
Abstract
With the ageing population all over the world, long-term care services, such as nursing care, are essential to provide care and treatments to elderly patients in the community. During the nursing care services, elderly patients who live in the nursing homes require to be treated and consulted in a number of healthcare organisations, for example hospitals, mental health centres and rehabilitation centres. Currently, the data management for the elderly is relatively centralised to establish their own electronic medical records and protected health information without decision support functionalities. The community and healthcare industry are eager to develop a safe and comprehensive system to provide adequate healthcare services and monitoring to the elderly. In this study, an internet of healthcare things (IoHT)-based care link system (IoHT-CLS) is proposed, which provides a structured framework on integrating IoHT and artificial intelligence (AI) to generate a one-stop solution for managing elderly’s healthcare facilities. The elderly can be effectively linked into the integrated IoHT system by using various sensing and data collection technologies. The collected data are further processed by means of the adaptive neuro-fuzzy inference system and case-based reasoning to provide the functionalities of risk management and customised elderly service programmes for the elderly care institutions. Consequently, this study contributes to the healthcare management through the enhancement of service quality in the community.
Introduction
In the nursing care industry, long-term care services are regarded as the crucial aspect in the social community to provide proper and timely care and treatments. In recent years, long-term care plan (LTCP) is established to structure the services and target patients in the community network. 1,2 LTCP 2.0 was formulated in 2017 to enhance front-end preventive care and back-end communications for supporting the multi-target healthcare and hospice services. In LTCP 2.0, a three-tier ABC community model is suggested, in which a cluster-tree structure is used to manage integrated community service centre, multiple service centre and long-term care station. Under the cluster-tree structure of the LTCP 2.0, the patients’ data and healthcare service are not fully integrated as a whole. Although the cluster-tree structure in healthcare management provides an efficient data management mechanism, the needs for the decision support in healthcare services, including the risk management and elderly care service customisation, cannot be addressed. This situation resulted in a gap to further improve the service quality in the healthcare industry for the elderly. Meanwhile, without the reliable data management and data transparency, the healthcare data analytics to customise care services have been under-researched. Long-term care service providers are keen on evaluating the risk of non-medical incidents, while the fall prevention to elderly patients is regarded as the most critical measure to eliminate tens of thousands of unintentional deaths globally. 3 Emerging studies have attempted to establish an effective fall prevention and detection mechanism by means of internet of healthcare things (IoHT) technologies and algorithms to accurately predict the fall occurrence. The living quality of the elderly in nursing homes must be improved. However, with effective data acquisition in the healthcare facilities, the data to be processed for the fall prevention can be limited, which may have a negative effect on the evaluation of the fall prevention in real-life situations.
To address the above-mentioned challenges in the current nursing care industry, an IoHT-care link system is proposed in this study, which comprise IoHT and artificial intelligence (AI) as a whole. The deployment of IoHT creates a platform for effective data transmission and exchange for the stakeholders in the elderly care services, such as the elderly, nurses and doctors. After the service-oriented architecture of the IoHT is built, a fall prediction mechanism is formulated by modifying an adaptive neuro-fuzzy inference system (ANFIS) based on the behaviour and characteristics of the elderly in the nursing care industry. Consequently, the pro-active strategy related to elderly care service programmes can be made to the elderly management inside the facilities by means of case-based reasoning (CBR). The contribution of this study is to integrate the IoHT and AI as a whole to enhance the data acquisition and analytics in the elder care industry, while the advantages from the proposed system facilitates the better management of the healthcare facilities. A backbone of building an integrated healthcare solution is built in this study, which can be further extended to a number of decision support functionalities in the elderly care industry.
This paper is organised as follows. The first section is the introduction. The second section provides the review of the related work and literature in the aspects of healthcare management, IoHT and AI techniques. The third section presents the modular framework of IoHT-CLS. The fourth section illustrates a case study in implementing the proposed framework. The fifth section shows the results and discussion related to performance and comparison of the proposed framework. Finally, the sixth section presents the study conclusions.
Literature review
Overview of the elderly care services
Among numerous social phenomena, ageing population is regarded as the most critical one that draws significant attention from the community and government. According to the estimated figures from United Nations Department of Economic and Social Affairs, 4 the increment of the number of the elder aged 60 years old or above will reach 22% in 2050 compared with the current figures with more than two billion elderly people in the world. Providing the best living quality and assistance to the elderly is necessary in the coming future; the government and international organisations are responsible for establishing various healthcare strategies and measures for driving the increased longevity and low fertility in the community. 5 However, such a phenomenon leads to social and economic impacts to the community and economies worldwide. Given that the demand of healthcare services has been rapidly increased recently, the pressure in the healthcare systems and workload on the healthcare-related personnel are hugely increased. At present, the healthcare services to the elderly are divided into two dimensions: (i) short-term healthcare services and (ii) long-term healthcare services.
With regard to the short-term healthcare services, hospitalisation is deemed to be the representative one to provide professional treatment and operations, for example diseases diagnosis, acute care surgery and emergency care, to the public. Apart from care services, hospitals originally play an important role in supporting long-term care service providers for outreaching the residential and home care services in the community. 6 Based on the report from Census and Statistics Department in 2017, the hospitalisation rate for people aged 65 year old or above in Hong Kong is substantially increasing due to the growing demands for short-term and long-term healthcare services driven by the ageing population. In managing such a large group of the elderly in the community, the healthcare resources, including equipment, facilities and professional staff, to support the long-term healthcare needs are relatively insufficient, resulting in long waiting time for investigations and treatments and poor service satisfaction. 7,8 To relieve the pressure and financial burdens on the hospitals, governments in different countries, such as Taiwan, China and US, have established various initiatives for LTCP to effectively promote a holistic healthcare services in the community, 2,9 This initiative aims to provide a one-stop healthcare services for the elderly, from preventative care to community-based healthcare support, and finally to hospice care.
