
Abstract
Background:
Osteochondral lesions of the talus are uncommon in children and adolescents. Surgical procedures differ from those used for adults to avoid iatrogenic physeal injuries. This study aimed to evaluate the clinical and radiological outcomes of surgical treatment in pediatric patients with osteochondral lesions, specifically investigating the patient age and the status of distal tibial physis as factors associated with surgical success.
Methods:
We retrospectively reviewed 28 patients who had symptomatic osteochondral lesions of the talus that were treated surgically between 2003 and 2016. If the lesion was stable and articular cartilage was intact, retrograde drilling was performed under fluoroscopic guidance. Lesions with detached overlying cartilages were treated by debridement of the cartilage combined with microfracture and drilling. Radiographic outcomes, American Orthopaedic Foot & Ankle Society ankle-hindfoot score, and skeletal maturity were evaluated.
Results:
Radiological improvement was observed in 24 (24/28, 86%) patients and complete and incomplete healing in 8 and 16 patients, respectively. Changes in pain grades, American Orthopaedic Foot & Ankle Society scores, and radiological healing after surgery were significant (pain grade, p < 0.001; American Orthopaedic Foot & Ankle Society, p = 0.018; radiological healing, p < 0.001). In addition, patients in the younger age group (≤13 years) showed greater improvements in pain grades than older patients (p = 0.02). Improvement in pain grade after surgery was better in the skeletally immature group than in the skeletally mature group (p = 0.048).
Conclusion:
Clinical and radiological improvements were observed after surgical treatment. The younger age group and open physis group showed more pain improvement.
Level of evidence:
Therapeutic level IV.
Introduction
Osteochondral lesion of the talus (OLT) is defined as a separation of a fragment of articular cartilage, with or without subchondral bone, and frequently occurs after an inversion ankle sprain. 1 OLT is a rare disease in children and adolescents. According to Kessler et al., 2 the incidence of OLT in patients aged 6–19 years is 4.6 per 100,000 individuals. However, the prevalence of OLT in children and adolescents has been increasing because of increased sports activities in this population. 3
After Berndt and Harty introduced the staging system for OLT, 4 most studies have used this system to grade the lesions of the talus and have suggested treatment based on the grade. Canale et al. 5 suggested that grade 1, 2, and 3 (medial) lesions should be managed conservatively, while stage 3 (lateral) and 4 lesions should be managed surgically. Furthermore, they stated that stage 1 and 2 lesions that fail to respond to conservative treatment should be managed surgically. 3
However, the results of conservative treatment in OLT patients are controversial. Lam et al. 6 reported a 100% success rate of conservative treatment, while a systemic review of 14 studies found only a 56% good or excellent rate of nonsurgical treatment in chronic symptomatic OLT. 7 Reilingh et al. 8 reported that 92% of children (mean age = 13 years) who were managed conservatively eventually required surgery. Letts et al. 9 retrospectively analyzed the success rate of conservative treatment of OLT in 23 children with a mean age of 13.4 years (range = 6 years 7 months to 17 years 1 month) and reported good results in only 9 children (39%) who were conservatively managed. Despite published studies in which surgical treatment was attempted more actively, there is still a paucity of literature on surgical outcomes in pediatric OLT.10–12 In particular, reports comparing surgical outcomes in mature and immature OLT patients are few. 10
This study aimed to evaluate the surgical outcomes in children and adolescents diagnosed with OLT clinically and radiologically, specifically investigating the patient age and the status of distal tibial physis as factors associated with surgical success.
Materials and methods
Study design
This study was performed in accordance with the World Medical Association Declaration of Helsinki. Patients aged ≤18 years who were surgically treated for OLT at our institution between 2003 and 2016 were analyzed retrospectively. After study approval by the ethics committee and the Institutional Review Board committee, data were gathered from electronic medical records (Picture Archiving and Communication System, INFINITT Healthcare Co., Seoul, South Korea). Thirty patients were eligible for this study. In all the patients, the indication for surgery was a symptomatic OLT that failed to heal with conservative management, including rest, restriction of (sports) activities, cast immobilization, and physical therapy for a period of 3 months. In cases where there was missing information, additional information was collected from patients via phone calls or e-mails by one author (J.P.). Two patients did not answer the phone call and e-mail; thus, they were excluded. Finally, 28 patients were included in the study.
