
Abstract
Abstract
Purpose
Surgical procedures, such as medial hamstring lengthening (MHL) and femoral derotational osteotomy (FDO), can improve the gait of children with cerebral palsy (CP); however, substantial variation exists in the factors that influence the decision to perform surgery. The purpose of this study was to use expert surgeon opinion through a Delphi technique to establish consensus for indications in ambulatory children with CP.
Methods
A 15-member panel, all established experts with at least nine years’ experience in the surgical management of children with CP, was created (mean of 20.81 years’ experience). All panel members also had expertise of the use of movement analysis for the assessment of gait disorders in children with CP. The group initially focused on two of the most commonly performed procedures, MHL and FDO, in an attempt to gain consensus (> 80%). This was obtained through a standardized, iterative Delphi process.
Results
For MHL, a total of 59 questions were surveyed: 41 indication questions and 18 outcome questions, for which there was consensus on ten indication questions and seven outcomes. For FDO, a total of 55 questions were surveyed: 43 indication questions and 12 outcome questions, for which there was consensus on 29 indication questions and eight outcomes.
Conclusion
This study is the first to use an expert panel to identify best-practice indications for common surgical procedures of children with CP. The results from this study will allow for more informed evaluation of practice and form the basis for future improvement efforts to standardize surgical recommendations internationally.
Level of Evidence
Level IV
Introduction
Cerebral palsy (CP) is the most common cause of physical disability in children 1 and improving the physical function of ambulatory children with CP positively impacts both their quality of life and that of their caregivers.2,3 Surgical procedures, such as medial hamstring lengthening (MHL) and femoral derotational osteotomy (FDO), can improve the gait and physical functioning of children with CP;4,5 however, substantial variation exists in the clinical and patient-level factors that influence the decision to perform surgery.6,7 This variation likely leads to both under- and overuse of these procedures in this population, who are already at higher risk of surgical complications than the general population. More traditional research approaches to the study of clinical decision making, such as case control studies and randomized controlled studies, have been performed but are limited due to the clinical heterogeneity of the patient population, the large menu of 30 to 40 commonly performed procedures and the variety of combinations of procedures and surgical techniques.
Consensus methodology, including indications for surgery and interpretation of gait analysis, has been successfully used to develop guidelines for the management of orthopaedic conditions.8,9 Our hypothesis is that it is feasible to use a combination of best available evidence and expert orthopaedic surgeon opinion through a Delphi technique to establish consensus for surgical indications for MHL and FDO in ambulatory children with CP. If successful, this process will serve as a model for developing indications for additional procedures and provide evidence for clinical equipoise for more traditional research techniques in specific areas with poor consensus.
Our methodology is broken down into four aims. First, convene an international group of experts with clinical experience in the treatment of children with CP and the use of 3D movement analysis. Second, create a defined list of commonly performed orthopaedic procedures from which to work to establish surgical indications. Third, establish and agree upon a construct for categorizing indications. Fourth, using the above structure, develop consensus around indications for MHL and FDO in ambulatory children with CP using the Delphi method.
