
Abstract
Purpose:
There is marked variation in indications and techniques for hamstring surgery in children with cerebral palsy. There is particular uncertainty regarding the indications for hamstring transfer compared to traditional hamstring lengthening. The purpose of this study was for an international panel of experts to use the Delphi method to establish consensus indications for hamstring surgery in ambulatory children with cerebral palsy.
Methods:
The panel used a five-level Likert-type scale to record agreement or disagreement with statements regarding hamstring surgery, including surgical indications and techniques, post-operative care, and outcome measures. Consensus was defined as at least 80% of responses being in the highest or lowest two of the five Likert-type ratings. General agreement was defined as 60%–79% falling into the highest or lowest two ratings. There was no agreement if neither of these thresholds was reached.
Results:
The panel reached consensus or general agreement for 38 (84%) of 45 statements regarding hamstring surgery. The panel noted the importance of assessing pelvic tilt during gait when considering hamstring surgery, and also that lateral hamstring lengthening is rarely needed, particularly at the index surgery. They noted that repeat hamstring lengthening often has poor outcomes. The panel was divided regarding hamstring transfer surgery, with only half performing such surgery.
Conclusion:
The results of this study can help pediatric orthopedic surgeons optimize decision-making in their choice and practice of hamstring surgery for ambulatory children with cerebral palsy. This has the potential to reduce practice variation and significantly improve outcomes for ambulatory children with cerebral palsy.
Level of evidence:
level V.
Introduction
Cerebral palsy (CP) is the most common motor disease of childhood. Despite advances in medical care, CP remains a prevalent problem in children and adults. 1 Currently, there are approximately 17 million people with CP worldwide.
Knee problems, particularly crouch gait, interfere with gait and function, particularly in ambulant children with CP.2–5 Rethlefsen et al. 6 reported crouch in more than 50% of 1005 children and adolescents with CP who presented to a gait laboratory. Even with a high level of consistency in patient evaluation (e.g. through high-quality motion analysis laboratories), there is still marked variability in the application of various interventions, which can result in significant variation in outcomes. Although some of these relate to variation in patient characteristics, much of the variation is surgeon-specific.1,6–10
The goal of this study was to use the Delphi method to establish areas of consensus for surgical indications, intraoperative considerations, and outcome assessment for hamstring lengthening (HSL) and hamstring transfer (HST) surgery in ambulatory children with CP, and to identify where there is less agreement and a need for more evidence.
Research design and methods
We convened an international group of 16 experts with clinical expertise in the treatment of children with CP and the use of computerized gait analysis in an attempt to come to consensus recommendations regarding the care of these children, as previously reported.11,12 The panel consists of pediatric orthopedic surgeons who practice in tertiary orthopedic centers in the United States, Canada, the United Kingdom, Europe, and Australia. The members of the panel had a mean of over 20 years of experience (range: 10–41 years) in the orthopedic care of children with CP and a mean of 19.8 years (range: 7–31 years) of experience using computerized gait analysis in children with CP. No members withdrew.
The panel used consensus methodology (Delphi method) to identify indications (including those for physical examination, observational gait analysis, computerized gait analysis, intraoperative considerations, post-operative care, and outcomes measures) for HSL and HST surgeries for ambulatory children with CP. The Delphi methodology is well established in determining appropriateness criteria in medicine11–14 and was used to assess for consensus. Institutional review board approval for the study and approval from each participating member were obtained.
The panel agreed to and created a structured series of questions that could be assessed using a 5-point Likert-type scale regarding indications, intraoperative considerations, post-operative care, and outcomes measures of success for HSL and HST for ambulatory children with CP. The five rounds of statements and feedback were supplemented with face-to-face meetings of the expert panel as described previously11,12 and were subsequently supplemented by video teleconferences due to the ongoing COVID-19 pandemic. All statements undergo each round of query, unless they already have met criteria for consensus or non-consensus. For each round of statements, an electronic survey was created in REDCap (Version 9.1.0; Vanderbilt University, Nashville, TN, USA) and sent to all panel members, and each responded to the statements autonomously. No statements were dropped from the survey.