Image analysis
Lesions were evaluated using X-ray and magnetic resonance imaging (MRI) and graded using the Berndt and Harty 4 and Hepple et al. 13 classification systems, respectively, by a single observer (D.-Y.K) blinded to patient history. The Berndt and Harty classification is based on plain radiographs: stage I, small area of subchondral bone compression; stage II, osteochondral fragment partially detached; stage III, osteochondral fragment completely detached but not displaced; stage IV, osteochondral fragment completely detached and displaced. The Hepple classification is based on MRI: stage I, articular cartilage edema; stage IIa, cartilage injury with underlying fracture and surrounding bony edema; stage IIb, stage IIa without surrounding bone edema; stage III, detached but nondisplaced fragment; stage IV, displaced fragment; stage V, subchondral cyst formation. X-ray images taken just before the procedures and during follow-up periods were reviewed, and changes were classified as “healed,” if the lucency between the osteochondral fragment and the remainder of the bone was not observed; “improved,” if slight lucency between the osteochondral fragment and the remainder of the bone was observed but showed improvement compared with preoperative X-ray images; “unchanged,” if there was no change; or “worse,” if the lucency between the osteochondral fragment and the remainder of the bone or subchondral cyst had become larger (Figure 1). 14 The growth plate (physis) status was evaluated using preoperative MRI and classified as open, partially open, or closed according to the method published by Jopp et al. 15 using a three-stage visual grading system. Patients with closed physes were defined as skeletally mature. 16