Background and significance
CP is a heterogeneous group of motor disorders caused by nonprogressive injury to the brain during early development and is the most common cause of physical disability in children, with an estimated global prevalence of approximately 17 million people. 1 The symptoms of CP include abnormalities in muscle tone, strength and motor control, along with other secondary symptoms, that can affect physical function and the ability to ambulate.1,6 Improving the physical function of ambulatory children with CP can positively impact both their quality of life and that of their caregivers.2,3 A primary goal in the orthopaedic surgical treatment of ambulatory children with CP is improvement in gait, often accomplished with single-event multilevel surgery (SEMLS), where multiple procedures such as musculotendinous lengthening and corrective osteotomies, are included in one surgery.6,10,11
Although SEMLS avoids repeat episodes of anaesthesia, hospitalization and recovery, the combination of procedures makes evaluation of surgical indications and outcomes of specific procedures challenging. 11 A 2012 systematic review of SEMLS found a low level of evidence in support of SEMLS due to low quality of study design, short period of follow-up for outcome assessment and limited description of participants. 12 Given the variability in outcomes, along with the potential risks that accompany surgery in children with CP, it is critical to identify which patients should undergo SEMLS and the optimal indications for each specific procedure. Two common procedures often performed as part of SEMLS are MHL and FDO. MHL is often considered for children with flexed-knee gait, which can lead to joint pain, arthritis and progressive gait deterioration, 13 whereas FDO can be considered in patients with excessive femoral anteversion and increased internal hip rotation. 5 Currently, no standardized indications exist to assist orthopaedic surgeons in deciding which patients would be good candidates for specific procedures.14–17 As a result, surgeons use a combination of history, physical examination awake or while under anaesthesia, radiographic findings, 3D gait analyses and past experience; however, some evidence suggests that a more standardized approach may lead to improved outcomes.18,19
Consensus methodology has been successfully used to develop guidelines for the management of orthopaedic conditions, including indications for surgery and interpretation of gait analysis.8,9 This process can lead to the development of specific indications for MHL and FDO for ambulatory children with CP, which when applied consistently, will allow for improved assessment of long-term outcomes. The results from this study will allow for more informed evaluation of practice and form the basis for future improvement efforts to standardize surgical recommendations worldwide, and they can be easily extended to assess indications for other surgical procedures.
Materials and methods
This study used established consensus (Delphi) methodology to identify indications for MHL and FDO in ambulatory children with CP.
The Delphi methodology is a well-established method to develop appropriateness criteria.20–22 Institutional review board approval for the study and from each participating member was obtained. No participants dropped out from the study.
Expert panel formation
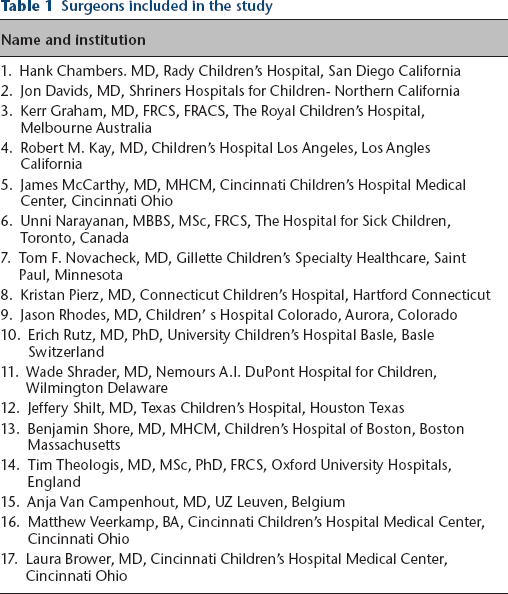
We formed a 15-member panel; all are established experts in the surgical management of children with CP (Table 1). Members were chosen from experts around the world. All experts were trained orthopaedic surgeons with at least nine years of focused clinical expertise in the orthopaedic surgical care of children with CP and access to and experience with a clinical movement analysis laboratory. On average, the experts had a mean of over 20 years of experience (mean 20.81 years, range 6 to 30) with the orthopaedic treatment of children with CP, for a combined total of over 300 years of experience. All panel members also had expertise with the use of movement analysis for the assessment of gait disorders in children with CP, on average 18.81 years (6 to 30).
Surgeons included in the study
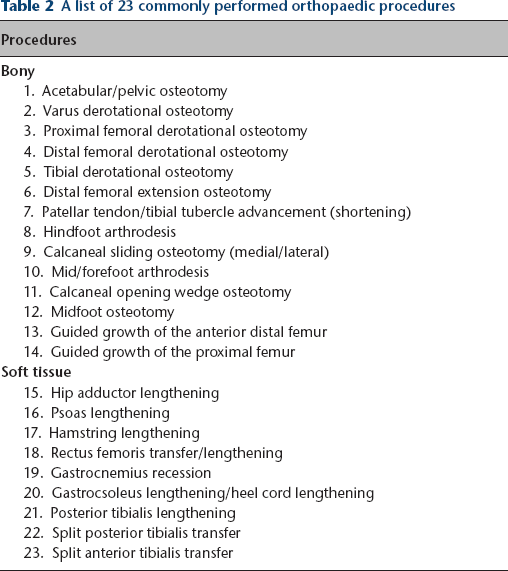
Our expert panel created a list of 23 commonly performed orthopaedic procedures (Table 2). From this list, we agreed to initially focus on two of the most commonly performed procedures, MHL and FDO as our initial attempt to gain consensus.