In the long-term care services, home care and residential care are regarded as two primary focus in the healthcare industry. Home care includes an extensive range of healthcare services, covering personal care, supportive care, technical nursing care and domestic aid, at the elderly’s homes. 10 Caregivers are also equipped with a wide range of professional healthcare skills, for example home health aides, physical training and mental support. Although home care services can be customised and effective to the elderly, the complexity of providing such services is relatively high, such as workforce scheduling and adequacy of the care skills. 11 In view of having various health problems for the elderly, one caregiver assigned to serve a single elderly may not be sufficient; consequently, the elderly who needs ‘many-on-one’ care services cannot be catered. Therefore, residential care services have been promoted as another long-term care services for providing ‘many-on-many’ care services for the elderly in centralised facilities. Among numerous residential care services, nursing homes are the major long-term healthcare service providers in the community, which provide a wide range of medical and nursing care, personal care and social support to the elderly. 12 In United States, a quarter of the elderly are currently living in nursing homes, and the demand for the residential care services is expected increase in near the future. Overall, with the increasing awareness for living quality and health conditions, particularly under the current outbreak of epidemic situations all over the world, the growing demand on effectively managing healthcare services to the elderly leads to active investigations for the enhancement of their health and safety.
Internet of things (IoT) and AI
IoT is regarded as an active research area to establish the digital linkage between physical objects and virtual world. Generally, IoT is defined as an interconnection of objects (i.e. things) in the physical world assimilating and sharing data with other objects and systems over the Internet. 13 Given that IoT is referred to a general use of smart devices, software and systems in industrial scenarios, several subdomains of IoT have been developed to cater various industrial needs and requirements. In the healthcare industry, internet of medical things (IoMT) and IoHT are two emerging paradigms to collect medical and healthcare data through IoT devices, respectively. Compared with IoMT, IoHT is an amalgamation of healthcare systems, medical devices and other healthcare-related objects to achieve healthcare information systems via networking technologies. 14 To effectively interconnect the elderly in the community, IoHT is deemed to be more suitable to be adopted in monitoring and measuring the health conditions and needs from the elderly through different advanced technologies, such as sensing devices and wearables. 13,15 The presence of IoHT re-defines the position of IoT in the e-healthcare systems for connecting physical healthcare services and the elderly into the digital world. Meanwhile, the health-related data acquisition, such as blood pressure, weight and blood oxygen saturation, can be facilitated. The deployment of IoHT can be standardised under a network architecture with considering the perception, mist, fog, cloud and application layers based on the system requirements. With the secure and reliable data collection, various applications to support the decision-making process in the healthcare industry can be established, wherein emerging technologies and techniques can be integrated as a whole, for example, AI. The appropriate data analytics for the system users can also be effectively formulated to embed the intelligence in the traditional operations. 16 Some recent studies show that the use of AI can further strengthen the service quality and clinical decision support. 17,18 Meanwhile, the AI methodologies can be integrated as a whole to strengthen the decision support functionalities in real-life situations, such as CBR and ANFIS. CBR was developed as a backbone in the application system for solving new problems through referring to the previous cases stored in the case library, while its mechanism is built by 4Rs, which stands for retrieval, reuse, revision and retention. 19 Furthermore, the CBR is capable of integrating with other existing AI methodologies to create a synergy for various application domains. The ANFIS was designed for facilitating predictive analytics and machine learning through the integration of Sugeno-type fuzzy inference system and artificial neural network. 20,21 The network of the ANFIS can be trained adequate for formulating the corresponding decision support systems by using the historical datasets as the supervised learning approach. Consequently, the application of the ANFIS is potential to be further extending to the area of falling-down prediction in the elderly care management. 22
The results of the review of the above studies indicated that the existing healthcare systems are diversified, which cannot link together to provide better decision support and healthcare services to the elderly. With regard to long-term care services, the effective healthcare system is essential to provide better living quality and nursing care to the elderly. To connect every healthcare things, the IoHT is considered for collecting multidimensional data in the elderly care industry, while such data can be used to build a holistic system to enhance the healthcare management in the elderly care industry.
Design of an IoHT-based care link system
In this section, the IoHT-based care link system (IoHT-CLS) is designed through referring the system framework of IoHT, where the intelligent elderly service programme customisation is established. Inside the programme customisation, the falling-down prediction is constructed by using the ANFIS, while the customised care plans for the elderly are generated by means of the CBR. Figure 1 shows the system architecture of the IoHT-CLS with two major components, namely, (i) structured framework of deploying IoHT and (ii) intelligent elderly service programme customisation. Therefore, all the healthcare-related information of the elderly can be linked in a centralised manner to provide the customised and adequate elderly care services.
