90° of flexion using a patient-specific osseous CT-based 3D model of a patient with severe SCFE after previous in situ pinning.
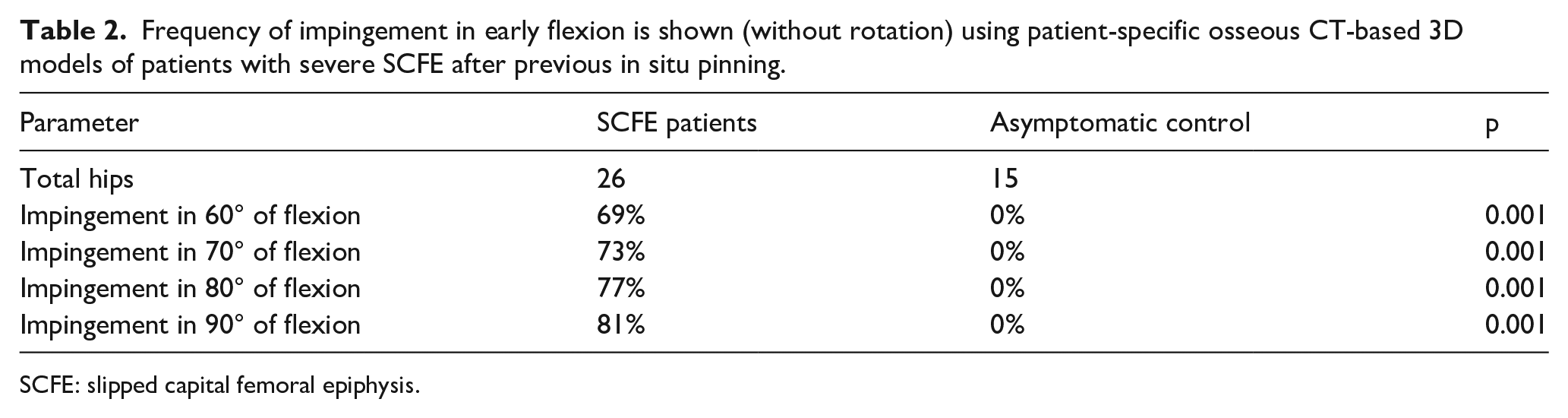
Regarding the third aim of this study, no uninvolved contralateral hip showed impingement with flexion from 60° to 90°. The proportion of hips with detected impingement with pure flexion (no rotation) increased with increasing degrees of hip flexion of severe SCFE patients after in situ pinning. A significantly higher proportion (p < 0.001) of severe SCFE hips after in situ pinning showed impingement in flexion from 60° to 90° (Table 2) compared to the control group.
Frequency of impingement in early flexion is shown (without rotation) using patient-specific osseous CT-based 3D models of patients with severe SCFE after previous in situ pinning.
SCFE: slipped capital femoral epiphysis.
Discussion
The residual deformity of the proximal femur after in situ pinning for severe SCFE may partially remodel through impaction or inclusion impingement between the metaphyseal bump and the acetabular rim.8,18 However, impingement after severe SCFE is known to cause articular cartilage damage and is associated with long-term osteoarthritis.3 –5,11,28 In this study, we used postoperative CT images to create 3D models of patients with severe SCFE after in situ pinning to better understand the pathomechanics of FAI by measuring the impingement-free hip motion and assessing the specific location of impingement on the femur and acetabulum compared to the uninvolved contralateral hip.