A list of 23 commonly performed orthopaedic procedures
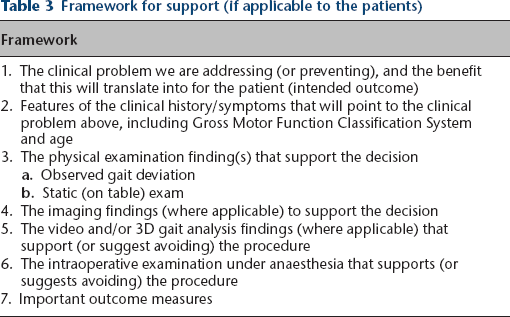
Our expert panel then created and agreed to a structured format for categorizing the indications as shown in Table 3. This format consisted of five categories including the clinical problem/history and symptoms, physical exam including observational gait analysis, imaging findings, 3D movement analysis data, intraoperative exam under anaesthesia and important outcome measures.23–25
Framework for support (if applicable to the patients)
Round 1: based on the literature review and submitted indications, we then used this structure to create open-ended questions regarding the surgical indications for MHL and FDO. These questions were then collated by category, and a well-structured questionnaire was created.
Round 2: an anonymous electronic survey was created in REDcap (Vanderbilt University, Nashville, Tennessee, USA)26,27 to formally rate the level of evidence supporting each indication using a Likert 5 level scale.21,22 This survey was sent to all experts in the group. Response options were strong indication, indicated, neutral, not indicated and strongly not indicated. Consensus for an indicated criterion was awarded when at least 80% of experts agreed to the top two Likert scales (strong indication or indication) or to a non-indicated procedure if at least 80% of experts agreed to the bottom two Likert scales (not indicated or strongly not indicated). Opportunity for comments was provided for all questions. General agreement was awarded for questions with at least 60% but less than 80% of experts agreeing to the top two Likert scales, or general disagreement for questions with at least 60% but less than 80% of experts agreeing to the bottom two Likert scales.
Round 3: from this survey, results were compiled. Those questions in which consensus was not achieved were evaluated, comments were collated, and (if needed) the question was clarified. This summary report was sent to all participants and responses to all non-consensus questions were re-submitted.
Two in-person meetings occurred in conjunction with international academic meetings, making the scheduling of an in-person meeting feasible, but still difficult given our international group of experts. During this process, panel members discussed ratings from round one, explored reasons for disagreement and modified indications.