Thresholds for consensus were pre-determined. Consensus for agreement occurred when at least 80% of experts selected one of the highest two responses on the 5-point Likert-type scale (strongly agree or agree). Consensus for disagreement occurred when at least 80% of the panel selected one of the lowest two responses (strongly disagree or disagree). General agreement occurred when 60%–79% chose one of the highest two responses, and general disagreement occurred when 60%–79% chose one of the lowest two responses. There was “no consensus” if fewer than 60% of the panel responses were in either the highest or the lowest two categories for a given statement. Opportunity for comments was provided for all statements.
Results
Hamstring lengthening
The panel responded to 38 Likert-type statements regarding HSL. Consensus was reached regarding 21 of these criteria, general agreement for 11, and no consensus for 6.
Regarding physical examination, the panel came to consensus that a popliteal angle >60° may be an indication for HSL, but consensus was not reached for a popliteal angle either > 40° or >50°. There was general agreement that for HSL to be considered, there should be a knee flexion contracture <10°. There was no consensus about the use of the hamstring shift test pre-operatively, but if it was done there was general agreement that a large shift may be a contraindication to HSL.
Many gait parameters met consensus or general agreement as part of the indication criteria. Most of these focused on the level of the knee, but the panel also agreed that pelvic tilt is an important measure in these children. There was consensus that posterior pelvic tilt (PPT) is a strong indication for HSL and that anterior pelvic tilt (APT) is a relative contraindication.
The panel reached consensus regarding many potential indications for HSL which are clarified or confirmed on three-dimensional gait analysis (3DGA), including increased knee flexion at initial contact (especially if >30°), increased minimum knee flexion in stance (especially if >20°), and increased knee flexion in terminal swing. With respect to hamstring modeling data, all respondents agreed that HSL is indicated if hamstrings are both short and slow in swing phase, but only 50% agreed that the hamstrings must be both short and slow to indicate HSL (Figure 1(a) and (b)). When the criteria were separately assessed, 100% agreed that short hamstring length in terminal swing may be an indication for HSL, and 75% agreed that slow hamstring velocity in swing phase may be an indication.15,16
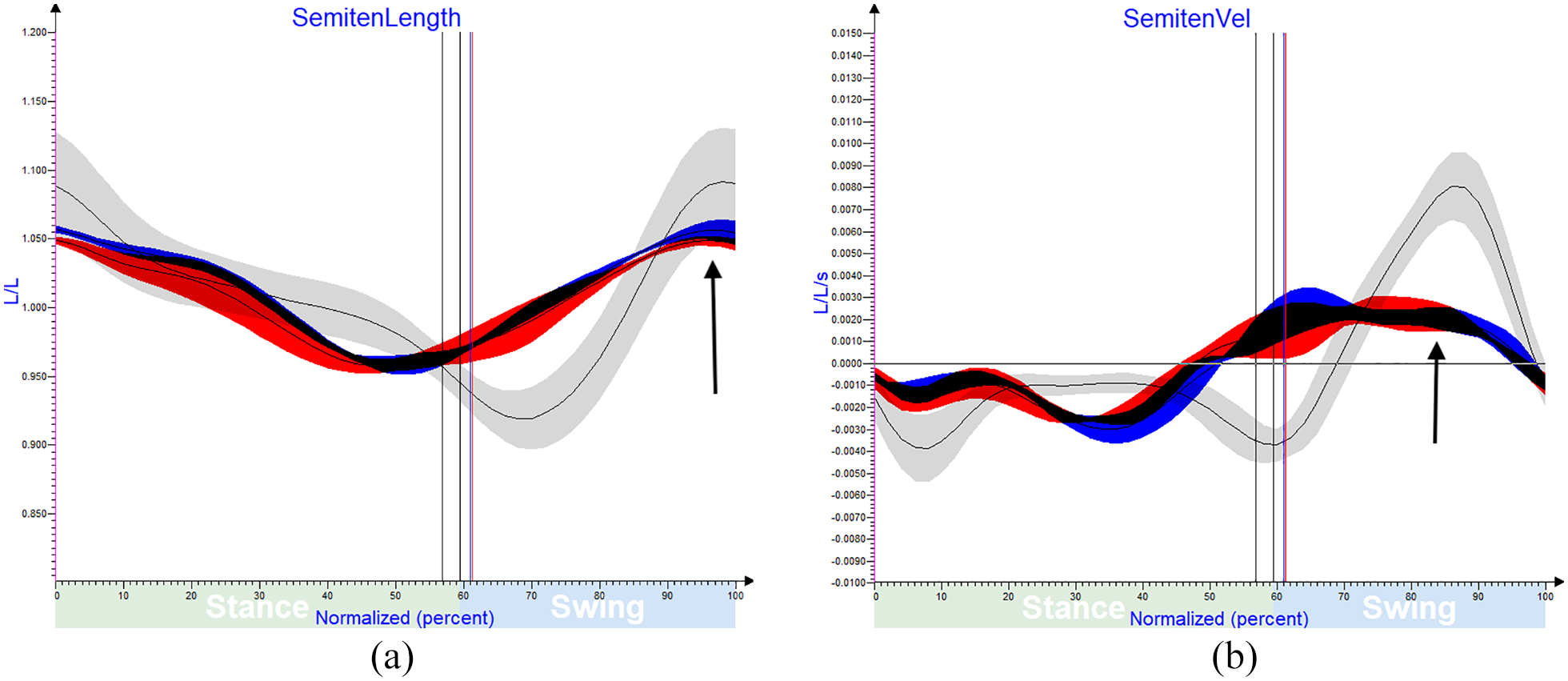
