
Abstract

Thank you for allowing the opportunity to respond to questions regarding our article, and it appears that there are two principles that have been raised which we would like to help address.
Study methods for radiologic assessment and our definitions for malunion.
Surgical technique utilized in this cohort.
Study methods
It is true that we did not have contralateral radiographs available for comparison at the most recent follow-up x-ray. With this limitation (inherent to such retrospective studies), to define coronal plane malunion we chose a Baumann’s angle of 75° to be normal and a deviation of 15° in either direction to be a malunion. We did not measure the capitellohumeral angle, and this would have helped characterize sagittal plane deformity to be angular or translational or both. Yet because most surgeons recommend pinning of a supracondylar humerus fracture when the anterior humeral line does not intersect the capitellum, we used this as our threshold to define sagittal plane malunion. Finally, it is very difficult to assess malrotation as we do not have 3-dimensional studies. We choose a difference of 5 mm in the width of the fractured surface to be indicative of rotation of the fracture. We wish that there were published data that correlated this measure with actual malrotation on 3-dimensional studies and further whether this indicated clinical disability. As pointed, this does not exist.
Surgical technique
Rehm et al. nicely summarize the aspirational goals of lateral pin fixation in regard to pin technique and pin size. We believe that our article has value as it represents “real world” outcome of Type 3 supracondylar humerus fractures (SCHFx-3) managed by relatively well-trained surgeons, including practicing general orthopedists, fellowship-trained pediatric orthopedic surgeons and orthopedic traumatologists. We highlight increasing rates of rotational malunion of all lateral pinning when compared with crossed K-wires, which tended to occur in those fractures with posterolateral displacement. We hypothesize that this could be due to torn medial periosteum that could not provide stability with all lateral pins. Conversely, posteromedial displaced fractures would have more stability from having an intact medial periosteum when paired with all lateral pinning.
We include an example of a recent case (not from our study) of a 6-year-old boy with a completely displaced fracture who underwent treatment by an orthopedic traumatologist who performed an anatomic reduction with three lateral pins and had a cast applied (Figure 1).
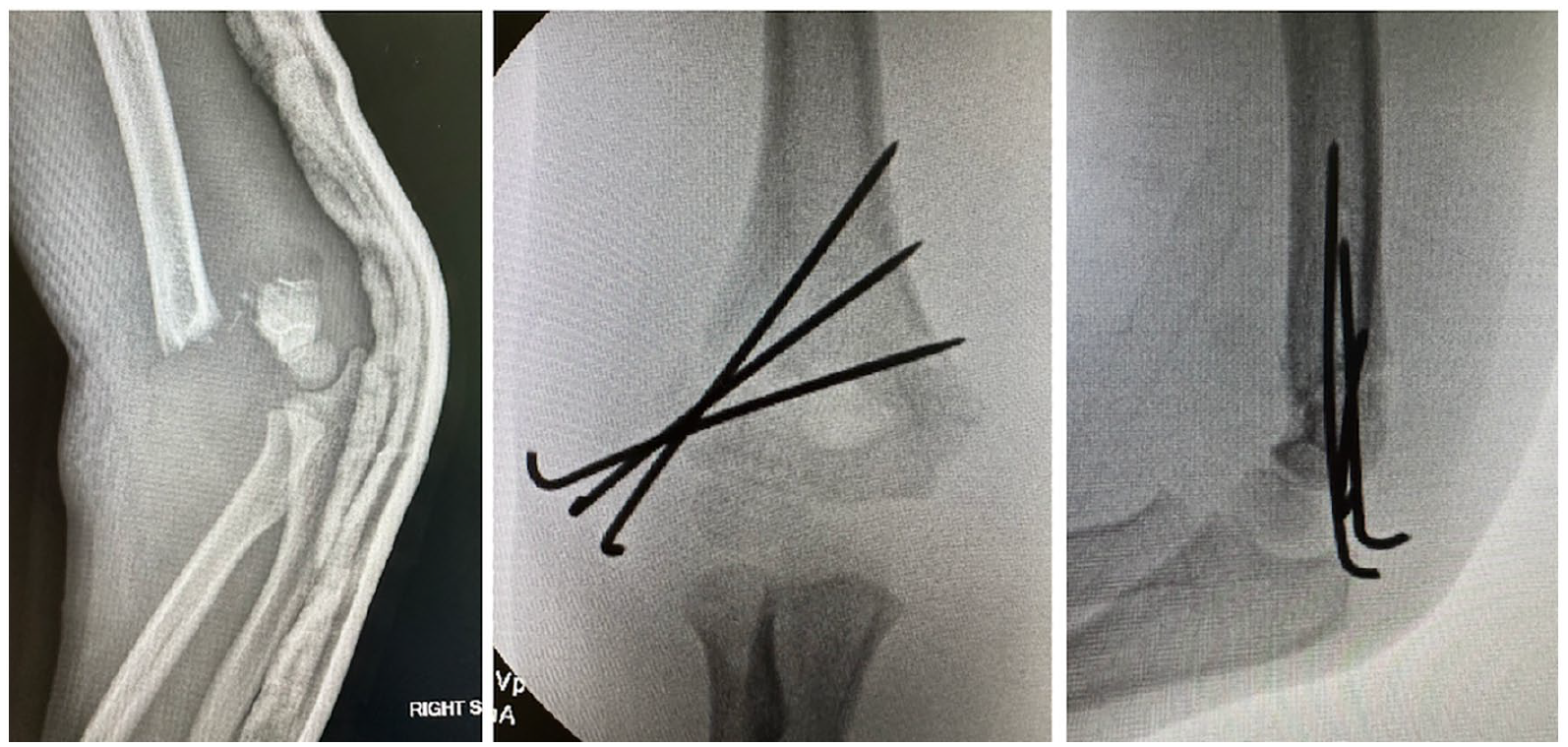
Six-year-old boy with a SCHFx-3 treated with reduction and pinning. He was placed in a cast and had intraoperative radiographs which demonstrated stable positioning without displacement.
