
Abstract
Background:
Percutaneous femoral derotational osteotomies are performed in both adult and pediatric patients. There is little published on the outcomes after femoral derotational osteotomy in pediatric patients.
Methods:
A retrospective cohort study of pediatric patients treated with percutaneous femoral derotational osteotomy by one of two surgeons between 2016 and 2022 was performed. Data collected included patient demographics; surgical indications; femoral version; tibial torsion; magnitude of rotational correction; complications; time to hardware removal; pre-operative and post-operative patient-reported outcome scores, including Limb Deformity–Scoliosis Research Society and Patient-Reported Outcomes Measurement Information System; and time to consolidation. Descriptive statistics were used to summarize the data and t tests used to compare means.
Results:
Thirty-one femoral derotational osteotomies in 19 patients were included with an average age of 14.7 (9–17) years. The average rotational correction was 21.5° ± 6.4° (10°–40°). The average length of follow-up was 17.9 ± 6.7 months. There were no instances of nonunion, joint stiffness, or nerve injury. No patients returned to the operating room for additional surgeries other than routine hardware removal. There were no cases of avascular necrosis of the femoral head. Of the 19 patients, 8 completed both a pre-operative and post-operative survey set. There were significant improvements in the Limb Deformity–Scoliosis Research Society Self-Image/Appearance sub-category and the Patient-Reported Outcomes Measurement Information System Physical Function sub-category.
Conclusion:
Femoral derotational osteotomy using a percutaneous drill hole technique with antegrade trochanteric entry femoral nail is safe in the pediatric population and improves self-image in patients with symptomatic femoral version abnormalities.
Introduction
Rotational malalignment of the lower extremity is potentially debilitating with a host of short-term and long-term implications. Femoral rotational deformities include excessive anteversion, in which the angle between the axis of the femoral neck and the transcondylar axis of the knee is abnormally high, and excessive retroversion, in which this angle is low. 1 Typically, 10°–20° of anteversion is considered normal, with angulation above and below this range constituting excessive anteversion and retroversion, respectively. Both conditions may be associated with gait abnormalities, difficulty with physical activity, pain, and poor self-image. 2 There is some evidence that rotational malalignment may lead to hip pathology, patellofemoral instability, and degenerative changes.1,3,4 Excessive anteversion is normal in children, but usually remodels by around the age of 8 years. 5 Symptomatic version abnormalities after age 8 are unlikely to remodel naturally. In these cases, children may benefit from surgical intervention. 2 While there are multiple options for correcting version abnormalities, a diaphyseal osteotomy with trochanteric start antegrade intramedullary nail fixation is highly advantageous due to small incisions, reliable healing, and early full weight-bearing. 2 Our practice has implemented this technique successfully for many years and has found that an antegrade nailing technique is safe in pediatric patients without any cases of avascular necrosis (AVN) of the femoral head or proximal femoral deformity to date. 6
There is currently a paucity of data on the short- and long-term outcomes of femoral derotational osteotomy in the pediatric population. To our knowledge, there are very few studies investigating the surgery’s impact on patient-reported outcome measures (PROMs). This study aims to highlight the clinical and radiographic outcomes after femoral derotational osteotomy in a pediatric cohort of patients and report on PROMs in this group.
Methods
Following ethics board approval, a review of our surgical database was performed for all pediatric patients (below 18 years old) who had a femoral derotational osteotomy for either symptomatic excessive femoral anteversion or retroversion between 2016 and 2022 by one of two surgeons. Patients with concomitant surgery for additional deformity correction (tibial derotation, distal femoral osteotomy, etc.) were included. Patients were excluded if they had less than 8 months of follow-up or underwent a rotational correction of less than 10°. Collected information included patient demographics, indications for surgery, femoral version, tibial torsion (if applicable), magnitude of rotational correction, complications, time to hardware removal, pre-operative and post-operative PROMs outlined below, and time to consolidation. Version measurements were performed by the treating surgeon on computed tomography (CT) scans with cuts through the hip, knee, and ankle, as previously described. 5 The magnitude of each correction was measured intra-operatively—a goniometer was used to measure the degree of divergence between two rotational navigation pins before they are aligned in the axial plane. Consolidation was considered achieved when at least three cortices displayed confluent bridging bone at least 2 mm thick.
