
Abstract
The literature has suggested that social norms and perceptions of risk and severity are critical variables in predicting protective health behaviors. Using an integrative conceptual framework, this study evaluates educational level, socioeconomic status, injunctive pro-care norms, perception of risk, and severity of COVID-19 as predictors of hygiene behaviors, mask use, and physical distancing. Participants included 2,075 adults from Chile, Mexico, and Colombia, three countries with the worst pandemic management. A structural equation model including the hypothesized structure of relations among the study variables fitted the data well and was invariant among Chilean, Mexican, and Colombian data. As proposed, injunctive pro-care norms against COVID-19 predicted protective health behaviors directly and indirectly through the perception of the risk and severity of COVID-19, and educational level predicted pro-care norms against COVID-19. These findings are essential in light of the development of prevention campaigns and the promotion of COVID-19 care strategies.
Introduction
Controlling the COVID-19 pandemic relies on mass vaccination and people maintaining the recommendations proposed by the World Health Organization [WHO], which include adopting protective behaviors, such as hygiene, physical distancing, and the use of masks (Phillips, 2021). Countries have followed the WHO guidelines and have implemented the adoption of different strategies to face the pandemic. Examples of these strategies include the mandatory use of masks, the constant recommendation of handwashing, and the use of thermometers and alcohol gel when entering closed spaces. When case numbers were high, measures were also more severe, such as lockdowns, restrictions on the number of people in closed places, and recommendations to avoid crowded spaces (Anderson et al., 2020; Anderson, Hollingsworth, et al., 2020; Block et al., 2020; Cavazos-Arroyo & Pérez de Celis-Herrero, 2020; Gerber et al., 2021; Paterlini, 2020; Sabat et al., 2020). Evidence has shown that these measures have effectively slowed the spread of COVID-19 (Anderson et al., 2020). Maintaining protective behaviors against COVID-19, especially when considering the new variants and the politics of returning to normality after two years of the pandemic, is of particular importance.
Countries with high levels of social inequality, extreme poverty, and informal labor markets have shown lower adoption and maintenance of healthcare behaviors. Consequently, with its high levels of social and structural inequities, disparities in access to health services, high prevalence of chronic diseases, and governance and human resource limitations, Latin America has become one of the most vulnerable regions to the effects of the pandemic (Americas Society & Council of the Americas, 2021; Castro, 2020). Chile, Mexico, and Colombia are among the 10 countries with the worst pandemic management (Lowy Institute, 2021). These countries have shown low adherence to protective behaviors and have more confirmed cases and deaths (per million people and as a proportion of tests). Despite these similarities, the impact of the pandemic has been uneven within countries.
Specifically, a re-analysis of the results obtained by Meda-Lara et al. (2021) of the data from Chile, Mexico, and Colombia revealed that Colombians reported lower health behaviors, such as “Washing my hands with soap and water” than Chileans and Mexicans. When asked about wearing masks (regardless of the presence or absence of symptoms), Chileans reported greater use, and Mexico had lower use of masks. Finally, regarding keeping a distance from other people, Chileans adhered more to this specific measure, and Mexicans had the lowest adherence. It is important to note that the findings of Meda-Lara et al. (2021) should also consider sociocultural aspects. Mexico and Colombia are characterized by being collectivist cultures and in them prevails the cultural value of familism, which emphasizes the strength of family ties with feelings of loyalty, reciprocity, solidarity, and obligation towards one's own nuclear and extended family (Losada et al., 2010; Nicasio et al., 2019). The value of familism and the positive evaluation that significant others have on one's behavior has shown associations with protective and healthcare behaviors in Latino populations (Le, 2020). Meanwhile, although Chile also has high levels of familism, it has been moving towards individualism (Garner, 2015) and, during the last years, has shown a decrease in the number of children per family, reducing the number of people living in one house. Furthermore, after eight months of lockdowns and several restrictive measures, every country began to experience “pandemic fatigue”. This phenomenon is characterized by a diminished motivation to adhere to the recommendations regarding protective behaviors (World Health Organization, 2020). Therefore, despite knowing the importance of taking care measures, these could not always be carried out due to the several reasons mentioned above, such as structural, economic, health, and cultural (Gerber et al., 2021), which could lead to inconsistencies between what should be done and what is done (Smith et al., 2012).
Understanding why people follow or do not follow these health behaviors and comply with the health policies to control COVID-19 is most important to foresee the end of the pandemic. Several health models in social and health psychology have studied and identified some critical variables associated with the adoption of different health behaviors, such as alcohol consumption, drug and condom use, and vaccination, among others (Conner & Sparks, 2005). In the current study, we are interested in testing Betancourt's integrative model for studying health behaviors (Betancourt et al., 2010; Flynn et al., 2011). This theoretical model suggests that health behaviors are influenced by variables of a different nature, differentiating between population categories (sociodemographic variables), cultural variables, and psychological processes. This model suggests that the most direct determinants of health behaviors are psychological processes (e.g., perception, emotions), which are influenced by socially shared beliefs such as norms and values associated with the specific health behavior (cultural variables). These cultural variables could affect behavior directly and indirectly through psychological processes. Finally, sociodemographic variables have a distal effect on health behaviors since they impact the generation of certain socially shared beliefs, norms, and values, functioning as sources of cultural variation.
The present study aimed to evaluate predictors of three specific COVID-19 protective behaviors: hygiene behaviors, mask use, and physical distancing. Using the integrative model of health developed by Betancourt and Flynn (2009); Betancourt et al. (2010), we will test predictors such as the perception of the risk and severity of COVID-19 as a psychological process and social norms for COVID-19 as a cultural variable. Educational level and socioeconomic status will be addressed as sociodemographic variables.
