
Abstract
Purpose:
The migration percentage is a widely used criterion for surgery in displaced hips. Literature suggests that no hip can spontaneously improve if the migration percentage exceeds 45%, in a mixed population of cerebral palsy children. The aim of the present article was to identify the point of no return of the migration percentage in a selected sample of non-ambulatory cerebral palsy children, being the most exposed to hip luxation.
Methods:
This single-center retrospective cohort study included patients with spastic or dyskinetic cerebral palsy, Gross Motor Function Classification System level IV or V, age 0–18, having at least three pelvic radiographies, excluding radiographies relative to hips having previously undergone surgery. The following information was collected: sex, cerebral palsy subtype, Gross Motor Function Classification System level, presence of drug-resistant epilepsy, migration percentage, age at assessment, use of walking or standing assistive devices, previous botulinum injection, oral or intrathecal baclofen, and hip pain. Data were analyzed at the level of the individual hips. Descriptive statistics were presented. Receiver operating characteristic curve analysis was conducted to investigate which value of the migration percentage could be adopted as the “point of no return”: that is, the cutoff value beyond which no migration percentage reduction, by more than 5%, could be expected.
Results:
The optimal cutoff value was identified as migration percentage ≥50%, with a sensitivity of 84.5% and a specificity of 100% (p-value <0.001).
Conclusion:
Based on the present study, migration percentage ≥50% is the “point of no return” for Gross Motor Function Classification System IV-V cerebral palsy patients, representing the cutoff value beyond which no spontaneous cerebral palsy reduction may be expected, unless addressing surgery.
Level of evidence:
level II—retrospective study.
Introduction
Children affected by cerebral palsy (CP) have an increased risk of progressive hip luxation. Complete luxation, also called dislocation, corresponds to a migration percentage (MP) of 100%; subluxation or displacement is mostly defined as an MP of between 30% and 99%. 1 The incidence of subluxation is related to CP severity, which is defined according to the Gross Motor Function Classification System (GMFCS). More severe non-ambulatory bilateral patients (GMFCS IV and V) are known to be the most vulnerable to hip displacement.2–4
Screening programs are strongly recommended5–7 to intercept hip luxation at early stages and to implement treatment. 8 A multimodal approach is recommended in CP surveillance programs. It includes conservative treatments, such as postural management and botulinum,9–13 although they are supported by limited evidence, and surgery, which has been demonstrated to be effective in reducing the MP.14–16 Age and type of surgery are still under debate, although recent studies are in favor of early 17 and bone surgery.14–16,18 The MP is mostly advocated as the parameter to address surgery; generally, it is considered for MP >40%.16,19,20 Wordie et al. 21 specifically investigated this aspect in children registered in the Cerebral Palsy Integrated Pathway (CPIP) Scotland surveillance program, who did not undergo any surgical approach to the hip. The authors performed a remarkably interesting analysis to find out a cutoff MP value, which determined the point of no return: it corresponded to MP ≥46%. This finding is important because it identifies the limit beyond which no MP reduction may be expected, unless proceeding surgery. The examined sample included all five GMFCS levels. But it is known that GMFCS levels IV and V are the most exposed to the risk of progression and might have a different trend if separately considered. Therefore, a specific analysis limited to this subgroup is advisable.
A retrospective cohort study was conducted, involving 162 CP patients, GMFCS levels IV–V, who attended our tertiary referral center. The objective of the study was to identify the cutoff MP value, beyond which no spontaneous reduction of hip displacement might be expected.
Methods
Participants
Inclusion criteria were: bilateral spastic or dyskinetic CP, according to Surveillance of CP in Europe (SCPE) classification; GMFCS level IV or V; age 0–18 years; having attended the Children Rehabilitation Unit at the S. Maria Nuova Hospital in Reggio Emilia, before March 2020; having at least three pelvic radiographies (≥1-year interval between two consecutive radiographies), with MP reported or measurable, excluding radiographies relative to hips having previously undergone surgery; informed consent of the parents for minors; informed consent of the adult patient if he or she was able to independently subscribe it or of the support administrator for vulnerable adults. The study was approved by the Area Vasta Emilia Nord Ethics Board on 21 April 2020 (200/2020/OSS*/AUSLRE).
We acquired the following information from the patients’ charts.
