
Abstract
Spinal angiolipomas (SALs) are extremely rare benign tumors composed of both mature fatty tissue and anomalous vascular channels. We present two cases of SALs and review the clinical presentation, radiological appearance, pathological aspects, and treatment of this distinct clinicopathological mass. The patients’ neurologic symptoms improved postoperatively and follow-up revealed no signs of tumor recurrence or neurological deficit. SAL should be considered as a differential diagnosis in patients with spinal cord compression. Magnetic resonance imaging is important for detecting and characterizing SALs. The gold standard treatment modality should be total resection.
Introduction
Spinal angiolipomas (SALs) are extremely rare benign tumors composed of both mature fatty tissue and anomalous vascular channels. SALs were first described by Berenbruch in 1890, and since that time about 200 cases have been reported.1,2 They constitute about 0.04% to 1.2% of spinal axis tumors and about 2% to 3% of extradural spinal tumors.2–4 The typical clinical symptoms in patients with SALs are similar to those of spinal cord or nerve root compression. Magnetic resonance imaging (MRI) is an important technique for detecting and characterizing SALs, which present with a typical appearance and can be enhanced by gadolinium (Gd). Angiolipomas are ultimately diagnosed by histopathological examination of the removed lesion following surgery. Here, we report two cases of SALs, including one thoracic and one lumbar angiolipoma, and describe the diagnosis and surgical treatment of these patients. We also provide a thorough review of SALs reported in the literature.
Case presentations
Case 1
A 47-year-old woman presented with a 7-year history of progressively severe back pain, especially over the past 2 years. Her back pain was particularly obvious at night and often resulted in insomnia. However, she had no radiation pain, numbness in the lower limbs, or urinary or fecal incontinence. Her medical history showed obesity but no other diseases. Her body mass index (BMI) was 33.2 kg/m2.
Physical examination showed obvious tenderness at L1 to L2 levels. Muscle volume, strength, and reflexes of the upper and lower limbs were normal, and there were no positive neurological results.
Computed tomography (CT) examination of the lumbar spine revealed a posterior extradural mass extending from L1 to L2 with spinal cord compression (Figure 1a, b). MRI was performed to obtain more information, and the mass was hypointense on T1-weighted sagittal MRI, while the midthoracic spine showed a heterogeneous signal on T2-weighted sagittal MRI (Figure 1c, d). The topography of the mass was clearly hyperintense at L1 to L2 levels on post-contrast T1-weighted sagittal and axial MRI (Figure 1e, f). The lesion was about 4.3 cm × 2.1 cm × 1.0 cm. Intraspinal epidural fatty lesions were suspected based on the MRI results.

(a) T1-weighted sagittal magnetic resonance imaging (MRI) showing lesion (arrow) as nearly isointense with normalfat and hypointense to the spinal cord. (b) T2-weighted sagittal MRI of midthoracic spine showing heterogeneoussignal in the lesion (arrow). (c) Post-contrast T1-weighted sagittal MRI showing maximalenhancement of the lesion (arrow), extending from L1 to L2. The tumor shows a large component hypointenseto fat and hyperintense to vascular channels. (d) Post-contrast T1-weighted axial MRI showing “noodle” sign (arrow). (e) Sagittal lumbar computed tomography (CT) showing low-density posterior extradural mass(arrow) extending from L1 to L2. (f) Transverse lumbar CT showing compressed spinal cord (arrow). (g, h) Postoperative X-ray showing internal fixation in place. (i) Histopathological image (hematoxylin-eosin staining, ×100) showing mature adipose tissue with numerous small vascular channels.
After explaining the condition to the patient in detail, we chose to carry out surgery. An L1 to L2 laminotomy was carried and a 5-cm × 2-cm × 1-cm mass was totally removed, followed by internal fixation to stabilize the lumbar spine (Figure 1g, h). Postoperative X-ray and CT revealed total resection of the tumor and the well-placed internal fixation. Histopathological examination of the mass showed mature adipose tissue with numerous small vascular channels (Figure 1i).
The patient’s back pain was significantly relieved after the operation, with a decrease in visual analog scale (VAS) pain score from 9 preoperatively to 2 postoperatively. The patient was discharged home 2 weeks postoperation. She reported a greatly improved quality of life and significant pain relief at 1 year of follow-up.
Case 2
A 61-year-old man presented with a 6-year history of progressively worsening back pain. However, he ignored the pain until 2 months prior to admission, when he noted aggravated back pain and a sudden increase in radiation pain, numbness, and weakness in both legs, resulting in an inability to walk. His medical history revealed hypertension and type 2 diabetes for 5 years. His BMI was 27.8 kg/m2.