Perception of the risk and severity of COVID-19 as a psychological predictor of COVID-19 health behaviors
According to Brewer et al. (2007), risk perceptions are conceptualized as an assessment of the potential harm from specific events to which people might be exposed. The COVID-19 pandemic has posed a severe threat to the health of the world population due to its quick spread, many contagions, and deaths (Schneider et al., 2021). Health models have stated that risk perception is a crucial variable predicting engagement in several preventive measures (Wiedemann & Schütz, 2005) and healthcare behaviors, such as vaccination intention (Brewer et al., 2007) and the adoption of protective measures against COVID-19 (Gerber et al., 2021; Salazar-Fernández et al., in press). This means that when people perceive themselves as being at risk or consider the threat to be severe, they are more likely to engage in health behaviors (Gerber et al., 2021; Huang et al., 2020; Magnan et al., 2021; Savadori & Lauriola, 2021; Shao et al., 2017; Williams et al., 2010).
Risk perception is also associated with perceived severity, which is the assessment of the risk of contracting a condition, that is, how well people perceive themselves to be at high risk of contracting the disease (Cavazos-Arroyo & de Celis-Herrero, 2020). Perceived severity has also been shown to be a good predictor of health behaviors (Cho & Lee, 2015), such as protective care behaviors during the H1N1 pandemic (Ibuka et al., 2010) and the intention of getting the vaccine for H1N1 (Coe et al., 2012).
It is essential to highlight that during the COVID-19 pandemic, the WHO has proposed that some groups of people are more vulnerable and represent a higher risk of severe COVID-19. This group includes people older than 60 or with health conditions like lung or heart disease, diabetes, or conditions affecting their immune systems (Jordan et al., 2020). Despite recognizing higher-risk groups for which the coronavirus poses a severe risk, health authorities have stated that COVID-19 threatens all people. Therefore, they have called on everyone to adopt protective behaviors and prevent the spread of the virus.
Perceptions of the risk and severity of COVID-19 are critical in determining the public's willingness to adopt protective behaviors during pandemics, including frequent hand-washing, wearing masks, physical distancing, and avoiding public places (Dryhurst et al., 2020). Perception of risk and severity is influenced not only by previous experiences, attitudes, (mis)conceptions, and feelings towards the threat but also by social, cultural, and contextual factors (Cori et al., 2020). In this study, one of the aims is to investigate the influence of others (social norms) in determining the perception of risk and severity of COVID-19.
Socially shared norms as a sociocultural predictor of COVID-19 protective behaviors
Neville et al. (2021) have stated that when times are uncertain and threatening, people start looking to others within their social groups (i.e., ingroup) for guidance on how to behave. Social psychology literature has referred to this phenomenon as social norms, defined as rules or standards about the expectations of behaviors that can guide people's actions (Cialdini et al., 1991; Smith, 2020). Social norms have also been defined as cultural norms or shared standards for behaviors among members of a group or community (Chudek & Henrich, 2011; Gelfand & Jackson, 2016). Two aspects of norms, complementarily but differently, guide and impact behavior: descriptive and injunctive (Cialdini et al., 1991; Cialdini & Trost, 1998; Jacobson et al., 2011). Descriptive norms involve perceptions of others’ expected, typical or conventional behaviors and influence behavior through informational cues about others’ actual conduct (i.e., what others do), generating genuine and voluntary behaviors. In contrast, injunctive norms involve perceptions of which behaviors are approved or disapproved of by others (i.e., what others should do). Injunctive norms motivate behavior due to social rewards or punishments associated with executing the specific behavior (e.g., group pressure), causing ambivalent and non-lasting behaviors (Cialdini et al., 1991; McDonald & Crandall, 2015; Neville et al., 2021).
In the current COVID-19 pandemic, descriptive and injunctive norms are of utmost relevance because behavioral changes, such as adopting protective behaviors, must be implemented and maintained over time. Meta-analytic findings have shown that descriptive and injunctive norms have robust predictive value in several health behaviors, such as alcohol consumption, blood donation, and exercise, among many others (Sheeran et al., 2016). These findings highlight the relevance of significant others in executing different behaviors. This rationale suggests that it is expected that social norms would directly impact the adoption of COVID-19 protective behaviors. As anticipated, there is strong evidence that social norms, descriptive and injunctive, are relevant to the adoption and implementation of COVID-19 protective behaviors (Fischer & Karl, 2021; Gerber et al., 2021; Goldberg et al., 2020; Rivera Baeza et al., 2021; Salazar-Fernández et al., in press).
Although descriptive and injunctive norms are often aligned (i.e., what others should do is usually what is done), sometimes this is not the case (Eriksson et al., 2015). Governments and different communications media have made it difficult for people to comply with the rules to prevent the spread of the virus. For example, although reporters warn the public about the importance of using a secure mask, they may not be using one on live television. Alternatively, the media states that people should maintain a physical distance from each other, but they show footage of people in crowded places. Smith et al. (2012) have called this phenomenon the boomerang effect, which is when injunctive and descriptive norms are conflicted (e.g., people do not practice what they preach). These mixed norms could affect the perception of risk and severity because people do not know how to act. Chile, Mexico, and Colombia are among the 10 countries with the worst pandemic management, associated with higher confirmed cases and deaths per million people (Lowy Institute, 2021). This poor management and lack of efficiency during the pandemic has shown us that, at least at a country level, the influence of others performing protective behaviors is insufficient to encourage them to do the same (i.e., as a descriptive norm). That said, it is essential to study whether injunctive norms—what others should do—are associated with protective behaviors. Specifically, in this study, we expect people to be more likely to adopt protective measures if their significant others are worried about taking protective measures against COVID-19 and encourage or approve of pro-care norms (i.e., injunctive norms).
