
Abstract
Purpose:
The purpose of this study was to describe gait evolution in patients with unilateral spastic cerebral palsy (USCP) using modified Gait Profile Score (mGPS without hip rotation), Gait Variable Score (GVS), walking speed, and the observed effects of single-level surgery (SLS) after 10 years.
Methods:
Fifty-two patients with USCP (Gross Motor Function Classification System I) and data from two Clinical Gait Analyses (CGAs) were included. The evolution of patients’ mGPS, GVS, and walking speed were calculated. Two “no surgery” and “single-level surgery” patient categories were analyzed. Paired t-tests were used to compare the data between CGAs and as a function of treatment category. Pearson’s correlations were used to examine relationships between baseline values and evolutions in mGPS and walking speed.
Results:
Mean ages (SD) at first and last CGAs were 9.3 (3.2) and 19.7 (6.0) years old, respectively, with an average follow-up of 10.5 (5.6) years. Mean mGPS for the patients’ affected side was significantly lower at the last CGA for the full cohort: baseline = 8.5° (2.1) versus follow-up = 7.2° (1.6), effect size = 0.73, p < 0.001. Significant improvements in mGPS and GVS for ankle and foot progression were found for the SLS group. The mGPS change and mGPS at baseline (r = −0.79, p < 0.001) were negatively correlated.
Conclusions:
SLS patients demonstrated a positive long-term change in gait pattern over time. The group that had undergone surgery had worse gait scores at baseline than the group that had not, but the SLS group’s last CGA scores were relatively closer to those of the “no surgery” group.
Level of evidence:
This was a retrospective comparative therapeutic study (level III).
Keywords
Introduction
Unilateral spastic cerebral palsy (USCP) is the most prevalent cerebral palsy (CP) subtype. 1 It is characterized by alterations in movement coordination, balance impairments, muscle weakness, spasticity, limited selective voluntary motor control, and limited muscle tone regulation affecting lower and upper limb motor function on one side. 2 These alterations directly impact functional abilities, postures, movements, and gait. Nevertheless, most children with USCP walk independently, without assistance. The most common gait disorders observed among USCP patients are foot equinus due to calf-muscle spasticity and contracture, limited knee extension, and femoral or tibial torsions.3,4 Clinical gait analysis (CGA) is generally recommended to establish a functional diagnosis for these patients and to support treatment decision-making.5–9 CGA can also be used to objectively monitor the evolution of patients’ gait quality thanks to specific gait measurement scores such as the Gait Deviation Index (GDI), the Gait Profile Score (GPS), or the Gait Variable Score (GVS). 10 The GPS and the GVS evaluate the difference between the kinematic curves measured during the gait cycles of patients with a gait deviation and subjects with no gait deviations (defined from a normal reference database). 11 These scores are relevant indicators of overall gait pathology (expressed in degrees) for assessing pathological gait characteristics and detecting changes, such as before and after treatment. 12
Several studies in the literature have observed the long-term gait evolution of children with CP, mostly focusing on patients with bilateral CP13–19 and showing improved gait scores thanks to surgery. However, to the best of our knowledge, few published articles have examined the long-term gait evolution of USCP patients. Schranz et al. 20 reported on the long-term outcomes of 14 patients with USCP, but only a specific subgroup who had undergone single-event multilevel surgery (SEMLS). Their GPS were improved by SEMLS and maintained at a 10-year follow-up. The literature lacked long-term, longitudinal gait evolution studies (≥5 years of follow-up) among young adults with USCP, specifically including groups who had and had not undergone single-level surgery (SLS).
Thus, the present study’s first objective was to evaluate long-term gait outcomes, between two CGAs, using the modified GPS (mGPS), the GVS, and the normalized walking speed of a cohort of young adult patients with USCP, regardless of their treatment. The second objective was to describe how long-term gait outcomes differed between the “no surgery” and “SLS” patient groups.
Materials and methods
This ambidirectional cohort study included some data available from a historical CP cohort and some data collected prospectively. The gait function of young adults with ambulant CP was measured at two time points, with a minimum of 5 years between their two CGAs. The study was approved by the local ethics committee (CER: 10–135), and all participants provided their written informed consent.