Physical examination showed hyperreflexia of both legs. Pinprick sensation was severely decreased (2/10) below the T5 dermatome level, muscular weakness was seen in the iliopsoas (3/3), quadriceps (3/3), and tibialis anterior (4/4), and the results of a bilateral straight leg-raising test were negative.
The results of plain radiography and laboratory tests were normal. CT revealed a low-density shadow from T5 to T7 (Figure 2e, f). MRI examination of the midthoracic spine was performed, and T1-weighted sagittal MRI showed a hypointense lesion, while T2-weighted sagittal MRI showed a heterogeneous signal (Figure 2a, b). Post-contrast T2-weighted sagittal MRI showed the lesion as an enhanced hyperintense signal extending from T5 to T7 (Figure 2c). The spinal cord was compressed and displaced anteriorly (Figure 2d). The lesion was about 4.8 cm × 2.5 cm × 1.5 cm. The MRI results suggested an epidural benign lesion, with a high fat content.
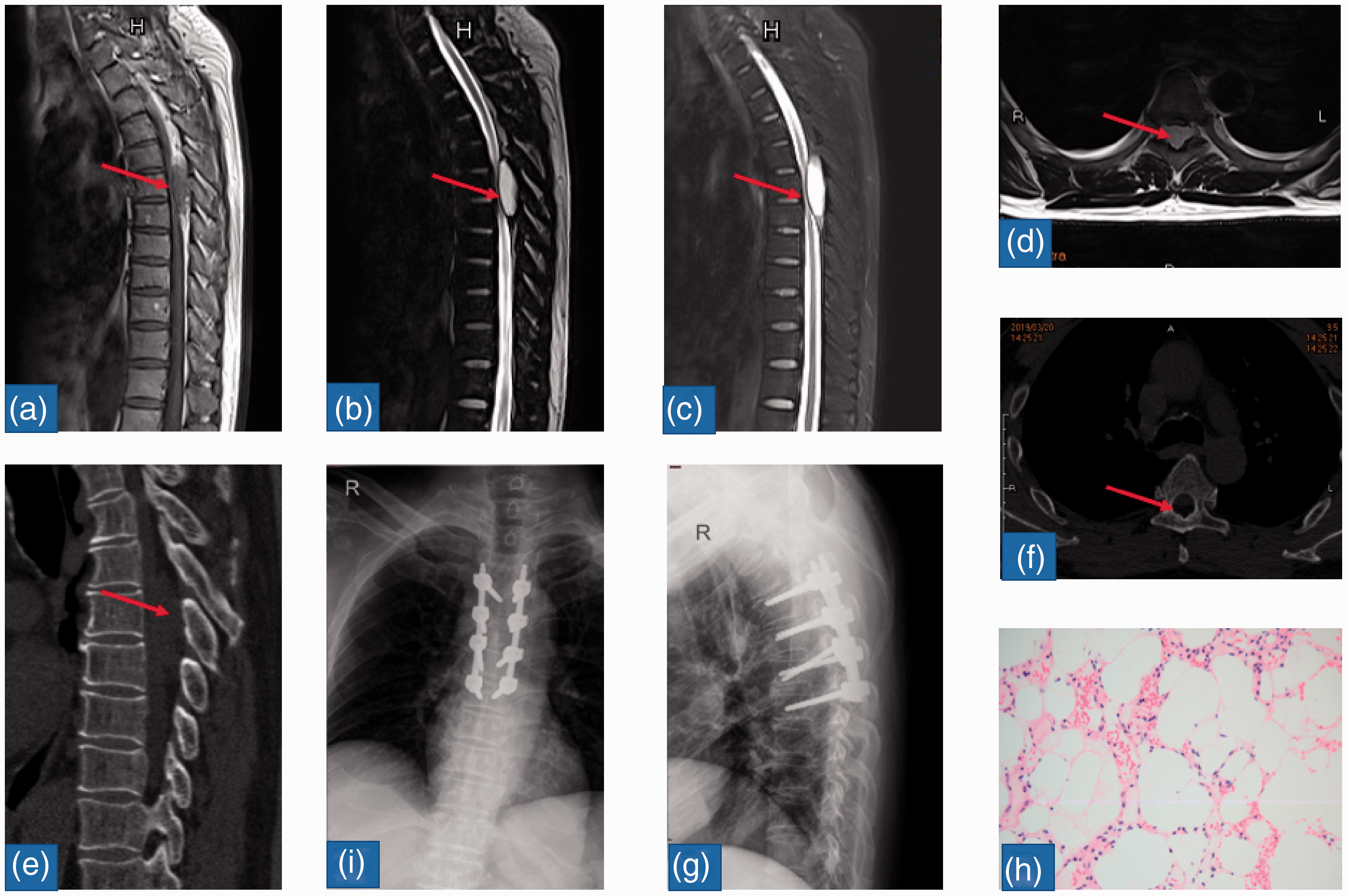
(a) T1-weighted sagittal magnetic resonance imaging (MRI) of the midthoracic spine showing hypointense lesion (arrow). (b) T2-weighted sagittal MRI of the midthoracic spine showing heterogeneous signal in the lesion (arrow). (c) Short-TI inversion recovery sequence of T2-weighted sagittal MRI showing tumor (arrow) extending from T5 to T7. (d) T2-weighted axial MRI showing “noodle” sign (arrow). (e) Sagittal lumbar computed tomography (CT) showing low-density posterior extradural mass (arrow). (f) Axial thoracic CT showing compressed spinal cord (arrow). (g, i) Postoperative X-ray showing internal fixation in place. (h) Histopathological image (hematoxylin–eosin staining, ×100) showing mature adipose tissue with numerous small vascular channels.
