
Abstract
Background:
Rapid and accurate diagnosis of musculoskeletal infection in children is critical to enable appropriate, targeted surgical interventions. Distinguishing between septic arthritis, myositis, and osteomyelitis around the hip can be difficult using clinical criteria and ultrasound scan alone.
Materials and methods:
We performed a retrospective 5-year observational review of selective magnetic resonance imaging scanning for hip sepsis in a pediatric tertiary referral center. Included were children with atraumatic hip pain with symptom duration <2 weeks, minimum of two positive modified Kocher’s criteria, and a hip effusion on ultrasound. All cases were followed up to discharge. We evaluated hip ultrasound and magnetic resonance imaging findings, operative procedures, microbiology results, duration of treatment, outcomes, and complications.
Results:
Fifty-one patients, 55% male, with a mean age 6.4 (0–16) years were included. Thirty-nine underwent magnetic resonance imaging scan for suspected septic arthritis of the hip; 24 prior to surgical washout (pre-emptive), and 15 afterwards (postoperative). In the pre-emptive group, 1/24 had septic arthritis, 7/24 had osteomyelitis, 6/24 had myositis, 5/24 had osteomyelitis and myositis, and 5/24 had no evidence of infective pathology. In the postoperative group, 3/15 had myositis, 3/15 had osteomyelitis, 3/15 had re-accumulation of the hip effusion requiring repeat washout, 3/15 had myositis and osteomyelitis, and 1/15 had septic arthritis of a contiguous joint.
Conclusion:
Pre-emptive magnetic resonance imaging scanning avoided unnecessary hip washout in 23 cases and enabled targeted drainage of an alternative focus in four of those. Magnetic resonance imaging scanning after hip washout indicated that four cases required further surgery to drain a different focus of infection.
Introduction
Septic arthritis of the hip is a surgical emergency. Delayed treatment risks serious complications that include chondrolysis, osteonecrosis, and systemic sepsis. Clinical and laboratory criteria for diagnosis have the potential for high sensitivity depending on the threshold set, but there may be a high number of false positives. 1 Submitting an unwell child to general anesthesia to wash clear fluid out of the hip joint is a disappointing experience that does not further the investigation of a cause for the illness.
The use of magnetic resonance imaging (MRI) scanning in the evaluation of children with suspected hip joint infection can improve diagnostic accuracy. Myositis used to be considered rare outside tropical environments and case reportable, 2 but the incidence of diagnosis has increased; either because it has become more common or because of the increasing availability of MRI to diagnose it. In a recent American series, selective MRI scanning of pediatric hips at presentation found a surprisingly high 35% rate of pericapsular myositis, with a reactive but sterile hip joint effusion, among 53 children with clinical features suggestive of septic arthritis. 3
Only 15% had joint infection. The authors concluded that inaccurate diagnosis can lead to unnecessary debridement of the hip in the presence of extra-articular infection, potentially contaminating the joint, and miss other important diagnoses such as co-existent osteomyelitis. This study was carried out in a tertiary pediatric referral center in Nashville, TN, USA. Another study found a preponderance of serious complications—osteonecrosis, chondrolysis, growth disturbance, and pathological fracture, in septic arthritis with contiguous osteomyelitis. 4 They concluded that primary septic arthritis and the same with contiguous osteomyelitis differ to such an extent in their propensities for adverse sequelae that they should be differentiated early and managed differently.
Since 2010, our protocol for the unwell child with an acutely irritable hip and a joint effusion on ultrasound has been for pre-emptive MRI scanning if there is uncertainty around the diagnosis of septic arthritis based on a low number of clinical criteria or equivocal effusion on ultrasound scan. An MRI scanner in the operating theater corridor enables direct transfer to an operating theater, under general anesthesia if already anesthetized, if joint washout or drainage of a collection is required. This is typically available in tertiary children’s facilities but may be less common in non-specialist hospitals. We also have a low threshold for MRI scanning children who fail to improve after hip exploration without a pre-emptive scan. We have collected and analyzed data for both groups to test the following hypotheses: first that pericapsular myositis is at least as common as septic arthritis in this group; second that some clinical features might predict for the presence of myositis rather than septic arthritis; third that children with septic arthritis and contiguous osteomyelitis have a different outcome profile compared to those with septic arthritis alone.