We found that IR with the hip in 90° of flexion and mean hip flexion were significantly decreased in hips with severe SCFE following in situ pinning compared to the normal hips. Mamisch et al. 29 simulated hip motion in 31 patients with SCFE who had CT imaging before surgical treatment and found that although for mild SCFE, the hip motion was comparable to the unaffected side, for severe SCFE, there was near complete loss of normal motion. They found lower motion in flexion (4.4° ± 12.4°) but higher measurements of IR (8.4° ± 26.2°) compared to the current study reporting mean of 43°± 40° flexion and mean IR with the hip in 90° of flexion of −16° ± 21°. Another study 19 performed simulations with different proximal femoral osteotomies and investigated ROM after SCFE using a specific software and CT image of 19 patients with moderate and severe SCFE. Again here, that study showed lower mean flexion (4° ± 13°) but higher IR (8° ± 23°) compared to the results of the current study. The slight discrepancy between ours and previous studies findings may be related to the software used in those studies but also to the fact that hips with severe SCFE do not have a homogeneous deformity. Rather, the location of the epiphysis in relation to the metaphysis varies in hips with severe SCFE and is influenced by the remodeling process. Jones et al. 30 classified hips based on the anterior head and neck profile and showed that hips that failed to remodel the anterior head-neck had decreased range of IR compared to hips that remodel. Mamisch et al. 29 noted that the Jones type 3 deformity (the femoral epiphysis is positioned dorsal in relation to the metaphysis) is associated with impaction type of impingement and severely decreased hip flexion and IR compared to type 2 Jones deformity (epiphysis and metaphysis are on the same level in ventral direction).
In this study, the location of impingement zones on the femur with hip flexion was more anterosuperior in the hips with severe SCFE after in situ pinning compared to the uninvolved contralateral group. With IR in 90° hip flexion, the impingement zones on the acetabulum were located more superiorly (between 12 and 2 o’clock, Figure 4) in hips with severe SCFE. There is limited literature analyzing the location of the impingement in hips with SCFE. Recent studies have used patient-specific 3D models to analyze the slip direction 31 and for 3D printing 32 to simulate corrective surgery. Femoral and acetabular osseous impingement locations have been reported for hips with cam and pincer FAI. 23 However, specifically to severe SCFE, few studies investigated individual hip impingement location in IR and flexion. A study reporting intraoperative evaluation of articular cartilage damage in patients undergoing surgical treatment for symptomatic FAI post-SCFE has described the location of damage in the anterior–superior acetabulum. This is consistent with the results of acetabular impingement location (Figures 3 and 4) found in the current study, and it provides a biomechanical explanation for the previously reported acetabular cartilage damage.
The proportion of hips with severe SCFE after in situ pinning with detected impingement with pure flexion (no rotation) increased with increasing degrees of hip flexion. It is well accepted that patients with severe SCFE walk with an outward rotation of the lower extremity and to flex the hip, it is mandatory that the hip rotates externally – the so-called Drehmann 33 sign. The found results in the current study of −16° of IR in 90° of flexion represents 16° of forced ER. Our findings are in line with Kamegaya et al.’s 34 study that investigated 80 SCFE patients (92 hips) treated with in situ pinning and noted that 25% of hips with Jones type A deformity, 75% of hips with Jones type B, and 100% with hips with Jones type C exhibited the Drehmann sign. The authors assessed three patients with a dynamic 3D-CT during testing for Drehmann sign and noted a direct contact between the femoral metaphysis and the acetabulum as early as in 30° of flexion. With additional flexion (at 70° of flexion), the location of impingement changed as the femur rotated externally. We believe that the limited impingement-free range of hip flexion in hips with severe SCFE may be an essential component to the disfunction often observed in these patients. Notably, Kamegaya et al. reported after a mean 12-year-follow up that 7 (25%) of the 28 patients with a positive Drehmann sign reported pain or limp, while patients with a negative Drehmann sign reported no pain.
Our results showed that hips with severe SCFE exhibit severe limitation of hip motion and a high proportion of anterior impingement with simple hip flexion after in situ pinning. However, this treatment purely does not alter the problem acutely. In severe SCFE, complete resolution of impingement would require either an intertrochanteric osteotomy,35–37 a subcapital realignment through a modified Dunn 38 or a combined approach using the surgical hip dislocation with a femoral osteotomy. 39 However, these procedures may be associated with surgical complications, and because of the stabilization and the good short-term outcomes of SCFE patients after in situ fixation,3,4 most pediatric orthopedic surgeons prefer to treat severe SCFE with percutaneous pinning. We believe that, in the setting of limited hip motion and with an obligatory ER test (Drehmann sign), patients with severe SCFE should be counseled for repetitive follow-up examinations to monitor for the development of symptoms and radiographic signs of osteoarthritis. Independent of the planned surgical treatment for symptomatic FAI in patients with previously pinned severe SCFE, the severe limitations of hip motion due to early hip impingement and the location of impingement described in our study should be considered for preoperative planning.