The mediating role of the perception of the risk and severity of COVID-19
Kasperson et al. (1988) proposed the idea of the social amplification of risk, which states that hazard events interact with cultural, social, and psychological processes through the perception of risk, shaping different behaviors. In the same vein, Renn et al. (1992) argued that risk perceptions are determined by cultural and social channels and have the potential to impact individual psychological processes and behaviors. That said, the recognition, interpretation, and communication from and to others of a threat impact the perception of its risk (Popovic et al., 2020; Renn et al., 1992). These authors suggest that social norms and informal interactions about threatening events determine risk perception, and, sequentially, the perception of risk impacts behavior. This sequence could imply that risk perception could mediate the relationship between injunctive social norms and protective behaviors. Furthermore, according to Betancourt's model (Betancourt & Flynn, 2009; Flynn et al., 2011), an indirect effect through the perception of risk and severity on the association between injunctive norms and protective behaviors should be expected. This mechanism would allow us to hypothesize that the concern and pressure of significant others to perform protective behaviors (i.e., social norms) could be explained by the increased perception of the risk and severity of COVID-19 (Savadori & Lauriola, 2021).
Injunctive norms as expectations and pressures from significant others could impact how risk information is processed (Grothmann & Patt, 2005; Renn, 2011; Swim et al., 2010). Thus, if my significant others believe it is appropriate to adopt protective behaviors against COVID-19 and I feel the pressure and motivation to meet these expectations, then COVID-19 will be perceived as a threat to the ingroup. Consequently, this increased perception of risk and severity would lead, probably, to the implementation of protective behaviors to cope with COVID-19, such as hand-washing, using a mask, and physical distancing (Gerber et al., 2021; Huang et al., 2012; Magnan et al., 2021; Savadori & Lauriola, 2021; Shao et al., 2017; Williams et al., 2010).
Contrary to Kasperson et al. (1988) and Renn et al. (1992), Norgaard (2011) and Wolf et al. (2010) have argued that social norms from family and friends could lead to decreasing the perception of risk and severity because they are perceived as part of the ingroup. According to Cruwys et al. (2020), the ingroup is not perceived as risky or threatening. When shared social identities are robust (e.g., with family and friends), the assessment of danger and threat is oriented to the outgroup rather than the ingroup. This approach is consistent with how COVID-19 has spread. Most contagions have occurred in the context of family or close friends and not among strangers because protective behaviors are relaxed when interacting with people with whom one is close but maintained in contact with strangers (Neville et al., 2021).
In the present research, we expect to provide evidence of the impact of injunctive norms on the perception of the risk and severity of COVID-19 and on the possible mediator effect of the perception of risk and severity between injunctive norms and protective behaviors. We will study relationship patterns in three Latin American countries characterized by strong social identities within the family and close friends (i.e., familism) (Valdivieso-Mora et al., 2016) to shed light on how these variables work in non-WEIRD (Western, educated, industrialized, rich and democratic) contexts (Henrich et al., 2010).
Sociodemographic variables on COVID-19 protective behaviors
Most of the current literature has focused on the associations between educational level and socioeconomic status in adopting protective behaviors against COVID-19. Specifically, researchers have found that people with lower educational levels are less likely to adopt healthy behaviors (Ross & Wu, 1995) or protective behaviors against COVID-19 (Gerber et al., 2021; Lüdecke & von dem Knesebeck, 2020; Sánchez-Arenas et al., 2021). Meanwhile, higher socioeconomic status and income are associated with adopting protective behaviors (Atchison et al., 2020; Bermejo-Martins et al., 2021; Mena et al., 2021; Papageorge et al., 2021; Sánchez-Arenas et al., 2021; Wright et al., 2020). Despite the above, Betancourt et al. (2011) have suggested that sociodemographic variables are not directly associated with health behaviors; instead, they should impact the cultural variables. In this study, social norms (i.e., injunctive pro-care norms) are expected to be influenced by socioeconomic status or educational level. Thus, the present study expects to find whether socioeconomic status or educational level—as sociodemographic variables—are possible sources of variability in the social influence of family and friends on protective behaviors against COVID-19. Specifically, it is expected that injunctive pro-care norms are determined by socioeconomic status and/or educational level. For example, it is possible that when people have a high educational level and come from a high socioeconomic status, they can access more trustworthy information about the prevention and contagion of COVID-19 (Gerosa et al., 2021; Zhong et al., 2020). When people understand what to do to prevent the spread of COVID-19, they are expected to be more likely to appreciate that their family and/or close friends value the adoption of injunctive norms that enhance protective behaviors against COVID-19, which can affect the adoption of these protective measures.
The present research
In the present study, we will test the Betancourt and Flynn (2009) integrative model to predict protective health behaviors against COVID-19, such as hygienic behaviors, mask use, and physical distance behaviors. First, we will explore whether this integrative model of health is invariant across three Latin American countries: Chile, Mexico, and Colombia. Secondly, we will examine the influence of psychological, cultural, and sociodemographic variables in predicting these protective health behaviors. Moreover, we will analyze the possible mediator role of the perception of the risk and severity of COVID-19 in the relationship between injunctive pro-care norms and protective behaviors. Finally, we will test the influence of educational level and socioeconomic status on injunctive pro-care norms.