Patients
Patients with CP who had undergone a CGA between 1993 and 2017 were contacted and asked to participate whether they met the study inclusion criteria: (1) USCP diagnosed by clinical symptoms and medical imaging; (2) being aged between 7 and 14 years old at their first CGA; (3) being aged older than 14 at their last CGA (occurring between 2010 and 2022); (4) a minimum 5-year interval between those CGAs; and (5) being categorized at Gross Motor Function Classification System (GMFCS) level I (Figure 1). Our hospital’s electronic medical database was used to collect patient characteristics such as age, sex, diagnosis, and treatments (e.g. botulinum toxin injection, lower-limb orthotic management, and lower-limb treatment history). Eligible patients were divided into “no surgery” and “SLS” treatment groups.
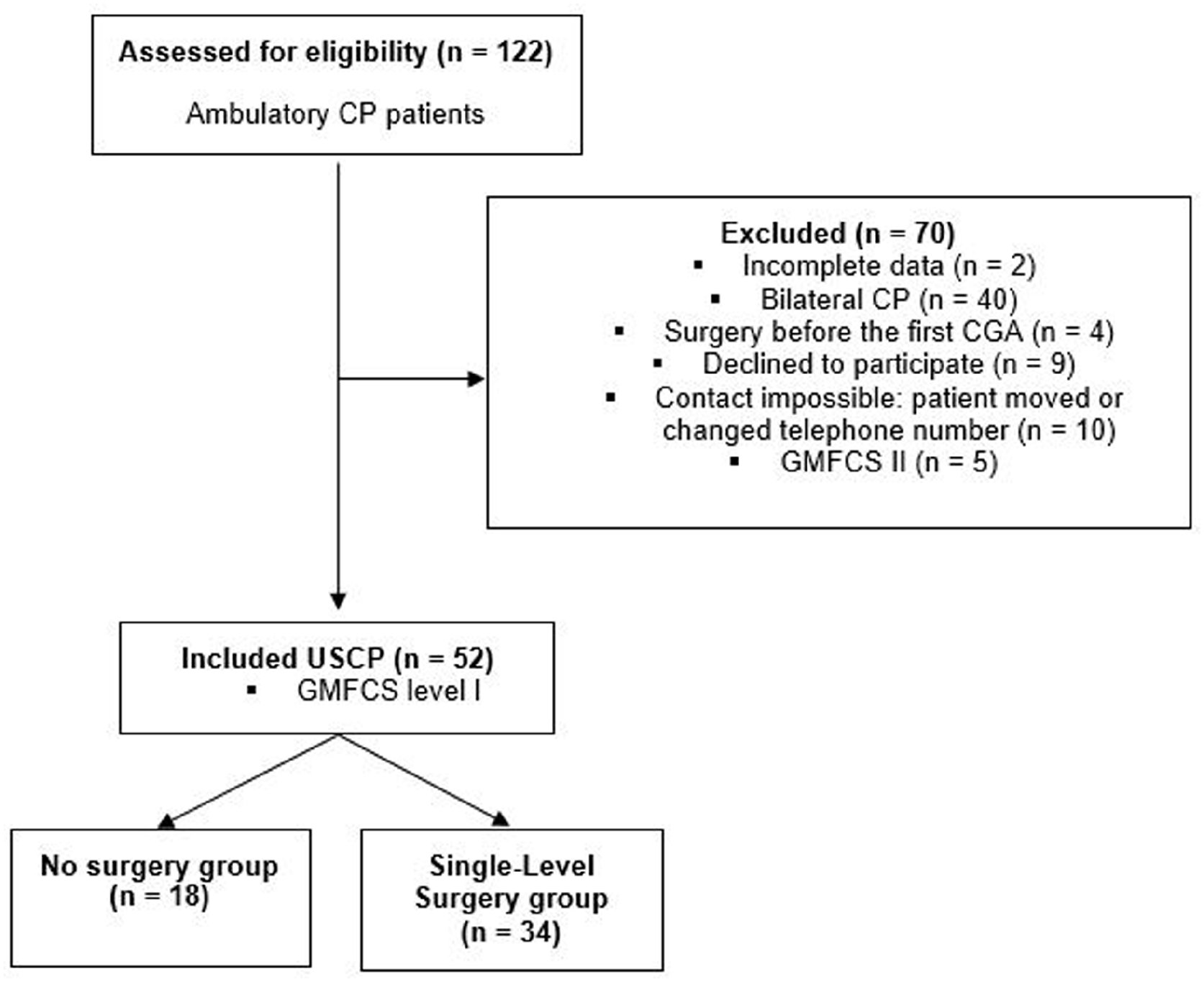
Flow chart of patients with cerebral palsy (CP) as a function of inclusion and exclusion criteria. Definition of three groups as a function of their treatment: no surgery and single-level surgery (SLS).