Classification of postoperative X-ray lesion change: (a) healed, (b) improved, (c) unchanged, and (d) worse.
Operative procedure
All procedures were performed by a senior surgeon (W.J.Y). The patients were placed in the supine position with a thigh tourniquet. After induction of general anesthesia, all patients underwent diagnostic arthroscopy. A standard ankle distractor was used to facilitate joint access and visualization. Standard anteromedial and anterolateral portals were established. Arthroscopy was performed with a 2.7-mm diameter 30° arthroscope. If the lesion was stable and articular cartilage was intact, retrograde drilling and curettage (Figure 2) was performed under fluoroscopic guidance. Lesions with detached overlying cartilages were treated by debridement of the cartilage combined with microfracture and drilling (Figure 3). After the procedure, all patients were given a plaster cast for 4 weeks. Patients were kept non–weight bearing for 4 weeks, and full weight bearing was allowed at 6 weeks postoperatively. Running was allowed at 3 months postoperatively, and a full range of sports activities were allowed at 6 months postoperatively.
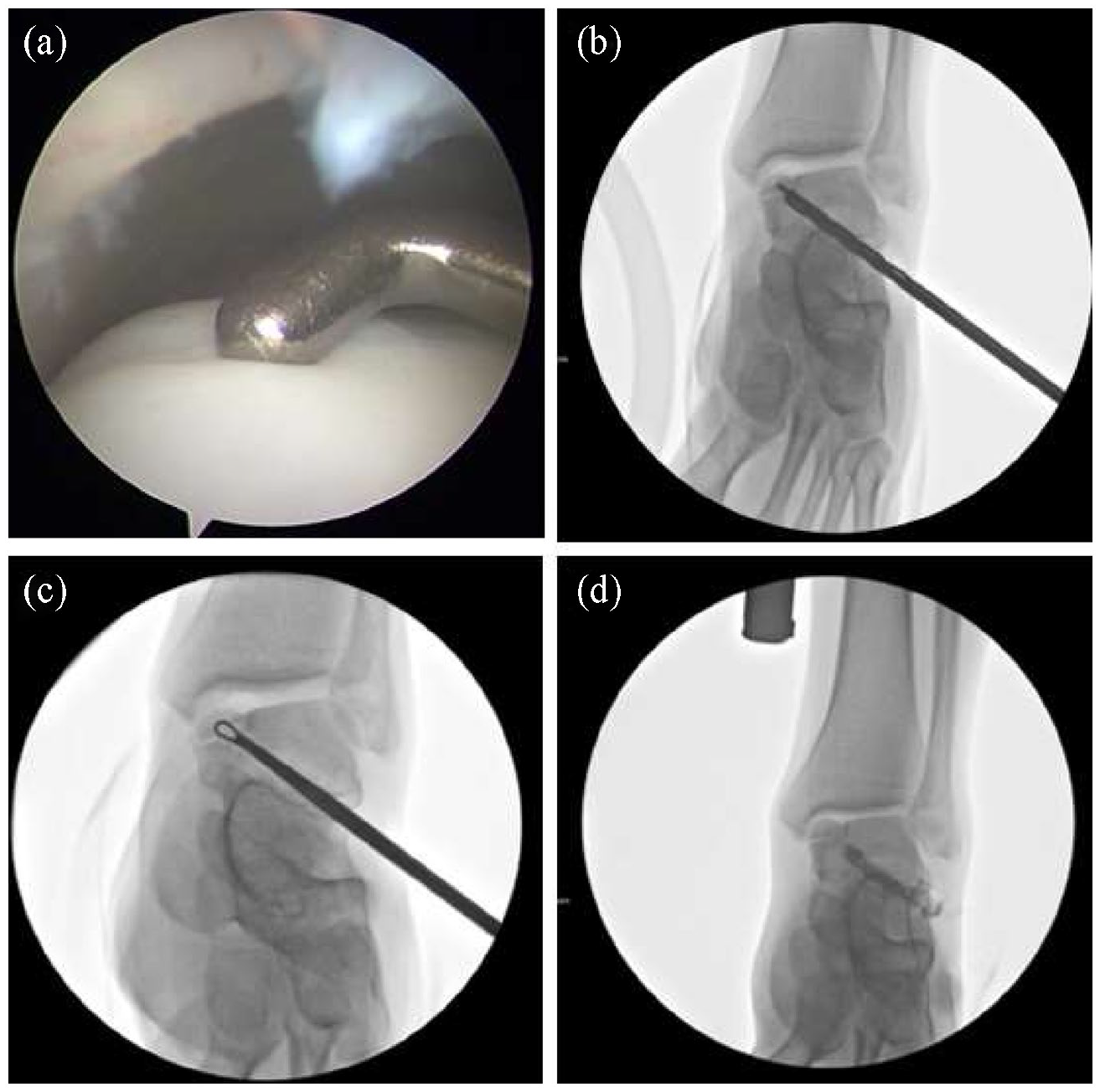
Retrograde tunneling with bone graft. (a) Fluoroscopic anteroposterior image shows stable osteochondral lesions of the talus (OLT). (b) Fluoroscopic anteroposterior image shows drilling into the OLT. (c) Fluoroscopic anteroposterior image shows curettage to the OLT. (d) Anteroposterior fluoroscopic (using iodine) view shows an intact cartilage.
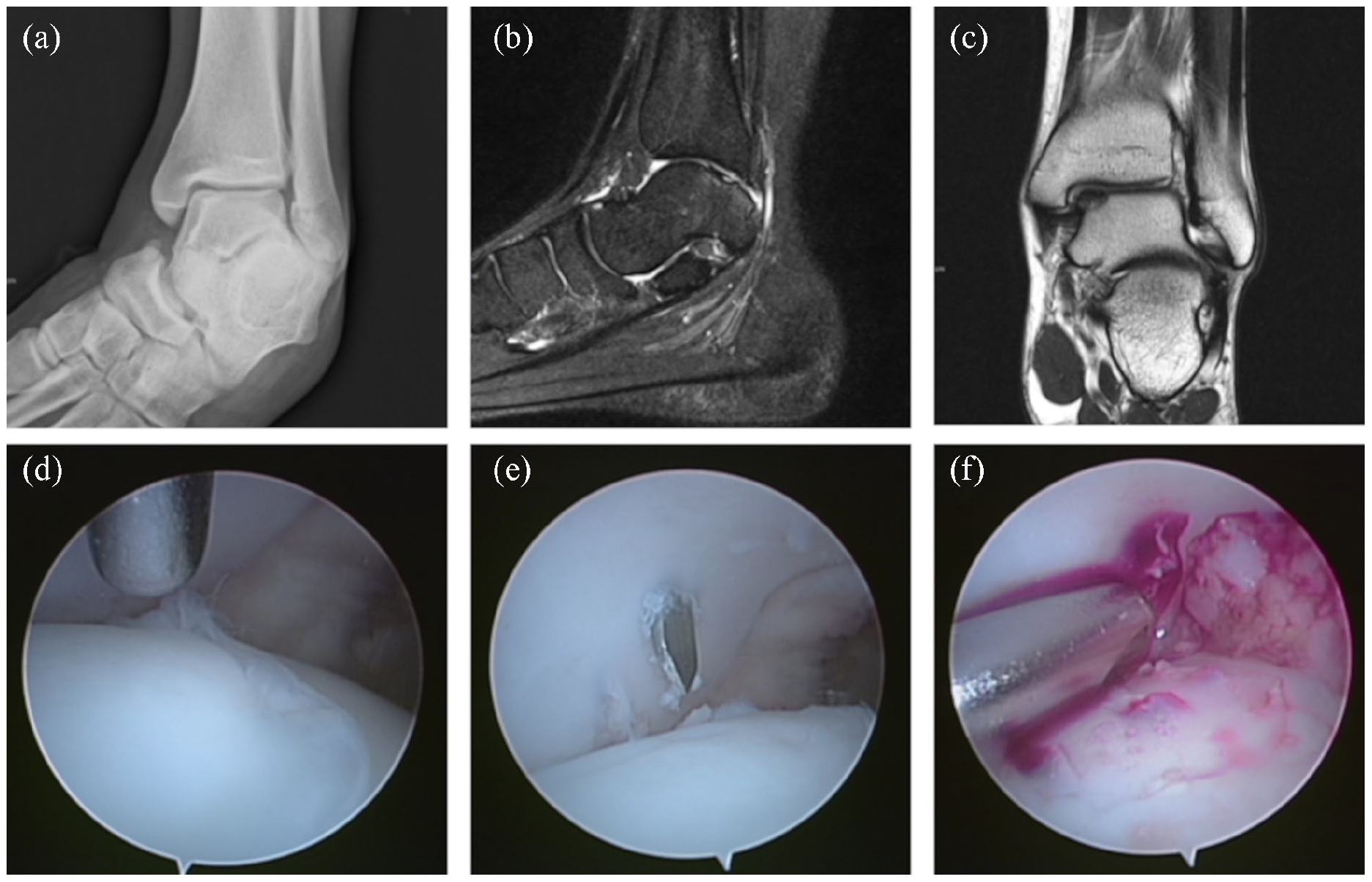