Methods
Participants
Through non-probability international sampling, 2,886 people participated in the study by answering an online questionnaire. We exclude 779 participants because they have missing data in the study variables. Our final sample was 2,107. This sample size surpass the minimum sample size to detect a small effect size (i.e., 0.1), and considering a statistical power level of 0.8 for the relationship pattern tested in this study (see Figure 1), which is 1,454 participants (Soper, 2022). Of these participants, 48.3% lived in Chile, 27.1% in Mexico, and 24.6% in Colombia. Inclusion criteria considered participants of legal age (over 18 years old) living in their country during the COVID-19 pandemic. The participants were primarily women (69.7%) and were aged between 18 and 89 years old (M = 35.12, SD = 14.59). Participants from each country showed differences in age, marital status, socioeconomic status, and educational level. Supplementary Table 1 displays the participants’ sociodemographic characteristics from Chile, Mexico, and Colombia. Only participants with complete data in all the study variables were included in the analysis. The database of this study can be found at https://osf.io/9prk8.

Model (invariant for the Chilean, Mexican, and Colombian sample) predicting self-care COVID-19 behaviors.
Instruments
The participants responded to several study instruments (in Spanish), which are listed below (see Supplementary Table 2).
Injunctive pro-care norms against COVID-19
We used an adaptation and translation to Spanish by Cavazos-Arroyo and de Celis-Herrero (2020) of the self-reported scale developed by Harmsen et al. (2012). This scale was previously used by Rivera Baeza et al. (2021) and Salazar Fernández et al. (in revision). These three items assessed the influence of significant others on adherence to protective behaviors relating to the COVID-19 pandemic. The items were: “My significant others appreciate that I protect myself from COVID-19” (i1); “My significant others motivate me to protect myself from COVID-19” (i2), and “My significant others give me recommendations on how to protect myself from COVID-19” (i3). These items showed good levels of internal reliability across the three countries (Chile ω = .883, Mexico ω = .830, Colombia ω = .847). Participants responded using a 5-point Likert scale, from (1) Totally disagree to (5) Totally agree. Higher scores indicate an injunctive pro-care norm of significant others on pro-care behaviors against COVID-19.
Risk and severity perception of COVID-19
We used two adapted items to measure the perception of risk and severity. To measure the risk perception of COVID-19, we employed the item created by Rajamoorthy et al. (2018) and adapted to Spanish by Cavazos-Arroyo and de Celis-Herrero (2020): “I think I have a high risk of getting COVID-19.” The item assessing severity perception, “My body could resist COVID-19 infection,” was created by the research team. In both items, the participants indicated their degree of agreement with the statements using a 5-point Likert scale, from (1) Totally disagree to (5) Totally agree. High scores on the perception of risk item indicate a higher perception of risk of COVID-19 contagion, while high scores on severity perception indicate lower perceived severity of COVID-19 (i.e., indirect item). In each country, inter-item correlations between risk and severity perception were significant, of small magnitude, and negative (Chile r (1163) = −.201, p < .001; Mexico r (561) = −.182, p < .001, Colombia r (643) = −.103, p = .009).
Protective behaviors against COVID-19 scale
These items assess different protective behaviors against COVID-19, such as: “I wash my hands with soap or sanitizer after contact with others”; “I disinfect surfaces I touch (handles, tables)”; “I wear a mask”; “I avoid leaving my house”; “I avoid physical contact with other people,” and “I avoid large groups of people” (e.g., restaurants, shopping malls). Participants were asked to indicate the frequency of performing these behaviors using a 5-point scale ranging from (0) Never to (4) Always. Exploratory factor analysis of these items revealed a two-factor structure. One factor grouped the items of hygiene behaviors related to COVID-19 (Chile ω = .671, Mexico ω = .667, Colombia ω = .681). The other factor grouped the items related to physical distancing (Chile ω = .790, Mexico ω = .822, Colombia ω = .779). The item related to mask use was not associated with the two factors, so we used it as a one-item indicator. Higher scores in the two factors and on the item related to mask use indicate a greater frequency of adopting protective behaviors to avoid the spread of COVID-19.
Sociodemographics
Participants responded to several questions about their sociodemographic backgrounds, such as gender, age, educational level (on an 8-point scale, from incomplete middle-school [1] to postgraduate studies [8]), and perception of socioeconomic status (on a 6-point scale, from lower [1] to very high [6]).
Data collection
The ethics committees of the universities of each country approved the data collection. The survey was applied using the online platform QuestionPro (between December 2020 and April 2021) and disseminated through different social networks (e.g., Facebook, Instagram, Twitter, and WhatsApp). It included an informed consent form that indicated the study's objective, ensured anonymity and confidentiality, and provided the contact details of the responsible researchers. Answering the survey took approximately 15 min.