Objective gait assessment
Three-dimensional motion analysis systems were in use in our institution during the follow-up analysis period. From 1993 to 2008, gait was measured using a six-camera motion analysis system (Vicon 460, UK); from 2008 to 2014, a 12-camera motion analysis system (Vicon Mx3 +, UK) was used; and since 2015, measurements have been made with another 12-camera motion analysis system (Oqus 7+, Qualisys, Sweden). Markers were placed on the lower limbs and pelvis following the Conventional Gait Model. 21 Barefoot gait (at a self-selected speed) was recorded along a 12-m walkway, and a minimum of five gait cycles were used for data analysis. Visual 3D (C-Motion, Inc., Germantown, USA), the open-source Biomechanical ToolKit package, 22 and Matlab R2021b (MathWorks, USA) software were used to compute kinematics, analyze data, and calculate gait scores.
Biomechanical outcomes
The GPS is computed using nine kinematic lower-limb variables (pelvic tilt, obliquity, rotation; hip flexion, abduction, rotation; knee flexion; ankle flexion and foot angle progression) across the gait cycle as the root mean square distance between the patient’s joint kinematic curve and their mean normative curve, expressed in degrees. 11 Schwartz and Rozumalski 23 reference data set (including 83 subjects) was used to compute mGPS scores. The GVS is also calculated using the nine kinematic variables as the root mean square distance from a set of normal reference data, also expressed in degrees. A lower GPS reflects a gait pattern closer to the norm, and Backer et al. 24 determined a minimal clinical important difference (MCID) of 1.6°. However, Barton et al. 25 recently recommended excluding hip rotation from the calculation of gait scores as this parameter is less reliable than the others. Based on this, we calculated a modified GPS (mGPS) without the hip joint rotation angle. Thus, the mGPS was our main outcome characteristic of patient gait quality over time. In addition, to evaluate SLS’s post-operative impact on gait in more detail, GVS were also calculated over time (except for the hip rotation outcome). Subsequent analyses calculated the mGPS and GVS for the affected side and mGPS for the unaffected side. The follow-up mGPS minus the baseline mGPS was calculated and called the mGPS change. Finally, dimensionless walking speed 26 was analyzed at the first and last CGAs, and follow-up dimensionless walking speed minus baseline dimensionless walking speed was calculated and called the change in dimensionless walking speed.
Clinical outcomes
Gross motor function was determined using the GMFCS. 27 For patients whose first CGA was before 1997, the GMFCS level was evaluated from the videos of gait and functional movements recorded during those analyses. The classification proposed by Rodda and Graham 28 was also used to classify the cohort’s gait patterns.
Data analysis
Because the full cohort’s data were normally distributed, means and standard deviations (SD) were calculated to describe them. A two-tailed, dependent Student’s t-test was calculated for paired samples to compare mGPS, GVS, and walking speeds at the first and last CGAs for the full cohort and for the “no surgery” and “SLS” groups. Pearson’s correlations were calculated to assess relationships between mGPS changes and mGPS at baseline on the affected side and between changes in walking speed and walking speed at baseline. Correlation coefficients of 0.0–0.3 were considered weak, >0.3–0.5 fair, >0.5–0.7 good, and >0.7 high. 29
To interpret these results, Cohen’s effect sizes were calculated as the mean unadjusted differences divided by the pooled SD of the corresponding mean parameters. 29 An effect size of r < 0.2 is considered trivial, 0.2 ≤ r ≤ 0.5 is small, 0.5 < r ≤ 0.8 is moderate, and r > 0.8 is large. Statistical analyses were performed using STATA software, version 13.1 (StataCorp LP, College Station, Texas, USA), and R software, version 1.4.1106 (R Foundation for Statistical Computing, Vienna, Austria, URL https://www.R-project.org). Statistical significance was set at p < 0.05 (two-sided).
Results
Patient cohort characteristics at baseline and follow-up CGAs
The study included 52 USCP patients (27 males), with a mean interval between CGAs of 10.5 (5.2) years. Mean ages at the first and last CGAs were 9.3 (3.2) and 19.7 (6.0) years old, respectively. Eighteen patients had not undergone SLS because they had no clinical indication at baseline. Thirty-four patients underwent SLS because of tendon shortening, muscle disbalance in the foot, torsion malalignment of the femur and tibia, or lever arm dysfunction of the foot.