(a) Hamstring lengths for a child with CP. The black line denotes normal hamstring length and the gray area represents 1 standard deviation above and below normal. When the patient traces are below the shaded area, the hamstrings are short. Red denotes the right leg and blue the left. The arrow points to shortened right and left hamstring lengths in terminal swing. (Reproduced with permission of Children’s Orthopaedic Center, Los Angeles) (b) Hamstring velocity with same colors as (a). The arrow points to the slow hamstrings in swing phase bilaterally. In this example, the hamstrings are both short and slow. (Reproduced with permission of Children’s Orthopaedic Center, Los Angeles).
In response to statements about which hamstrings should be lengthened, there was consensus that the indications for combined medial and lateral HSL are very limited in children functioning at Gross Motor Function Classification System (GMFCS) levels I–III. Every expert on the panel agreed with the statement “I rarely (if ever) perform lateral HSL in GMFCS I and GMFCS II children.” For children functioning at GMFCS III, 75% of respondents also indicated that they “rarely (if ever)” perform lateral HSL. The panel was unanimous in noting that they “rarely (if ever)” perform isolated lateral HSL. Regarding which musculotendinous units to lengthen at the time of HSL, there was consensus regarding lengthening of the semitendinosus (ST), semimembranosus (SM), and gracilis, although specific lengthening techniques were not explored in detail.
Gait outcome measures deemed important following HSL, and for which consensus was reached, included decreased crouch, improved knee extension in stance, improved step length, and maintenance of pelvic tilt (i.e. no worsening of APT). Other important outcome measures included improved patient satisfaction (which reached consensus), along with general agreement regarding the absence of a knee flexion contracture and improvement in various clinical outcome measures, such as the Functional Mobility Scale, Functional Activity Questionnaire, Gross Motor Function Measure, Gait Outcomes Assessment List (GOAL®), Gait Variable Score, and Gait Profile Score.17–21
Hamstring transfer
HST surgery was a controversial subject for our panel, with only 50% of the panel (8/16) performing this surgery. There was no consensus about whether there are specific indications for HST surgery. For those who perform HST surgery, six statements were presented and there was general agreement for four, consensus for one, and consensus against the other one (Table 1). In general, it was felt that this is an option for children with increased APT for whom an HSL was felt to be needed.
Statements regarding hamstring transfer surgery.