Statistical analysis
Data were explored descriptively in each country. The internal consistency of the measures used was evaluated with McDonald's omega (Revelle & Zinbarg, 2009). Then, we used multigroup structural equation models on the R software's Lavaan package (Rosseel, 2012). Estimations were made using the WLSMV estimator, which is more suitable for ordinal data (Flora & Curran, 2004). Before estimating the structural coefficients of the model across countries, we assessed the model invariance. Sass and Schmitt (2013) have stated that measurement invariance is necessary for testing structural coefficients across groups (see Figure 2 for an overview of the statistical analysis involved to ensure measurement invariance). Following the sequence proposed by Milfont and Fischer (2010), we imposed hierarchical constraints on our model (form, factor loading, intercepts, and residuals) and tested whether the model fit did not worsen (see Mackinnon et al. [2022] for a tutorial and respective code using lavaan). The proposed relationship pattern was modeled by imposing successive restrictions, as suggested by Putnick and Bornstein (2016). First, the model was adjusted separately for each sample without any restrictions. Secondly, we tested the configural model, which was restricted to having the same form or configuration between countries. Then, the metric equivalence was tested, constraining the factor loadings to be equal across countries. This step ensures that the latent factors have the same semantic meaning. If the restriction of the factor loadings did not worsen the model fit, then metric invariance is achieved, and scalar invariance should be tested. Scalar invariance implies the restriction of the intercepts across countries. By imposing an equality restriction of the intercepts, the model assures that the mean differences in the latent construct capture all mean differences in the shared variance of the items, which allows meaningful comparison between groups. If the fit of the scalar invariance is not worse than the fit of the metric invariance, then scalar invariance es accepted. Although scalar invariance is necessary to assess meaningful comparisons between groups, the restriction of residuals ensures a more restrictive invariance. Strict invariance means that the sum of the variance not shared with the factor (specific variance) and the measurement error (error variance) is similar across groups. If the fit of the strict invariance model is not worse than the fit of the scalar model, then strict invariance is achieved. Once we had shown that our model has measurement invariance, we tested structural invariance. Structural invariance implies the restriction of the structural paths or regression coefficients to be equal between countries. If the model fit is adequate, the complete model is equivalent between countries. To decide whether to accept or reject the invariance model tested, we used the CFI and the RMSEA. According to Rutkowski and Svetina (2017), and Sass et al. (2014), if
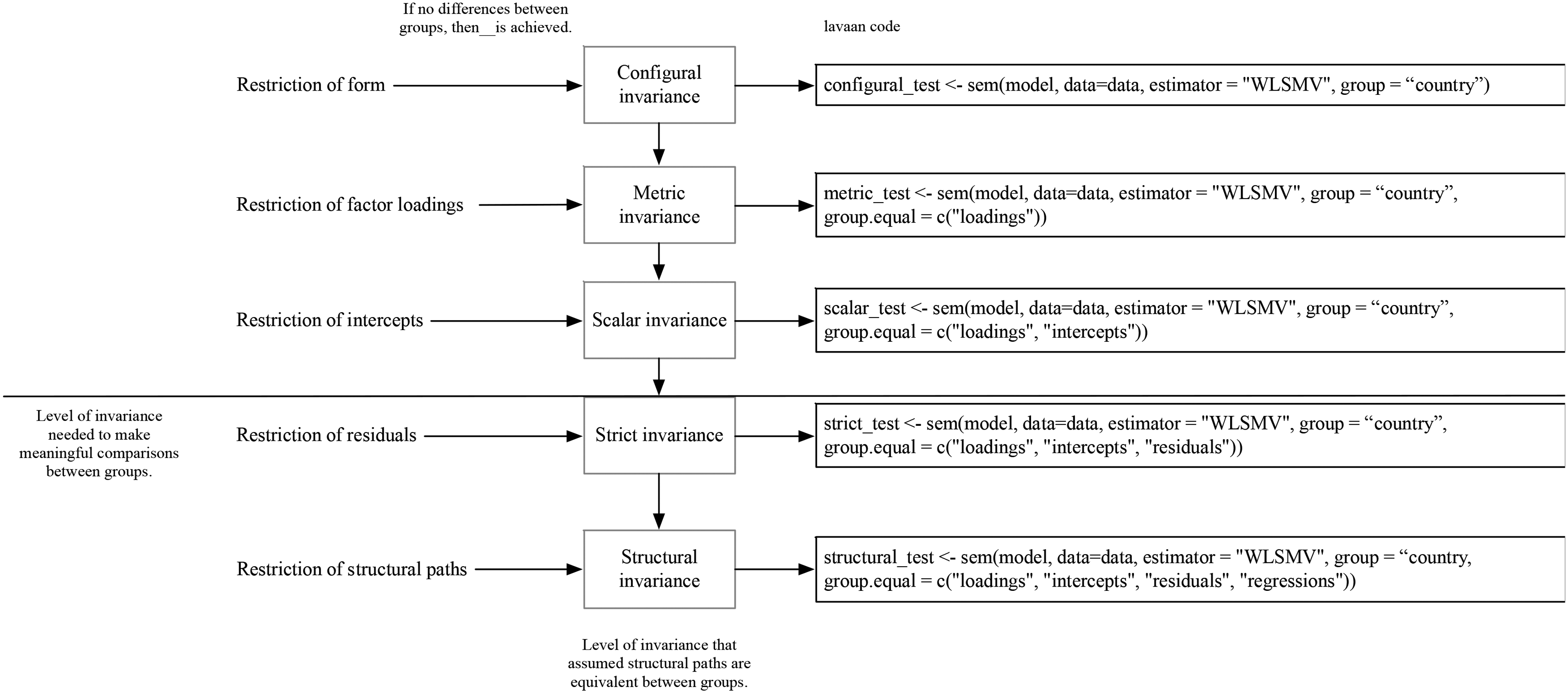
Overview of the statistical analysis to assess invariance between countries with their respective Lavaan code.
The estimated models were evaluated according to the following global fit indices: χ2, the comparative fit index (CFI), the Tucker–Lewis index (TLI), the square root of the standardized mean residuals (SRMR), and the square root of the mean error of approximation (RMSEA), with its confidence interval at 90%. According to the conventional goodness-of-fit criteria, these indices were interpreted: CFI and TLI > .95, and SRMR and RMSEA ≤ .08 (Marsh et al., 2004; Schermelleh-Engel et al., 2003).
Results
Correlations between the variables of the present study are shown in Table 1. This analysis revealed moderate associations.