Radiographic evaluation
MP was measured for right and left hips for each acquired radiography. The MP was calculated on an anterior-posterior radiography of the pelvis, acquired in a supine position with the legs parallel, avoiding either pelvic rotation or anteversion.22,23 The MP was calculated as the percentage of ossified femoral head lying lateral to Perkin’s line. The Perkin’s line was drawn through the lateral acetabular margin and perpendicular to Hilgenreiner’s line. The latter one passed through the superior aspect of the triradiate cartilage or, if this one was closed, through the inferior ischii. In case of severe acetabular dysplasia, when identifying the acetabular margin might be challenging, the peak of the “gothic arch” was considered to derive the Perkin’s line. 23
Clinical and functional assessment
Sex; CP subtype according to SCPE; GMFCS level; the presence of drug-resistant epilepsy, as a marker of CP severity; age corresponding to the date of the acquired radiography; having undergone botulinum (BoNT-A) injections in hip muscles during the 6 months prior to the radiography; the presence of pelvic obliquity and/or lumbar scoliosis, either clinically or radiographically recorded; hip pain, as a dichotomous variable (pain/no pain), reported by patients or caregivers, or clinically evidenced; the use of assistive devices for standing or walking (such as standing tables or weight support walkers); ongoing treatment with oral baclofen or intrathecal baclofen (ITB).
The participants used several types of assistive devices, according to individualized needs. All of them were provided with sitting system, either customized on cast or predisposed. They both were set in order to ensure comfort, pelvis and trunk best alignment, and to facilitate participation in activities of daily living. Whenever possible, based on clinical and contextual individual characteristics, walking and/or standing devices were provided. Walking devices ensured total or partial body weight support, freeing up propulsive strategies otherwise impeded in quadriplegic patients. The standing devices kept the patients in a straight and aligned position, either vertical or slightly prone or supine, depending on the severity of the CP. If needed, a pelvic support to relieve weight was provided. Maximum attention was paid to avoid sustained asymmetric or pathological postures or patterns of movement (i.e. scissoring or pelvic obliquity) by adjusting the devices and/or providing targeted botulinum injections. If those were not avoidable or if the child showed low compliance, the devices were suspended. Both walking and standing devices were mostly used in everyday settings, such as home or school, involving children in playful and/or social activities, according to children’s compliance and contextual barriers.
Botulinum injections in hip muscles during the 6 months prior to radiography were recorded. Injection sites might involve either one or more of the following muscles: adductors, hamstrings, gracilis, rectus femoris, and psoas. BoNT-A dose (dilution 1–2 mL) was individually calculated considering the child’s weight, characteristics, and number of muscles injected.
Statistical analysis
Descriptive statistics are presented for baseline demographic clinical characteristics of participants. Continuous variables are presented as mean, standard deviation (SD), minimum (min), and maximum (max); categorical variables are presented as frequency (N, percentage (%)).
Data were then analyzed at the level of the individual hips. For each hip, three MP measures were considered: the first available MP measure, the worst intermediate MP measure (i.e. the highest), and the last available MP measure. The overall trend was enquired by plotting the change in MP for each individual hip against age.
Receiver operating characteristic (ROC) curve analysis was then conducted to investigate which value of the MP could be adopted as the “point of no return”: that is, the cutoff value beyond which no MP reduction, by more than 5%, could be expected; conversely, increasing displacement may incur. An ROC curve describes the relationship between the sensitivity and specificity of a test by plotting the two against one another while varying the evaluation, which determines the outcome of a test. The two are inversely related, because as one increases, the other decreases. Conventionally, since both values range between 0 and 1, the sensitivity (true positive rate) is plotted against 1 minus the specificity (false positive rate). The plot is, therefore, in essence a representation of the trade-off between detecting true and false positive cases. The discriminatory capacity of the MP cutoff value for spontaneous improvement of hip subluxation was assessed by the area under the curve (AUC). Sensitivity and specificity were then calculated to establish the cutoff points for MP. Then, the chi-square test (χ2) was performed to verify whether the established cutoff points were associated.
Student’s t-test was used to compare the means of the demographic and clinical variables between two subgroups, defined according to the presence or absence of the cutoff value found.
Finally, a logistic regression analysis was performed to verify the effect of the considered variables, adjusted for covariates that showed associations with p < 0.20 in the bivariate analysis, and to calculate the odds ratio (OR) to measure the strength of the association found. A 95% confidence interval and a p-value of 0.05 were adopted for statistical significance of data.
MedCalc Statistical Software version 14.8.1 (MedCalc Software bvba, Ostend, Belgium; http://www.medcalc.org; 2014) and STATA program version 14 (StataCorp LP, College Station, TX, USA) were used to perform the statistical analysis.