Table 1 details each patient’s clinical characteristics and the treatments they underwent during the follow-up period. Table 2 summarizes patients’ parameters at their first and last CGAs. Supplementary Table 1 details each patient’s sex, side of USCP, age at first and last CGA, the interval between CGAs, mGPS of the affected side, normalized walking speed, main gait deviations at the first and last CGAs, as per Nieuwenhuys et al. 30 and their Rodda Classification. 28
Individual characteristics and treatments at each clinical gait analysis.
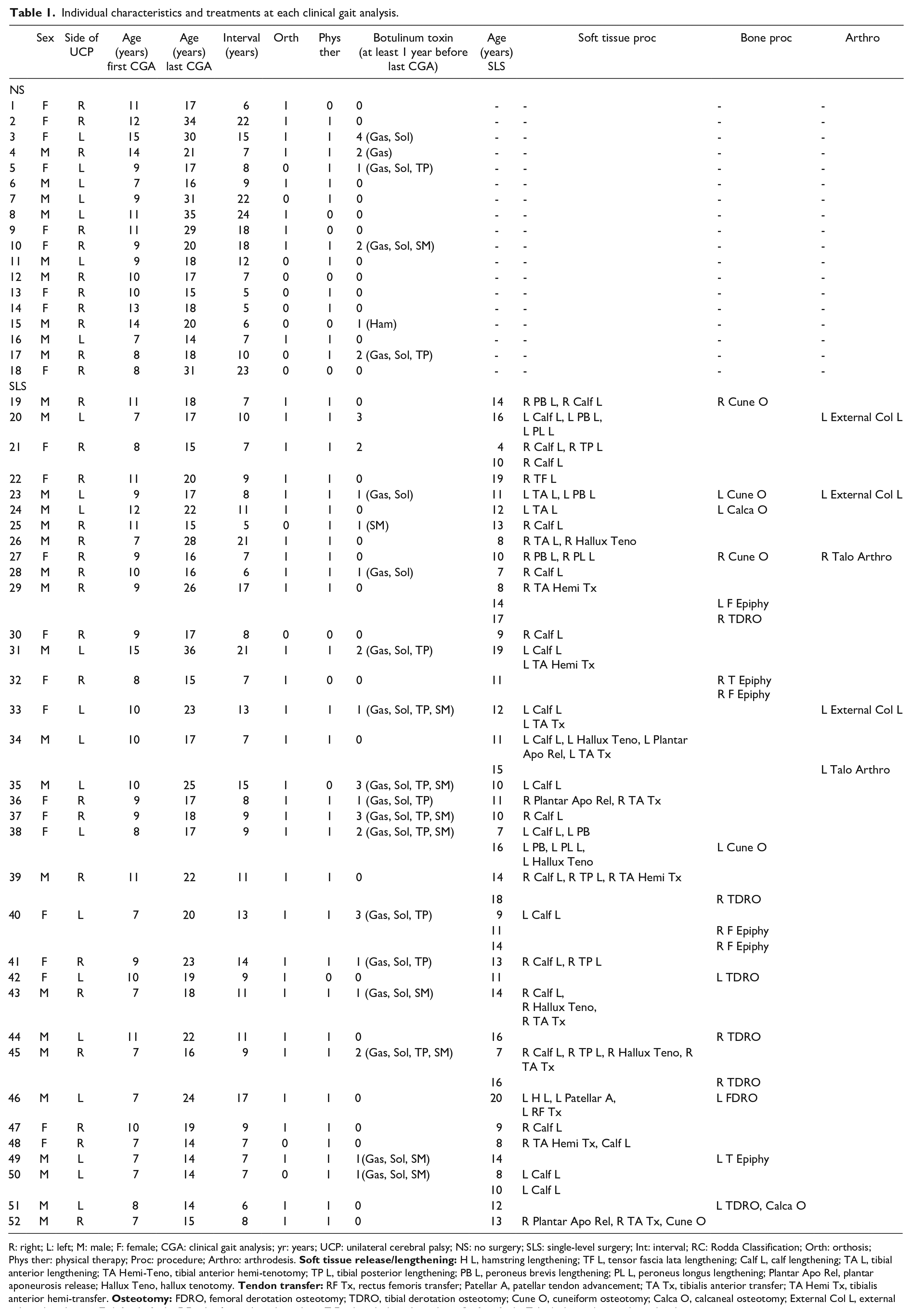
R: right; L: left; M: male; F: female; CGA: clinical gait analysis; yr: years; UCP: unilateral cerebral palsy; NS: no surgery; SLS: single-level surgery; Int: interval; RC: Rodda Classification; Orth: orthosis; Phys ther: physical therapy; Proc: procedure; Arthro: arthrodesis.
