
Abstract
Introduction:
Pediatric back pain evaluation nowadays relies on patient history, physical examination, and plain radiographs to identify underlying pathologies. Constant pain, night pain, radicular pain, and abnormal neurological examination were previously recommended as clinical markers to assess the need for magnetic resonance imaging evaluation. Recent studies have challenged the use of these clinical markers, recommending further studies. This study aimed to assess pain intensity as a predictor of underlying magnetic resonance imaging pathology in children with back pain.
Methods:
An observational cross-sectional study of pediatric patients between 8 and 17 years with back pain for more than 4 weeks from 2009 to 2021 was conducted. A whole spine magnetic resonance imaging was performed on patients with back pain without an identifiable cause and no prior spine treatment. The numerical rating scale questionnaire was administered to each patient, and answers were divided into three groups: mild (1–3), moderate (4–6), and severe (7–10) numerical rating scale score. Student’s t-test and chi-square analysis were used to correlate differences between continuous and categorical values, respectively.
Results:
Of 590 patients (70% female and a mean age of 15.25 years), there were 35.1% of patients had a magnetic resonance imaging underlying pathology. No association was found between severe numerical rating scale score and the presence of underlying MRI pathology (p = 0.666). Patients with low or moderate numerical rating scale scores had similar associations to an underlying magnetic resonance imaging pathology as patients with a severe numerical rating scale score (p = 0.256; p = 0.357, respectively).
Conclusions:
Back pain intensity was not found to be an effective clinical marker for predicting underlying magnetic resonance imaging pathology in pediatric patients with back pain.
Introduction
Back pain is a symptom with a broad spectrum of severity. Due to the complex presentation and variable symptoms, evaluation and treatment of back pain are challenging. Pediatric back pain was reported as an uncommon complaint in the past and highly linked with serious pathology.1,2 Recently, studies have suggested that pediatric back pain is more frequent than previously reported, with a limited association with organic pathologies. 3 Now, most cases of back pain in the pediatric population have been attributed to benign mechanical causes. 4
The great dilemma in evaluating pediatric back pain relies on the ambiguity of the patient history, physical examination, and plain radiographs to identify an underlying pathology. 5 In 2006, Feldman et al. 5 presented a diagnostic algorithm based on several clinical markers such as constant pain, radicular pain, night pain, or abnormal neurologic findings as a discriminant to prescribe magnetic resonance imaging (MRI) if the initial history, physical examination, and radiograph were non-diagnostic. Several years later, Ramirez et al. 3 found a weak sensitivity and specificity of constant, night, and radicular pain as clinical markers to request an MRI. The authors recognized that further studies are necessary to identify other clinical markers to evaluate pediatric back pain. 3 Later, Nolte et al. 6 developed a scoring system for evaluating pediatric back pain using neurological deficit, nocturnal symptoms, sudden onset, leg pain, lumbar pain, and age as clinical markers to guide the use of an MRI. A reliable clinical marker that could define the MRI indications when a patient has a non-diagnostic history, physical examination, and radiograph is still debatable.
Pain intensity is a crucial parameter for understanding the impact of a person’s experience of pain and should be considered as a possible clinical marker that could predict the presence of underlying MRI pathology.7,8 The validation of pain intensity as a clinical marker for predicting an underlying MRI pathology in the pediatric back pain population after a non-diagnostic history, physical examination, and initial plain radiographs has been scarcely evaluated.
This study aimed to assess pain intensity using the numerical rating scale (NRS) and determine its predictive power on underlying MRI pathology in pediatric back pain. The authors hypothesized that a severe NRS score would be associated with the presence of an underlying MRI pathology.
Method
Participants and study design
An observational cross-sectional study in all pediatric patients between 8 and 17 years of age who presented with chronic back pain (lasting more than 4 weeks)) from 2009 to 2021 at La Concepcion Hospital Pediatric Orthopaedic Clinic in San German orthopaedic clinic in Puerto Rico was conducted. A whole spine magnetic resonance image (MRI) was performed on all patients with back pain without an identifiable cause and no prior spine treatment (surgical or conservative); after undergoing a non-diagnostic history, physical examination, and spinal X-ray, as utilized in previous studies.3,5,9,10 Institutional review board (IRB) approval was obtained.
Patients with any previous pain-related diagnosis, developmental delay or cognitive impairment, history of trauma, neurological abnormalities identified at initial evaluation, or radiographic diagnostic findings (spondylolysis, spondylolisthesis, or Scheuermann’s kyphosis); were excluded from the study.