Results
A total of 1208 subjects with quadriplegic CP attended our Unit between January 2008 and February 2020, according to our records. However, as charts prior to 2015 were not available for consultation, only those of 530 patients could be examined.
Finally, a total of 162 subjects affected by bilateral CP fulfilled the inclusion criteria. A large amount of patients were excluded because either they were addressed to surgery or they did not have three radiographies available (≥1-year interval between two consecutive radiographies); moreover, a few ones did not give their informed consent. The mean age at the first visit was 4.01 years (SD, 2.80). There were 64 females and 98 males, 64 subjects within GMFCS IV and 98 within GMFCS V, and 141 cases of spastic and 21 of dyskinetic CP. A total of 12 patients had drug-resistant epilepsy (they all were GMFCS V). The data were analyzed at the level of the individual hips and then 324 hips were studied, with a mean of 4.5 (SD 1.8, 3–13) consecutive radiographies each. The mean length of follow-up was 5.5 years (SD 3.5; 3–11.8 years). For each hip, three MP measures were considered: the first available MP measure, the worst intermediate MP measure (i.e. the highest), and the last available MP measure. Provided that, a total of 972 MP measurements were considered for the analysis.
A Spaghetti plot (Figure 1) is used to represent the progression of each of the individual hips, considering the first, the worst intermediate (i.e. the highest), and the last available MP measure. As it can be observed, most of the individual MP trends, displayed as noodles, flow under the red line, which represents the cutoff value of MP ≥50%.
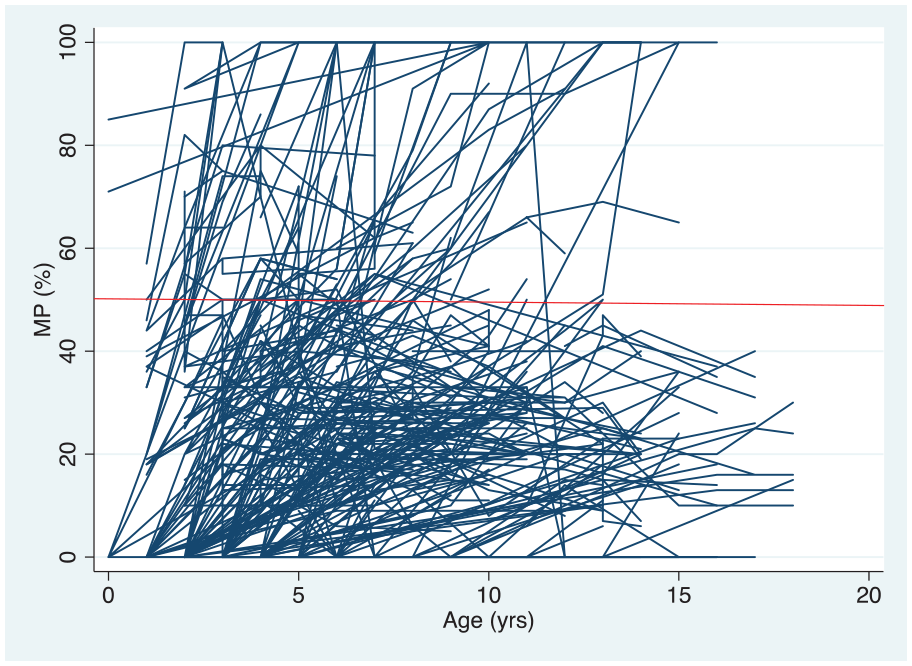
Individual progression of all the hips through the three MP measures considered: the first and the last one, across the highest intermediate one. The red line indicates a migration percentage of 50%.
ROC curve analysis was conducted to investigate which value of the MP could be adopted as the cutoff value beyond which no MP reduction, by more than 5%, could be expected. Calculation of specificity for each MP resulted in an optimal specificity at an MP of 50%. The discriminatory capacity of MP ≥50%, as the cutoff value for spontaneous improvement of hip subluxation, was assessed by AUC. Sensitivity and specificity were calculated to establish the cutoff points for MP ≥50%. The χ2 test was performed to verify whether the established cutoff points were associated. The AUC was 1.00 (95% confidence interval (CI), 0.98–1.00; p < 0.001) with a sensitivity of 84.5% and a specificity of 100% (p < 0.001). Then MP ≥50% was confirmed to be the optimal cutoff value.