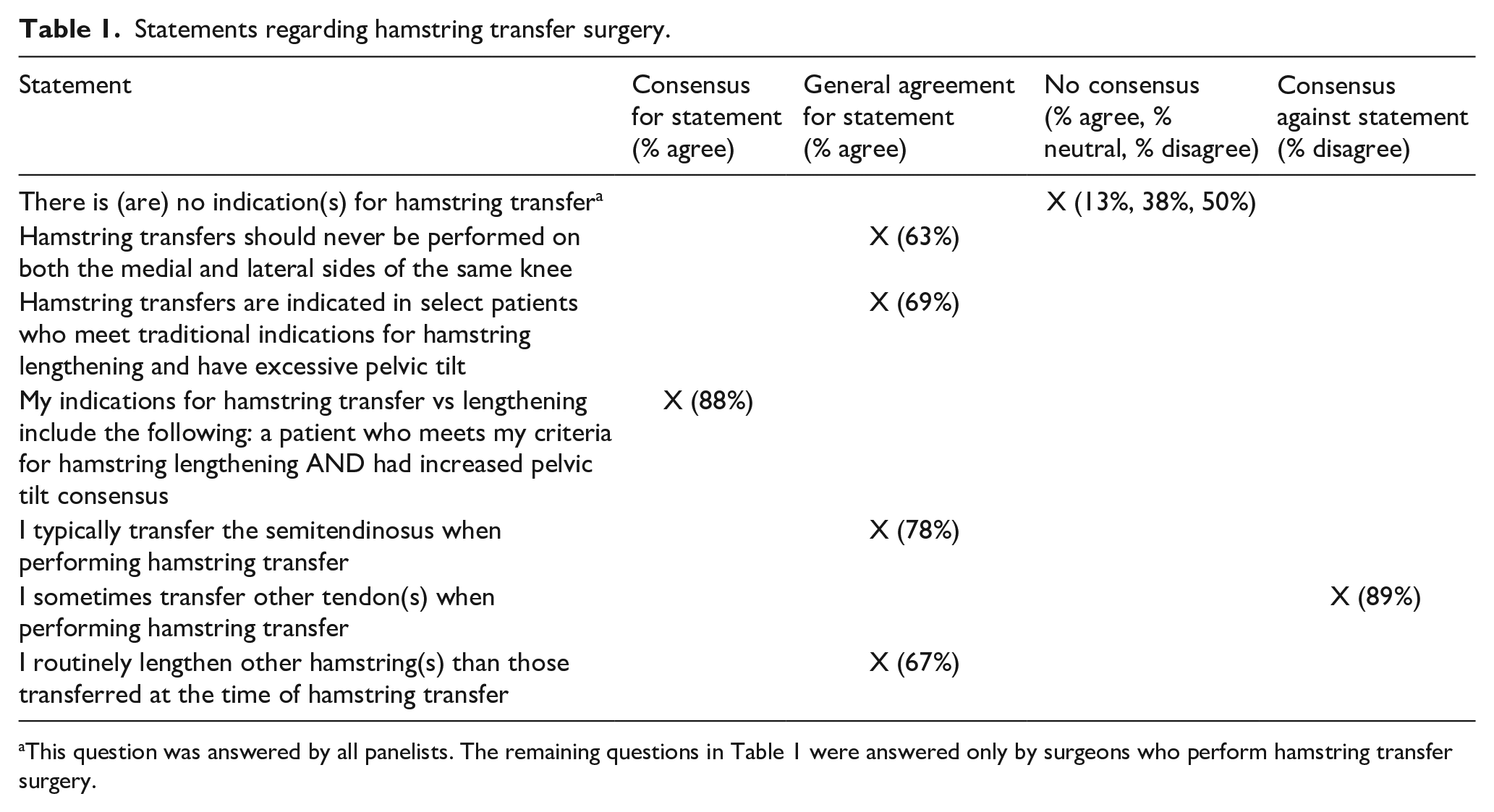
This question was answered by all panelists. The remaining questions in Table 1 were answered only by surgeons who perform hamstring transfer surgery.
Discussion
Using an iterative process, this panel of pediatric orthopedic surgeons with expertise in both the care of children with CP and in the use of computerized gait analysis sought to elucidate areas of consensus and others for which consensus could not be reached.13,14 The panel chose to use the Delphi method, a well-described process for developing consensus. An expert Delphi method aims to provide guidelines on issues that may be controversial because of insufficient evidence. The results of such a process can help synthesize both published and unpublished data and help the reader make decisions about their patients. The areas of disagreement not only provide useful information for practicing orthopedic surgeons, but can also allow the field to identify and focus on the questions and controversies that remain to be addressed through better-quality prospective cohort studies and clinical trials while also seeking to corroborate (or refute) the areas of consensus in these future studies.