Pre-operative patient evaluation included a detailed history; physical examination; gait examination; hip-to-ankle radiographs to assess for coronal plane deformities or limb length discrepancy (LLD); a CT version study with cuts through the hip, knee, and ankle; calibrated AP (antero-posterior) and lateral femur films for pre-operative templating; and hip magnetic resonance images if there was concern for hip pathology. All of these diagnostic tools factor into the planning and execution of each correction. All patients received a standard set of patient-centered surveys pre-operatively. The first survey was the Limb Deformity–Scoliosis Research Society (LD-SRS) questionnaire. This is a reliable, validated version of the Scoliosis Research Study (SRS) that asks Likert-type-scale questions pertaining to various aspects of quality of life. Each response is converted into a numerical score from 1 to 5, with 1 representing the worst possible response and 5 representing the best response. 7 These numeric scores are then averaged and stratified to generate a total score and four subscores, each representing a different facet of quality of life. The second survey is the patient-reported outcomes measurement information system (PROMIS), which is a similar questionnaire that assesses multiple aspects of patient health on a scale from 1 to 50, where 1 represents the worst possible score and 50 represents the best score. The responses are averaged to generate four subscores, similar to the LD-SRS. 8 Patients were encouraged to complete the same set of surveys at 4, 9, 18, and 36 months post-operatively.
Details of our operative approach have been reported previously.3,9 Briefly, a percutaneous drill hole corticotomy is performed at the site of the intended osteotomy, but the osteotomy is not completed prior to reaming. A greater trochanteric start point is visualized using fluoroscopy and reaming is then performed over a ball-tipped guidewire. Performing the drill hole corticotomy prior to reaming allows for egress of marrow elements at the site of the osteotomy during reaming as well as venting of the femur to prevent excess pressure while reaming the intact femur and fat emboli. 10 Rotational navigation pins are then placed into the femur proximal and distal to the osteotomy site. The proximal pin is placed posterior to the intended path of the nail and the distal pin is placed proximal to the physis but distal to the intended distal extent of the nail. These bicortical pins are placed so that their degree of divergence in the axial plane is the same as the degree of intended rotational correction. This allows for pins that are parallel after correction. The degree of divergence of the pins is carefully measured using a sterile goniometer. Once the pins have been placed, the osteotomy is completed percutaneously using 0.5-inch osteotomes and the nail is passed across the osteotomy site while simultaneously derotating the femur. Once the pins are parallel, the rotational correction is held with an external fixator rod and clamps. The distal and proximal interlocking screws are then placed and final fluoroscopic images are obtained.
As noted above, some of the included femoral derotational osteotomies were performed as part of a larger combined procedure. Tibial derotational osteotomies were performed in a similar percutaneous manner to the femoral derotational osteotomies and a prophylactic anterior compartment release was performed in 12 of 14 cases. Tibial derotational osteotomies were performed in the diaphysis and fixation was with an intramedullary nail or external fixator. Coronal plane angular deformity was corrected in several cases with a second femoral osteotomy (distal) which was stabilized with a plate and screws and was distal to the intramedullary nail. However, the proximal aspect of the plate did extend past the distal tip of the nail to avoid a stress riser. In one case, a coronal plane angular deformity was addressed with guided growth (hemiepiphysiodesis using a tension band plate) distal to the intramedullary nail.
Descriptive statistics were used to summarize data, and Student’s t tests and paired t tests were used to compare means. All tests were two-tailed with significant difference set at p < 0.05. Means and standard deviations (SDs) were reported for continuous variables. Analyses were performed using either Microsoft Excel 2019 Statistical Analysis Toolpak (Redmond, WA, USA) or DATAtab Team (2021; DATAtab: Online Statistics Calculator. DATAtab e.U. Graz, Austria).
Results
From August 2016 to March 2022, 31 femoral derotational osteotomies were performed in 19 patients. The cohort included 7 males and 12 females, with an average age of 14.7 ± 2 years (9–17 years). Of the 31 femurs, 9 were skeletally immature at the time of the surgery. Two patients with hip pain were evaluated with a magnetic resonance imaging (MRI). No labral tears were noted. Surgical sites and deformity overviews are summarized in Tables 1 and 2. Of the 12 bilateral procedures, 11 (22 of 24 bilateral surgeries) were performed in a staged fashion with an average time between procedures of 3.2 ± 2.2 months (21 days–7 months). Indications for surgery are summarized in Table 3. The pre-operative and post-operative rotation profiles for each group are summarized in Table 4.
Surgical site.
Deformity summary.
Indications for surgery.
Rotational profile.