Methods
We performed a retrospective observational review of all children referred to us for the evaluation of potential hip joint infection over a 5-year period from the beginning of 2010 to the end of 2014. Our institution is a dedicated tertiary referral pediatric facility and the major trauma center for children in the southwest of England. Inclusion criteria were age 0–16 years, acute presentation with symptom duration less than 2 weeks, symptoms and signs localized to one hip, the presence of two or more positive Kocher et al.’s5,6 criteria, and signs of a hip effusion on ultrasound scan. Children were excluded if there was a known inflammatory arthropathy or plain radiographic changes of established osteomyelitis at presentation.
Data for clinical features, blood tests, radiological investigations, surgical interventions, follow-up, complications, and outcomes were collected. Ultrasound and MRI scans were performed or reported by a specialist pediatric radiologist. All diagnoses made from initial clinical and radiological assessment were cross-checked with follow-up records to confirm accuracy. Positive modified Kocher’s criteria suggestive of septic arthritis were defined as white blood cell (WBC) >12 × 103/L, non-weight-bearing, fever >38.5°C, and c-reactive protein (CRP) >20 mg/L. 7 Transient synovitis was a diagnosis of exclusion if a benign clinical course followed a presentation of atraumatic hip pain with a joint effusion on ultrasound and 0–1 positive Kocher’s criteria only.
The National Health Service (NHS) costs of a pediatric pelvic MRI range between £170 and £200 depending on the age of child and whether contrast is administered. Statistical univariate analysis was performed using the Mann–Whitney U test for continuous variables and Fisher’s exact test for categorical variables. p-values of <0.05 were considered statistically significant. Formal ethical approval for this retrospective study was not required by our institution.
Results
One hundred fifty-two children were referred to our service with atraumatic hip pain and a hip joint effusion during the study period. One hundred and one were diagnosed with transient synovitis with a benign clinical course at follow-up without treatment. There was no case of missed sepsis in this group during the study period.
Fifty-one remaining cases fulfilled the inclusion criteria. They had a mean age of 6.4 years (5 weeks–16.6 years); 55% were male. They were discharged from routine follow-up at a mean 22 months (6 months–10 years).
Group 1 (pre-emptive MRI)
Twenty-four of 51 children had a modest or equivocal hip joint effusion at presentation. Two had reported ultrasound signs of possible osteomyelitis and two of possible myositis. There was no joint debris on any of these 24 ultrasounds. A reactive effusion to an adjacent focus of infection rather than primary septic arthritis was considered possible. Of these twenty-four patients, eight had two positive Kocher’s criteria, eleven had three positive Kocher’s criteria, and five had four positive Kocher’s criteria. This group underwent urgent MRI scanning prior to treatment (Table 1). Half (12 patients) were under 5 years of age, and therefore required general anesthesia for the MRI scan. The average time from presentation in the emergency department to ultrasound scan was 2.25 h (range = 1–4.75 h). The average time between the ultrasound and MRI was 5 h (range = 1.9–13 h). The longer waits were in the eight children with two positive criteria only in whom septic arthritis was less likely. No child with three or more positive Kocher’s criteria and a joint effusion on ultrasound waited more than 4 h for MRI scan, which time included induction of general anesthesia for children under 5 years of age.
Results of selective pre-emptive MRI scanning (n = 24).