Measurements
In the patient’s first pediatric orthopaedic assessment, a single validated 10-point NRS questionnaire10,11 was administered. Individually, patients were asked: “On a scale from zero to ten, where zero means no pain and ten means the most or worst pain, how much pain are you experiencing?” Afterward, the sample data collected from pain intensity responses (NRS) were stratified into the following three groups: mild NRS score (one to three), moderate NRS score (four to six), and severe NRS score (seven to ten) pain intensity. 9 The cutoffs of each group were chosen given the previous models of score categorization described in previous studies. 10 Additional patient factors such as sex, age, frequency, night pain, neurological exam, and presence of an underlying pathology were compared between groups.
Statistical analysis
Each of the variables collected (i.e. sex, age, pain frequency, and NRS score categories) were evaluated to observe their association with the presence of an underlying MRI pathology. The student’s t-test was used to evaluate the differences between continuous variables, and the chi-square test was used to assess the difference between categorical variables. The independent variables’ positive and negative likelihood ratios were calculated. A p value less than 0.05 was considered statistically significant. Data were analyzed using SPSS® and Microsoft Excel® software.
Results
Demographics
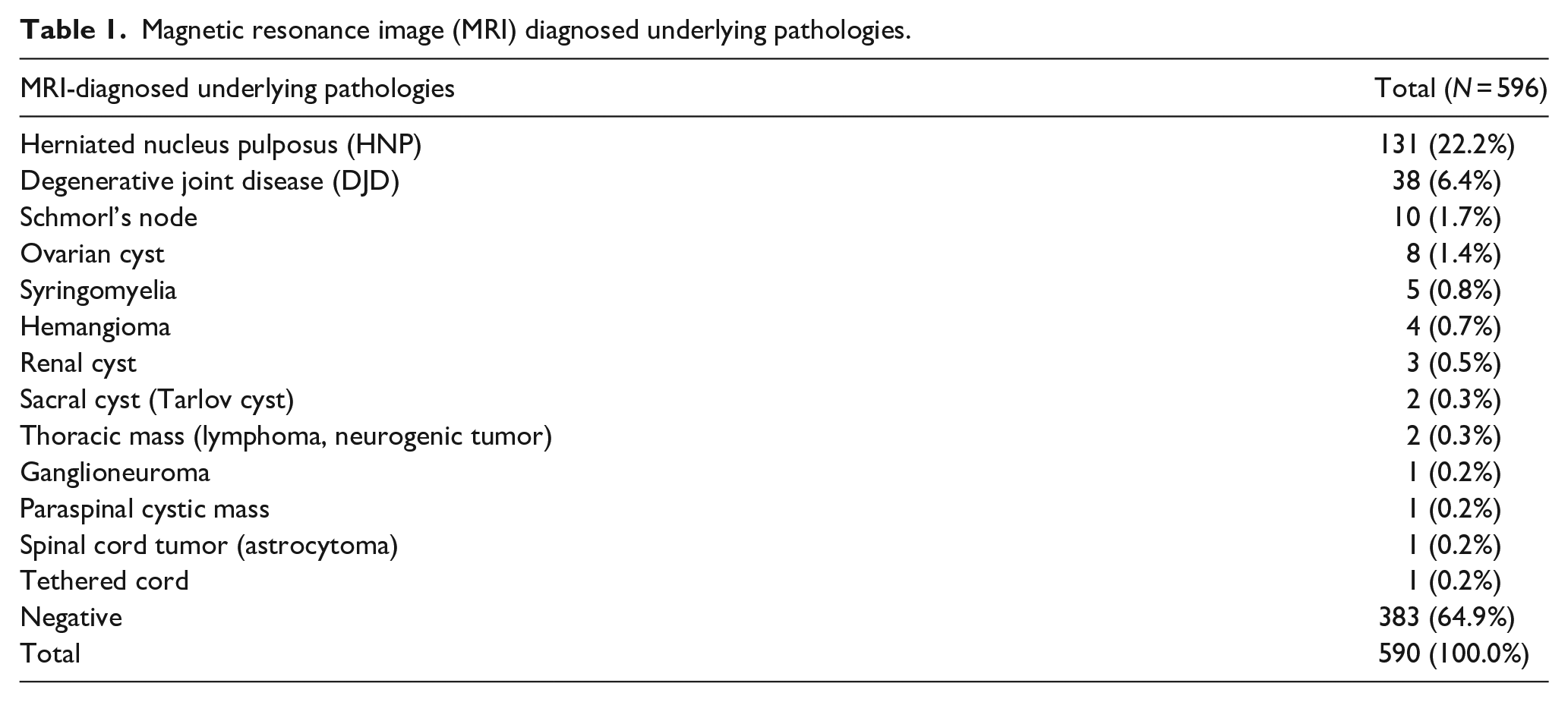
A total of 590 patients were included with a mean of 15.25 ± 2.75 years of age: 70.0% (410/590) being female. All the participants completed the NRS questionnaire, with 33 patients (5.59%) reporting a low NRS, 243 patients (41.19%) a moderate NRS, and 314 patients (52.22%) a severe NRS score. Overall, 207 out of 590 patients (35.10%) were found to have an MRI underlying pathology. The distribution of the MRI-diagnosed underlying pathologies is illustrated in Table 1.