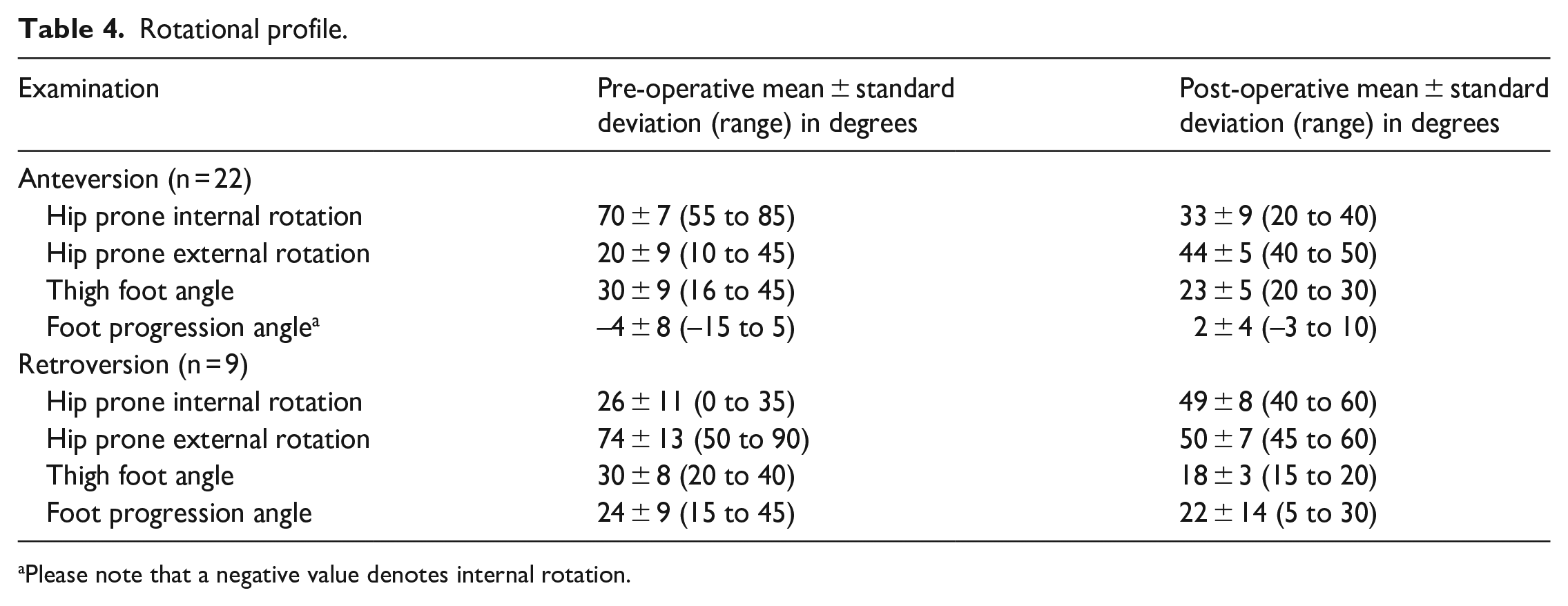
Please note that a negative value denotes internal rotation.
There were 22 femurs that underwent derotation for excessive anteversion (9 femoral anteversion alone, 11 femoral anteversion + external tibial torsion, and 2 femoral anteversion + angular correction segments). The degree of malrotation and subsequent surgical correction were specified through CT scan analysis. An average version of 35° ± 9° (19°–57°) was measured. The average correction in this group was 21° ± 6° (10°–35°).
There were nine femurs that underwent excessive retroversion correction (five femoral retroversion alone, three femoral retroversion + external tibial torsion, and one femoral retroversion + angular correction segment). The average pre-operative version measured via scan was −7° ± 9° (–19° to 11°). The average correction in this group was 24° ± 8° (10°–40°). Among the 14 cases of external tibial torsion correction, the average pre-operative torsion was 47° ± 6° (39°–58°) and the average correction was 21° ± 4° (15°–30°).
The average time to consolidation for the anteversion cohort was 64.6 ± 16.5 days (40–90 days), and the average time to consolidation for the retroversion cohort was 69.7 ± 17.3 days (40–96 days) (p = 0.45). For patients who underwent concomitant tibial derotational osteotomies, the average time to consolidation was 74.9 ± 13.9 days (53–96 days). Comparatively, patients who strictly underwent derotational osteotomies of the femur, regardless of retroversion or anteversion, had an average time of consolidation of 58.8 ± 15.4 days (40–90 days) (p = 0.05). Indeed, the longer time to bone consolidation for those undergoing simultaneous femur and tibia derotations compared to strictly femoral malrotation corrections was statistically significant.
The average length of follow-up was 17.9 ± 6.7 months (8.9–36.9 months). There were seven femurs with less than 1-year follow-up. All patients achieved union in 3 months or less. No patients returned to the operating room for additional surgeries related to the femur other than routine hardware removal. Twenty-eight femoral nails have been removed to date, with an average time to removal of 12.8 ± 3.9 months (6–21 months). No patients suffered complications related to the femur, and there were no cases of AVN of the femoral head. Figure 1 demonstrates an example of the clinical improvement of a patient in our cohort who had bilateral femoral and tibial derotational osteotomies. Figure 2 demonstrates an example of the right femur pre-operative planning and 7-month post-operative radiographs obtained in the same patient as Figure 1. Figure 3 shows the pre-operative femoral and tibial version measurements for the same patient using axial CT cuts through the hip, knee, and ankle.