Spearman correlations between the study variables
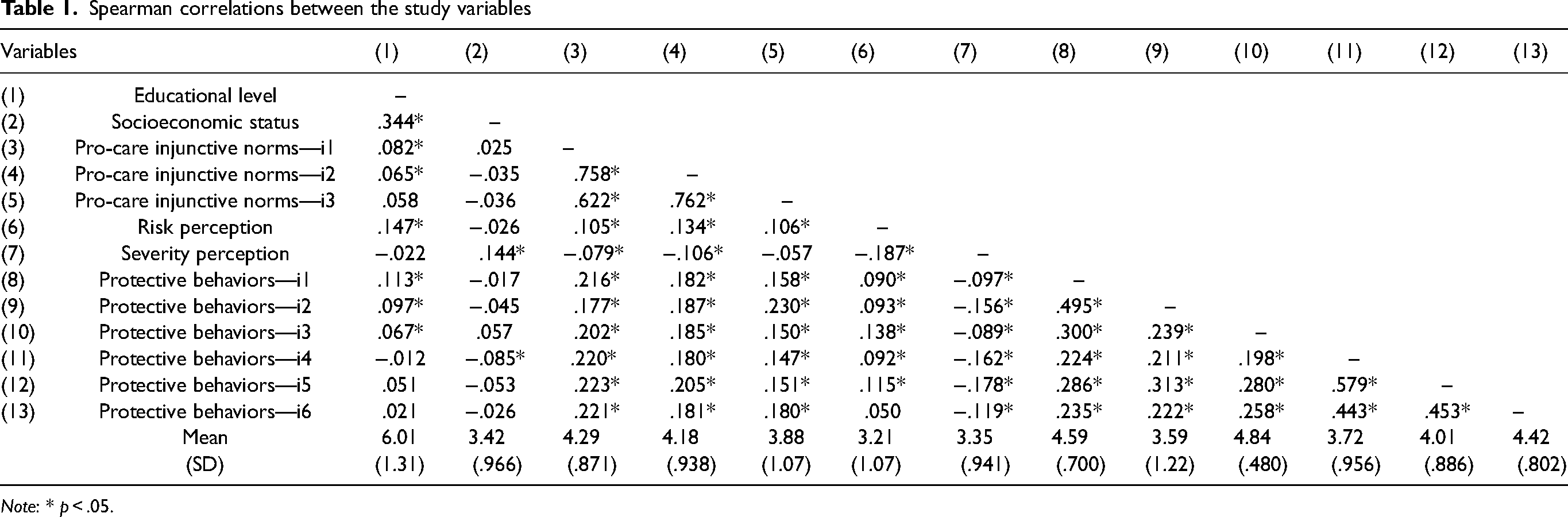
Note: * p < .05.
Model invariance
Using the model of Betancourt and Flynn (2009); Betancourt et al. (2010) for health behaviors, we tested whether COVID-19 protective behaviors (hygiene, mask use, and physical distancing) were predicted by the perception of the risk and severity of COVID-19—as a psychological factor—and injunctive COVID-19 pro-care norms as a cultural variable. Educational level and socioeconomic status were used as sociodemographic variables influencing the cultural factor (see Figure 1). Because we found statistically significant differences across countries regarding the age of the participants (F (2, 1151.995) = 94.875, p < .001), we decided to control this variable in our model. Controlling for the age of the participants, we found an excellent model fit in each country, Chile:
Fit indices for invariance tests

Note: Configural invariance implies restriction of the model across countries; Metric invariance implies restriction of the factor loadings across countries; Scalar invariance implies restriction of the intercepts across countries; and Strict invariance implies restrictions of the residuals across countries.
A model predicting protective behaviors in Chile, Mexico, and Colombia
Regarding our model (see Figure 1), we found that while educational level was positively associated with injunctive pro-care norms (β = .051, p = .007, 95% CI = [.008, .049]), socioeconomic status was not (β = .012, p = .587, 95% CI = [−.024, .042]). At the same time, injunctive pro-care norms were positively and directly associated with the perception of the risk and severity of COVID-19 (β = .221, p < .001, 95% CI = [.059, .182]), with COVID-19 hygienic behaviors (β = .225, p < .001, 95% CI = [.109, .221]), mask use (β = .162, p < .001, 95% CI = [.069, .161]), and with physical distancing behaviors (β = .189, p < .001, 95% CI = [.091, .242]). Regarding the perception of risk and severity of COVID-19, we also found that it was positively associated with hygienic behaviors (β = .308, p < .001, 95% CI = [.192, .635]), mask use (β = .262, p < .001, 95% CI = [.152, .532]), and with social distance behaviors (β = .489, p < .001, 95% CI = [.448, .884]). All the variables in our model managed to account for 15% of the variance of hygienic behaviors, 5.4% of the variance of mask use, and 14.9% of the variance of physical distancing behaviors. We also found a partially mediated effect between injunctive pro-care norms through the perception of risk and severity on hygiene behaviors, the use of a mask, and physical distancing behaviors, respectively (b = .050, p = .006, 95% CI = [.005, .046], b = .095, p = .002, 95% CI = [.034, .157] and b = .041, p = .010, 95% CI = [.010, 073]). More importantly, the partial mediation effect on the hygiene behaviors represents 25.5% of the total effect, 44.2.% of the total effect on the use of a mask, and a 25.5% of the total effect on physical distancing behaviors.
Discussion
This study aimed to evaluate predictors of three specific COVID-19 protective behaviors: hygiene behaviors, mask use, and physical distancing in three Latin American countries: Chile, Mexico, and Colombia. Despite the numerous differences between these countries, we found that the model, controlling for age, remained invariant across countries. Injunctive pro-care norms and the perception of risk and severity, which also mediates this relationship, were the main predictors of COVID-19 protective behaviors. Only educational level was associated with the adoption of injunctive pro-care norms.