Magnetic resonance image (MRI) diagnosed underlying pathologies.
Mild pain intensity NRS score 1–3
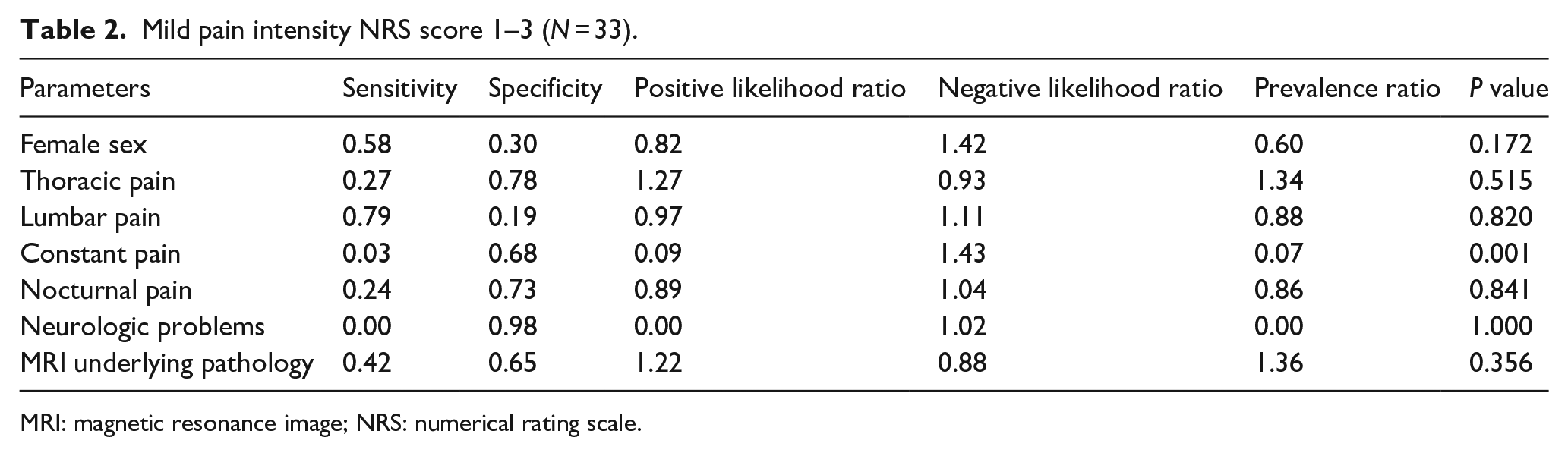
Among patients who reported mild pain intensity, an average pain score of 2.70 ± 0.53 was found. There was an average patient age of 15.10 ± 2.61 years, with 57.60% of patients being female. The number of underlying MRI pathologies found in this group was 14/33 (42.40%), while the prevalence of an underlying pathology found in patients without a low NRS score was 293/557 (52.60%). The prevalence ratio between patients with low NRS scores versus patients without low NRS scores was 0.68 (p = 0.256). The sensitivity was 0.42, and the specificity was 0.47 for low pain NRS scores for predicting the presence of an underlying MRI pathology. The positive likelihood ratio was 0.81, and the negative likelihood ratio was 1.22 (see Table 2).
Mild pain intensity NRS score 1–3 (N = 33).
MRI: magnetic resonance image; NRS: numerical rating scale.