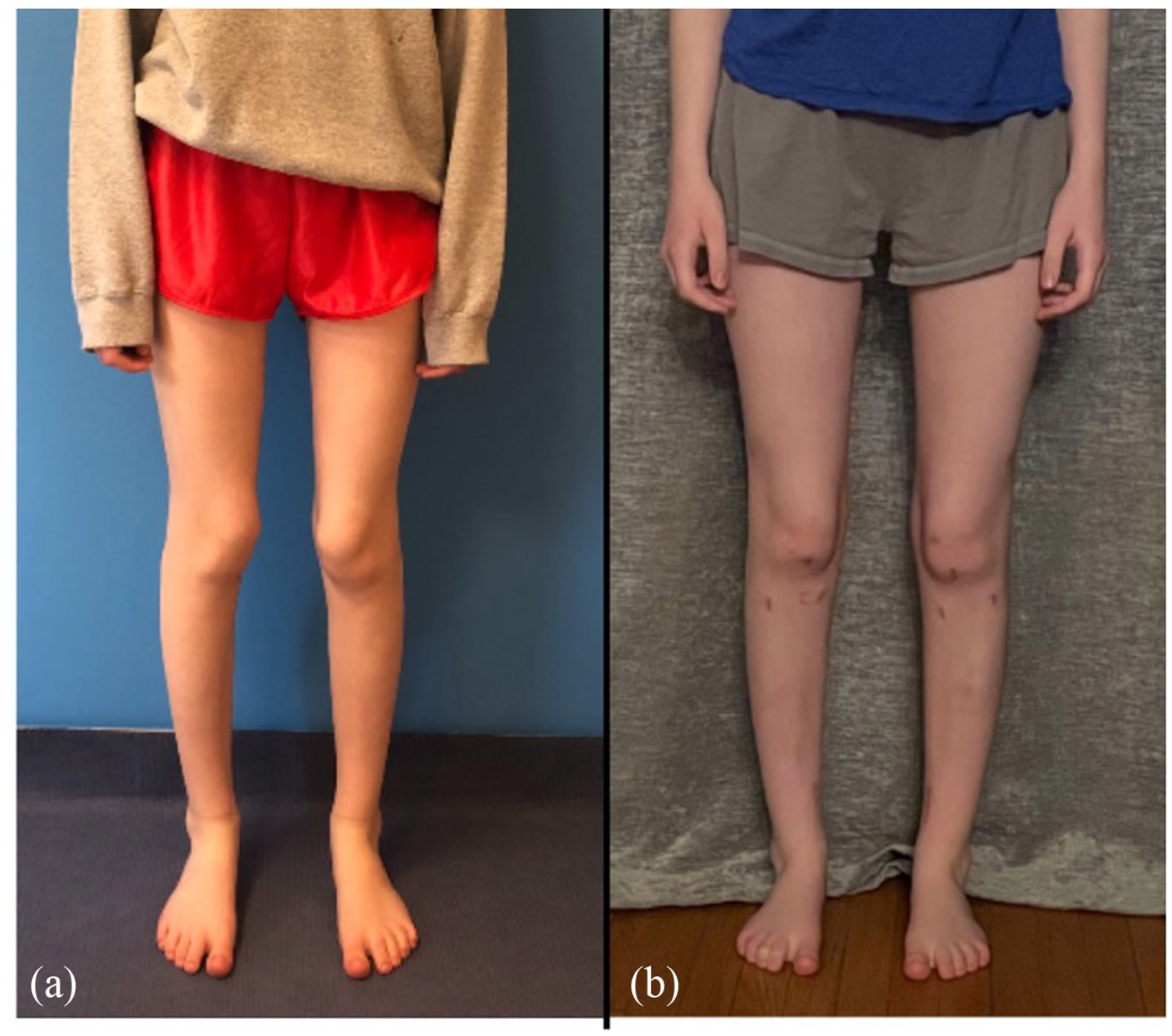
Pre-operative (a) and 16 months post-operative (b) clinical photographs of a 17-year-old female who had 20° of excessive femoral anteversion and 25° of excessive external tibial torsion corrected bilaterally. Note the “winking patellas” pre-operatively.