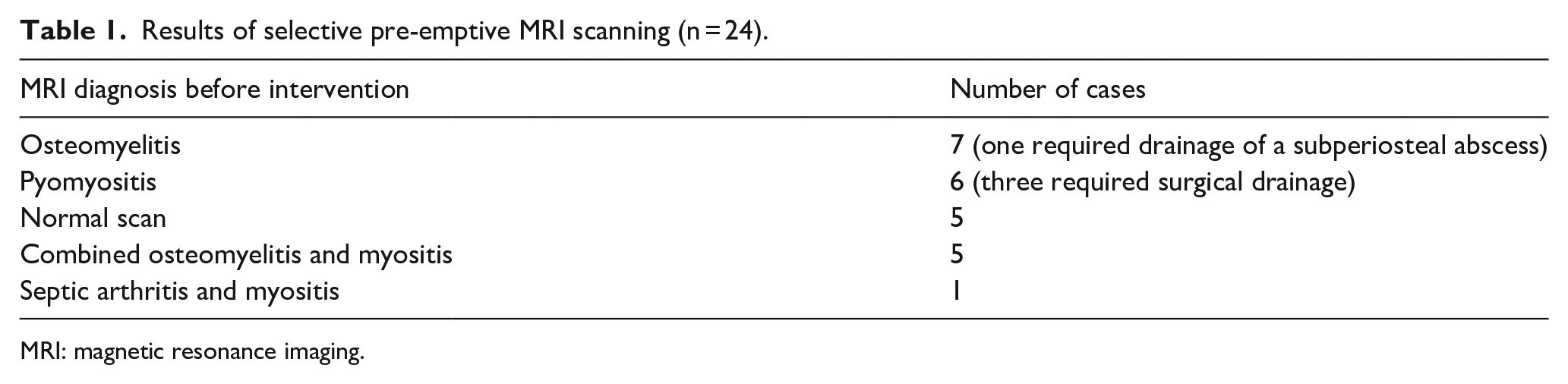
MRI: magnetic resonance imaging.
Only one case had septic arthritis in this group. This patient was female, 7 years old, and had three positive Kocher’s criteria at presentation, but the ultrasound scan, performed 1.5 h after presentation, reported an equivocal hip effusion. She was admitted for overnight observation and blood cultures, her hip became more irritable the following day and an awake MRI demonstrated a small hip joint effusion with pericapsular myositis. Blood cultures returned positive growth for coagulase-negative Staphylococcus and the CRP increased. She was taken to theater the same day for hip aspirate that yielded pus. She underwent arthrotomy, washout, and tunneled intravenous line insertion. After 6 weeks of antibiotics, she made a good recovery without further intervention. There was no adjacent osteomyelitis, and there were no long-term adverse sequelae. She was discharged to open review after 18 months follow-up.
Eighteen cases had MRI diagnosis of an infective focus that was not septic arthritis. Seven had isolated osteomyelitis that underwent biopsy in four cases. The locations were as follows: two in the ilium; two in the proximal femur; one in the distal femur; one in the proximal tibia; and one multifocal affecting the pelvis and proximal femur. Six had isolated myositis affecting the gluteal, adductor, psoas, obturator externus, and iliopsoas muscles. Five had MRI signs of both: osteomyelitis of the sacroiliac region and myositis of the piriformis muscle; pelvic osteomyelitis and myositis in the obturator externus (Figure 1); proximal femoral osteomyelitis and adductor myositis; and iliac osteomyelitis and gluteal myositis. Ten children were successfully managed non-operatively with empirical or blood culture–directed antibiotics. Four children required targeted surgical drainage of a pyomyositis or subperiosteal abscess. Two had a medial approach to drain a pyomyositis from the adductor compartment; 8 one was explored for proximal femoral osteomyelitis with associated subperiosteal abscess; and one underwent drainage of an iliacus pyomyositis via an anterior approach to the pelvis.