The findings of the current study build on our previous publications11,12 and are meant to be integrated with our work regarding additional procedures about the knee in children with ambulatory CP. The panel reached consensus or general agreement for 84% of statements for hamstring surgery, which is higher than for other surgeries the experts previously evaluated.11,12 We feel this can help guide the practicing pediatric orthopedic surgeon in their approach to the care of children with CP and knee dysfunction. The panel noted the importance of optimal “dosing” of knee surgery to maximize patient outcomes. 12
The panel emphasized the importance of a thorough evaluation of the child and their gait in order to optimize treatment.1–5 Assessments typically include static physical examination, observational gait analysis, radiographs when indicated, and 3DGA when surgery is being anticipated.9,8 Static examination is comprehensive, typically including measures of range of motion, strength, spasticity, selective motor control throughout the lower extremities, rotational profile, and measures of foot alignment. Deficits of muscle strength and/or selective motor control are a warning that achieving improvements in gait and function may be more challenging for a specific patient. On some occasions, major deficits in these areas may contraindicate surgery or modify the surgical prescription. As with all procedures, consideration of hamstring surgery in children with CP requires a careful weighing of the risk to benefit ratio for a given child.
At baseline, children with CP are often weak 22 and have a poor strength to weight ratio. Surgical lengthening of a muscle tendon unit results in acute weakness which may persist.23,24 Previous authors have used botulinum toxin injections to weaken specific muscle groups before anticipated surgical lengthening of the muscle tendon unit to predict which patients would not benefit from surgery. 23 Other authors have reported the importance of appropriate post-operative rehabilitation to strengthen the muscles post-operatively.24,25 The panel recognizes the great importance of appropriate post-operative rehabilitation to maximize strength, recovery, and function following multilevel surgery. Regaining strength is crucial for optimal post-operative recovery and function. A well-planned and executed surgical intervention will not be successful without appropriate rehabilitation and strengthening after surgery.
When surgery is performed, the panel emphasized the importance of the single-event multilevel surgery (SEMLS) concept to optimize outcomes and to reduce the number of surgeries and episodes of rehabilitation to a minimum. HSL and HST are rarely performed as isolated procedures. Correction of all contractures and lever-arm deformities should be considered to optimize the improvement from HSL and HST at the knee.8–10 The knee must be assessed in the overall context of the child’s gait and function. The thorough assessment must include evaluation of the problems at all levels and in all planes. Previous authors have reported the high prevalence of knee problems in children with CP, including the fact that crouch gait has been reported in over half of all children presenting to a computerized gait laboratory. 6 For the purposes of this article, the panel focused on HSL and HST surgery, and bony surgery at the knee will be considered in another study.
Hamstring lengthening
For children with excessive knee flexion in stance phase, a long-standing approach has been to perform distal HSL. Although knee extension is typically improved in children following HSL surgery, the results are variable. This is not surprising, given that flexed knee gait is typically multifactorial with contributions from weakness (at the level of the hip, knee, and/or ankle), hamstring spasticity or dystonia, impaired selective motor control, and lever-arm deformities, leading to deficient plantar flexion–knee extension coupling.1–6 It is imperative that the orthopedic surgeon assess all of these potential contributors to flexed knee gait, and not simply assume that the hamstrings are the culprit.
This group reported on indications for HSL previously, 11 but due to the importance and prevalence of this type of surgery, the panel felt it important to delve more deeply into this area, further elucidating indications and contraindications for, and technical aspects of, HSL. Some of the areas addressed more deeply included the outcomes of repeat HSL surgery, the role and indications for HSL using hamstring modeling, and which specific hamstrings should be lengthened. The panel reached consensus that popliteal angle >60° may be an indication for HSL but did not reach consensus for popliteal angle either >40° or >50°. The specific choice of wording that popliteal angles of certain degrees may be an indication for surgery was purposeful so that there would not be any confusion that such a static measurement would be a definite indication for surgery. Clearly, such a static measurement is only one consideration when contemplating hamstring surgery in children with CP, and there are many other factors—many of which are dynamic gait parameters—deemed more important by many panel members. As emphasized by the panel, kinematic data at other levels, not just at the knee, are critical components of surgical decision-making in these children, as are dynamic hamstring length and velocity, based on hamstring modeling data and discussed further below. Discussion among panel members indicated that a child with an elevated popliteal angle measurement with long hamstring length would not be deemed a good candidate for HSL surgery. For patients in whom hamstring modeling data are not available, pelvic tilt is often a proxy for hamstring length, as those with APT typically have long hamstrings and those with PPT often have short hamstrings.
The panel reached consensus that PPT is a strong indication for HSL because hamstring modeling confirms that in the majority of patients with PPT the hamstrings are short in swing phase. APT is a relative contraindication for HSL, especially for combined medial and lateral HSL. Concerns raised by the panel about HSL in a child with APT were that APT may be an indication that the hamstrings are not short and also that APT would likely be further exacerbated following HSL in the face of significant pre-operative APT.