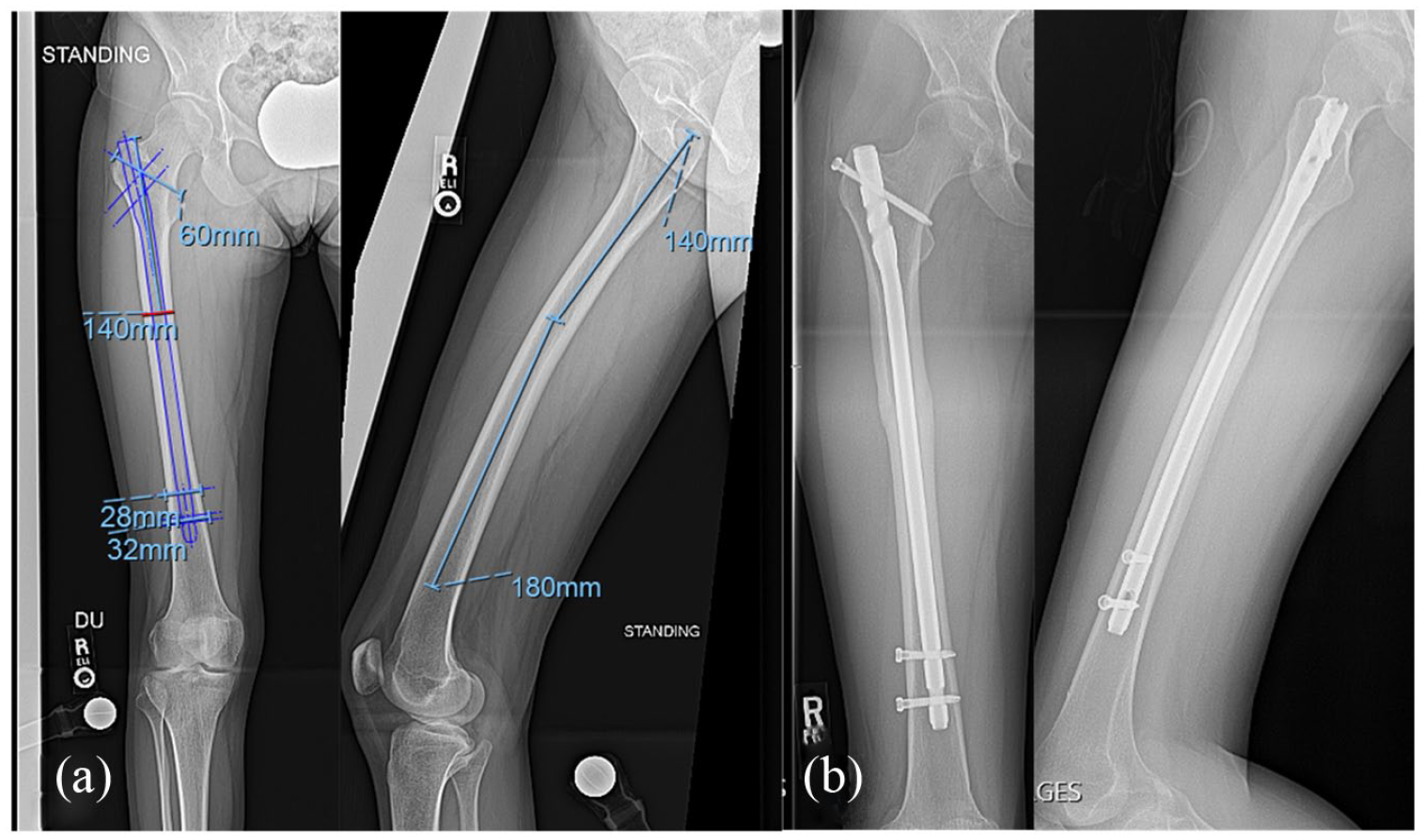
Pre-operative templating of the right femur including AP and lateral radiographs (a). There is a trochanteric entry nail planned for the femur with the osteotomy 140 mm distal to the tip of the greater trochanter, which corresponds to the apex of the anterior femoral bow. AP and lateral radiographs of the right femur 7 months after surgery (b) demonstrate union at the osteotomy sites.