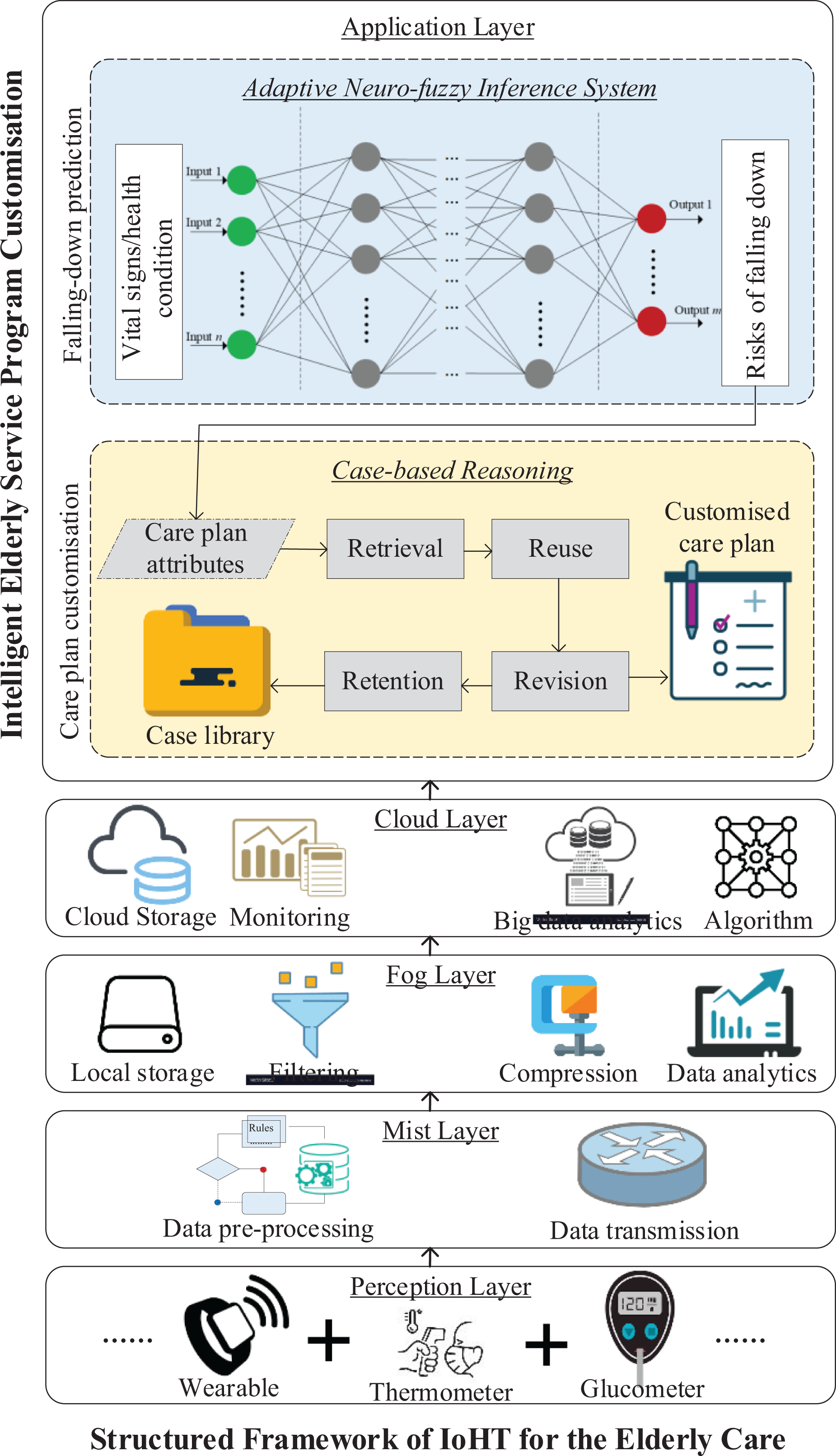
System architecture of the IoHT-CLS.
Structured framework of IoHT for the elderly care
On the basis of the work by Tang et al. 13 and Tsang et al., 23 a structured IoHT framework can be formulated in the context of elderly care with five essential layers, namely, (i) perception layer, (ii) mist layer, (iii) fog layer, (iv) cloud layer and (v) application layer. Under such a structured framework, a large number of IoT devices can be effectively managed, in which voluminous and heterogeneous data are securely and efficiently transmitted to a centralised cloud platform. Under the resource-efficient system environment, the applications on the prediction of falling-down rates and care plan customisation are established.
Layer 1: Perception layer
The perception layer is regarded as the first layer of the entire structured framework, which refers to the data acquisition from IoT devices, such as sensors and wearables, equipped with the elderly. In nursing homes, vital signs of the elderly are recorded at a regular basis, including heart rate, blood pressure, blood glucose, body temperature, oxygen saturation and respiration rate, depending on the elderly’s health situations. For instance, a wearable device (e.g. WearPai WP107) can be installed to measure the heart rate, blood pressure and blood oxygen; a thermometer (e.g. Nokia SCT01) can be used to evaluate the body temperature of the elderly in a wireless manner; a glucometer (e.g. iHealth BG5) can be applied to measure the level of blood glucose. In addition, the elderly can be effectively managed by using identification technologies, such as barcode, quick response (QR) code and radio frequency identification; therefore, all the collected health-related data can be associated with their own identities. Given that some of the above-mentioned devices can be working in a wireless mode, the internet connection of Wi-Fi should be fully deployed in the indoor environment to ensure the effective coverage and connectivity of the devices. Apart from the real-time health-related data for the elderly, this layer also covers nonreal-time data collection from various sources, such as electronic health records (eHRs), personal information and unstructured clinical notes. After the data collection is authorised, all the collected data can be managed in a centralised manner to further build data analytical models, while the data can be further transmitted into designated overlaying layer, namely, mist layer or fog layer, according to the data processing requirements.
Layer 2: Mist layer
The mist layer is introduced in the IoHT-based solution by using mist computing due to the needs of time-critical data processing. The extreme edge of a network is deployed by using microcontrollers in IoT devices for effectively transmitting the data to the fog computing. The data transmission process from the IoT devices to the local/cloud servers can be constructed using various wireless communication technologies, such as Wi-Fi, Bluetooth and Zigbee, with edge routers, for example smart phones and wireless router. Moreover, the rule-based data pre-processing is conducted for structuring the sensor data for further analytics and domain applications, resulting in an efficient data transmission in the aspects of computation resources, power consumption, communication bandwidth and so on.
Layer 3: Fog layer
After the collected data are polished in the mist layer, the data are then transmitted into the fog layer, in which the fog computing provides high responsiveness and minimal latency for managing the collected data. In comparison with the cloud computing, the fog computing is relatively close to the mist computing for supporting the functions of local data storage, data fusion, data compression and partial data analytics to reduce the load of the cloud-based solutions. Accordingly, the system performance, quality of service (QoS) and utilisation of backbone bandwidth can be improved. Instead of centralising all the collected data, the data in the fog layer are relatively decentralised in numerous local fog computing with different computing resources and application services. Filtering and basic data analytics can be established by embedding the fog computing in the proposed system to generate different types of reports for supporting daily operations and managerial evaluation of the elderly care facilities. In addition, the nodes in fog computing are constrained by its computational power and size limitations to proceed data generated at a high frequency, where the computational power in the fog layer is used to provide the functions of data processing and primitive analysis. 24 Subsequently, the fog layer is connected to the cloud layer to create the on-demand and cloud-based solution widely spread in the industry.