Our results highlight that the integrated model of health developed by Betancourt and Flynn (Betancourt et al., 2010; Flynn et al., 2011) provides an appropriate theoretical framework that allows the understanding of sociodemographic, cultural, and psychological variables in protective health behaviors in the context of the COVID-19 pandemic. Moreover, the model was invariant, or equivalent, in the countries assessed in our study: Chile, Mexico, and Colombia. This model allowed us to better comprehend and integrate the critical variables from social and health psychology to direct the fight against COVID-19. This invariant model contributes to the development of generalizable strategies, even when countries have implemented different health measures to deal with the pandemic.
As the previous literature has stated, the perception of risk and severity is a critical variable in predicting protective behaviors against COVID-19 (Dryhurst et al., 2020; Gerber et al., 2021; Magnan et al., 2021; Savadori & Lauriola, 2020). Research suggests that when persons perceive themselves as being at high risk of getting infected with COVID-19 or having a severe prognosis, they are more likely to adopt protective behaviors such as hygienic behaviors, mask use, and physical distance behaviors. Our results, in three different countries, confirm this. These findings are particularly relevant because the WHO has identified higher-risk groups with the worst prognosis of COVID-19, such as persons older than 60 years with heart or lung conditions, diabetes, or who are immunocompromised. Nevertheless, people without these conditions have also developed adverse health outcomes (e.g., chronic symptoms and death) (Jordan et al., 2020). This highlights the crucial role of the perception of risk and severity in all populations.
It is also essential to draw attention to the ongoing flexible normalization strategies for COVID-19 implemented in several countries in the world, including optional or no use of masks and the resurgence of large group activities in open and closed spaces without considering physical distancing. These measures could reduce the perceived risk of COVID-19 and promote a new wave of contagion (Bauer et al., 2021; Wise, 2022). Thus, public health strategies must maintain an adequate perception of risk and severity to promote the adoption of COVID-19 protective behaviors for as long as the pandemic lasts. Health policies should also encourage people to vaccinate with the complete schema and updated doses because the new variants (e.g., delta, omicron, and subvariants such as BA.3, BA.4, and B.A.5) are potentially as contagious and dangerous as the former virus. In promoting the adoption of protective behaviors, social and psychological sciences play a relevant role in providing empirical evidence to generate effective communication strategies focusing on these critical variables (Chou et al., 2020). For example, governments and the media should be aligned in promoting norms (injunctive and descriptive) associated with the use of masks and hygienic and physical distancing behaviors to avoid the boomerang effect (Smith et al., 2012).
Furthermore, our results also provide evidence of the direct impact of pro-care injunctive norms against COVID-19 on the adoption of protective behaviors, which is in line with previous research (Collis et al., 2022; Fischer & Karl, 2021; Gerber et al., 2021; Goldberg et al., 2020; Rivera Baeza et al., 2021; Salazar-Fernández et al., in press). As Neville et al. (2021) declare, in times of uncertainty and threat such as the pandemic, people guide their behaviors by following what their social groups appreciate and value, such as people they are close to (i.e., family and friends). Our results suggest that if significant others value the adoption of protective behaviors, it is more likely that individuals will endorse hygienic behaviors, mask use, and physical distancing behaviors to protect themselves from COVID-19. More importantly, pro-care injunctive norms directly affect protective behaviors and are mediated by the perception of risk and severity. This partially mediated effect (more than 25% of the effect was mediated) is consistent with previous studies proposing that cultural, social, and psychological processes impact different behaviors through the perception of risk (Kasperson et al., 1988; Renn et al., 1992). Moreover, we found evidence supporting the notion that the concern and appreciation of significant others regarding the adoption of protective behaviors will lead to an increased perception of the risk and severity of COVID-19. This concern should motivate and pressure individuals into adopting protective behaviors such as hygiene, use of masks, and physical distancing (Gerber et al., 2021; Huang et al., 2012; Magnan et al., 2021; Savadori & Lauriola, 2021; Shao et al., 2017; Williams et al., 2010). This partial mediation hints that injunctive norms are also a key variable promoting protective behaviors, acting directly on those behaviors and indirectly through the perception of risk and severity. Our results are also coherent with familism, a cultural value characteristic of Latin cultures that emphasizes strong bonds and solidarity with one's nuclear and extended families (Valdivieso-Mora et al., 2016). Familism implies that what the family thinks about what should (not) be done is fundamental (Cahill et al., 2021; Nicasio et al., 2019). Thus, familism can guide self-care behaviors because the pressure to follow the family's norms and expectations is strong (Campos et al., 2019; Christophe & Stein, 2022; Falzarano et al., 2021) in countries such as Chile, Mexico, and Colombia. Although we did not measure familism in this study, future research should consider this variable in adopting health behaviors because these behaviors benefit individuals and others, emphasizing a sense of “we” instead of “I.”
Regarding the sociodemographic variables, we only found empirical support for educational level showing a positive but small association with injunctive pro-care norms, while socioeconomic status did not. The previous literature has suggested that persons with higher educational levels are more likely to know, distinguish, and access trustworthy information about how COVID-19 spreads and how to prevent it (Gerosa et al., 2021; Zhong et al., 2020), so it is more probable that they will develop pro-care norms about COVID-19. Although research has also found evidence for socioeconomic status as a predictor, our results do not confirm this (Atchison et al., 2020; Bermejo-Martins et al., 2021; Mena et al., 2021; Papageorge et al., 2021; Sánchez-Arenas et al., 2021; Wright et al., 2020). One possible explanation relates to the way this variable was measured. This item is a proxy for socioeconomic status because the question asks for the perception of socioeconomic status, which might not be related to the respondents’ actual status or income. Future studies should consider this problem and address it.