Results
MHL
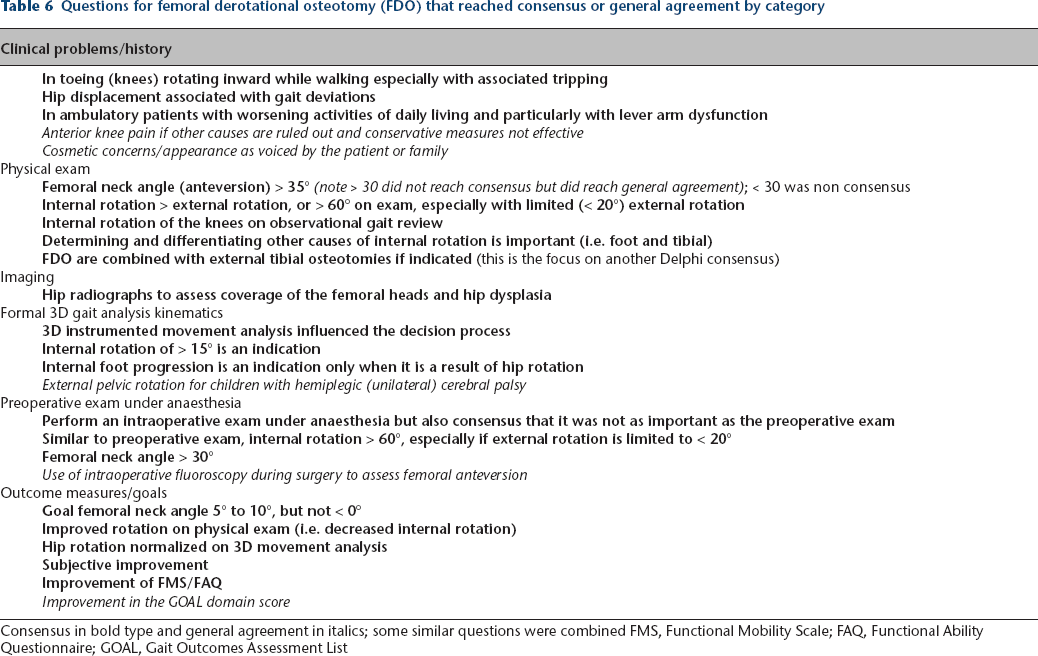
A total of 59 questions were surveyed: 41 indication questions and 18 outcome questions, for which there was consensus on ten indication questions, general agreement on eight more and consensus on seven outcome measures with general agreement on eight more. Consensus and general agreement by category are listed in Table 4. Questions for which there was consensus (bolded) and general agreement (italics) are listed in Table 5. 28
Consensus and general agreement by category for medial hamstring lengthening (MHL) and femoral derotational osteotomy (FDO)
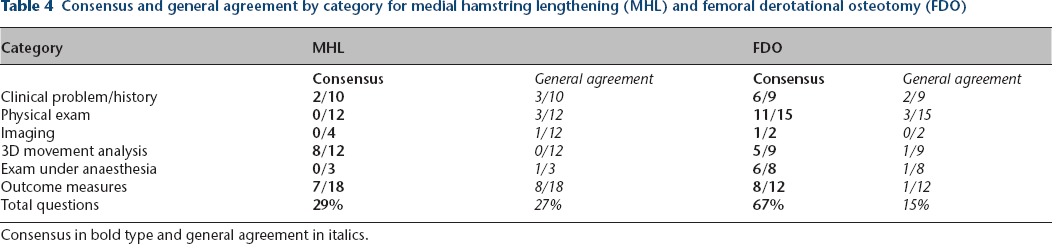
Consensus in bold type and general agreement in italics.
Questions for medial hamstring lengthening (MHL) that reached consensus or general agreement by category
Consensus in bold type and general agreement in italics; some similar questions were combined FMS, Functional Mobility Scale; FAQ, Functional Ability Questionnaire; GMFM, Gross Motor Function Measure; GOAL, Gait Outcomes Assessment List; GVS, Gait Variable Score; GPS, Gait Profile Score
Commonalities from the expert panel can be elucidated for MHL. Most experts lean heavily on instrumented 3D movement analysis, with a total of eight of their ten consensus points falling into this category. Indications are focused on data that directly support a shortened hamstring during gait as determined by computer modelling techniques or evaluation of excessive knee flexion at initial contact or terminal swing (when the hip is also flexed) and decreased (from normal) pelvic tilt. MHL is uncommonly performed as an isolated procedure by this group of experts, and the trend appears to be that fewer MHL are being performed and for more specific indications. MHL, if performed inappropriately, could contribute to worsening anterior pelvic tilt. The experts use the physical exam as a supplement to the movement analysis data, and caution against performing an MHL if the fixed knee flexion contracture is greater than 10°. In such cases, it was recommended that the knee flexion contracture be addressed at the time of surgery or beforehand. They also caution against vigorous testing of the popliteal angle while the patient is under anaesthesia (even gently) or after the MHL is performed, as it could lead to a stretch injury to the sciatic nerve.