Patient characteristics for the full cohort (mean, effect size, and standard deviation (SD)) with proportions for sex and Gross Motor Function Classification System (GMFCS) level.
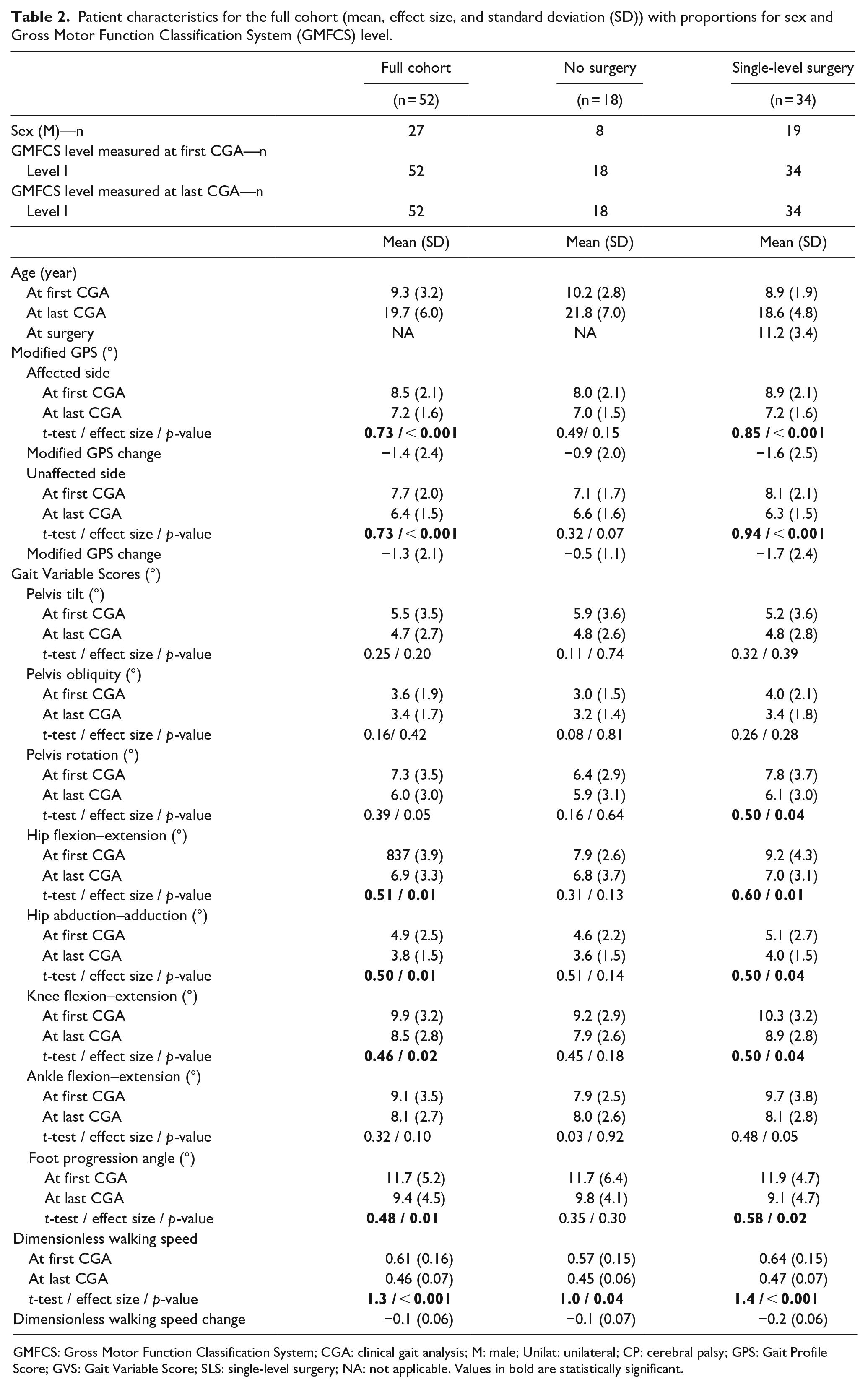
GMFCS: Gross Motor Function Classification System; CGA: clinical gait analysis; M: male; Unilat: unilateral; CP: cerebral palsy; GPS: Gait Profile Score; GVS: Gait Variable Score; SLS: single-level surgery; NA: not applicable. Values in bold are statistically significant.