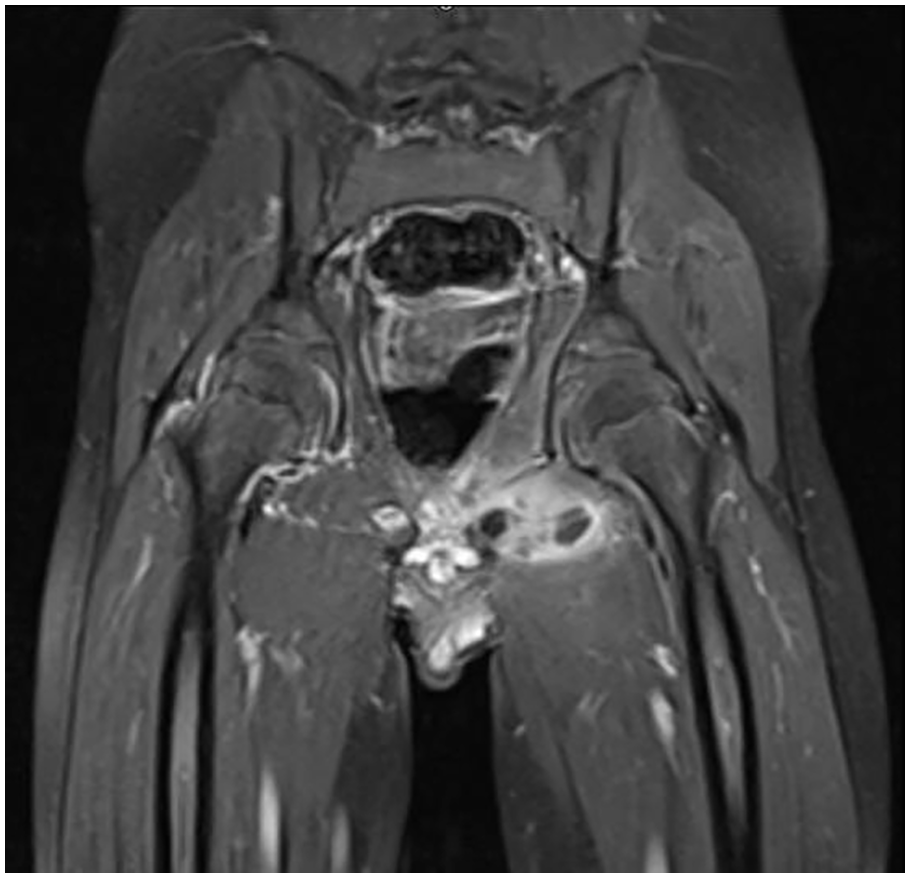
Myositis of left obturator externus muscle (T2-weighted coronal MRI with gadolinium enhancement).
In five cases, the MRI scan did not confirm a hip joint effusion, and no cause for the abnormal clinical signs was found. One had a further outpatient MRI at 3 months which remained reassuring. All were discharged after a short period of follow-up.
Group 2 (postoperative MRI)
Twenty-seven of 51 children had 2 or more Kocher’s criteria and ultrasound confirmation of a significant hip joint effusion. Two of these ultrasound scans reported debris within the joint, two had co-existent ultrasound-reported signs of myositis without abscess formation, and one had ultrasound-reported signs of proximal metaphyseal femoral osteomyelitis. Of these 27 patients, 3 had 2 positive Kocher’s criteria, 14 had 3 positive Kocher’s criteria and 10 had 4 positive Kocher’s criteria. All 27 had proceeded directly to hip joint aspiration, arthrotomy, and open washout under general anesthesia as an emergency without pre-emptive MRI. The average time between ultrasound scan and washout was 2.25 h (range = 1.5–4.75 h). One case had clear fluid aspirated, and therefore did not undergo open washout. This patient was treated for severe cellulitis with antibiotics. The remainder aspirated turbid fluid (7) or pus (19) and had open hip joint washouts. Eight of these fluid samples grew Staphylococcus aureus, five beta hemolytic Streptococcus, four Group A Streptococcus, one Escherichia coli, and one grew a mixture of Group A Streptococcus and S. aureus. Four samples had no organism identified; unfortunately, we do not have data for the last three samples. An anterior approach was used in the interval between the tensor fascia lata and sartorius muscles. The origin of rectus femoris was preserved. A “T” or “H”-shaped capsulotomy was left open. No drains were sited. No exploration of adjacent bone or muscle for infection was undertaken.