FDO
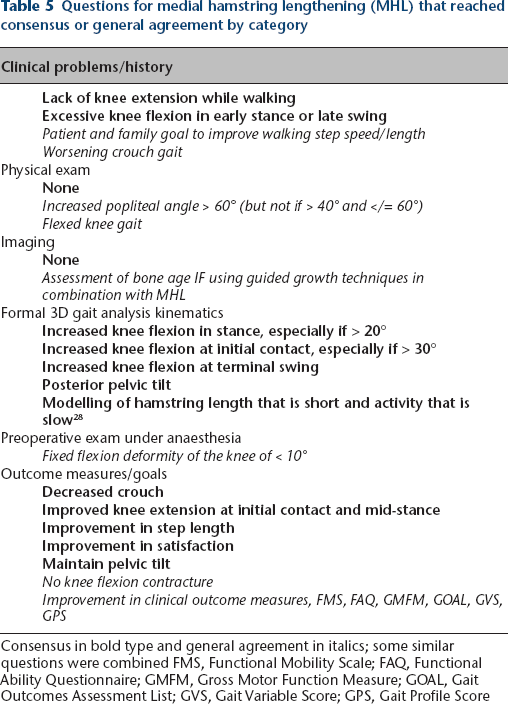
A total of 55 questions were surveyed: 43 indication questions and 12 outcome questions, for which there was consensus on 29 indication questions, general agreement on seven more and consensus on eight outcome measures with general agreement on one more. Consensus and general agreement by category are listed in Table 4. Questions for which there was consensus (bolded) and general agreement (italics) are listed in Table 6.
Questions for femoral derotational osteotomy (FDO) that reached consensus or general agreement by category
Consensus in bold type and general agreement in italics; some similar questions were combined FMS, Functional Mobility Scale; FAQ, Functional Ability Questionnaire; GOAL, Gait Outcomes Assessment List
Commonalities from the expert panel can be elucidated for FDO. In general, there was much greater consensus for this procedure (67%) than for MHL. Excessive internal rotation was felt to be an important contributor to gait deviations. Physical exam was important and consistent but problems with reliability were recognized. As with MHL, the decision for surgery must be taken in context with the entire patient assessment. Consensus for consideration of FDO was reliably reached when the internal rotation was greater than 15° on instrumented 3D movement analysis or a femoral neck angle (anteversion) of greater than 30° and internal rotation of greater than 60° degrees on physical examination, especially with limited external rotation. Although these measurements loosely correlate, the instrumented movement analysis consensus data were the strongest. Many experts commented on incorporating mild overcorrection (rotation), especially in younger patients.
A case example demonstrates physical exam and instrumented gait analysis results (Figs 1 and 2) as indications for MHL and FDO. Specifically, the movement analysis shows increased knee flexion at initial contact and at midstance as the consensus indication for bilateral MHL. Additionally, the physical exam and movement analysis show asymmetric femoral rotation (internal > external) as the consensus indication for FDO on the left, and knee flexion contractures (less than 10°) as the consensus indication for MHL.