Layer 4: Cloud layer
In this layer, the deployment of the cloud computing is formulated to connect the perception, mist and fog layers to contribute the application layer. In the cloud computing, all healthcare data related to the elderly are aggregated in a centralised manner for long-term storage and big data processing. A number of application programming interfaces (APIs) and external services can also be linked into the cloud platforms, such as the eHR and e-prescription, with consolidation of all the real-time and nonreal-time data of the elderly. The elderly can be monitored in a holistic view, in which alert management, health monitoring and report generation can be made for enhancing the effectiveness and efficiency of the routine operations. In the cloud computing, different database structures, such as relational database and NoSQL, can be utilised, depending on the needs of the applications and system design. The data can be effectively queried and analysed in the application layer.
Layer 5: Application layer
After the IoT transmission, mist computing, fog computing and cloud computing are built, the application for the intelligent elderly service programme customisation can be established. Inside the application, the functions of fall-down prediction and care plan customisation are included as the primary research areas in the proposed system. In the proposed system, the user interfaces are provided to connect the stakeholders and end users in the elderly care industry. Moreover, this layer can control the access rights and privileges of users in the proposed system to retrieve the relevant resources from the cloud and fog computing to the stakeholders.
Intelligent elderly service programme customisation
Under the structured IoHT framework, two primary functions are formulated, namely, falling-down prediction and care plan customisation. These two functions are interconnected, while the likelihood and consequence of the elderly’s falling down are used as the attributes to formulate the customised care plan for the elderly.
Falling-down prediction by using ANFIS
This section presents an intelligent method for falling-down prediction of the elderly living in the nursing homes by using the ANFIS and the relationship between the elderly’s health data (e.g. vital sign) and risk of falling down (e.g. likelihood and severity). Specifically, the risk of falling down to specific elderly can be predicted according to their health conditions. Firstly, in the training phase, a well-defined dataset for the historical healthcare data in which the input and output attributes are defined in advance is collected. According to Rajagopalan et al., 25 the biological and demographic fall risk factors can be considered to build the fall prediction under the IoHT environment. The input attributes include: (i) age of the elderly Vage (in years), (ii) average heart rate Vahr (in beat per minute), (iii) average body temperature Vabt (in °C), (iv) average respiration rate Varr (in breath per minute) and (v) average systolic and diastolic blood pressure, Vasp and Vadp (in mmHg); the output attributes cover the following: (i) likelihood of falling down Lfd (in units) and (ii) severity of falling down Sfd (in units). The ANFIS can accurately and effectively perform input–output fitting through two phases, namely, model training and operation, through the replicated learning process.
The ANFIS integrates the method of ANN and fuzzy inference system to automatically generate the corresponding membership functions and fuzzy rules by using the training data set. With regard to the architecture of ANFIS, five structured layers exist, as shown in Figure 2. Layer 1 refers to the corresponding fuzzy class C(i, j) , called the linguistic label, of the input variable xi , where i ∈ [1, n] and j ∈ [1, m] denote the number of the input variables and fuzzy classes, respectively. Moreover, n is the maximum number of input variables, and m is the maximum number of fuzzy classes for the specific input variable. Subsequently, the membership function Mi of the input variable xi can be defined, as shown in equation (1). The value of the membership functions ranges between 0 and 1 with the specific membership shapes, such as bell-shape and Gaussian-shape.


Deployment of the ANFIS in the falling-down prediction.
In layer 2, the incoming signals from layer 1 are combined through multiplying the membership values to compute the firing strength of a rule wj , as shown in equation (2). Afterwards, the firing strength of a rule is then normalised by calculating the ratio between all the potential rules in layer 3, as shown in equation (3). Therefore, the output of this layer is called the normalised firing strength.


In layer 4, a square node is considered with the node function, as shown equation (4). The normalised firing strength is then multiplied with the output parameters of the ANFIS, where x0 is equal to 1. To compute the overall output of the ANFIS, the summation of all incoming signals from layer 4 is conducted, as shown in equation (5).


Given that the membership functions and fuzzy rules can be obtained in the ANFIS, the fuzzification process and knowledge repository management can be simplified. A real-time data set can be inputted with the Sugeno inference engine, while the demand of the new products can be estimated from the defuzzification process. The Sugeno inference engine is designed to handle either a constant value or linear equation in the consequence part. For example, the fuzzy if–then rules can be ‘If x1 is low and x2 is average, then y is c’, and ‘If x1 is low, and x2 is average, then f1 = r11x1 + r12x2 + r1 ’. Consequently, the NPDF can be achieved in a systematic manner by using the proposed approach.
Care plan customisation by using CBR
Given that ANFIS evaluates the risks of falling down for the elderly, the results can be further used to customise the care plan for the elderly living in the nursing homes. To achieve this goal, the CBR is adopted to obtain the solution from the historical cases in the case library with four major phases, namely, retrieval, reuse, revision and retention. Firstly, when the review of the care plan takes place, the retrieval of past relevant cases from the case library is conducted through the evaluation of a number of attributes, including but not limited to age, self-care ability, communication ability and mobility. The attributes defined in the case retrieval process are subject to the requirements and coverage of the nursing homes. Considering a number of attributes, the similarity (Si
) between the inputted and the historical cases can be evaluated for the comparison, as in equation (6), where

The past care plans may not be updated and adequate in the current situation because the health status of the elderly is deteriorated along the time of living in the nursing homes. Therefore, the revision of the re-used case should be made by the domain expert in the nursing homes, for example, professional caregivers and care plan manager. The care plan can be customised according to the needs and health situation of the elderly to maintain the quality of care and their living quality. After the care plan is successfully revised, the finalised care plan for the elderly is then stored in the case library for supporting the future case retrieval and analysis.
