
Abstract
Kimura’s disease is a rare, chronic inflammatory condition with a high recurrence rate, primarily affecting young to middle-aged Asian males. It typically manifests as masses in the head and neck, accompanied with regional lymphadenopathy. This report describes the case of a 50-year-old man initially diagnosed with Kimura’s disease 13 years ago, following surgical removal of a left submandibular mass. Subsequent recurrences involved the parotid and contralateral submandibular regions, requiring radiotherapy and intermittent oral prednisone therapy. After 6 years, he developed progressive proptosis and visual impairment, revealing multiple orbital masses bilaterally. A puncture examination of the left submandibular mass was indicative of Kimura’s disease. Throughout the follow-up period, the eosinophil levels correlated with prednisone use. This case highlights the disease’s capacity for multisite recurrence within the head and neck over an extended duration. The extensive orbital involvement without renal manifestations is a rare presentation. Long-term follow-up is crucial in Kimura’s disease management, and oral prednisone can effectively control disease progression.
Background
Kimura’s disease (KD), also known as eosinophilic hyperplastic lymphogranuloma, was first reported in 1937 by a Chinese surgeon,
1
Dr. Xianzhai Jin, and then systematically described in 1948 by the Japanese scholars Kimura and Ishikawa.
3
It was later widely known as KD. KD mainly occurs in the head and neck region, often causing facial asymmetry, and affecting the esthetic appearance.
3
In this case, the patient has had multiple occurrences of KD in different sites of the head and neck over a period of 13 years. Initial onset was treated by surgical removal, followed by 2 months of radiotherapy, after which the disease was controlled by intermittent hormone therapy
The clinical data used in this study were published after obtaining written informed consent from the patient. The study was approved by the Ethics Committee of the Affiliated Hospital, Yanbian University (ethical approval number: 2024149). This report conforms to the Case Report (CARE) guidelines.
Case presentation
In December 2010, a 50-year-old man presented to the Affiliated Hospital of Yanbian University with a painful mass in the left submandibular region for 10 months. Clinical examination revealed a mass of approximately 2.5 cm × 2.5 cm in size palpable under the left mandible with medium texture, clear boundaries, fair mobility, and tenderness to palpation (Figure 1). He had no history of food or drug allergy and had a high eosinophil ratio (EOS%). Computed tomography (CT) revealed that the left submandibular gland was enlarged with slightly increased density and irregular shape. There were various sizes of round soft tissue shadows around the gland, the largest of which was approximately 2.4 cm in diameter, and the boundary with the submandibular gland was not clear (Figure 2). The left submandibular mass and submandibular gland were surgically removed (Figure 3), and the postoperative pathological diagnosis was KD (Figure 4). Two months later, he presented a mass (approximately 5 cm × 6 cm in size) under the left mandible accompanied with ipsilateral cervical lymphadenopathy, and his EOS% was high with a normal eosinophil count (EOS#). After 1 month of radiotherapy, the mass was reduced to a size of 4 cm × 5 cm. The patient underwent a total of 25 radiotherapy sessions with a dose of 30 Gy; he was treated with prednisone (30 mg daily), and the dose was reduced to 5 mg every 5 days until attaining a dose of 10 mg. The tumor was controlled. Subsequently, long-term prednisone acetate was used, with the dose increasing from 5 to 15 mg and then to 25 mg. In 2012, a mass appeared in the left parotid gland. During this time, the patient stopped the medication on his own and developed symptoms such as sniffles, excessive phlegm, sneezing, and visual impairment. These symptoms were gradually alleviated after resuming the medication. A year later, a mass was found in the right submandibular region. At this time, the masses in the left parotid gland and submandibular region were significantly smaller than those detected previously, and puncture pathology of the mass in the left submandibular region was indicative of KD.

Preoperative facial photographs.

Plain computed tomography of the neck.

Glands and masses removed during surgery.

Postoperative pathology (hematoxylin and eosin staining, 400×). Follicular hyperplasia was noted in the left submandibular lymph node, a large number of eosinophil infiltrates were observed in the paracortical area between the follicles and capsule, and the capsule was thickened and the surrounding salivary gland was infiltrated by lymphocytes.