Postoperatively, 11 children responded well to treatment with antibiotics after a single washout. Fifteen children failed to improve with persisting fever, elevated CRP, and inability to weight bear on the affected side. They underwent postoperative MRI scanning during the same admission at 48–72 h from surgery (Table 2).
Results of postoperative MRI scan after unsatisfactory hip washout (n = 15).
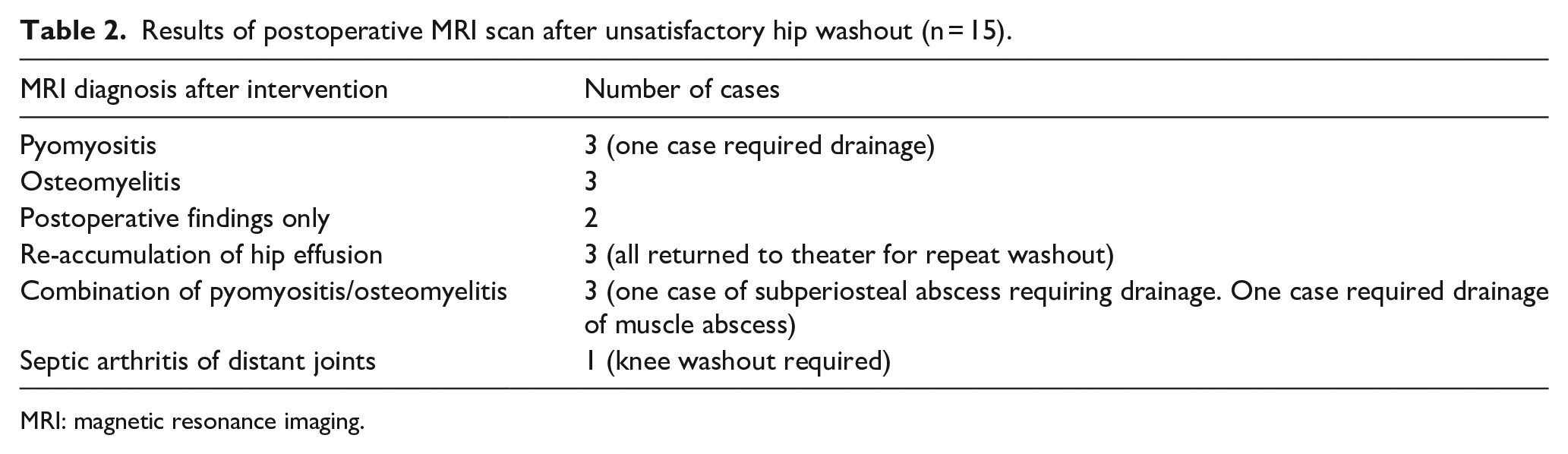
MRI: magnetic resonance imaging.
Two scans showed postoperative changes only with no additional focus identified. There were three cases of myositis: one of the left gluteus maximus, one of pectineus and iliopsoas, and one of the obturator internus. There were three cases of osteomyelitis: one affecting the ipsilateral talus with an isolated organism of beta hemolytic Streptococcus, two of the proximal femoral metaphysis, one with an isolated organism of Group B Streptococcus and the other did not have data available identifying an organism. Three cases showed re-accumulation of the hip effusion and underwent repeat washout in theater via the same anterior approach. One case had developed a subperiosteal collection of the distal femoral metaphysis and diaphysis with adjacent myositis of the anterolateral thigh requiring surgical drainage. One child had developed an iliacus abscess in the left hemi-pelvis that was jointly explored and decompressed over the superior pubic ramus with the pediatric surgical and orthopedic teams. The collection had a deep tract that tracked to the hip joint which was washed out again. The organism was S. aureus. There was one case of muscle abscess involving biceps femoris and semitendinosus, with adjacent ischial osteomyelitis, that underwent surgical drainage. One child developed multifocal sepsis with effusions of the knee and elbow that were washed out arthroscopically and by arthrotomy, respectively. The organism isolated in this case was Group A Streptococcus.