mGPS, GVS, and walking speed changes from baseline to follow-up CGA for the full cohort
The mean mGPS for the affected side was lower at the last CGA: baseline = 8.5° (2.1°) versus follow-up = 7.2° (1.6°), effect size = 0.73, p < 0.001, with a mean mGPS change of −1.4° (2.4°). Mean GVS at the last CGA were significantly improved for hip abduction–adduction angle, hip and knee flexion–extension angle, and foot progression angle (Table 2). Significant decreases in mean dimensionless walking speeds were also observed. The unaffected side’s mean mGPS was also significantly lower at the last CGA: baseline = 7.7° (2.0°) versus follow-up = 6.4° (1.5°), effect size = 0.73, p < 0.001, with a mean mGPS change of −1.3° (2.1°). Concerning the mGPS changes, no significant differences were observed between the affected and unaffected sides: −1.4° (2.4°) versus −1.3° (2.1), respectively, p = 0.175. Pearson correlations showed significant negative correlations between mGPS change and mGPS at baseline (r = −0.79, p < 0.001) and between walking speed change and walking speed at baseline (r = –0.77, p < 0.001).
mGPS and dimensionless walking speed at baseline and follow-up among “no surgery” and “SLS” patients
No significant differences were observed between the two groups, at baseline and at follow-up, in terms of their mGPS: baseline “no surgery” = 8.0° (2.1°) versus baseline “SLS” = 8.9° (2.1°), p = 0.15; follow-up “no surgery” = 7.0° (1.5°) versus follow-up “SLS” = 7.2° (1.6°), p = 0.74. No significant differences were found between the two groups for dimensionless walking speed at baseline or follow-up.
mGPS, GVS, and dimensionless walking speed changes among “no surgery” patients
The 18 “no surgery” patients’ characteristics are summarized in Tables 1 and 2. Significant changes were only found for dimensionless walking speed (baseline: 0.57 (0.15) versus follow-up: 0.45 (0.06), p = 0.04). No significant changes were observed for the mGPS of the affected side (baseline: 8.0° (2.0°) versus follow-up: 7.0° (1.5°), p = 0.15), the unaffected side, or the GVS during this period of follow-up.
mGPS, GVS, and dimensionless walking speed changes among “SLS” patients
The 34 “SLS” patients’ characteristics are summarized in Tables 1 and 2. Significant improvements were observed in the affected side’s mGPS (Figure 2) (baseline = 8.9° (2.1°) versus follow-up = 7.2° (1.6°), effect size = 0.85, p < 0.001) and the unaffected side’s mGPS (baseline = 8.1° (2.1°) versus follow-up = 6.3° (1.5°), effect size = 0.94, p < 0.001). However, no significant differences were observed for the mGPS change between the affected and unaffected sides, with −1.6° (2.5°) versus −1.2° (2.4°), respectively, p = 0.348. Significant improvements were observed for the mean GVS of the pelvis rotation angle, hip and knee flexion–extension angles, and the foot progression angle. Finally, significant changes were observed in mean dimensionless walking speed (baseline: 0.64 (0.15) versus follow-up: 0.47 (0.07), effect size = 1.4, p < 0.001).
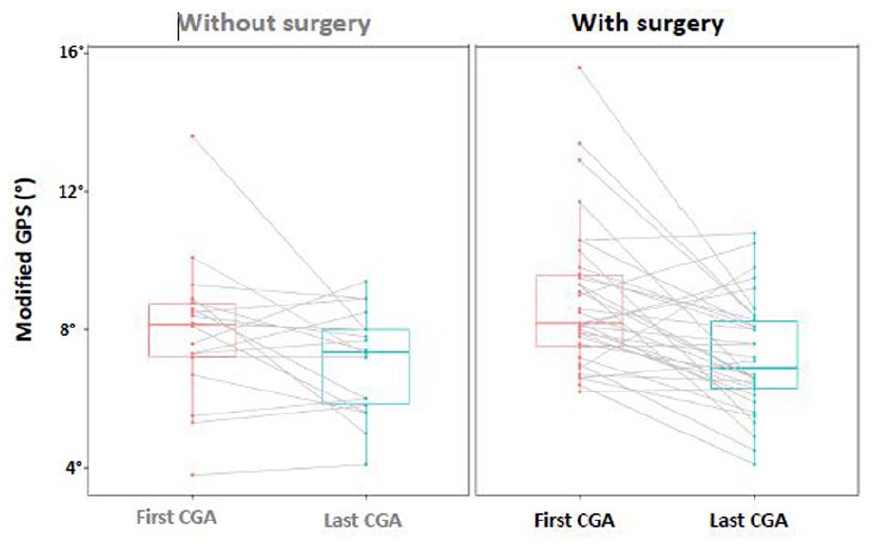
Boxplot for the modified GPS between the “no surgery” patient group and the “single-level surgery” patient group for each clinical gait analysis (first and last CGA).