In 2016, the patient experienced mild protrusion and vision loss in his left eye. A test revealed a visual acuity of 1.2 in the right eye and 0.1 in the left eye. The patient was diagnosed with cataracts; however, orbital magnetic resonance imaging (MRI) revealed no obvious abnormalities (Figure 5). The EOS% and EOS# were higher than the normal levels. Two years ago, after stopping the medication for a few days, the patient experienced significant protrusion and severe vision loss of the left eyeball; at that time, the visual acuity was 1.0 in the right eye and 0.02 in the left eye. Orbital CT (Figures 6–7) and MRI (Figure 8) revealed six tumors in the left orbit and three tumors in the right orbit, which were consistent with the findings of KD in combination with the medical history. After resuming medication in October of the same year, the EOS% and EOS# values returned to normal. The immunoglobulin (Ig) G level was 1628.17 mg/dL, IgG4 level was 10.2 g/L, and the gamma interferon release was 56.9 pg/mL. The Epstein–Barr virus-encoded small RNA (EBER) in situ hybridization method yielded a negative result. Over the past 13 years, the patient has been taking oral prednisone acetate intermittently. The dosage was 15 mg once daily and did not exceed 25 mg during severe illness. The patient was also taking other medications, including liver protection tablets, leucogen, adenine phosphate tablets, batilol, and vitamin B6. Discontinuation of each medication resulted in