Case study
To verify the feasibility of the proposed system, a company located in Hong Kong is eager to develop the system in the healthcare industry and deploy it in various nursing homes to improve the quality of care for the elderly. The company aims to established a quality-driven and elderly-oriented healthcare solution in the community. In this section, the company background and implementation details of the IoHT-CLS are discussed.
Company background
In this case study, S.T. Limited (alias) is a leading technology company in Hong Kong founded in 2000, which is eager to design and develop smart systems in various industries, such as healthcare and hospitality management, by using state-of-the-art technologies, including IoT and AI. Recently, the case company conducted an in-depth investigation in the healthcare industry in Hong Kong and found that existing healthcare-related systems, for example eHR, PHI and other healthcare decision support systems, are separately operating. The information from physical patients cannot effectively be transmitted to the smart systems to provide adequate healthcare support, particularly in the elderly care industry. In the elderly care industry, home care (i.e. the elderly is living in their home, while healthcare services are provided at a regular basis at home by a dedicated team of caregivers) and residential care (i.e. the elderly is living in designated healthcare facilities, while they are closely monitored by caregivers to provide comprehensive treatments and assistance) are two major types of services. The needs for creating an integrated smart healthcare system in the elderly care industry are substantially huge as the long-term healthcare services in the community. After consulting a number of industrial partners in the elderly care industry, this study found that the falling-down may cause the serious and unpredictable damage to the elderly, while the care plans are not effectively customised according to their health deterioration and conditions. In view of the above-mentioned issues, a systematic approach to provide real-time healthcare decision support is needed to foster the next evolution of the long-term care industry. Moreover, the intelligent systems can be the foundation of the establishment of future LTCP in the community
Implementation of the IoHT-CLS in the nursing home environment
The implementation of the proposed system in the industry is required to verify the technological feasibility of the proposed IoHT-CLS. In this section, the implementation plan is formulated step by step, which provides a system guideline to facilitate the deployment of IoHT in the healthcare facilities. Trial runs of the proposed system are conducted to walk through the entire proposed mechanism from installation of IoT devices, falling down prediction, to care plan customisation. Figure 3 shows the implementation flow of the proposed IoHT-CLS for the healthcare facilities in the elderly care industry.

Implementation flow of the proposed IoHT-CLS.
Step 1: Deployment of IoT sensors for health monitoring
Firstly, the appropriate IoT sensors are selected for the data collection of the elderly and living environment, which may affect the quality of care (QoC) to the elderly. Table 1 summarises the typical types of sensing technologies to be considered in the elderly care industry. The selection decision of IoHT devices should be based on the criteria of suitability and cost-effectiveness for the entire IoT deployment in the nursing homes. The requirements of nursing homes and routine operations in the proposed system are investigated in advance to collect the health-related and elderly-related data. Although many smart devices for data collection are available in the market, the cost-effectiveness of using such devices should be considered to meet the nursing homes’ expectation on return on investment and level of technology adoption. The five aspects needing sensing technologies are organised as follows: (i) vital sign and metabolic parameters, (ii) environmental conditions, (iii) elderly identity, (iv) fall detection and (v) activity and behaviour. Based on the five defined aspects, the relevant data to be collected are outlined, which are under total health monitoring and inputs for the healthcare decision support systems. The potential devices and solutions are also included in Table 1. Accordingly, healthcare facilities can select the appropriate combination of equipment based on resources, such as capital investment and number of skilled employees, and coverage of services. Given that the IoT devices and solutions are built by different vendors, data pre-processing to load, transform and extract useful data is required. Meanwhile, the basic monitoring functions, including sending alerts and generating reports, can be completed at this stage. Afterwards, the pre-processed data can be consolidated in a single payload through connecting multiple service APIs for supporting data storage and future query in the cloud environment. Such data payloads are also tagged with elderly’s IDs to effectively construct the association with their medical records and care plans.
List of sensing areas for building IoHT.

Step 2: Formulation of wireless sensor network (WSN) in healthcare facilities
After the appropriate sensing devices and solutions are selected, the WSN for the elderly and living places can be established to achieve the total health monitoring in healthcare facilities (Figure 4). In the WSN, each system node contains the data of the elderly specified by the IoT sensors in the five aforementioned aspects, while the system nodes are interconnected together as a whole in the healthcare facilities. The collected data are then transmitted to the cloud platform via an edge router, which plays a role of moderator to provide transmission scheduling between fog computing and computing. To structure the data transmission, wireless communication technologies (e.g. Bluetooth and Wi-Fi) and IoT protocols (e.g. MQTT and CoAP) are widely used between system nodes and the edge router and between the edge router to the IoT development platform, respectively. This technology maintains acceptable QoS for the deployed IoT services and solutions. Subsequently, the collected data can be stored and analysed in the IoHT development platform to build the designed decision support functionalities, namely, falling-down prediction and care plan customisation.

Graphical illustration of the WSN for the IoHT-CLS.
Step 3: Establishment of IoT development environment
When the data are successfully structured and transmitted from the edge router, the IoT development environment should be built to store, manage and analyse the collected data to deploy the proposed applications. Recently, numerous IoT development platforms can be used to construct the IoHT solutions, such as IBM Cloud, Microsoft Azure and Particle. These platforms are user-friendly in customising the solutions and data management, while on-demand subscription services are provided. For instance, in the IBM Cloud, such an IoHT application can be built on its Internet of Things Platform in node.js environment. Cloudant is used as the NoSQL data storage. The applications can be designed and developed in the Node-Red environment to ensure that the collected data can be simply linked to the front-end and back-end systems. Accordingly, the customised user interfaces for this IoHT application can be established, and the corresponding decision support functionalities can be deployed inside the IBM Cloud.