Discussion
The present study’s main objective was to observe long-term gait outcomes among USCP patients. After a mean follow-up of 10.5 years, most patients had improved or remained stable, regardless of surgery. Furthermore, patients with a poorer initial level of gait function and efficacy at baseline showed greater improvements over time, which was reflected in the strong correlation found a significant negative correlation between change in the mGPS and gait speed at baseline CGA: r = −0.79, p < 0.001. Similar results were observed in previous publications.14,31
Examining this study cohort in more detail, only 18 patients had not undergone surgery after their initial CGA. We observed improvement or stabilization in the “no surgery” treatment group’s mGPS on both their affected and unaffected sides but with no significant overall difference (Table 2). The same observation was made for the GVS of affected sides during this transition period to young adulthood (Table 2). A unique significant difference was observed for the walking speed between the two CGAs. Furthermore, most “no surgery” patients had small drop foot and/or internal foot progression angles (in-toeing gait) at their baseline CGA (Supplementary Table 1), sometimes exhibiting a natural improvement in these angles over time. However, it is important to note that most “no surgery” patients had benefited from childhood physiotherapy and/or ankle or foot orthosis to manage their main ankle- or foot-based gait deviations. 32 Similarly, four patients received botulinum toxin injections during childhood. Information on this subgroup is precious for better understanding this pathology’s prognosis as it shows that the natural evolution of some USCP patients can be favorable even without surgery. It is important to note that they had low-level gait impairments at baseline, which somewhat biases the results concerning the so-called natural evolution of USCP patients. Although this is usually why these patients did not need surgery, it is important to remember that it could also be a patient or family choice. Indeed, it is the patients with more severe impairments who usually undergo surgery.
The mean mGPS of the affected sides of the 34 patients in this cohort who underwent SLS improved significantly over time, with a strong effect size (Table 2). Supplementary Table 1 reveals that 18 patients showed a significant improvement in mGPS, 15 remained stable, and only 1 patient had a worse mGPS at their last CGA. Moreover, at the joint level, all the GVS on patients’ affected sides also improved, but only significantly for hip, knee, and ankle flexion–extension and for the foot progression angle. Finally, the effect sizes of these gait parameters reflected surgery’s moderate-to-large effect on gait quality. Furthermore, the mean mGPS of patients’ unaffected sides also improved significantly in this group, showing SLS’s impact on the voluntary coping and compensatory mechanisms developed on that side, too.33–36 We also noted that the mGPS changes for the affected and unaffected sides of the SLS group were similar. Regarding Table 1, the most used types of surgical procedure were muscle/tendon lengthening (e.g. tibialis posterior, gastrocnemius, Achilles tendon), the transfer or hemi-transfer of the tibialis anterior, calcaneal and cuneiform osteotomies, tibial or femoral derotational osteotomies, and epiphysiodesis. Orthopedic surgeons indicate which types of surgery are needed (depending on the type and severity of the CP), with, in most cases, the primary objective of managing USCP patients’ gait impairments in their ankles and feet (e.g. drop foot, equinus, in-toeing or out-toeing gait).19,37 These results accord with Schranz et al.’s, 20 which showed significant improvements in GPS after a 10-year follow-up of 14 patients with USCP who underwent SEMLS. They also found that GVS were significantly better for foot progression angle, ankle, knee, and hip flexion–extension angles, and (contrary to the present study) pelvis rotation. These differences might be explained by the fact that their cohort of USCP patients was different in terms of the surgeries undergone and the levels of function. Indeed, Schranz et al.’s subjects underwent SEMLS at around 12.1 years old and were GMFCS levels I and II, whereas, in the present study, patients had undergone their SLS at a mean age of 11.1 years old (95% CI, 9.6–12.6) and were only GMFCS level I (Table 1).