decreased vision, and the vision improved after resuming medication. In March 2024, the patient was treated for an ocular mass at Beijing Tongren Hospital with the following treatment protocols: intravenous methylprednisolone (80 mg/day for 3 days, 40 mg/day for 1 day), sequential oral prednisone acetate (50 mg/time once daily), combined with oral mycophenolate mofetil capsules (375 mg/time twice daily). Four days later, the left exophthalmos was significantly improved, without eye pain, eye distension, blurred vision, and other discomfort. The patient was satisfied with the effect of the current drug treatment, which resolved the obvious eye swelling and vision loss; he reported no physical discomfort. He preferred hormone therapy over surgical treatment. Figure 9 shows the appearance of the orbit before treatment (Figure 9). Figure 10 shows the appearance of the eyes half a month after treatment (Figure 10). Figure 11 shows the timeline of the patient’s disease progression (Figure 11).

Orbital magnetic resonance imaging-1. The bilateral eyeball morphology was normal, the left eyeball protruded slightly more anteriorly than the right eyeball, there was no obvious abnormal signal shadow in the orbit, the lens was in place, the optic nerve was not altered, and the left subocular rectus muscle was thickened.
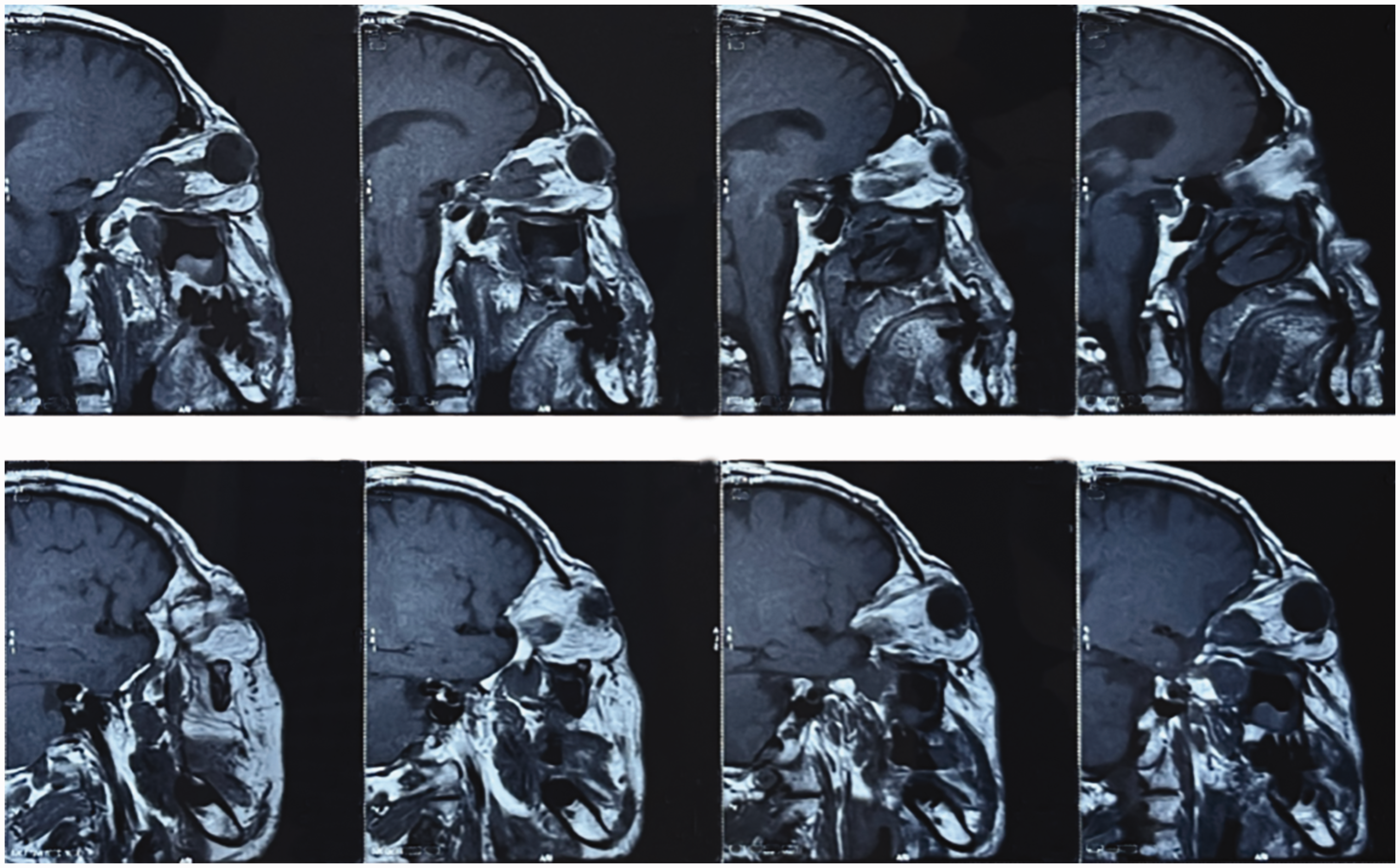
Orbital magnetic resonance imaging-2.
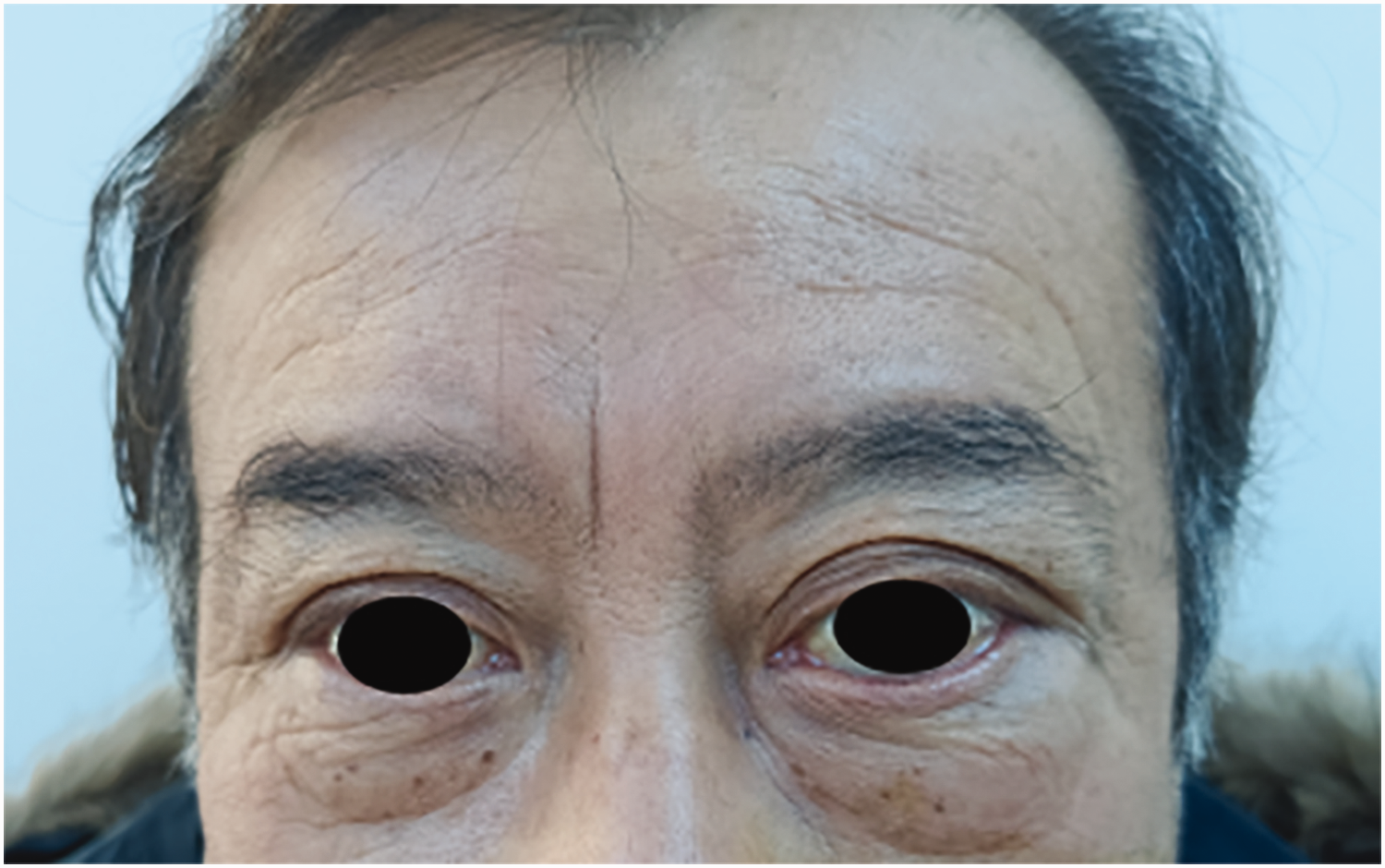
Findings before treatment (29 January 2024).