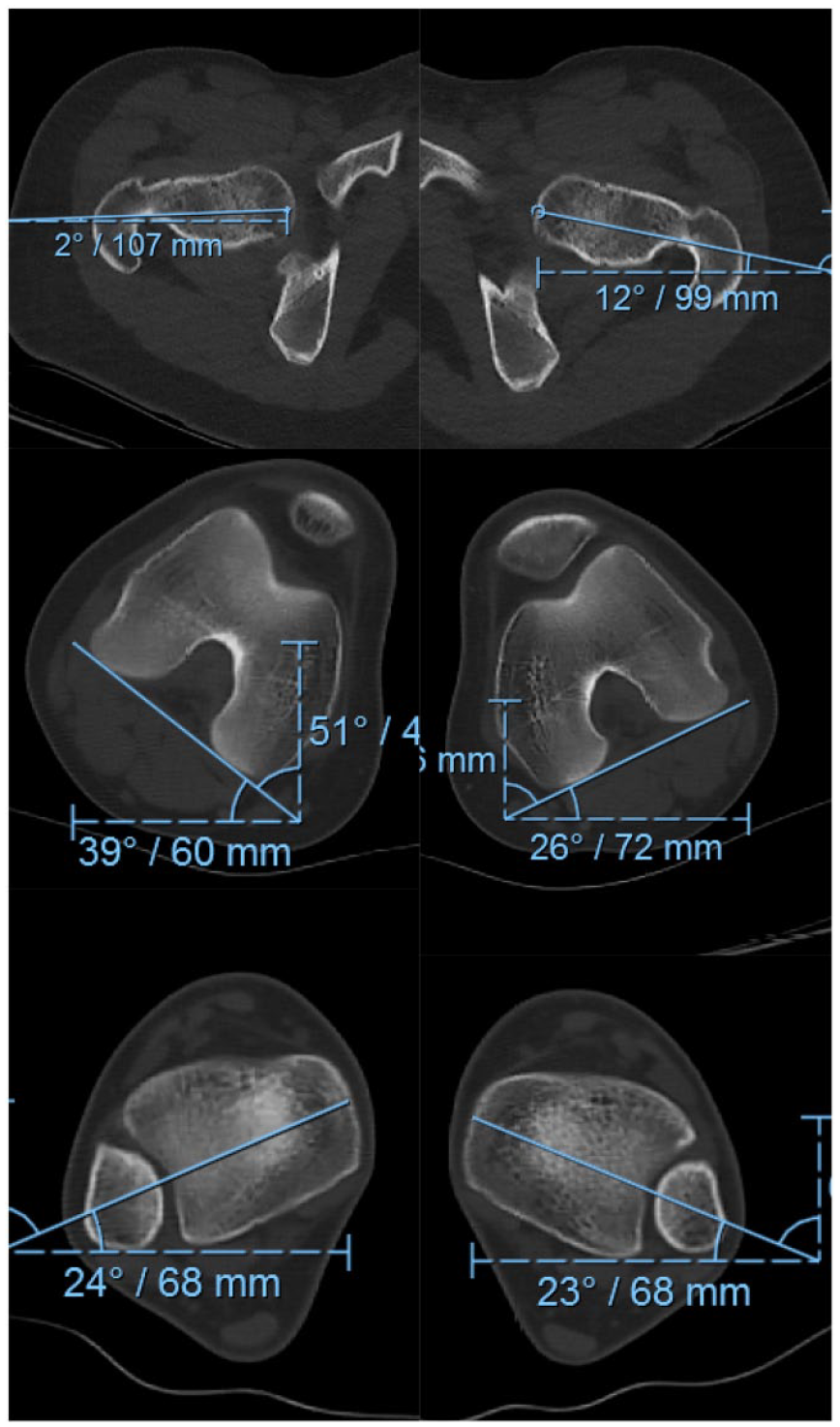
CT version study demonstrates femoral anteversion of 41° on the right and 38° on the left (normal ~10°–20°). Tibial torsion is 63° external on the right and 49° external on the left (normal ~25°–35°).
Of the 19 patients, 8 (42%) completed both a pre-operative and post-operative survey set that included the LD-SRS and PROMIS questionnaires which are used to evaluate each patients’ self-reported satisfaction with their treatment. Of these eight patients, four presented with femoral anteversion + external tibial torsion, three presented with femoral anteversion, and one with femoral retroversion. The average post-operative survey time of completion was 14.6 ± 9.4 months (7–35 months) following surgery. The total survey scores (and subscores) of these eight patients are summarized in Table 5. There were statistically significant improvements in the LD-SRS Self-Image/Appearance sub-category from 3.28 pre-operatively to 4.24 post-operatively (p < 0.01) and the PROMIS Physical Function sub-category from 46.44 pre-operatively to 49.51 post-operatively (p = 0.03). There were no significant differences identified in the total LD-SRS, total PROMIS Pediatric Global Health, or remaining sub-categories from pre-operative to post-operative values.
PROMs outcomes.