It is interesting to note that the only significant difference between our two groups was observed in the mean increase in dimensionless walking speed in the last CGA, with no other significant differences observed at baseline and follow-up in terms of their mGPS. This observation could indicate that, over time, patients who undergo surgery achieve the ability to walk as efficiently as patients who did not require SLS.
We found similar results in a previous study of the long-term evolution (10.5 years of follow-up) of gait in patients with bilateral CP. This revealed that patients who did not undergo surgery and had good gait function at baseline (10 patients at GMFCS level I) maintained their gait quality, whereas patients who underwent SEMLS (18 patients at GMFCS levels I and II) showed—in the majority of cases—improved gait quality at follow-up. 14 Thus, for both USCP and bilateral CP patients, the long-term beneficial impacts of surgery on gait quality are noteworthy, as measured using mGPS and GVS.
The present study had some limitations, the main one being the cohort’s small size. However, compared with similar studies of the long-term evolution of gait among USCP patients, it was the largest sample analyzed to date.8,20 The second limitation was that it only included patients at GMFCS level I. This choice was made because this was the level of most of the eligible patients with USCP at baseline; it provided a more homogeneous final cohort and more consistent results. The third limitation results from there being no prior MCID for the mGPS available in the literature. However, as hip rotation has been shown to be the least reliable parameter calculated from 3D kinematics, we would expect the MCID for the mGPS to be lower than those of 1.6° calculated in the literature.24,25 The fourth limitation concerns the reference database of subjects used to calculate mGPS. These data came from another gait laboratory and could be different in terms of population and marker placements, even if the laboratories used an identical biomechanical model. Finally, patients were not randomly allocated to one of the two treatment groups.
In conclusion, the present study highlighted that most USCP patients maintained or improved their gait function and abilities during their transition from childhood to young adulthood. Moreover, it revealed that the majority who were selected for single-level surgery had improved gait scores, and these were maintained over time.
This study filled a gap in the knowledge about the long-term longitudinal evolution of USCP patients, which remains poorly covered in the literature. Future studies aiming to refine our knowledge would benefit greatly from larger cohorts and being able to examine more parameters, taking into account different domains of the International Classification of Functioning, Disability and Health, such as participation, personal parameters, social well-being, and environmental factors. 38
Supplemental Material
sj-docx-1-cho-10.1177_18632521231154975 – Supplemental material for A 10.5-year follow-up of walking with unilateral spastic cerebral palsy
Supplemental material, sj-docx-1-cho-10.1177_18632521231154975 for A 10.5-year follow-up of walking with unilateral spastic cerebral palsy by Alice Bonnefoy-Mazure, Geraldo De Coulon, Pierre Lascombes, Aline Bregou and Stéphane Armand in Journal of Children’s Orthopaedics
Research Data
sj-xlsx-2-cho-10.1177_18632521231154975 – Supplemental material for A 10.5-year follow-up of walking with unilateral spastic cerebral palsy
Supplemental material, sj-xlsx-2-cho-10.1177_18632521231154975 for A 10.5-year follow-up of walking with unilateral spastic cerebral palsy by Alice Bonnefoy-Mazure, Geraldo De Coulon, Pierre Lascombes, Aline Bregou and Stéphane Armand in Journal of Children’s Orthopaedics
Research Data
sj-xlsx-3-cho-10.1177_18632521231154975 – Supplemental material for A 10.5-year follow-up of walking with unilateral spastic cerebral palsy
Supplemental material, sj-xlsx-3-cho-10.1177_18632521231154975 for A 10.5-year follow-up of walking with unilateral spastic cerebral palsy by Alice Bonnefoy-Mazure, Geraldo De Coulon, Pierre Lascombes, Aline Bregou and Stéphane Armand in Journal of Children’s Orthopaedics
Footnotes
Acknowledgements
This work received statistical and other support from the University of Geneva’s and Geneva University Hospitals’ Clinical Research Center.
Author contributions
Alice Bonnefoy-Mazure: study design, literature review, data acquisition, data analysis and interpretation, and manuscript writing. Geraldo De Coulon: fundraising, data interpretation, and critical revision of the article’s important intellectual content. Pierre Lascombes: critical revision of the article’s important intellectual content. Aline Bregou: critical revision of the article’s important intellectual content. Stéphane Armand: fundraising, protocol development, data analysis and interpretation, and critical revision of the article’s important intellectual content.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by Geneva University Hospitals and the University of Geneva.
Informed consent
This study followed the ethical standards of Geneva University Hospitals’ institutional research committee and those of the 1964 Declaration of Helsinki. All patients provided written informed consent.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.