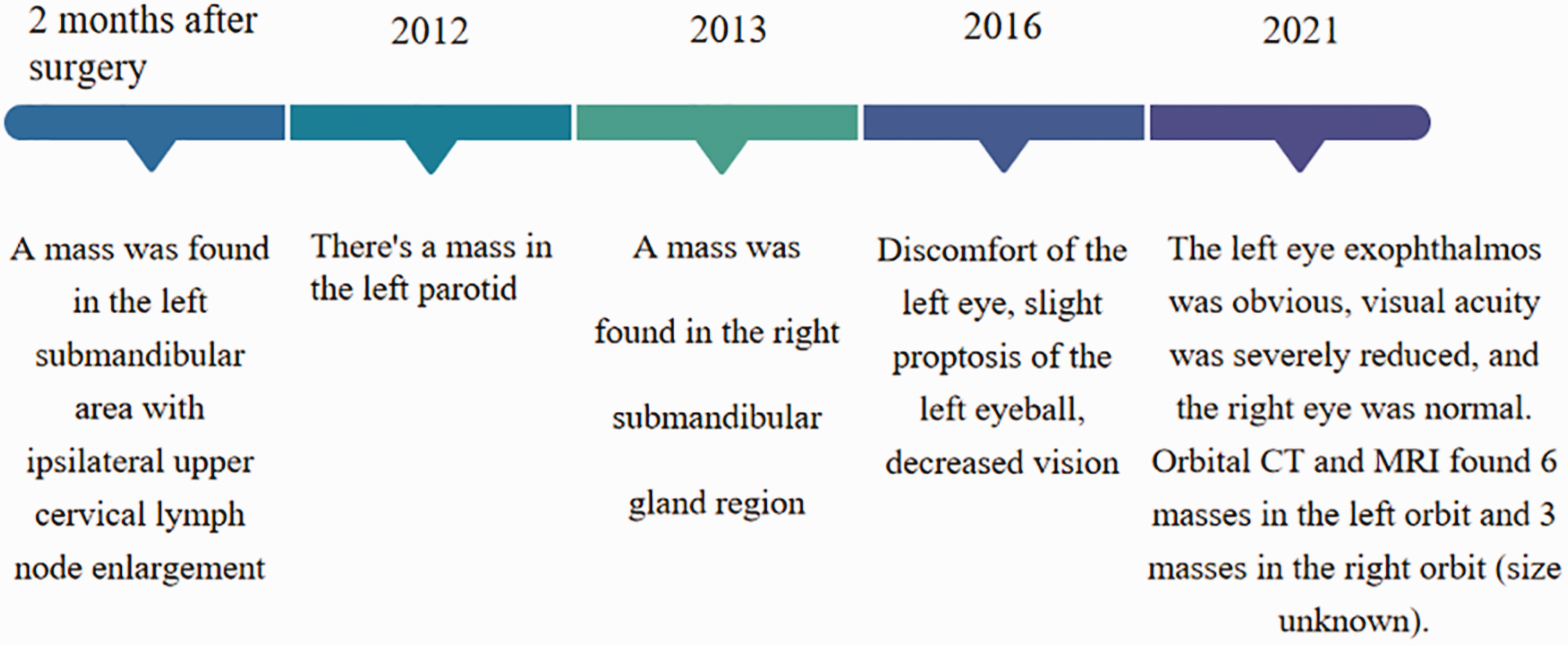
Timeline of disease progression.