In total, therefore seven children required a return to theater after the MRI scan; four for foci outside the hip that had not been identified on the preoperative ultrasound scan. The remaining eight children were managed with ongoing antibiotics for myositis, osteomyelitis, or presumed septic arthritis that had been adequately treated without requirement for a further hip joint or other debridement. Ten children had undergone hip washout that was potentially avoidable based on the postoperative MRI scan.
Clinical risk factors
Univariate analysis of age, sex, and the modified Kocher’s risk factors indicated that only weight-bearing status might be helpful to differentiate septic arthritis of the hip from pericapsular infection (Table 3). Patients with pericapsular myositis without septic arthritis were more likely to weight bear at presentation than those diagnosed with septic arthritis (p < 0.05).
Clinical predictors of extra capsular infection or septic arthritis.
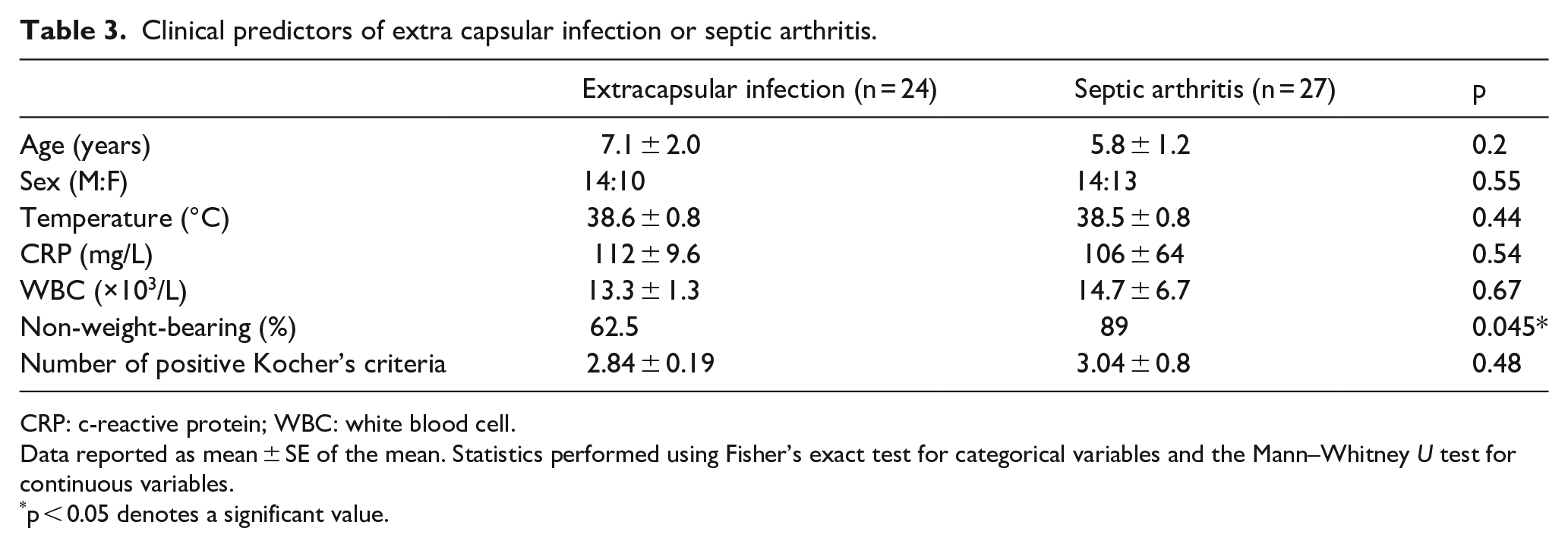
CRP: c-reactive protein; WBC: white blood cell.