Images from one patient. (a) Mortise radiograph of the right ankle demonstrates a subtle area of lucency representing an osteochondral lesion in the medial talar dome. (b) Sagittal proton density with fat saturation magnetic resonance imaging (MRI) shows a cleft-like line beneath the osteochondral lesions of the medial talar dome. (c) Coronal T1-weighted MRI shows the osteochondral lesions of the medial talar dome with undisplaced fragment. (d) The arthroscopic image shows the detached cartilage. (e and f) Arthroscopic images show drilling of the osteochondral lesions of the talus via a transtalar approach and subchondral bone bleeding.
Clinical outcome measures
Clinical outcomes were evaluated using pain severity and the American Orthopaedic Foot & Ankle Society (AOFAS) hindfoot score. The AOFAS is scored between 0 and 100, with 0 indicating worst clinical condition and 100 indicating best clinical condition. 17 Pain severity was graded into four classes using the Numeric Rating Scale (NRS): grade 1, if patients had no pain by NRS score 0; grade 2, for pain during strenuous activity by NRS scores 1–3; grade 3, for pain during light activity by NRS scores 4–6; and grade 4, if the patient had pain during activities of daily living by NRS scores 7–10.
Statistical analysis
Non-parametric tests were used after testing for normal distribution with the Shapiro–Wilk test. Wilcoxon’s signed-rank test was used for continuous data. The chi-square test was used for categorical data. The correlation between the variables was analyzed using Pearson’s correlation. Linear-by-linear association was conducted for evaluation of the relationship between age of patients at the time of surgery and improvements in pain grades. Linear regression models were fitted for improvements in pain grades between the postoperative X-ray groups. Two-tailed values of p < 0.05 were considered significant, and all analyses were performed with SPSS (v23.0; IBM Corp., Armonk, NY, USA).