Sagittal orbital computed tomography. The left optic nerve was partially thickened, and a soft tissue mass was observed in the posterior frame of the eyeball, approximately 2.8 cm × 1.6 cm in size, with smooth edges and unclear boundaries with the optic nerve. The left eyeball protruded slightly outward, with uniform intrabulbar density. The right eye ring was continuous and complete, the shape of the eyeball was normal, the density of the bulb was uniform, the lens was in place, the anterior chamber was clear, the density of the extraocular muscles was uniform, there was no swelling, no obvious abnormality was observed in the interruption of the right optic nerve, and the retrobulbar fat gap was clear.

Horizontal orbital computed tomography.
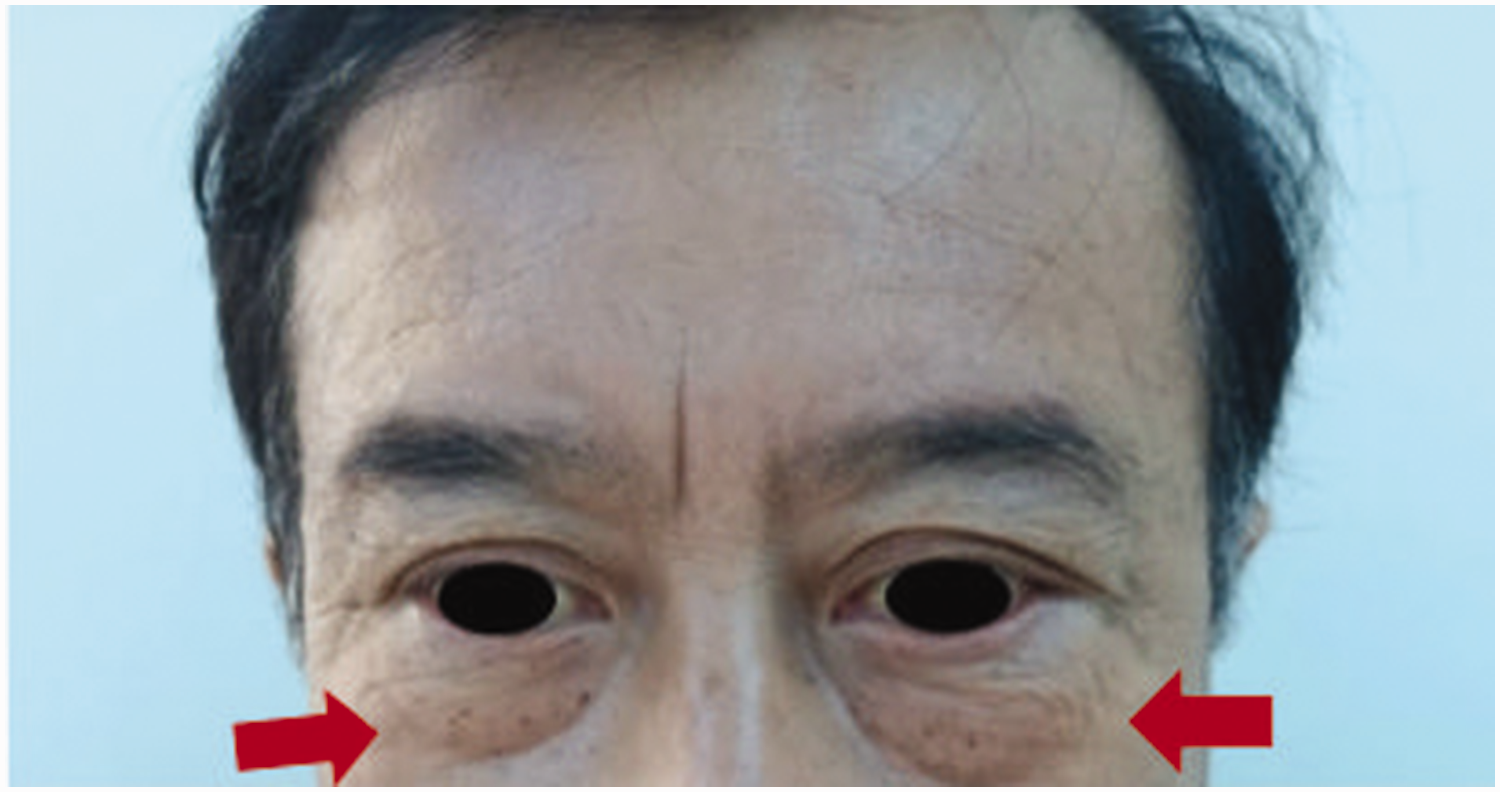
Findings after treatment (14 February 2024). Bilateral eye asymmetry, swelling of the skin around the left eye with normal color, and protrusion of the left eyeball were observed.