Step 4: Development of healthcare decision support functionalities
Given the data collection and management of IoHT are achieved, the collected data can be further used to provide the functions of falling-down prediction and care plan customisation. To demonstrate the proposed methods, a set of training and testing data with the size of 50 are considered, and five sets of elderly data are simulated to show the feasibility of the proposed methods. To examine the feasibility of the proposed system, five elderly patients are invited from the case company to measure their risks of falls and identify the most relevant past case for care plan customisation.
In the falling-down prediction, the ANFIS is trained by 50 rows of historical data, where 35 of them are used as training data and the rest as validation data. Table 2 shows the selected settings used in formulating the ANFIS in terms of FIS structure, number of membership functions, type of membership functions and epoch number. Subsequently, two ANFIS engines can be trained to evaluate the values of likelihood and severity of falling down for specific elderly patients. In predicting the likelihood of falling down (scale from 1 to 10), the minimal training and validation errors are 0.5 × 10−5 and 4.01172, respectively, measured by the using root mean square error. In predicting the severity of falling down (scale from 1 to 10), the minimal training and validation errors are 0.4 × 10−5 and 4.44201, respectively.
Attributes of building ANFIS for falling-down prediction.

Consequently, two trained and validated ANFIS engines can be deployed for evaluating the index of falling down prediction. Figure 5 presents the graphical illustration of the prediction mechanism by means of ANFIS. The incoming datasets are inputted to the trained and validated ANFIS engines to evaluate the likelihood and severity of falling down. The index of falling down prediction Ifd is calculated by multiplying the likelihood and severity together. Table 3 shows datasets of five current elderly patients who live in the nursing home, in which the corresponding likelihood, severity and indexes are measured. The resultant index of falling down prediction is scaled from 1 to 100, which shows the gravity of falling down for specific elderly patients. When the index value is high, the risk of falling down is correspondingly high in terms of likelihood and severity. Therefore, elderly patients with high index values needs extra attention on daily care and activities, and their care plans should be revised to maintain a high QoC when living in the nursing home in future.

Mechanism of using ANFIS to predict falling down for the elderly.
Results of measuring the index of falling down prediction for five elderly patients.

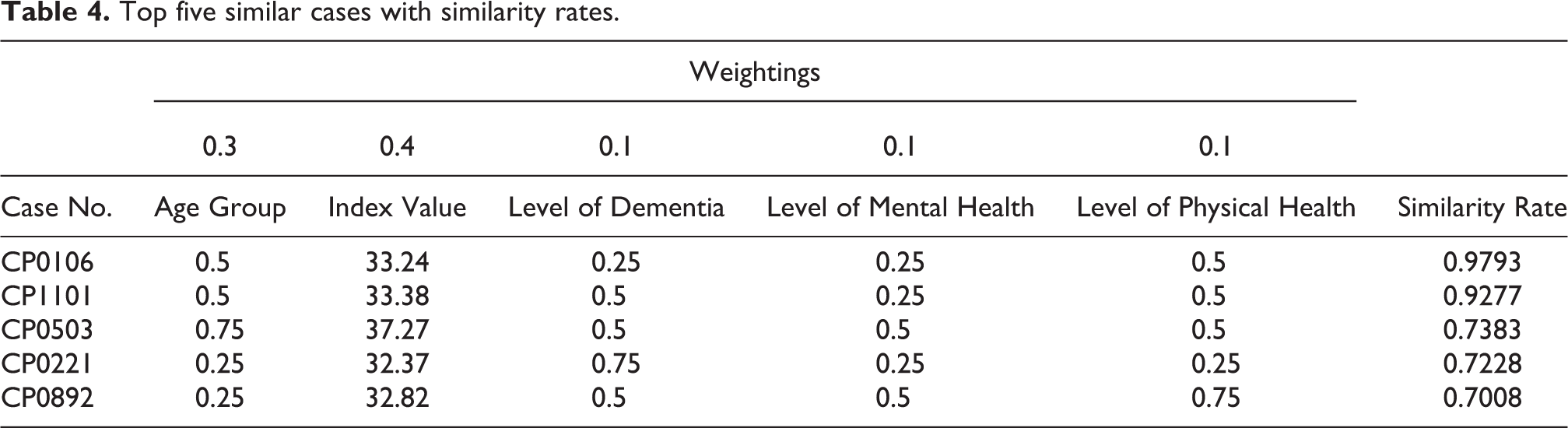
In the care plan customisation, the CBR mechanism is adopted to modify the existing care plans based on previous cases through executing retrieval, reuse, revision and retention (Figure 6). The attributes of index value, age group, level of dementia, level of mental health and level of physical health are considered to retrieve the past cases from the case library. To demonstrate the mechanism of the CBR, the elderly patient (#4) is selected, while the status of the attributes is {0.5, 31.52, 0.25, 0.25, 0.5}, which denotes the age group, index value of fall prediction, level of dementia, level of mental health and level of physical health, respectively. Except the index value of fall prediction, the other attributes are measured as nominal values. In the age group, the value 0.5 refers to the group ageing between 61 years old and 70 years old; the value 0.25 of level of dementia and level of mental health refer to the relatively mild symptoms and situations; the value 0.5 of the level of physical health denotes the intermediate situation. Subsequently, the similarity between the selected elderly patient and past cases stored in the case library can be calculated, and the top five similarity values with the case parameters are presented in Table 4. After ranking the similarity rates, the most similar case from all the past cases is selected as the source for updating the elderly’s care plan. A serious drop of similarity values was observed between cases CP1101 and CP0503 from 0.9277 to 0.7383. This result is a sign that the case library does not sufficiently include relevant cases. Although only the most relevant case is selected for assisting the care plan customisation, the sufficient large case library is beneficial to provide accurate reasoning to the care plan customisation. The domain experts, such as caregivers, are required to consider the selected past care plan to revise the current care plan to truly satisfy the elderly’s needs and health conditions. After the care plan is revised and updated, the approved care plans are then retained to the case library, and the finalised care plan is released to the designated elderly patients.