Results
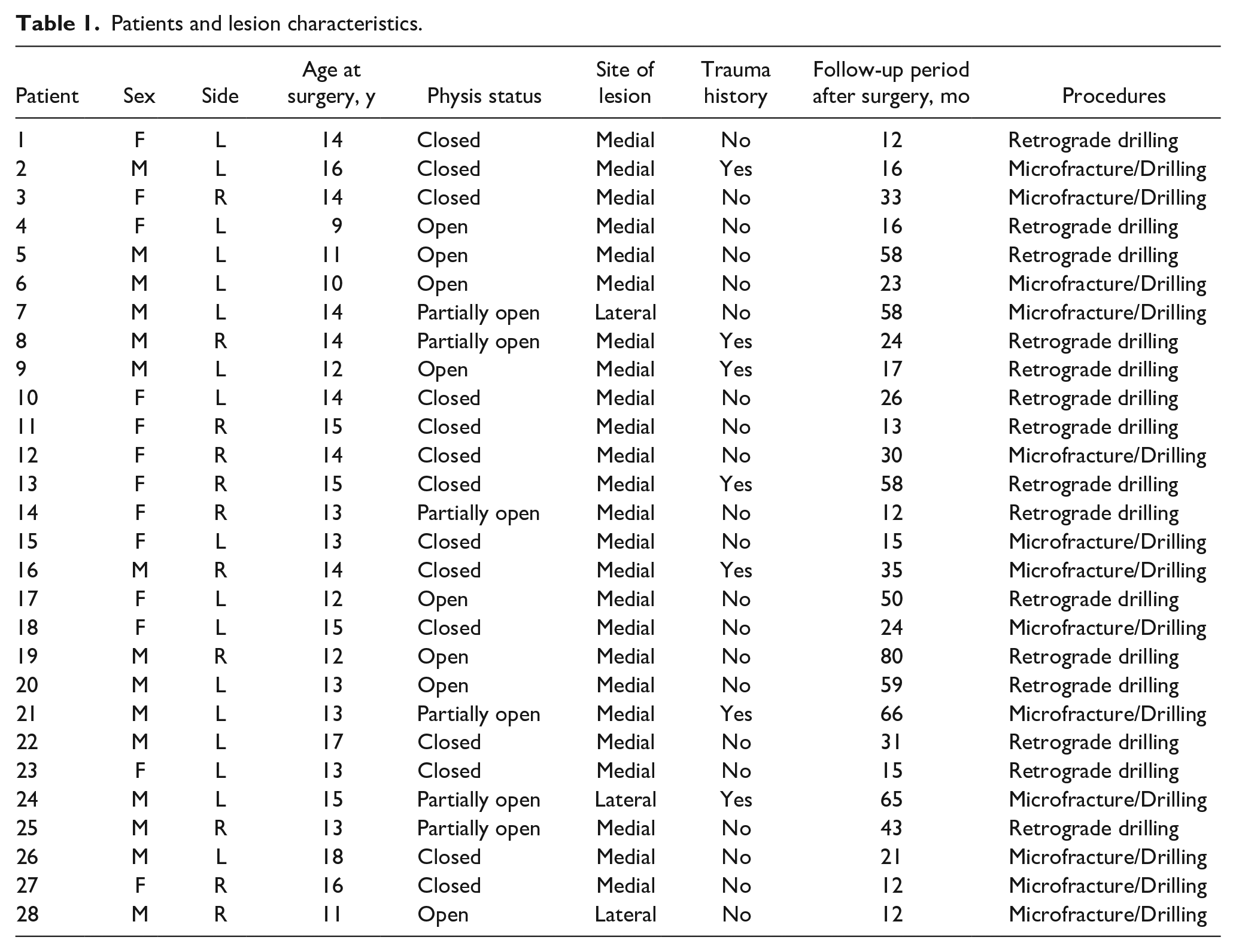
This study group consisted of 15 males and 13 females. The right and left talus were affected in 11 and 17 patients, respectively. The lesions were located on the medial side of the talus in 25 patients and the lateral side in 3 patients. Seven patients had a preceding history of trauma, while 21 patients had no remarkable history of trauma. There were 14 skeletally immature patients (8 with open physes, 6 with partially open physes) and 14 skeletally mature patients (closed physes). The average duration of symptoms was 12.65 (range, 1–61) months. The mean age at the time of surgery was 13.57 (range, 9–18) years, with a mean follow-up duration of 33.00 (range, 12–80) months (Table 1).
Patients and lesion characteristics.
The patients were treated with retrograde drilling and curettage (n = 15), or microfracture and drilling (n = 13). The mean Berndt and Harty classifications were 3.21 preoperatively and 2.07 postoperatively, which were significant (p < 0.001) (Table 2). On postoperative X-ray images, lesions were judged as “healed” in 8 (29%) cases, “improved” in 16 (57%), “unchanged” in 1 (4%), and “worse” in 3 (10%)
Stage of OLT at the time of surgery and follow-up (Berndt and Harty classification).