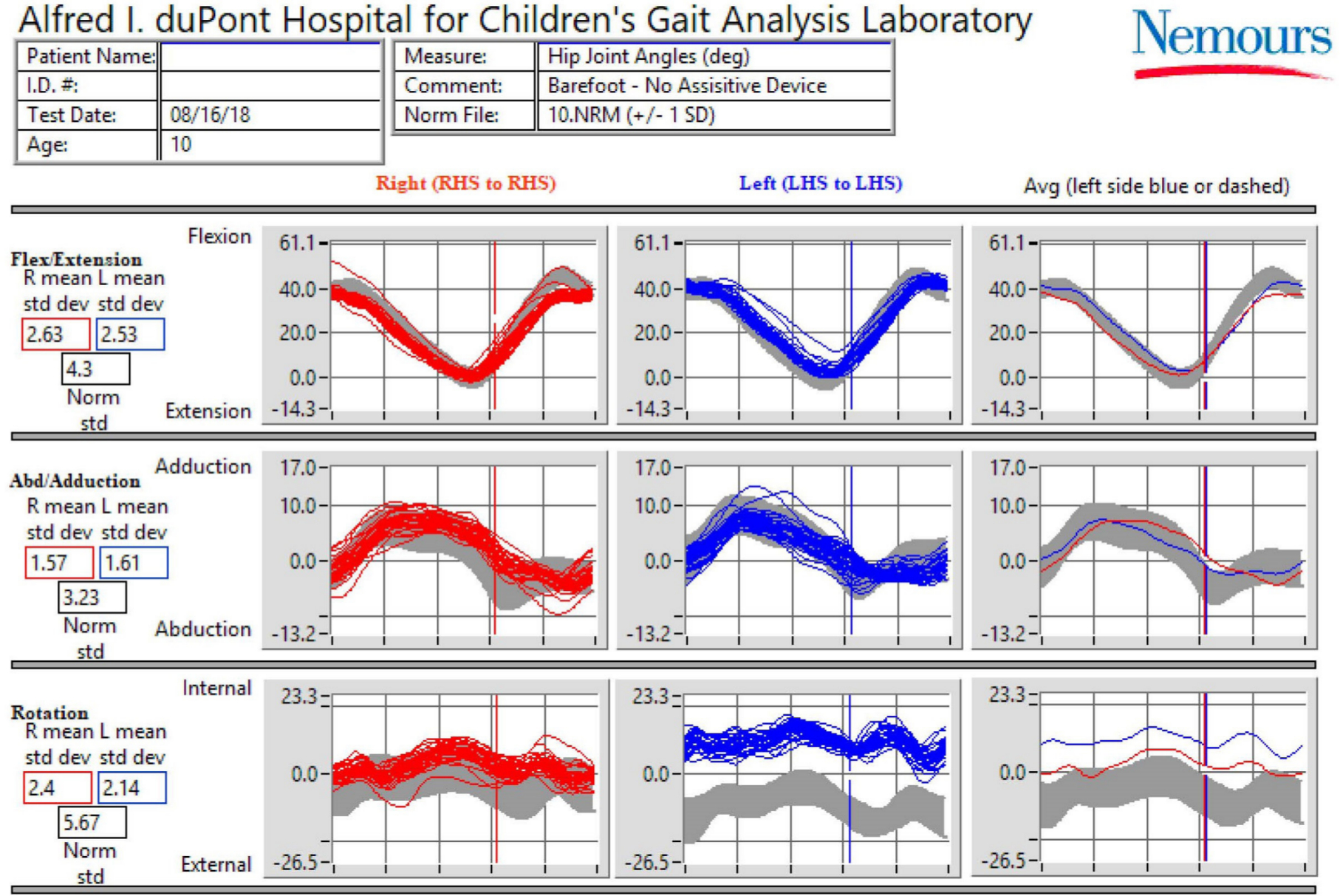
Hip kinematic data example of indications for femoral derotational osteotomy and medial hamstring lengthening L (HS, left heel strike; RHS, right heel strike).