Surgery was carried out to decompress the T4 to T7 spinal cord via laminotomy, together with internal fixation to stabilize the thoracic spine (Fig. 2g, h). We achieved complete resection after dissecting the tissue around the lesion. The mass was yellow and measured about 5.0 cm × 2.4 cm × 1.8 cm. Histopathological examination of the mass showed mature adipocytes interlaced with numerous small vascular channels (Figure 2i).
The patient recovered well after the operation. His symptoms including back pain, radiation pain, numbness, and weakness resolved, and he was able to walk again. His VAS score decreased from 8 preoperatively to 2 postoperatively. The patient was very pleased with the outcome, and reported no back pain, radiation pain, numbness, or weakness in either leg, and there was no recurrence on MRI, at 1 year of follow-up.
Discussion
SALs are extremely rare benign tumors, first reported in 1890, with up to 200 reported cases. 2 SALs have been reported in patients between 1.5 and 85 years old, with most occurring between 40 and 60 years, predominantly in women.6–8 A few cases of SALs in children have been described. 6 SALs may be located in the cervical, thoracic, or lumbar region,9–11 with most occurring in the thoracic region.6,12 SALs usually involve two to three vertebral segments, and lesions including more than six segments are rare.8,13 The main features of SALs based on reported studies are shown in Table 1.
Features of spinal angiolipomas in the literature.
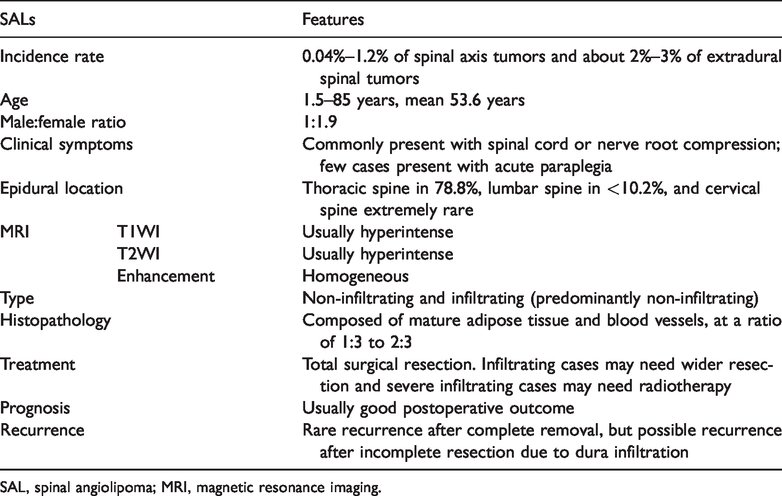
SAL, spinal angiolipoma; MRI, magnetic resonance imaging.
Despite increasing numbers of reported cases, the etiology of SALs remains to be elucidated. Some studies suggest that SALs may originate from primitive, pluripotent mesenchyme tissue 14 and congenital malformations, 15 and an abnormal developmental origin was proposed based on the finding of SALs in patients with birth defects outside the central nervous system. 4 Some authors have presumed that SALs may arise from pluripotent stem cells with secretory activity. 16 Various pathogenic mechanisms may thus be responsible for SALs.