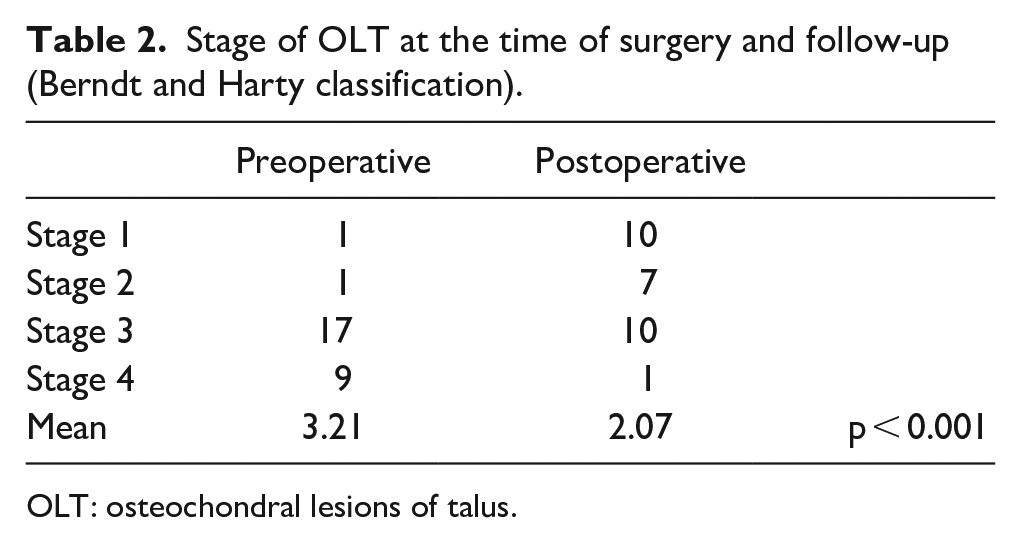
OLT: osteochondral lesions of talus.
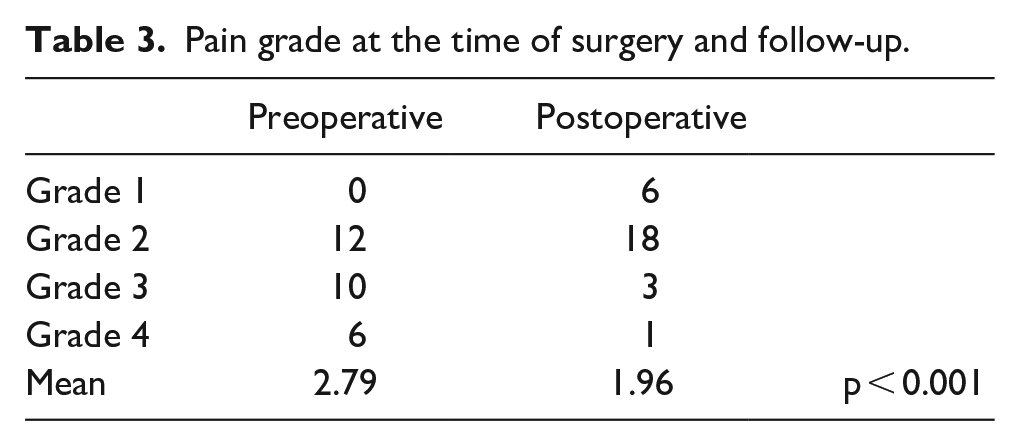
The mean pain grades were 2.79 preoperatively and 1.96 postoperatively, which were also significant (p < 0.001) (Table 3). Moreover, 18 (64%) patients showed improvements in pain, and 24 (86%) patients reported improvements in AOFAS scores. The median pre- and postoperative AOFAS scores were 69 (range, 20–88) and 86 (range, 70–100) respectively; these were also significant (p = 0.018).
Pain grade at the time of surgery and follow-up.
The sex, lesion location, and trauma history were not significantly different between pre- and postoperative pain grades, AOFAS scores, Berndt and Harty classifications, and X-ray changes. The age of patients at the time of surgery correlated with improvements in pain grades (p = 0.008). Patients aged ≤13 years showed greater improvements in pain grades than older patients (p = 0.02). There were no significantly associated improvements in pain grades between the postoperative X-ray groups.