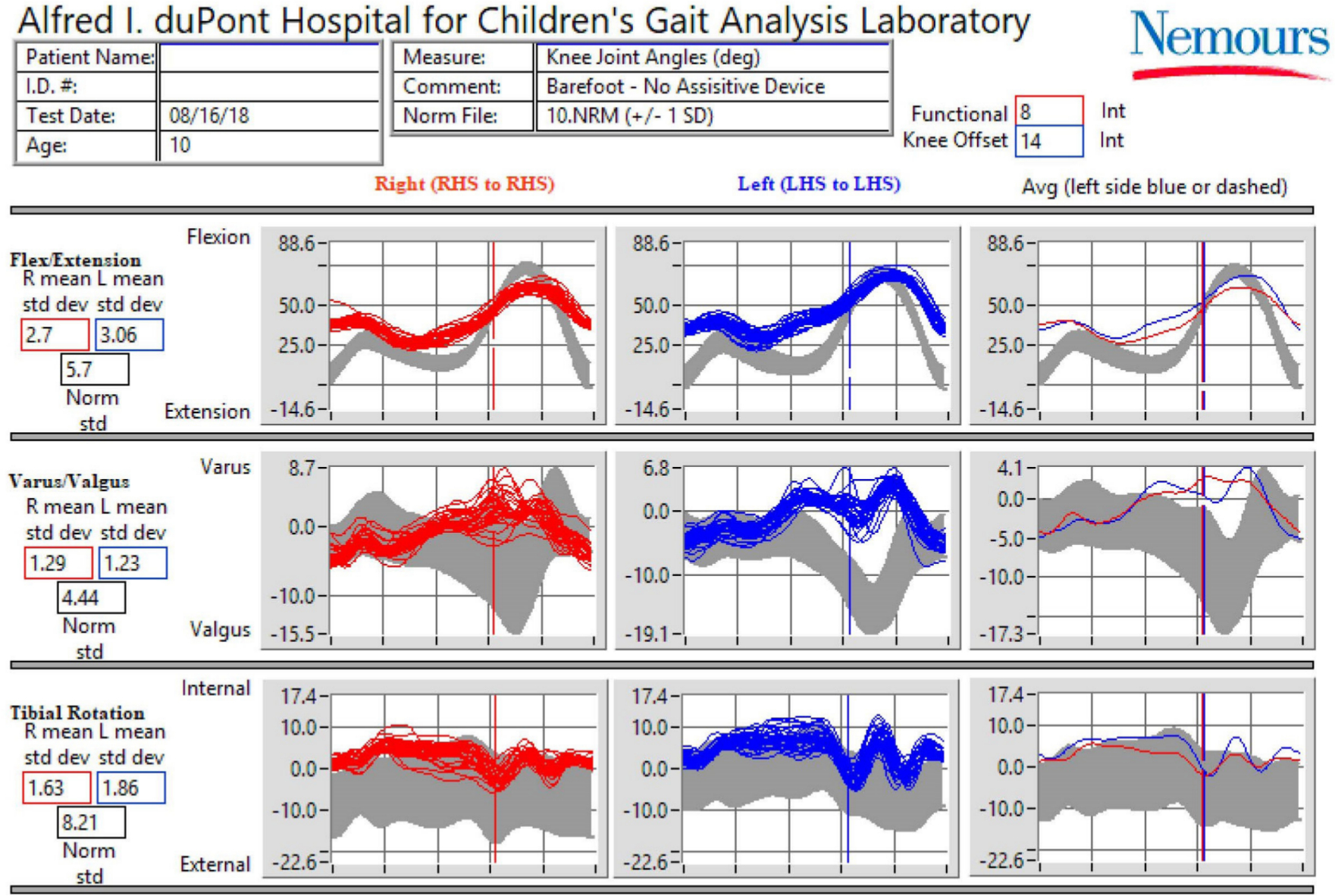
Knee kinematic data example of indications for femoral derotational osteotomy and medial hamstring lengthening (LHS, left heel strike; RHS, right heel strike).
Discussion
This study has multiple strengths. It is the first, to our knowledge, to use a panel of experts in the field of orthopaedic surgery in children with CP to combine best available evidence and expert opinion to identify best-practice indications MHL and FDO, common surgical procedures. The results from this study will allow for more informed evaluation of practice and form the basis for future improvement efforts to standardize surgical recommendations internationally, and are well set up for future multicentre evaluation and improvement studies through the relationships established via the consensus process.
This consensus is especially important for children with CP, who present with a very heterogeneous and often unique combination of biomechanical, neurological and social characteristics. In addition, the treatment options are numerous and often implemented in different combinations. This nearly infinite combination of procedures, in such a diverse group of patients, makes traditional comparison studies very difficult. Gaining consensus from an international group of experts with over 300 years of combined clinical experience can provide insights and help identify areas of consensus, and also bolster clinical equipoise in support of more traditional clinical research study designs.