Moderate pain intensity NRS score 4–6
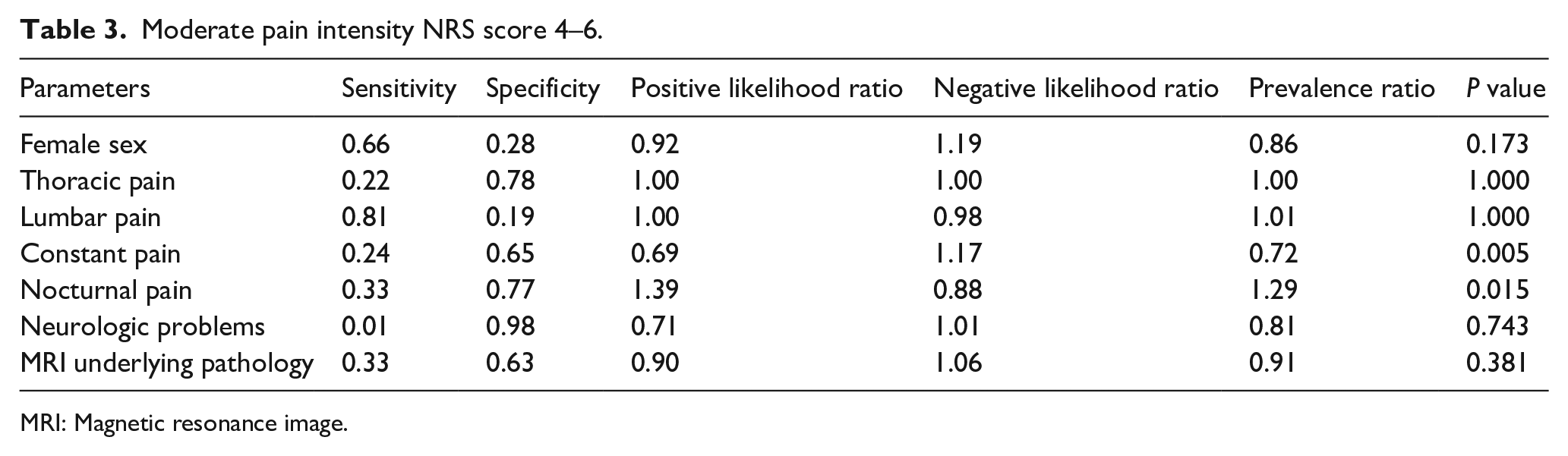
Among children with moderate pain intensity, an average pain score of 5.26 ± 0.62 was found. There was an average patient age of 14.83 ± 2.65 years, with 66.3% of patients being female. An underlying pathology found by MRI in patients with a moderate NRS score was 80/243 (32.90%), while an underlying pathology in patients without a moderate NRS score was found in 127/347 (36.60%). A comparison of the prevalence ratio of an underlying pathology diagnosed by MRI in children with moderate pain intensity and children without moderate pain intensity was 0.91 (p = 0.357). The sensitivity was 0.33, and the specificity was 0.63 in moderate pain NRS score for predicting the presence of an underlying MRI pathology. The positive and negative likelihood ratios were 0.90 and 1.06, respectively (Table 3).
Moderate pain intensity NRS score 4–6.
MRI: Magnetic resonance image.
Severe pain intensity NRS score 7–10
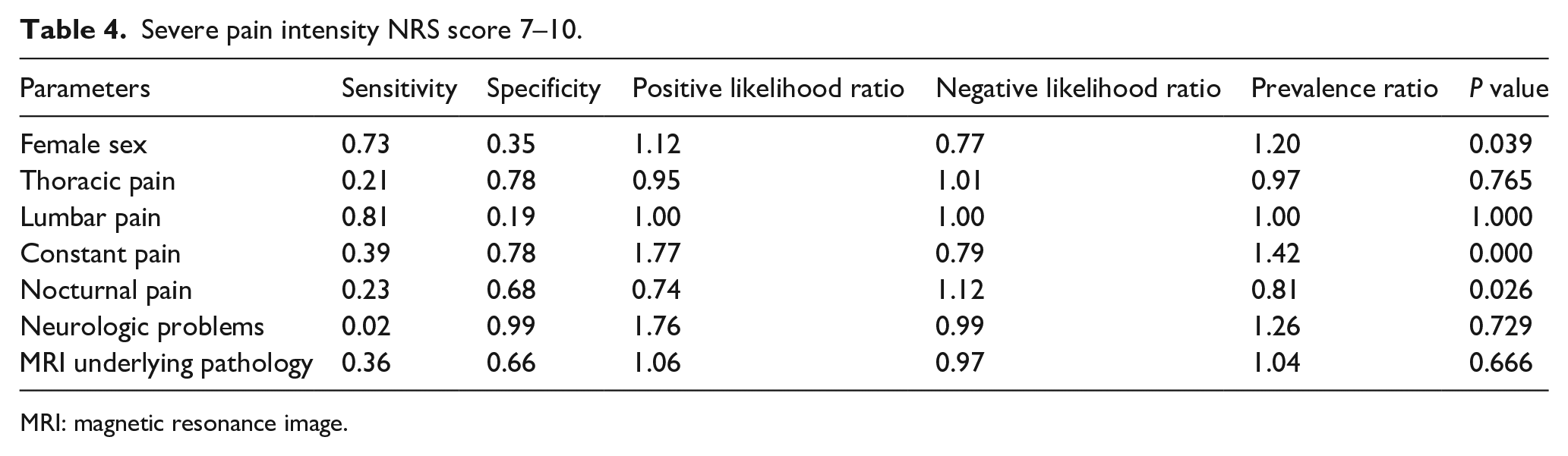
Among patients who reported severe pain, an average pain score of 8.19 ± 1.13 was found. There was an average patient age of 15.55 ± 2.79 years, with 57.6% of patients being female. The number of underlying pathologies found in patients with a severe pain intensity was 113/314 (36.0%), compared to 94/276 (34.06%) in patients without severe pain. The prevalence ratio of underlying MRI pathology in children with and without a severe NRS score was 1.04 (p = 0.666). The sensitivity was 0.36, and the specificity was 0.66 in severe NRS scores for predicting the presence of underlying pathology. The positive and negative likelihood ratios were 1.06, and 1.00, respectively (see Table 4).