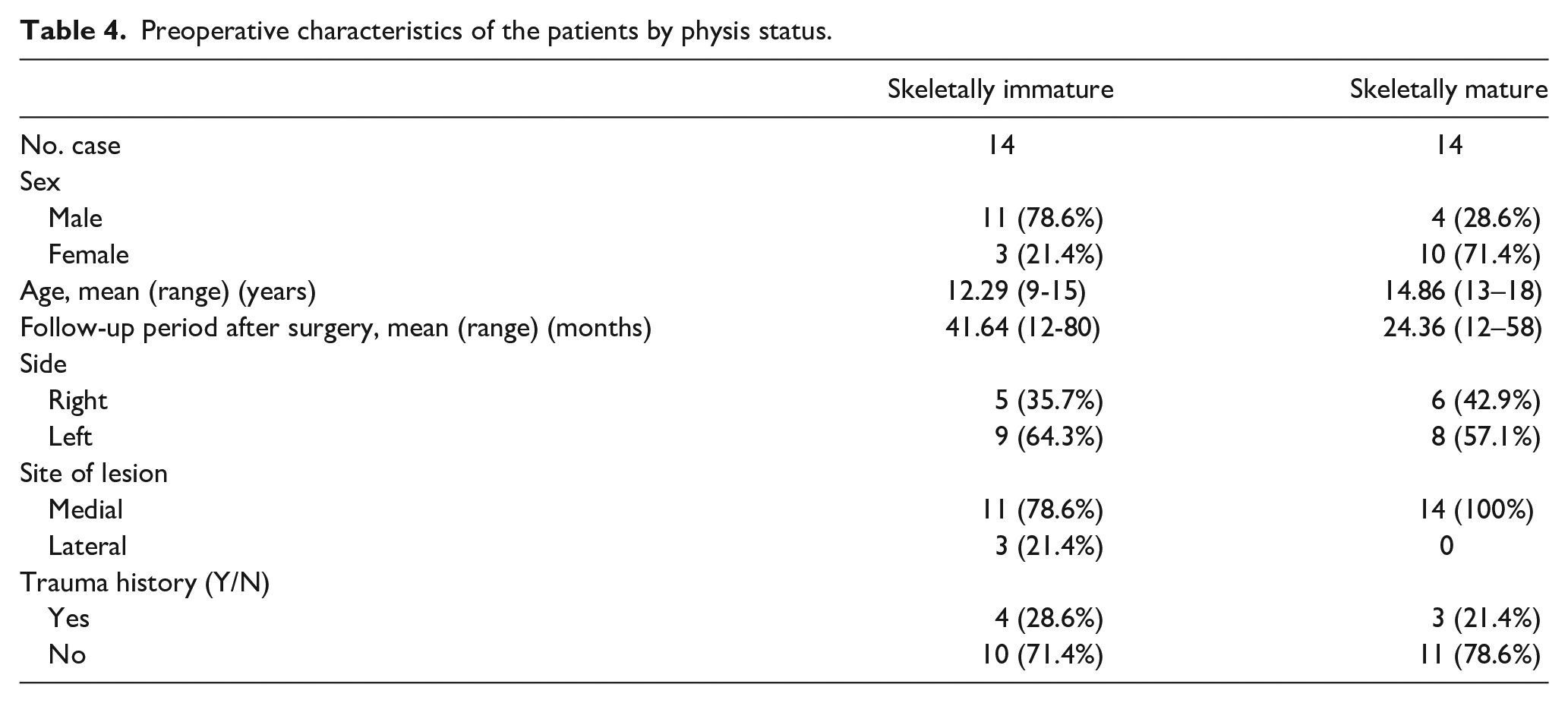
The skeletally immature and mature groups are described in Table 4. Between the two groups, the improvement in pain grade was better in the skeletally immature group than in the skeletally mature group (p = 0.048). AOFAS scores and radiological changes within the two groups were not significantly different.
Preoperative characteristics of the patients by physis status.
Discussion
The major findings of our study were that postoperative pain grade and AOFAS score were significantly improved in pediatric OLT patients. Furthermore, pain grade significantly improved as the patient was younger and the growth plate was not closed.
OLT is an idiopathic focal injury to the subchondral bone that subsequently affects the overlying cartilage. The etiology is controversial; however, traumatic-microtraumatic factors seem to be major contributing factors to OLT. 18 In our study, only seven cases had definite preceding histories of trauma; however, we were unable to evaluate them because information on the levels of sports activity was missing. Letts et al. 9 and Schachter et al. 19 stated that lateral lesions were more likely to be associated with a preceding history of trauma. However, in our study, no obvious relationship was found between a history of trauma and lesion location (p = 0.736)
Conservative treatment of OLT includes rest, no weight bearing, bracing, and rehabilitation with or without the use of nonsteroidal anti-inflammatory drugs.20–22 Some studies have reported high success rates of conservative treatments of OLT6,18,23; however, the results are conflicting. According to Letts et al., 9 13 out of 24 patients (54%) who had undergone conservative treatment failed the treatment, and surgical treatment was performed. Reilingh et al. 8 reported that 92% of pediatric patients required surgery. In this study, it was not possible to evaluate the effectiveness of conservative treatment because only patients who underwent surgical treatment were included.