The sample was subdivided into two groups, based on the presence or absence of MP ≥50%. A total of 772 (79.4%) hips resulted in having an MP <50%, while 200 (20.6%) hips had MP ≥50%. Student’s t-test was used to compare the means of the demographic and clinical variables between the two subgroups and logistic regression analysis was conducted. A statistically significant association was found between MP ≥50% and females (OR, 2.31; 95% CI, 1.68–3.17; p < 0.001), GMFCS V (OR, 4.4; 95% CI, 2.96–6.65; p = 0.001), drug-resistant epilepsy (OR, 4.48; 95% CI, 2.74–7.34; p < 0.001), oral baclofen (OR, 1.80; 95% CI, 1.27–2.53; p = 0.001), hip pain (OR, 4.7; 95% CI, 2.21–10.12; p < 0.001), and lumbar scoliosis (OR, 1.84; 95% CI, 1.19–2.86; p = 0.006). Conversely, the dyskinetic subtype (OR, 0.57; 95% CI, 0.33–0.96; p = 0.036) and the use of standing (OR, 0.44; 95% CI, 0.31–0.60; p < 0.001) or walking (OR, 0.35; 95% CI, 0.24–0.51; p < 0.001) devices appeared to reduce the odds of having an MP ≥50%. Detailed data are represented in Table 1.
Details of the 972 hips included and regression analysis considering the demographic and clinical characteristics as independent variables and MP ≥50 as the dependent variable.
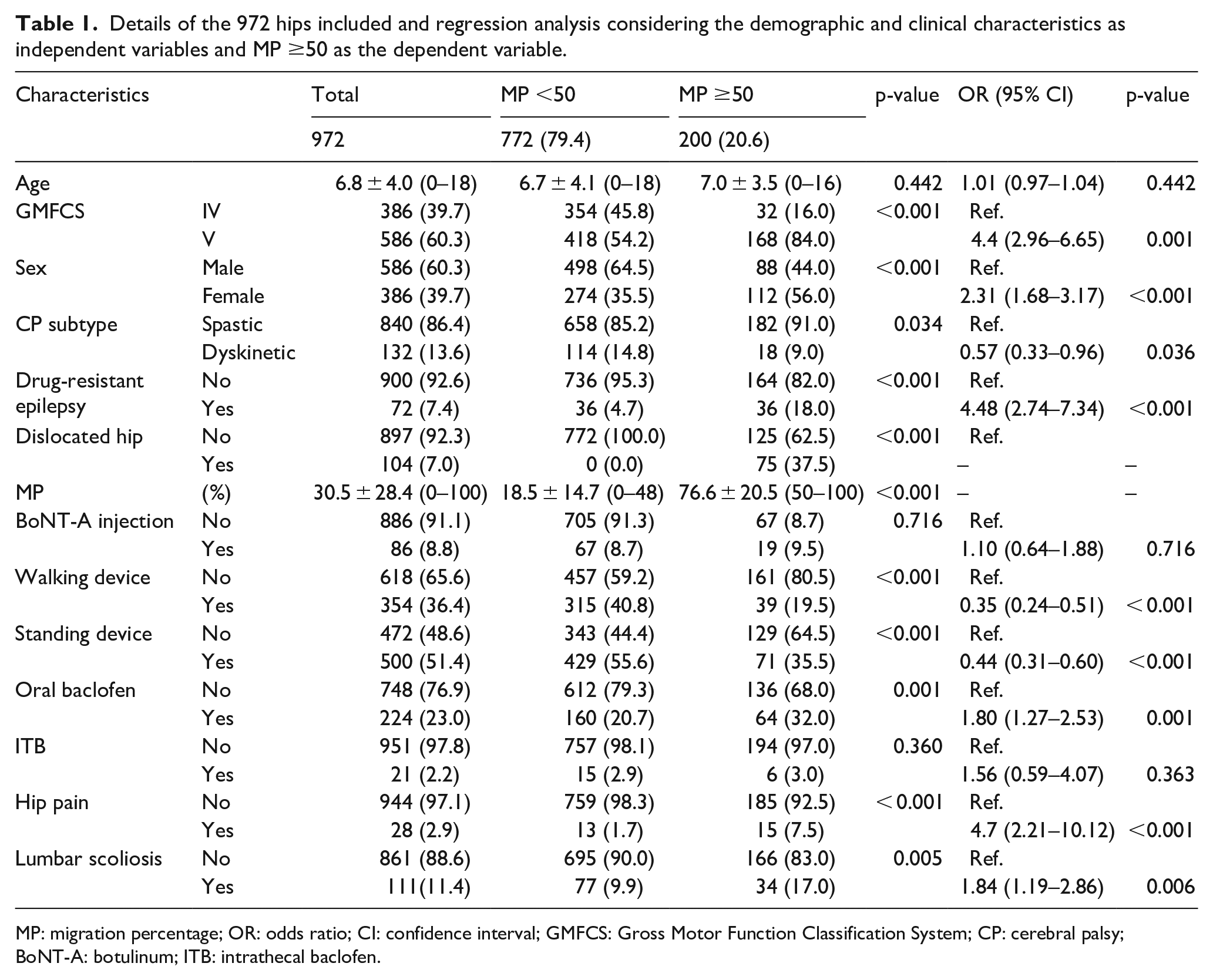
MP: migration percentage; OR: odds ratio; CI: confidence interval; GMFCS: Gross Motor Function Classification System; CP: cerebral palsy; BoNT-A: botulinum; ITB: intrathecal baclofen.