This study has limitations. First, the software for collision detection calculates the osseous ROM, without considering soft tissue (labrum, muscles, or cartilage). This is unavoidable using pelvic CT scans for 3D modeling and could be integrated using MR in the future. It is possible that the clinical ROM for SCFE patients could be decreased. In addition, pelvic CT scans have a considerable radiation exposure, especially for young patients. Low-dose CT scans or MR could be used to reduce radiation exposure in the future. Unfortunately, clinical ROM could not be assessed for all patients in the current study due to hip pain and the retrospective nature of the chart review. In addition, the used asymptomatic control group of a previous study does not necessarily have a “normal” hip joint because of the theoretical risk of a contralateral slip. Patients analyzed in this study were from a pediatric university center in Boston, USA with limited generalizability and potential selection bias for referred patients. No detailed patient-related hip outcome scores or clinical examinations were evaluated because this was not the aim of this study. Hip pain was reported by all patients at the time of CT acquisition and 85% of them underwent subsequent hip preservation surgery. Finally, we did not evaluate the effect of other anatomic parameters, including pelvic tilt, and acetabular and pelvic morphology, which could also affect hip ROM.
Conclusion
Patient-specific 3D bone models of severe SCFE patients showed restricted flexion and IR of the hip at 90° of flexion and a high proportion of forced ER in 90° of flexion and a high frequency of impingement with isolated hip flexion after in situ pinning. This study also describes the specific location of impingement in hips with severe SCFE after in situ pinning. Patient-specific 3D models of hips with severe SCFE may facilitate standardized diagnosis and surgical planning for a hip preservation surgery that can stabilize the slip and treat the impingement, avoiding additional damage to the acetabular cartilage and hopefully preventing the development of osteoarthritis. However, future investigations will be needed to investigate whether patient-specific designed corrections are safe and impact treatment outcomes in patients with severe SCFE deformity.
Supplemental Material
sj-docx-1-cho-10.1177_18632521231192462 – Supplemental material for Hip Impingement of severe SCFE patients after in situ pinning causes decreased flexion and forced external rotation in flexion on 3D-CT
Supplemental material, sj-docx-1-cho-10.1177_18632521231192462 for Hip Impingement of severe SCFE patients after in situ pinning causes decreased flexion and forced external rotation in flexion on 3D-CT by Till D Lerch, Young-Jo Kim, Ata Kiapour, Adam Boschung, Simon D Steppacher, Moritz Tannast, Klaus A Siebenrock and Eduardo N Novais in Journal of Children’s Orthopaedics
Supplemental Material
sj-pdf-2-cho-10.1177_18632521231192462 – Supplemental material for Hip Impingement of severe SCFE patients after in situ pinning causes decreased flexion and forced external rotation in flexion on 3D-CT
Supplemental material, sj-pdf-2-cho-10.1177_18632521231192462 for Hip Impingement of severe SCFE patients after in situ pinning causes decreased flexion and forced external rotation in flexion on 3D-CT by Till D Lerch, Young-Jo Kim, Ata Kiapour, Adam Boschung, Simon D Steppacher, Moritz Tannast, Klaus A Siebenrock and Eduardo N Novais in Journal of Children’s Orthopaedics
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
Each author certifies that his or her institution approved the human protocol for this investigation, that all investigations were conducted in conformity with ethical principles of research, and that informed consent for participation in the study was obtained.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: T.D.L. has received funding from the Swiss National Science Foundation (Early Postdoc.Mobility P2BEP3_195241).
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.