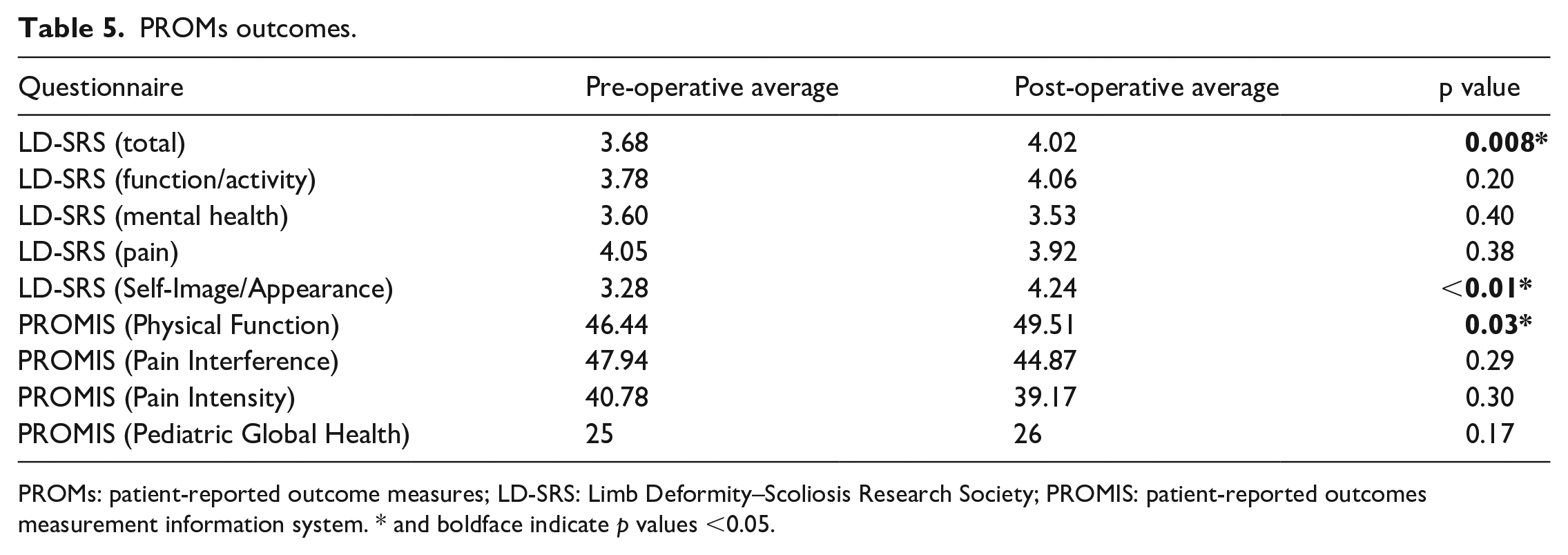
PROMs: patient-reported outcome measures; LD-SRS: Limb Deformity–Scoliosis Research Society; PROMIS: patient-reported outcomes measurement information system. * and boldface indicate p values <0.05.
Discussion
We sought to evaluate the clinical, radiographic, and patient-reported outcomes of a pediatric cohort after femoral derotational osteotomy for symptomatic version abnormality. We found that using a percutaneous drill hole osteotomy technique with fixator assistance and antegrade trochanteric entry femoral nail is safe in pediatric patients with none of the patients in our cohort experiencing complications related to their femoral procedures. All femoral osteotomies were consolidated by 3 months post-operatively and no patient developed AVN of the femoral head during procedures. In 8 of 19 of our patients, a statistically significant improvement was observed in comparing the pre-op LD-SRS Self-Image/Appearance and post-op PROMIS Function scores. To our knowledge, this is only the second study to report on PROMs after femoral derotational osteotomy in a pediatric population. Hamid et al. used the pediatric outcomes data collection instrument to investigate changes in PROMs following this procedure. 11 They noted improvements in transfer/basic mobility, sports/physical function, global functioning, and satisfaction with symptoms in their internal torsional deformity patients. In their external torsional deformity patients, they noted an improvement in satisfaction with symptoms after surgery. Our findings corroborate Hamid’s findings of improvements in PROMIS Physical Function and LD-SRS Self-Image/Appearance while further demonstrating the value of the femoral derotational osteotomy in pediatric populations.
The statistically significant improvement in the LD-SRS Self-Image/Appearance sub-category from 3.28 to 4.24 (0.96 difference, p < 0.01) is likely clinically significant as the minimum clinically important difference (MCID) of the LD-SRS score is approximately 0.3. 7 Many patients with rotational deformities are unhappy with the appearance of their lower extremities and self-conscious of their gait abnormalities. Derotational osteotomy immediately corrects the deformity, which is likely why we found a significant improvement in this PROM with a small percentage (40%) of the cohort filling out both pre-operative and post-operative surveys.
Heath et al. 12 found a significant difference in LD-SRS Self-Image/Appearance scores in patients with LLD, angular deformity, or combined LLD and angular deformity compared to healthy controls. To our knowledge, there has not been a similar study performed comparing LD-SRS scores of patients with version abnormalities to healthy control patients. Based on this study, it is likely that patients with symptomatic version abnormalities have significantly lower LD-SRS Self-Image/Appearance scores than their peers, but this should be confirmed in future studies.