At 3.5-week follow-up, his fracture had lost reduction and healed in a rotated position (Figure 2). At 1 year, he had slight varus and rotational differences to the contralateral elbow (Figure 3).

At 3.5-week follow-up, he had healed in a mal-reduced position.
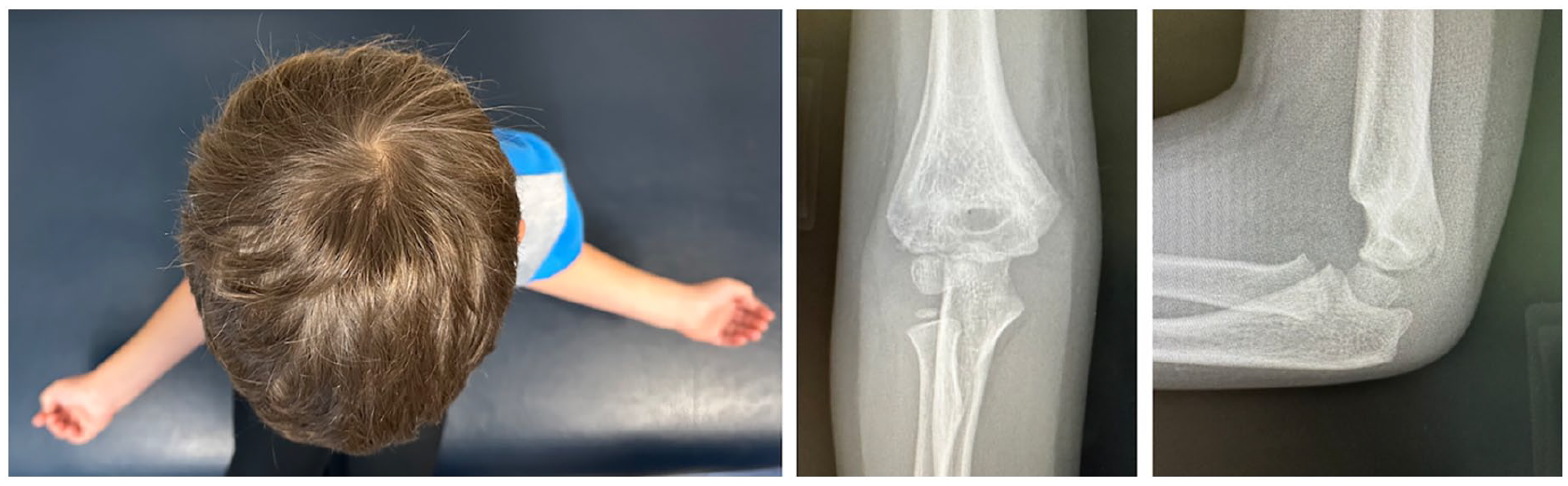
One year later, he follows up with a mal-rotated humerus with slight varus.
While one could argue this is not a “perfect pinning,” we hypothesize that most surgeons would have been satisfied with the reduction and that the three pins spread across the fracture would have been sufficient in a cast; yet in this case, it wasn’t.
In conclusion, we appreciate the comments raised and the opportunity to respond to concerns about our article. While our criteria for what constitutes a malunion may differ from others, all lateral pinning may result in some loss of reduction in completely displaced supracondylar humerus fractures. In our past experience and in the recent case, we have demonstrated that good surgeons doing the very best they could do not always obtain perfect results with all lateral pinning in SCHFx-3. This would be supported by our finding equal results between fellowship-trained pediatric orthopedists and traumatologists and that these results were better than in general orthopedists. For less than perfect surgeons, more reliable results might be obtained with two lateral pins and adding a medial pin placed through a small incision (thereby protecting the ulnar nerve).
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.