Data reported as mean ± SE of the mean. Statistics performed using Fisher’s exact test for categorical variables and the Mann–Whitney U test for continuous variables.
p < 0.05 denotes a significant value.
Outcomes
The mean time to discharge from follow-up for the study group of 51 cases was 22 months (1 month–10 years). Longer follow-up was required for combined osteomyelitis and myositis whereas myositis alone had the shortest time to discharge with isolated septic arthritis in between (Table 4).
Mean time to discharge by diagnosis.

There were six major complications (Table 5). Growth disturbance was associated with osteomyelitis with or without septic arthritis. Femoral head osteonecrosis developed in two cases of septic arthritis with contiguous osteomyelitis and one case of pyomyositis.
Major complications.

Discussion
The first hypothesis that pericapsular myositis is at least as common as septic arthritis, in children presenting with two or more Kocher’s criteria and a hip joint effusion, is supported by this study.9,10 There were nine cases of isolated pyomyositis and eight cases of combined pyomyositis and osteomyelitis compared to 17 cases of septic arthritis (involving the ipsilateral hip joint). There were also nine cases of isolated osteomyelitis. Caution is therefore required when considering surgical drainage of a hip effusion with clinical criteria suggestive of septic arthritis because there is a risk of seeding a joint that is not the primary focus of infection.
Pre-emptive MRI scanning of 24 selective cases (47%) where there was clinical suspicion of a reactive effusion did not delay hip joint washout in the one case of septic arthritis in this group. On the contrary, it confirmed this diagnosis after an equivocal ultrasound scan. The remaining 23 cases had a normal MRI scan (5 cases) or an adjacent focus of infection (18 cases). Unnecessary surgery was avoided in this group, and targeted drainage was performed in four cases—three for muscle abscess and one for subperiosteal abscess (Table 1). Ultrasound alone did not identify these alternative important diagnoses.
Twelve cases (24%) did not undergo MRI scanning. They improved after hip washout based on Kocher’s criteria and the presence of a hip effusion on ultrasound scan. There were no adverse sequelae in this group. Preoperative MRI scanning is not likely to have refined the diagnosis in this group and would probably have delayed hip joint washout.
Fifteen cases did not improve after hip washout. Postoperative MRI scanning indicated the requirement for a return to theater in seven cases—four for foci in adjacent muscle or bone that had not been identified on the preoperative ultrasound scan and three for re-accumulation of pus in the joint. Ten children in this group had undergone hip washout that may not have been necessary in all cases (Table 2).
Overall, 18/51 (35%) cases fulfilling inclusion criteria, of a hip effusion and two or more positive Kocher’s criteria, had septic arthritis. This is exactly the same figure as Mignemi et al.; 3 pericapsular myositis of the hip is indeed common nowadays even in populations living in a temperate climate. 2 Our interpretation is that universal pre-emptive MRI scanning would probably have avoided unnecessary hip washout in most of the remaining 33 cases (65%) among whom 8 instead required targeted drainage of a muscle or bone abscess. Only half of those eight cases avoided hip washout, that might have seeded the joint from the adjacent focus, with our selective use of pre-emptive MRI scanning. Another six cases are not likely to have benefited from their hip washout in this series.
We believe therefore that universal pre-emptive MRI scanning has potential merit, for children with two or more Kocher’s criteria and a hip joint effusion on ultrasound, provided there is no substantial delay to washout in those cases that require it. This is based on the fact that only 35% of these cases had septic arthritis. Universal pre-emptive MRI would have avoided unnecessary washout in 10 cases (20%) in this 5-year series using a protocol of selective MRI. Without MRI, up to 33 more cases (65%) would potentially have undergone unnecessary washout. However, hip washout could have been delayed by up to 4 h on average in those 18 cases that required it; except that in many cases this included time for general anesthesia that was maintained for the hip joint washout.