Modeling of hamstring length and hamstring velocity is used in order to help avoid lengthening hamstrings which are not short, despite kinematic evidence of crouch gait.15,16,26 The majority of the panel (69%) use hamstring modeling in their decision-making process. The panel views hamstring length in terminal swing and HSL velocity in swing phase as most important for surgical decision-making. There was consensus that short hamstrings in terminal swing are an indication for HSL and general agreement that decreased hamstring velocity in swing phase may be an indication (Figure 1(a) and (b)). Only 50% of the panel agreed that hamstrings must meet both of these two criteria to indicate HSL surgery.
Since there are many ways that HSL surgery can be performed, the panel assessed technical considerations for HSL. The panel clearly differentiated between medial and lateral HSL, noting that lateral HSL should rarely be undertaken, particularly for children functioning at GMFCS I–II and with primary HSL surgery.
For primary HSL, the panel reached consensus that it “routinely” lengthens the ST and “often” lengthens the SM and “often” lengthens the gracilis. For the ST, if the lengthening is done concomitantly with distal rectus femoris transfer or HST surgery, the ST is tenotomized (and the muscle belly may be sutured to the SM) prior to completion of the HST or distal rectus femoris transfer. If neither of the transfers is being performed, various panel members use the following three techniques for ST lengthening: (1) fractional lengthening via intramuscular tenotomy, (2) tenotomy distal to the musculotendinous junction, and (3) z-lengthening. For SM and gracilis lengthenings, fractional lengthenings are indicated, typically via aponeurotic lengthening of the SM at one of more levels and intramuscular fractional lengthening of the gracilis.
Lateral HSL is essentially never done in ambulatory children with CP by panel members. A fractional lengthening (such as via aponeurotic lengthening of the biceps femoris) may be considered in children functioning at GMFCS level III with short hamstrings and PPT in the absence of significant knee flexion contracture.
Panel members brought up the importance of avoiding excessive stretch on the peroneal nerve intraoperatively, noting that aggressively stretching to minimize the popliteal angle increases the risk of post-operative neuropraxia. Neuropraxia may result in dysesthesias and/or motor deficits and can significantly hinder surgical recovery and outcomes.
Problems reported in the literature after HSL include incomplete correction, recurrent crouch, over-correction and recurvatum, increased APT, and less favorable results following revision or repeat HSL.27–31 Excessive APT has long been identified as a potential problem following HSL,27,30,31 with recent authors indicating that APT seems to be an issue in children functioning at GMFCS level III, but not in those functioning at GMFCS levels I–II 31 and appears to be a greater risk following medial and lateral HSL, 27 after revision HSL, 28 and possibly in females. 32 Genu recurvatum may be more common with combined medial and lateral HSL, but can occur after isolated medial lengthening 33 and may be related to plantar flexion–knee extension coupling, due to either residual calf tightness or spasticity. The panel did not specifically address the controversial topic of open versus percutaneous methods for HSL, although previous studies have shown comparable results using these different approaches.34,35
The treatment of recurrent crouch following HSL surgery can be very difficult. This expert panel discussed repeat HSL surgery and concluded that repeat HSL is associated with smaller improvements in gait parameters at the knee and results in more unwanted effects, such as increased APT. Such conclusions are supported by previously published literature.28,29 Many panel members noted that repeat HSL (following previous HSL) often is not helpful, thus leading to the increased use of other soft tissue and bony procedures more recently, including anterior distal femoral hemiepiphysiodesis, distal femoral extension osteotomy, patella tendon shortening or advancement, or a combination thereof, for those with recurrent crouch. Alternatives to repeat HSL include guided growth in the skeletally immature patient, distal femoral extension osteotomy (DFEO) with patellar tendon shortening or advancement, and combinations of these procedures. These will be discussed in future reports by this panel.