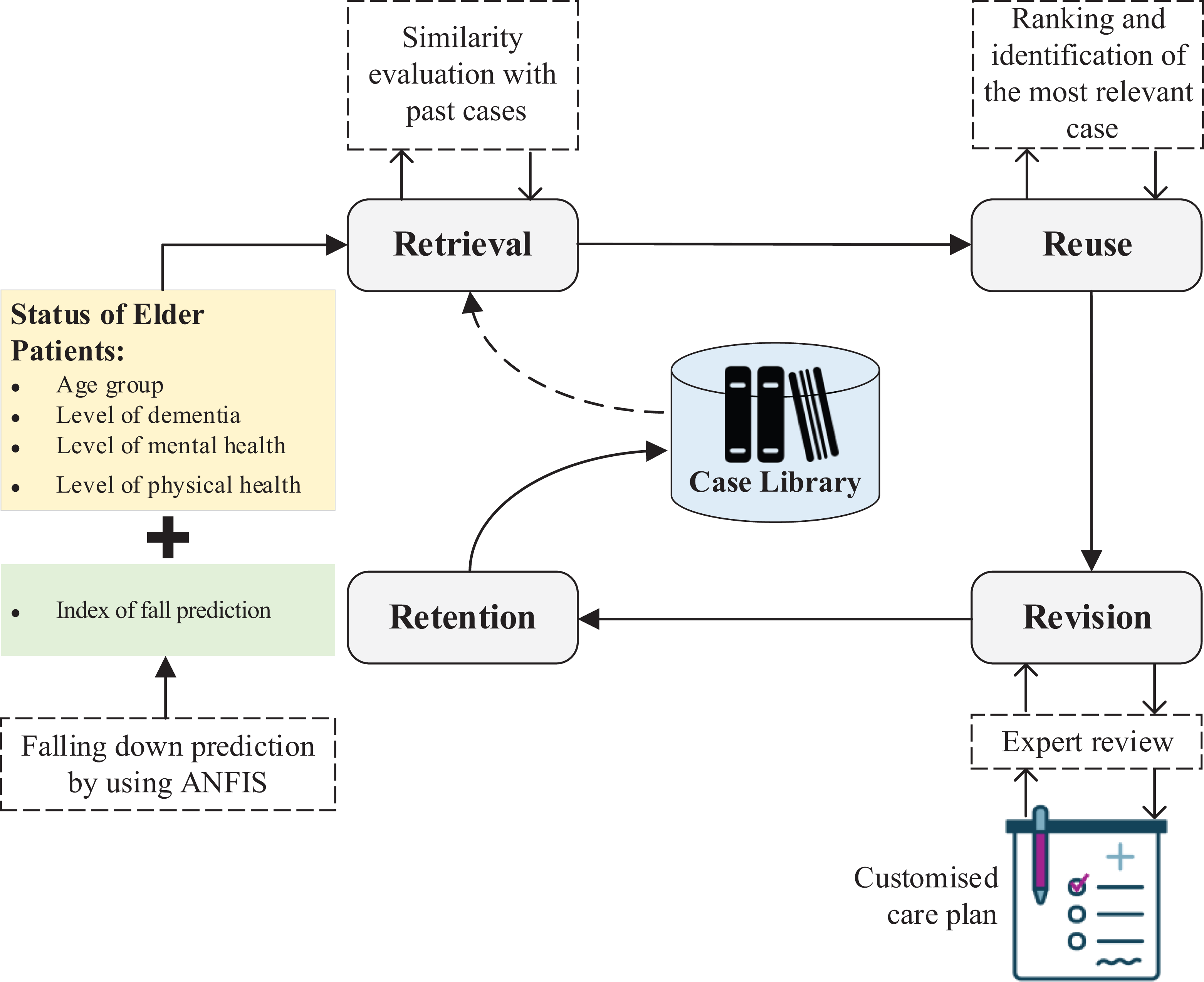
CBR mechanism for the care plan customisation.
Top five similar cases with similarity rates.
The care plan for the elderly patient (#4) is formulated with the aid of the proposed system, as shown in Figure 7. The revision of the care plan considers the personal health information of the patient (e.g. sex, age and body mass index), risk factors (e.g. swallowing difficulty, falls and wandering), functional assessment (e.g. medical history, mental state and mobility), needs of personal care (e.g. nursing care and social care) and other professionals’ comment to the patient. The entire care plan is divided into four major components, namely, (i) nursing diagnosis and concerns, (ii) goals and outcomes, (iii) interventions and (iv) review and evaluation.

Care plan sample for the elderly patient (#4).
Results and discussion
A systematic approach to connect elderly patients living in the healthcare facilities to the digital worlds is formulated by means of IoHT technology through the case study. The IoHT-enabled solution covers two functionalities of falling-down prediction and care plan customisation, which address the core needs of caregivers in the long-term care industry. On the one hand, the index value of falling-down prediction can be evaluated for all elderly patients based on historical records and performance by using ANFIS. The risk level of falling down for elderly patients can be quantified for caregivers to formulate and distribute adequate measures and remedies to maintain a designated level of QoC. On the other hand, care plan customisation is achieved by using CBR, wherein the new care plans for elderly patients are formulated according to high quality cases stored in the case library. To further discuss the values of this study, state-of-the-art comparisons and implications towards a next generation of LTCP are included in this section.