The statistically significant improvement in the PROMIS Physical Function score from 46.44 to 49.51 (3.07 difference, p = 0.03) may or may not be clinically significant. While the MCID of the PROMIS Physical Function score has not been reported specifically for limb deformity, in foot and ankle literature MCID for PROMIS Physical Function has been reported between 3 and 30 points (median = 11.3). 13 While it is likely that a patient’s physical functioning does improve after femoral derotational osteotomy due to improvements in gait mechanics, this study does not detect a clinically important difference in the PROMIS Physical Function score. Therefore, this conclusion cannot be made based on this study.
Indications for femoral derotational osteotomy are somewhat controversial, and there is no widely agreed-upon quantitative degree of anteversion or retroversion that is a firm indication for operative management. A 15° of femoral anteversion is often considered normal with a typical range between 10° and 20°. 5 Version that falls outside this normal range combined with symptoms, and a history and physical examination consistent with version abnormality is our indication for derotational osteotomy. Symptoms may include gait disturbances, frequent tripping, hip pain or instability, or patellofemoral instability. 1 The goal of surgery is to improve gait and reduce symptoms attributable to version abnormality. Femoral derotational osteotomies can be proximal, diaphyseal, or distal. 1 The authors prefer diaphyseal osteotomies as they can be stabilized with intramedullary nails, which allow for percutaneous incisions, minimal soft tissue dissection with no periosteal stripping, reliable union, and early weight-bearing and mobilization.
Gordon et al. 2 described the outcomes of a similar technique for femoral derotational osteotomy in skeletally immature patients with excessive femoral anteversion. The study retrospectively reviewed the results of the technique in 13 patients and 21 limbs with minimum 1-year follow-up. All patients complained of tripping and gait abnormalities pre-operatively. All patients noted gait improvement and no intra-operative or post-operative complications were reported. Healing of the osteotomy occurred at a mean of 6 weeks post-operatively. No patient developed AVN. In further follow-up of Gordon’s experience, Stambough et al. reported International Knee Documentation Committee-9 (IKDC-9), Marx, and Tegner activity scales of 28 adolescent patients with symptomatic excessive femoral anteversion who underwent derotational osteotomy using a similar technique as the current study. 14 They found that 78.5% demonstrated a mean significant improvement of 13 points for IKDC-9, which exceeded the MCID. Tegner inventory scores for the cohort improved by an average of 1.9 activity levels.
There were several limitations of this study, including a small number of patients and relatively short-term follow-up. Pre- and post-operative PROMs were collected on fewer than half of the included patients in the study (8 of 19). This may have introduced bias if the post-operative PROMs collected in the 8 patients were significantly different than the remaining 11 patients who did not complete post-operative PROMs. The study was likely underpowered to detect differences in the PROMs collected. While we can conclude that derotational osteotomy significantly improves patient’s perception of their physical appearance, we cannot conclude that the procedure does not improve any of the other PROMs or sub-categories measured. In addition, we were unable to report on the post-operative resolution of initial indications for surgery. Being that this study was a retrospective review, we were limited to reporting on only the data included in follow-up visit notes. While patients did well post-operatively, not all follow-up notes identified a specific improvement in a patient’s pre-operative symptoms. Despite its limitations, we feel that this study reports useful information.
Our technique for femoral derotational osteotomy in the pediatric population is safe and improves self-image and quality of life in patients with symptomatic femoral version abnormalities. While this study confirms Gordon et al.’s 2 findings that this procedure is safe and effective, further investigation is needed to refine the appropriate indications for the procedure as well as the addition of concomitant tibial procedures.
Conclusion
Our technique of femoral derotational osteotomy as described in the correction of symptomatic rotational deformity in the pediatric population is safe with anticipated improved outcomes for patients. This study confirms previous reports of the effectiveness of this surgical technique. Furthermore, outcome research might better define appropriate indications for the procedure as well as the addition of the concomitant tibial procedures.
Footnotes
Author contributions
All authors specified below contributed meaningfully to the content and design of the study, as well as preparation of the manuscript. All authors agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved. Additional specific contributions of each author can be found below:
Compliance with ethical standards
This study was approved by our institutional review board. This study is a retrospective study of prospectively collected data and is compliant with the Helsinki declaration.
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: S.R.R. is a consultant and receives royalties from Nuvasive and is a consultant for and owns Johnson & Johnson stock. Austin Fragomen is a consultant for Johnson & Johnson, Nuvasive, and Smith & Nephew. None of these disclosures are relevant to this paper. The other authors have no conflicts of interest to disclose.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.