Even with an MRI scanner in the operating theater corridor, it is difficult logistically to combine scheduling of an urgent MRI scan with availability of an anesthetic team and an emergency operating theater on standby. This can be justified on the basis of cost, by avoiding unnecessary surgery, and quality, by achieving an early, accurate diagnosis. We acknowledge that it is a challenge to set up this protocol; however, clinical and managerial staff recognize that, as often as not, the MRI scan dictates non-operative management. This frees up an emergency theater in which a hip joint would otherwise have been explored. The cost of an MRI scan compares favorably that of an operating theater (approximately £16 per minute).
MRI is the gold standard investigation for diagnosing adjacent infection in pediatric patients with septic arthritis. 11 It is highly sensitive and specific. 12 Adjacent infection has been reported in up to 60% of septic arthritis cases, 13 many of which may require operative intervention. This study confirms that ultrasound is helpful for diagnosis in cases of florid septic arthritis but has poor sensitivity for alternative and co-existent diagnoses. In three cases, the MRI identified a collection, in muscle or the subperiosteal space, of sufficient size to drain. In one of these cases, we found muscle edema rather than pus, but swab samples nonetheless yielded the causative organism. In the other 2 cases, we found frank pus as predicted by the MRI scan.
Our second hypothesis, that some clinical features might predict for the presence of myositis rather than septic arthritis, is partially supported by this study. The inability to weight bear was more strongly associated with septic arthritis than myositis (Table 3). This might be helpful to inform a protocol of selective pre-emptive MRI scanning. However, analysis of small subgroups in this way is methodologically poor. The ability to weight bear most definitely does not exclude septic arthritis but may tip the balance in favor of pre-emptive MRI scan in the absence of a large hip joint effusion with debris.
Our third hypothesis, that children with septic arthritis and contiguous osteomyelitis have a different outcome profile, compared to those with septic arthritis alone, is supported by this study. Follow-up was longer in cases where there was contiguous osteomyelitis and/or myositis. Major complications were seen only in subgroups of septic arthritis with myositis, 2 septic arthritis with osteomyelitis, 2 and isolated osteomyelitis, but these subgroups were also small (Table 4).
Limitations
This study is limited by its retrospective design and small subgroup numbers as discussed above. Septic arthritis is an uncommon but serious condition. We have reviewed a 5-year period of practice after a reasonable length of follow-up. We acknowledge that our findings may not be applicable to centers with limited access to MRI scanning in close proximity to an emergency operating theater.
Conclusion
We conclude that the decision to proceed with hip washout for septic arthritis based on Kocher’s criteria and ultrasound evaluation will be incorrect at least 50% of the time when a cut-off of two or more criteria is used. Ultrasound scan is reliable in the detection of a florid effusion but cannot diagnose pericapsular myositis and osteomyelitis in routine practice or distinguish a primary from a reactive effusion. Selective use of MRI reduces the rate of unnecessary hip washout and enables prompt, targeted drainage of pericapsular infection when indicated. Universal pre-emptive MRI scanning has the potential further to reduce the rate of unnecessary hip joint washout, avoid seeding of the joint from an alternative focus, predict early those cases for whom major complications are more likely, and target treatment in the majority who does not have septic arthritis. 14 This could only be justified, in our opinion, if resources enable it to be done without undue delay of hip washout in the minority of cases that require it.
Footnotes
Author contributions
N.C. contributed to the methodology, formal analysis, investigation, writing—original draft, and review and editing. S.B. contributed to the conceptualization, methodology, formal analysis, investigation, writing—original draft, and review and editing. J.H. contributed to the formal analysis, investigation, writing—original draft, and review and editing. S.T. contributed to the conceptualization, methodology, formal analysis, investigation, writing—original draft, and review and editing.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.