State-of-the-art comparisons
The proposed methodology (i.e. IoHT-CLS) in this study integrates IoHT, ANFIS and CBR as a whole to link elderly’s health conditions in real-time to provide decision support functionalities in the healthcare facilities. A comparison with state-of-the-art studies is conducted in this section to differentiate the values of the proposed methodology. In comparison with the work of Yu et al., 2 Asif-Ur-Rahman et al., 14 and Lam et al., 16 CBR was found to be promising in modifying the care plan in the healthcare industry, while the elderly satisfaction and QoC can be improved. Accordingly, the proposed methodology adopts a similar approach but additionally considering the falling prevention, which is the most critical risk in the elder care industry. The attributes in retrieving the historical cases are enriched through the inclusion of index value of falling down prediction by considering the fall prevention. Asif-Ur-Rahman et al. 14 adopted the IoMT technology in the context of long-term care, which was highly related to medical signs, information and treatments. Our work adopts the concept of IoHT technology for the long-term care to collect a wide range of healthcare-related data, including medical data, personal health status, activity and behaviour. A broader scope for the healthcare data collection and acquisition is suggested in the proposed methodology. In view of the fall prevention, previous work 20,21 examined the body movements and behaviour to establish the fall detection mechanism. However, the proposed methodology formulates a pro-active approach to form an index value of falling down prediction based on age and health condition. Apart from the existing robust fall detection mechanism, this study formulates the fall prevention by using ANFIS, while the estimates of fall prediction can be quantified to trigger the care plan revision and updates. Overall, this study presents an integrated and intelligent approach to connect data of the elderly in the physical world to the digital world, resulting in effective decision support for caregivers. This study creates an intelligence system for improving the QoC in nursing homes by means of real-time health monitoring, fall prediction and care plan customisation, which is regarded as a novel healthcare information system in the long-term care industry. The proposed system is designed and developed to cater for the needs in nursing home, while the routine process, including health monitoring, risk management and care plan formulation, can be digitalised.
To further validate the proposed system, a comparative analysis with existing IoT-based applications in the healthcare industry are considered, 26 –29 as shown in Table 5.
Comparison between the proposed system and existing studies.

2D-DWT-1L: 2D discrete wavelet transform 1 level; 2D-DWT-2L: 2D discrete wavelet transform 2 level; AES: advanced encryption standard; RSA: Rivest–Shamir–Adleman; ANFIS: adaptive neuro-fuzzy inference system; CBR: case-based reasoning.
Most existing healthcare systems were developed according to the typical IoT paradigm without considering the fog and mist computing in the system deployment. The data directly stored in cloud computing may jeopardise the health of the IoT network and consume substantial computational power and resources. In addition, the existing systems focused on the perception in the healthcare scenario, without using the data collected by IoT technologies to provide decision support functionalities in the healthcare industry. In view of the above-mentioned weaknesses, the proposed system addresses the pitfalls from the existing work, which is built according to the IoHT paradigm with integrating ANFIS and CBR to achieve fall prediction and care plan customisation. Therefore, such an intelligent system leads to the evolution of LTCP in the community.
Implications towards a next generation of LTCP
With the IoHT-enabled approach in the long-term care industry, decision makers, for example care managers and nurses, are effective in providing elderly-oriented care services to the patients, while maximisation of QoC and better cost control can be reached. In the current paradigm of LTCP 2.0, a holistic structure for providing long-term care services in the community is established, and the service customisation has been emphasised to cater specific elderly’s needs and wants, instead of managing them in a centralised manner. The better QoC in the care services can bring to the improvements of QoL to the elderly.
The potential of reaching the evolution of LTCP is substantially great in near future due to the dawn of smart systems, digital transformation and AI. From this study, the integration of IoHT and AI starts changing the existing operations and providing additional decision support functionalities in the industry. All the elderly’s data and information can be centralised for further data analytics, which can generate a positive impact to care services and operations. From the outlook of LTCP, the fusion of emerging technologies and methodologies can be continued to establish holistic and robust care services to the elderly, including home care and residential care. To treat this study as the foundation for future LTCP, digital twins for the elderly and care services can be established 30,31 . Accordingly, truly pro-active strategies on providing long-term care services can be established from the digital simulation of the elderly and operations 32 . In addition to connecting the physical world to the digital world, the decentralised identity by means of blockchain can also be formulated, and the identity verification between various healthcare centres can be simplified 33 . Medical and care records can be linked to the elderly in a secure and immutable manner 34 . Thus, the trust of the records can be established.
Concluding remarks
In summary, this study proposes an integrated approach consisting of IoHT and AI to improve the decision support functionalities under the environment of LCTP 2.0. To align the goal of elderly-oriented and -customised services, the proposed methodology enables the data acquisition by IoHT technology, while the fall prevention and care plan customisation are achieved by the data-driven analytics of ANFIS and CBR. The implementation plan is suggested along with the case study to deploy the proposed methodology in real-life situations, wherein the mechanism of falling-down prediction and care plan customisation are described step by step in detail. The risk level of falling down to the elderly can be effectively evaluated by using ANFIS, which can be further used in the CBR mechanism to modify the care plans in accordance with elderly’s requirements and health conditions. This mechanism contributes to the comprehensiveness of LCTP 2.0 and aligns to the objectives for long-term care services in the community. The technological fusion in the long-term care industry is still at a preliminary stage, which has a high potential to further develop various intelligent systems, such as digital twins and blockchain, to enrich the operational effectiveness and reliability of the care services.
The decision-making process on falling down prediction and care plan customisation is strengthened with the use of the proposed system in nursing homes. Meanwhile, the system autonomy and adaptability are enhanced through the deployment of IoHT and adoption of AI methodologies. However, this study is limited to only one case study to examine the effectiveness and performance of the proposed system, and the number of cases stored in the case library is limited for the illustration of the system mechanism. In the future, additional case studies should be considered for the implementation of IoHT, ANFIS and CBR in the nursing homes. Apart from the risk of falling down, other critical risk factors, including swallowing difficulty, wandering, cognitive impairment, emotion performance, behavioural problems and allergies, can be estimated by means of fuzzy inference systems. Overall, a robust and comprehensive healthcare solution can be developed to address the growing needs of nursing care to the elderly in the community.
Footnotes
Acknowledgement
The authors would like to thank the Department of Systems Engineering and Engineering Management of The City University of Hong Kong for inspiring the development of this research.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.