Hamstring transfer
HST to the femoral condyles was described by Eggers in 1952 as a method to enhance both hip and knee extension in children with CP. 36 As initially described by Eggers, this surgery (which typically also included release of the patellar retinacula) included transfer of SM, ST, gracilis and biceps femoris to the femoral condyles. With long-term follow-up at the same institution, there were several significant complications of this procedure, including severe recurvatum, weak knee flexor power, exacerbation of lumbar lordosis, and “loss of trunk control.” 37 Others also recognized the value of HST in patients with CP and flexed knees, but switched to transferring some, but not all, hamstrings in order to avoid recurvatum and knee flexor weakness,37–40 and later to correct internal rotation and crouch.41,42
HST seemed to fall out of favor after these early reports, prior to the widespread use of computerized gait analysis. More recently, however, there has been an increase in articles related to HST surgery.43–51 From a theoretical basis, transfer of ST to the adductor tubercle may have the following advantages over HSL. It converts a two-joint muscle to a one-joint muscle, thereby simplifying its action.46,47 By removing ST from acting on the tibia, the knee flexion moment is permanently reduced and there should be a lower relapse rate from recurrent contracture than from ST lengthening. By preserving the proximal moment generation, pelvic stability should be maintained, hip extensor power might be maintained, and hip extension might be increased.46,47 Of the nine more recent studies in the literature reporting the outcomes of ST transfer, five studies compared HSL and HST and four reported HST only.45–51 However, the studies were heterogeneous in terms of inclusion criteria, including GMFCS levels, as well as concomitant transfers and inclusion/exclusion of lateral HSL. The results were mixed, and some longitudinal studies from the same institution demonstrated that early differences between the HST and HSL groups dissipated over time. 45
Of the 16 panelists, only 50% reported performing HST surgery. The surgeons who do not perform HST note the inconsistent results in the literature and the questionable need for this surgery. The panelists who perform HST reached consensus that HST is indicated in a patient who meets criteria for HSL and also has increased APT. One also noted that if hamstrings are normal or long on muscle length charts, but the popliteal angle is markedly reduced and knee flexion is increased at initial contact, then isolated ST transfer may reduce the stiffness behind the knee on physical examination and on gait, without exacerbating APT. 46 Regarding the surgical technique, there was general agreement among those performing HST that the ST is the tendon which is transferred and consensus that other tendons are not transferred. There was also general agreement that the surgeons lengthen other hamstrings at the time of HST.
The panelists who perform HST cite the risk of increased APT after HSL as one of their reasons to consider HST. Increased APT leads to increased lumbar lordosis with an increased prevalence of low back pain, at long-term follow-up.46,47 Increased APT may also predispose to increased risk of recurrent knee flexion/recurrent hamstring contractures and recurrent crouch gait. Transfer of ST to the adductor tubercle is the most commonly reported HST in the literature although the gracilis is included by some.45–47,51 There are no contemporary reports of transfer of all three medial hamstrings because of the very poor outcomes from historical literature.36,37
The more recent interest in “conservative HST surgery” with transfer of only one hamstring, the ST, is driven by the effort to improve the magnitude and durability of improvements in knee extension and to minimize the effects of increased APT.45,46 The principal reason for choosing the ST for transfer is not its functional or morphological differences from the SM, but is simply pragmatism. The distal tendon of the ST is superficial, easier to isolate, and easier to transfer and attach the adductor magnus tendon than the SM. 47 None of the studies to date have commented in detail on the appropriate tension for HST.45–47 This is an area with little information to guide surgical practice. Panel members who perform transfer of ST to the adductor tubercle note that the tension should be enough to result in a relatively straight line of pull between origin and new insertion, without obvious sagging from too little tension. 47 In younger children, there can be progressive tightening of the transfer with time and growth, and if severe, this could theoretically impede hip flexion in swing phase.45,46 The literature on hamstring architecture and function is developing rapidly and is not yet settled.52–54 We readily concede that neither the theoretical nor clinical basis for HST has a high level of evidence in the literature. Additional basic science studies including musculoskeletal modeling are required. More importantly, randomized trials to compare HST to HSL are required to improve the level of evidence.
Important take-home points from this panel of international experts regarding hamstring surgery in children with CP include the following:
It is imperative to look at both physical examination and gait findings when considering hamstring surgery.
Pelvic tilt during gait should be assessed pre-operatively, as the pelvis typically tilts more anteriorly following hamstring surgery, particularly HSL.
PPT is typically associated with short hamstrings, while APT is associated with hamstrings that are normal or long.
Lateral hamstrings should rarely, if ever, be lengthened in ambulatory children with CP.
Hamstring modeling data are very helpful for patient selection.
The results of repeat HSL are often poor, and repeat lengthening is rarely indicated in ambulatory children with CP.