The three indexes—pain grade, AOFAS score, and X-ray classifications—improved after surgical treatment. Many previous studies have reported low radiographic healing rates despite improved clinical results.14,23–25 According to Higuera et al., 24 good or excellent clinical results were obtained in 95% of cases after surgery, while only 69% cases were classified as good or excellent radiologically. This study also showed results similar to previous studies. Pain grade was improved in 64% and the AOFAS score was improved in 86% of the patients, but the radiological improvement was evaluated as “healed” in only 29%.
In this study, the patient’s age at the time of surgery and physeal status were significant factors that affect the prognosis of surgery. The patient’s sex, location of lesion, and history of antecedent trauma were irrelevant to the outcome of the surgery. Bruns et al. 18 reported that compared with adult patients, adolescent patients showed better outcomes after surgery regardless of the stage of the lesion. In our study, children aged ≤13 years demonstrated better outcomes in terms of pain grades than middle adolescents (p < 0.05). Considering that the physis can close as early as 14 years for boys and 12 years for girls, 26 this result might be related to the state of the physis.
Only a few studies have compared surgical outcomes in patients depending on their growth plate status. Kramer et al. 14 reported that the state of the physis had no effect on clinical, radiographic, or functional results. Carlson et al. 10 recently reported no significant differences in satisfaction, outcome scores, or arthritis progression between the skeletally mature and skeletally immature groups. In contrast to these studies, greater improvements in pain grades were observed in the open physis group. However, no significant correlations in AOFAS scores or radiological changes were found between the two groups. The pain in OLT is caused by the repetitive high fluid pressure and decrease in pH, sensitizing the highly innervated subchondral bone. 27 Arthroscopic procedures, such as microfracture or multiple drilling, tend to stimulate the bone marrow to fill osteochondral defects with fibrocartilages. Generally, patients with open physis were believed to have had a higher chance of healing because of the enhanced remodeling capacity. This could have influenced the pain improvement in the skeletally immature group in our study. However, further research is needed on this aspect.
This study has a few limitations. First, the study design is retrospective and we could not perform a power analysis to calculate the number of patients needed. Second, the study had a relatively small number of participants. Third, a control group including patients who received conservative treatment alone was not included. Furthermore, MRI or computed tomography (CT) scans may give additional information on the quality of cartilage repair or subchondral bone healing compared to X-rays.
Conclusion
Surgical treatment in pediatric OLT patients was helpful in terms of pain relief, functional improvement, and radiological healing. Postoperative pain relief was better in the younger age group (age ≤13 years) and skeletally immature group. Therefore, when conservative treatment is unsuccessful, early surgical treatment is recommended in pediatric OLT patients.
Footnotes
Authors’ contributions
Dae-Yoo Kim, MD: Manuscript preparation, data collection, analysis and interpretation of results, writing—review & editing.
JiSu Park, MD: Performed measurements, manuscript preparation, statistical analysis, writing—original draft.
Ho Won Kang, MD: Data collection.
Chang Ho Shin, MD: Supervision.
Dong Yeon Lee, MD: Validation, supervision.
Tae-Joon Cho, MD: Supervision.
Won Joon Yoo, MD: Study design, validation, writing—review & editing.
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: T.-J.C. is a member of the Editorial Board of the Journal of Children’s Orthopaedics.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by a grant (NRF-2016R1D1A1B02009379) from the Bio & Medical Technology Development Program of the National Research Foundation (NRF) funded by the Ministry of Science & ICT, Republic of Korea. The funders had no role in study design, data collection and analysis, decision to publish, or preparation of the manuscript. Each author certifies that there are no funding or commercial associations (consultancies, stock ownership, equity interest, patent/licensing arrangements, etc.) that might pose a conflict of interest in connection with the submitted article related to the author or any immediate family members.
Ethical review committee statement
All ICMJE Conflict of Interest Forms for authors and Journal of Children’s Orthopaedics editors and board members are on file with the publication and can be viewed on request. Ethical approval for this study was obtained from Seoul National University Hospital, Seoul, Republic of Korea (approval number H-1806-035-949).