Our experts lean heavily on the dynamically derived data from 3D instrumented movement analysis for both decision making and outcomes assessment. This certainly is partly due to having access to movement analysis and also a great deal of experience with the evaluation and interpretation of this assessment. Because these treatments are administered in an effort to improve dynamic function and because numerous decisions are made to perform (or importantly not to perform) a particular surgery, it seems the only way to know whether one is making the right decisions. Not everyone will have access to these types of data but as the technology evolves, this barrier will likely be lowered.
No procedure can have a list of surgical indications that can be applied without full assessment of the patient as a whole. These consensus points are only meant as a guide. The process, though, can be applied quickly and provide the foundation for further study. Future plans will be to use this modelled process for additional procedures in the care of the ambulatory patients with CP, including plantar flexor lengthening and tibial osteotomies, as examples.
In conclusion, this expert panel of paediatric orthopaedists with experience in CP and gait analysis were able to achieve consensus on the surgical indications for MHL and FDO in ambulatory children with CP. This project serves as a model for further surgical indication consensus projects in the area of CP, and will hopefully lead to additional research in improving quality and decreasing practice variability in the care of these children.
Footnotes
KG has received research support from NHMRC-CRE outside the scope of the submitted work and is on the Surgeon's Advisory Board of OrthoPediatrics Corp, all outside the submitted work.
HC has received personal fees from OrthoPediatrics Corp. and Allergan Corp., outside the scope of the submitted work.
JRD is a consultant and board member of OrthoPediatrics Corp., outside the submitted work.
RMK owns stock in Zimmer/Biomet, Medtronic and Johnson and Johnson. He is also on the Editorial Board of the Journal of Pediatric Orthopaedics and his son works for Intrinsic Therapeutics.
JR has received personal fees from OrthoPediatrics Corp., outside the scope of the submitted work.
All other authors declare no conflict of interest.
MWS: Conception and design, Drafting of the article, Critical revision of the article for important intellectual content, Final approval of the article, Obtaining of funding.
KG: Conception and design, Drafting of the article, Critical revision of the article for important intellectual content, Final approval of the article.
MV: Conception and design, Acquisition of the data, Analysis and interpretation of the data, Drafting of the article, Critical revision of the article for important intellectual content, Final approval of the article, Statistical expertise, Obtaining of funding, Administrative, technical or logistical support, Collection and assembly of data.
LB: Conception & design, Drafting of the article, Critical revision of the article for important intellectual content, Final approval of the article
HC: Conception and design, Drafting of the article, Critical revision of the article for important intellectual content, Final approval of the article.
JRD: Conception and design, Drafting of the article, Critical revision of the article for important intellectual content, Final approval of the article.
RMK: Conception and design, Drafting of the article, Critical revision of the article for important intellectual content, Final approval of the article.
UN: Conception and design, Drafting of the article, Critical revision of the article for important intellectual content, Final approval of the article.
TFN: Conception and design, Drafting of the article, Critical revision of the article for important intellectual content, Final approval of the article.
KP: Conception and design, Drafting of the article, Critical revision of the article for important intellectual content, Final approval of the article.
JR: Conception and design, Drafting of the article, Critical revision of the article for important intellectual content, Final approval of the article.
ER: Conception and design, Drafting of the article, Critical revision of the article for important intellectual content, Final approval of the article.
JS: Conception and design, Drafting of the article, Critical revision of the article for important intellectual content, Final approval of the article.
BJS: Conception and design, Drafting of the article, Critical revision of the article for important intellectual content, Final approval of the article.
TT: Conception and design, Drafting of the article, Critical revision of the article for important intellectual content, Final approval of the article.
AVC: Conception and design, Drafting of the article, Critical revision of the article for important intellectual content, Final approval of the article.