Discussion and conclusion
KD predominantly occurs in Asian males aged between 20 and 50 years with a male-to-female ratio of 3.5 to 9:1. 5 It occurs mainly in the head and neck, particularly in the parotid region, and sometimes outside the trochlea, in the axilla, and in the gingiva and epiglottis. 6 KD is often associated with nephrotic syndrome 7 ; however, in this case, the patient never developed kidney disease. In 2022, color ultrasound of both kidneys revealed that “the contour of both kidneys was clear, the size and shape were normal, the lower cortex area of the right kidney showed strong echo spots, the remaining cortex echoes were uniform, the collecting area was not separated, the upper ureter was not dilated, and color Doppler blood flow imaging: blood flow distribution was normal.”
The laboratory findings of KD generally include elevated peripheral blood eosinophil and serum IgE levels. Histological characteristics of KD include lymphoid follicular hyperplasia with enlarged germinal centers, eosinophilic infiltration, accumulation of eosinophilic microabscesses, and capillary and small vein proliferation surrounded by circular collagen fiber deposition and fibrosis. 3 The diagnosis of KD is based on the triad of painless unilateral cervical lymphadenopathy or subcutaneous mass in the head and neck region, characteristic histologic features, blood eosinophilia, and markedly elevated serum IgE levels. 3
In this case, a positive γ-interferon release test and high IgG4 level were detected for Mycobacterium tuberculosis 2 years ago, and the diagnosis of KD was still made based on the medical history and existing histopathological examination. A negative EBER in situ hybridization test indicated that the disease was not caused by Epstein–Barr virus.
Surgical resection of the mass is the mainstay of treatment for KD, and surgical resection alone is prone to recurrence. Ye et al. believed that surgical resection combined with radiotherapy is associated with the lowest recurrence rate.2–14 The rate of local recurrence caused by surgery, drugs, radiotherapy, and combination therapy ranges from 41.2%–100.0%.15–17 According to previous reports, surgical resection combined with adjuvant therapy is recommended for patients with tumors ≥3 cm in diameter, duration of symptoms of ≥5 years, peripheral blood EOS% of ≥20%, and serum IgE levels of ≥10,000 IU/mL. 18 Patients with recurrent, recalcitrant KD or renal disease can be treated with steroids and cyclosporine. According to the 13-year analysis of the patient’s eosinophil levels (Table 1), the following patterns were elucidated: at the beginning of the disease, increased eosinophilia is observed; with oral prednisone acetate treatment, eosinophilia can be maintained in the normal range; the discomfort symptoms worsen after stopping the drug; and the EOS results are high. Unfortunately, serum IgE levels were not measured since the onset of the disease; thus, changes in this indicator could not be determined.
Changes in the eosinophilic ratio and count from 2010 to 2022.

Note: Reference range of the eosinophil ratio (0.5%–5.0%)
Reference range of the eosinophil count (0.02–0.52 × 109/L).
In conclusion, histopathological examination is required to confirm the diagnosis of KD, and this study reports a rich clinical case, in which the patient demonstrated recurrence of masses in multiple sites in the head and neck over the past 13 years. Thus, long-term follow-up of patients with KD is extremely necessary. Long-term oral prednisone acetate treatment can control the development of KD, and the patient’s medication dose should be monitored. For multiple KD, surgery combined with radiotherapy or drug combined with radiotherapy should be considered.
Footnotes
Acknowledgments
The authors have no acknowledgments to declare.
Authors’ contributions
Study concept and design: Xuan Yun-Ze.
Acquisition of data: Li Rui-Si.
Analysis and interpretation of data: Li Rui-Si and Zhang Xiang-Zi.
Drafting of the manuscript: Li Rui-Si and Quan Yu-Hua.
Critical revision of the manuscript: Xuan Yun-Ze, Li Rui-Si, Zhang Xiang-Zi, and Quan Yu-Hua.
All authors have read and approved the final manuscript.
Consent for publication
Written informed consent for the publication of clinical details and images was obtained from the patient.
Data availability statement
The datasets used and analyzed during the current study are available from the corresponding author upon reasonable request.
Declaration of conflict of interest
The authors declare no conflict of interest.
Funding
This study was not sponsored or funded by any organization.