Discussion
The results identified MP ≥50% as the “point of no return”: that is, the cutoff value beyond which no spontaneous MP reduction could be expected and increasing displacement may incur.
This value is a little higher than the cutoff found by Wordie et al. 21 (MP ≥46%), but the difference is comprised in the measurement error of ±5°, 23 so it should not be considered as significant.
The relevant finding is that the cutoff value that resulted from the present study is not lower than Wordie’s, 21 contrary to expectations, considering the sample of GMFCS IV–V. This might be attributed to individual characteristics of the population that was examined, which is not representative of the Italian population. In fact, different from Wordie et al., 21 the sample was recruited among patients having attended the Unit that promoted this study, not from a surveillance program of the general CP population in Italy, although patients referred to this Unit, a tertiary referral center, may have presented a more severe or complicated clinical situation than that of the general quadriplegic CP population.
The mean age of the present study was a little lower (6.4, 0–18 years) compared to Wordie’s 21 (11.6, 3–18 years). The mean follow-up was also a little shorter (5.5, 3–11.8 years) compared to Wordie’s 21 (6.5, 2–14.8 years). These aspects might justify the small difference found in the MP cutoff value.
The conservative approach adopted in the examined sample might have contributed to preserve a high cutoff MP value. As described, an individually tailored integrated program was provided, including postural management and spasticity treatment. Still the present analysis does not allow to draw conclusive evidence.
The cutoff value of MP ≥50% is consistent with several studies that consider an MP <50% a good outcome after surgery.15,16,24,25 Since the 1980s, some authors26–28 have suggested that if soft tissue surgery is executed before MP has reached 50%, further luxation may be prevented. Conversely, preoperative MP >50% has been associated with poor outcome after soft tissue surgery.15,16,24,29 Ha et al., 30 investigating preoperative radiologic predictors of successful soft tissue surgery, found no significant predictive value of the MP. Only the Acetabular Index (AI) significantly influenced the outcome, according to their findings. AI was not considered in the present analysis, and this accounts for a limitation of the study.
Provided a measurement error of ±5°, as calculated by Shore et al., 23 values of MP ≥45% should be considered with caution in the management of the subluxated hip in CP children GMFCS IV–V. The point of no return might be reached, and surgery might be the advisable option to prevent hip luxation. Conversely, in very frail children (i.e. Children with Medical Complexity), for whom any surgical approach is excluded because it is highly risky, hips with MP <55% might escape progression. In this case, ensuring an individually tailored postural management and, if needed, spasticity treatment remains advisable.
Future research is needed to identify other predictive factors, addressing surgical approach. The clinical situation, such as muscle contractures, is to be considered a rationale for surgery, even when radiologic parameters are negative.
Study limitations
The results of this study should be interpreted with caution as they derive from a retrospective design. Prospective long-term studies must be conducted to confirm the optimal cutoff MP value.
Moreover, the sample was recruited among patients attending or having attended the Unit that promoted this study, not from a surveillance program of the general CP population in Italy. Patients referred to this Unit, a tertiary referral center, may have presented a more severe or complicated clinical situation than that of the general quadriplegic CP population.
Conclusion
An MP ≥50% is the “point of no return” for patients with GMFCS IV–V CP, based on the present findings. It represents the cutoff value beyond which no spontaneous MP reduction could be expected and increasing hip displacement may incur, unless addressing surgery.
Footnotes
Acknowledgements
We thank Prof. Adriano Ferrari for the scientific and clinical guidance.
Author contributions
S. Faccioli: Conceptualization, data analysis, writing the manuscript.
S. Sassi: Conceptualization, data analysis.
E. Corradini: data extraction.
F. Toni: data extraction.
S. Kaleci: statistical analysis, writing the manuscript.
F. Lombardi: manuscript revision.
M.G. Benedetti: manuscript revision.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.