Severe pain intensity NRS score 7–10.
MRI: magnetic resonance image.
Discussion
The evaluation of back pain intensity, measured with the validated NRS score instrument, was not predictive of an underlying MRI pathology in pediatric back pain patients in this study. Interestingly, a low or moderate NRS score had similar associations to an underlying MRI pathology as patients with a severe NRS score.
Pediatric back pain is a topic that has historically been heavily debated in the medical community. In 2017, the American College of Radiologists (ACR) published the Appropriateness Criteria to establish guidelines for evaluating pediatric patients with back pain. 12 Previously, the sole complaint of back pain in pediatric patients was considered as an indication for imaging. This prompted the ACR to form a panel of experts to consider a more conservative approach.4,5,13 They recommended an algorithmic approach toward back pain in the pediatric population to avoid relying solely on back pain as an indication for imaging. The ACR recommends MRI for pediatric back pain if one of the following red flags is present: pain lasting more than 4 weeks, constant pain, night pain, and an abnormal neurologic examination. 12 However, there remains disagreement among the expert panel as to which clinical markers best predict the presence of underlying pathology. In 2019, Ramirez et al. 3 refuted the consistency of the clinical markers described above and reopened the search for other, more reliable clinical markers. In 2021, Rathjen et al. 14 evaluated the relationship between back pain and the presence of underlying MRI intradural pathology. They found that back pain does not have a clinical correlation with the presence of underlying MRI intradural pathology in pediatric patients.14,15 Amid the lack of available data regarding clinical markers that may predict the presence of underlying pathology, pain intensity was proposed as a reliable marker to predict the presence of underlying pathology.
Pain intensity is essential for guiding treatment options and improving patient outcomes.16–18 Self-reporting pain intensity is currently the gold standard for assessment in pediatric patients. 19 This parameter is crucial for measuring the impact of a person’s experience of pain and can be evaluated using numerous available self-report measures, making it an ideal clinical marker to assess. Since the study population consists of pediatric patients, the NRS tool was chosen due to its proven validity among the pediatric population. In addition, the lack of need for extra equipment, the simplicity of use, and its reproducibility make this tool preferable to other pain intensity scales. 20
This study has several limitations. First, pain is subjective. Second, patients were evaluated by a single orthopaedic surgeon. Therefore there was no inter-examiner evaluation performed. Finally, further studies exploring the predictive power of other clinical markers, such as back stiffness, should be considered in diagnosing underlying pathology in pediatric back pain patients.
Conclusion
This study provides evidence that back pain intensity measured via NRS scores was not a good clinical marker for predicting underlying MRI pathology in pediatric patients with back pain. While back pain intensity is certainly a clinical marker that can aid a physician in diagnosing underlying pathologies, it is not an effective singular instrument for predicting the presence of an underlying MRI pathology. Future studies that evaluate different markers that may predict underlying MRI pathology in pediatric patients must be considered to improve current predictive methods.
Footnotes
Author contributions
1. All authors made substantial contributions to the conception or design of the work; or the acquisition, analysis, or interpretation of data for the work.
2. All authors contributed to the drafting the work or revising it critically for important intellectual content.
3. All authors gave final approval of the version to be published.
4. All authors agreed to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Compliance with ethical standards
Institutional review board (IRB) support was granted to this study. The study was conducted in accordance with the Helsinki Declaration stating the protection of research participants. Patients included in the study provided written informed consent.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.