Lin and Lin categorized SALs into two types: non-infiltrating and infiltrating. 17 Non-infiltrating SALs, as the major type of lesion, are encapsulated and present a benign prognosis. They are always located in the posterior or posterolateral spinal canal, and do not invade the vertebrae or adjacent tissues. 2 In contrast, infiltrating SALs are non-encapsulated and may extend into the vertebrae and adjacent tissues.18–20 Most patients have a good prognosis after surgery, but some patients may experience recurrence as a result of incomplete resection, due to dura infiltration.21,22 Non-infiltrative SALs are more common in female patients, and infiltrative SALs have similar frequencies in male and female patients.7,23
The clinical signs and symptoms of SALs are similar to those of spinal cord or nerve root compression, although the severity varies according to the lesion location and proliferation rate. Idiosyncratic complaints are typically sensory disorders and motor deficits below the level of the lesion, and these symptoms usually progress over the course of months,24,25 ultimately leading to weakness in the lower limbs in the later stages. The diagnosis always takes more than 1 year. Previous studies have also demonstrated that pregnancy, weight gain, and other factors may accelerate the progress of SALs.22,26,27 Critical onset or aggravated neurological symptoms occur if the lesion grows rapidly because of tumor thrombosis and/or hemorrhage.28–31
X-rays of the spine often show negative results in patients with SALs, but might show erosion of the walls of the bodies and pedicles as a result of infiltrating tumors.8,32 Myelography was performed in some cases and showed a characteristic posterior extradural spinal lesion with partial or complete filling defect. 6 Angiography was performed in two reported cases and showed prominent vascularity in T9 33 and T6. 34 CT scans may reveal low or intermediate-density lesions in patients with SALs,35–37 and might also reveal tumor calcification, 38 trabeculation, 39 and erosion of the vertebral body and pedicle. 8 Positron emission tomography/CT showed slightly increased fluorodeoxyglucose uptake patients with SALs. 40 MRI is considered to be the most valuable radiological technique for diagnosing SALs, demonstrating features including: 1) a spindle-shaped lesion attached to the dura mater in sagittal aspect; 2) spinal cord shifted to the opposite side characterized by a “noodle” sign; and 3) adipose tissue hyperintense on both T1-weighted and T2-weighted images and hypointense on fat-suppressed images, blood vessels hypointense on T1-weighted images and hyperintense on T2-weighted images, and remarkably homogeneous enhancement after injection of Gd-DTPA.35,38,40–43
Histopathologically, SALs are composed of two distinct characteristic components: mature adipose tissue and blood vessels,44,45 with a ratio of fat to vessels ranging from 1:3 to 2:3. 46 The mature adipose tissues appear normal, and the blood channels include capillaries, thin- or thick-walled vessels, and occasional small arteries. 42 The histogenesis and pathogenesis of angiolipomas are poorly understood, but several theories have been discussed. Angiolipomas are more likely to arise from abnormal primitive pluripotent mesenchymal cells by divergent differentiation along with lipomatosis, and angiomatous and mixed tissues. 47 Some authors suggested that angiolipomas may arise from primitive mesenchyme.14,48 Willis, however, held the view that angiolipomas are congenital malformations or benign hamartomas, 6 while other authors 49 also insisted that they may have an abnormal developmental origin, based on the finding of SALs in patients with birth defects outside the CNS.
The standard treatment for both non-infiltrating and infiltrating SALs is total surgical resection of the lesion via an anterior approach, posterior laminectomy, or microsurgery.18,50,51 In the current cases, we carried out total surgical resection of the lesions via a posterior approach, with resolution of the presenting symptoms. However, the posterior column structures, especially the supraspinal ligaments and interspinal ligaments that play an important role in maintaining the stability of the spine, were destroyed during surgery, and we therefore used internal fixation devices to stabilize the spine in both cases. It is more difficult to achieve total resection in patients with infiltrating SALs because the lesions invade the vertebrae or adjacent tissues. Some authors recommend wider resection for infiltrating angiolipomas, 17 although others believe that the tumor-invaded vertebral body should be retained. 34 Some previous studies used more aggressive treatment, including postoperative radiotherapy, because of concerns over potential malignancy. 6 Conversely, adjuvant chemotherapy or radiotherapy was not recommended for SALs, and there was no difference in outcomes in relation to the use of adjuvant chemotherapy or readiotherapy.4,18,52 Although postoperative radiotherapy was administered in a few cases, adjuvant radiotherapy should not be applied, given that the prognosis of this benign pathological entity, even in the infiltrating group, is very good. Recurrence of SALs after complete removal was rare, 6 but myelopathy may recur following incomplete resection of SALs due to dura infiltration. 22
Conclusions
We report two cases of SALs that demonstrated typical features on MRI, including iso- or hyperintensity on T1-weighted images and hyperintensity on T2-weighted images. SALs are rare benign tumors, composed of both mature fatty tissue and anomalous vascular channels, with good postoperative outcomes. It is therefore important to achieve complete resection of lesions responsible for severe clinical symptoms.
Footnotes
Consent
Written informed consent was obtained from the patients for publication of these cases reports and any accompanying images.
Declaration of conflicting interest
The authors declare that there is no conflict of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.