Isolated hamstring surgery is typically indicated only if the knee flexion contracture is less than 10°. Other procedures are typically indicated for larger knee flexion contractures.
Do not aggressively check the popliteal angle following HSL in order to minimize the risk of post-operative peroneal neuropraxia.
Despite theoretical advantages of HST over HSL at both the hip and knee, the indications for HST remain controversial.
Conclusion
Crouch gait is extremely common in children with CP and is reported in over 50% of patients with CP presenting to a 3DGA laboratory. This panel of international experts with extensive experience in the treatment of children with CP and 3DGA has gone through an iterative process to provide useful information to help practicing pediatric orthopedic surgeons considering hamstring surgery for their patients. Looking to the future, higher level evidence would require prospective surgical trials to compare techniques such as open versus percutaneous HSL and HSL versus HST.
Footnotes
Author contributions
RMK: Conception and design, Analysis and interpretation of the data, Drafting of the article, Critical revision of the article for important intellectual content, Final approval of the article, Collection and assembly of data.
JM: Conception and design, Acquisition of the data, Analysis and interpretation of the data, Drafting of the article, Critical revision of the article for important intellectual content, Final approval of the article, Collection and assembly of data.
UN: Conception and design, Drafting of the article, Critical revision of the article for important intellectual content, Final approval of the article.
JR: Conception and design, Drafting of the article, Critical revision of the article for important intellectual content, Final approval of the article.
ER: Conception and design, Drafting of the article, Critical revision of the article for important intellectual content, Final approval of the article.
JS: Conception and design, Drafting of the article, Critical revision of the article for important intellectual content, Final approval of the article.
BJS: Conception and design, Drafting of the article, Critical revision of the article for important intellectual content, Final approval of the article.
MV: Conception and design, Acquisition of the data, Analysis and interpretation of the data, Drafting of the article, Critical revision of the article for important intellectual content, Final approval of the article, Collection and assembly of data, Statistical expertise, Administrative, Technical or logistical support.
MWS: Conception and design, Drafting of the article, Critical revision of the article for important intellectual content, Final approval of the article.
TT: Conception and design, Drafting of the article, Critical revision of the article for important intellectual content, Final approval of the article.
AVC: Conception and design, Drafting of the article, Critical revision of the article for important intellectual content, Final approval of the article.
KP: Conception and design, Drafting of the article, Critical revision of the article for important intellectual content, Final approval of the article.
HC: Conception and design, Drafting of the article, Critical revision of the article for important intellectual content, Final approval of the article.
JRD: Conception and design, Drafting of the article, Critical revision of the article for important intellectual content, Final approval of the article.
TD: Conception and design, Drafting of the article, Critical revision of the article for important intellectual content, Final approval of the article.
TFN: Conception and design, Drafting of the article, Critical revision of the article for important intellectual content, Final approval of the article.
KG: Conception and design, Drafting of the article, Critical revision of the article for important intellectual content, Final approval of the article.
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: RMK owns stock in Zimmer/Biomet, Medtronic, Pfizer, and Johnson and Johnson and is on the Editorial Board of the Journal of Pediatric Orthopaedics and his son works for Intrinsic Therapeutics, outside the scope of the submitted work. JM has received research support in royalties and as a consultant for Nuvasive. JR has received personal fees from OrthoPediatrics Corp., outside the scope of the submitted work. MWS is a member of the Editorial Board of the Journal of the Pediatric Orthopedic Society of North America and is a member of the National Advisory Board (NIH) on Medical Rehabilitation Research and the Eunice Kennedy Shriver National Institute of Child Health and Human Development (NICHD), all outside the scope of the submitted work. TD is Editor-In-Chief of the Gait & Posture Journal, Editorial Board member of Journal of Children’s Orthopaedics, and works as a consultant for Nuvasive. HC has received personal fees from OrthoPediatrics Corp. and Allergan Corp., outside the scope of the submitted work. JRD is a consultant and board member of OrthoPediatrics Corp., outside the scope of the submitted work. KG has received research support from NHMRC-CRE CP-Achieve and is on the Surgeon’s Advisory Board of OrthoPediatrics Corp, outside the scope of the submitted work. The other authors declare no conflict of interest.
Ethical approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards. This article does not contain any studies with animals performed by any of the authors.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed consent
All subjects were given informed consent and agreed to participate in the project.