The results of the present study are relevant considering the existing research because they offer a prediction model for COVID-19 protective behaviors integrating sociodemographic, cultural, and psychological variables. Furthermore, our model was equivalent for three Latin American countries: Chile, Mexico, and Colombia. Previous research, like that conducted by Meda-Lara et al. (2021) using Latin American samples, provides evidence of sociodemographic and psychological variables with a descriptive aim. Still, they do not consider how these variables interact with each other or their pattern of relationships. In contrast, the study by Gerber et al. (2021), using only a Chilean sample, tested a regression model using a longitudinal design. Still, their focus was not to test the relationship patterns between these variables and how they are associated with several protective behaviors in an integrative model.
The COVID-19 pandemic is far from over and has had a severe and long-lasting impact on the mental health of the population (Kumar & Nayar, 2021). Moreover, people have shown pandemic fatigue, which reduces their adherence to the pandemic restrictions (Reicher & Drury, 2021). In this context, authorities have called for a “new normality” in which people live as if COVID-19 has ended or is under control. Nevertheless, the threat of contagiousness is still present. Protective behaviors against COVID-19 will continue to be fundamental in dealing with the virus. In the last few months, cases of COVID-19 have fluctuated between increases and decreases, leading people to stop adhering to protective measures. This problem underlines the importance of this study as it allows us to propose possible guidelines for action by emphasizing the key variables that need to be addressed. First, risk communication is essential. Risk communication should properly alert the population when the health contexts are critical (rises in case numbers), so people can know when to re-adopt protective behaviors more diligently. However, risk communication should also give people some respite when the case numbers fall, such as after a massive vaccination campaign or when other respiratory diseases are controlled. These breaks are of utmost importance because critical and prolonged times of high-risk perception are associated with severe mental fatigue and lower adherence to protective measures (Reicher & Drury, 2021; Torrente et al., 2022). During these periods, prevention and control policies should be implemented because they play a role in reducing public anxiety and uncertainty (Ding et al., 2020). Second, health authorities should reinforce adopting protective behaviors based on shared responsibilities more than individual ones. As suggested by our findings on the direct and indirect role of injunctive pro-care norms, these messages should focus on taking care of our close ones, emphasizing that taking care is something that we should do (e.g., “we should be taking care of others”). Previous research has found positive evidence of the role of messages and interventions based on injunctive norms in different contexts (Bhanot, 2021; Lawrence, 2015; Zhuang, 2022).
This study has provided timely and empirical evidence on the pandemic and its consequences for individuals and society concerning the variables involved in adopting protective behaviors in the context of the COVID-19 pandemic in three Latin American countries, which have shown poor pandemic management. More importantly, we showed that, invariantly, educational level, injunctive pro-care norms, and the perception of the risk and severity of COVID-19 are critical variables that predict health behaviors. Nevertheless, our research presents some limitations. The first limitation is the use of cross-sectional data, which does not allow us to raise causal inferences about the relationship pattern tested, only associations between the variables of our model. Future longitudinal studies should test whether this model and its mediation can be maintained over time. The second issue relates to purposive sampling using online questionnaires. We decided to use this sampling method to collect data safely from participants during the pandemic. The problem of using non-probabilistic sampling also implies that the samples of each country might not be representative. Thus, the results described in this article should only apply to the specific sample characteristics. A third point that needs to be addressed is associated with the measures of protective COVID-19 behaviors. We used general items addressing the frequency of adopting each type of behavior. These items were not context-specific, so we could not test whether people were more or less likely to adopt these behaviors in intimate contexts, such as with friends or family. This knowledge would have provided more insight into how the spread of COVID-19 is more frequent when interacting with close ones than with strangers. This problem merits further investigation.
In conclusion, the results of this study highlight the importance of considering sociodemographic, sociocultural, and psychological variables in predicting the protective health behaviors of COVID-19 in Chile, Mexico, and Colombia. These findings have become essential in light of the development of prevention campaigns and the promotion of COVID-19 care strategies to mitigate the adverse effects of the pandemic and ensure the effectiveness of interventions, considering that the performance of these behaviors should be maintained since the new variants of the virus are highly contagious and have a high transmission capacity.
Supplemental Material
sj-docx-1-pac-10.1177_18344909231181763 - Supplemental material for Should we take care of each other? Enhancing COVID-19 protective behaviors, a study in Chile, Mexico, and Colombia
Supplemental material, sj-docx-1-pac-10.1177_18344909231181763 for Should we take care of each other? Enhancing COVID-19 protective behaviors, a study in Chile, Mexico, and Colombia by Camila Salazar-Fernández, María José Rivera Baeza, Natalia Salinas-Oñate and Diego Manríquez-Robles in Journal of Pacific Rim Psychology
Supplemental Material
sj-docx-2-pac-10.1177_18344909231181763 - Supplemental material for Should we take care of each other? Enhancing COVID-19 protective behaviors, a study in Chile, Mexico, and Colombia
Supplemental material, sj-docx-2-pac-10.1177_18344909231181763 for Should we take care of each other? Enhancing COVID-19 protective behaviors, a study in Chile, Mexico, and Colombia by Camila Salazar-Fernández, María José Rivera Baeza, Natalia Salinas-Oñate and Diego Manríquez-Robles in Journal of Pacific Rim Psychology
Supplemental Material
sj-docx-3-pac-10.1177_18344909231181763 - Supplemental material for Should we take care of each other? Enhancing COVID-19 protective behaviors, a study in Chile, Mexico, and Colombia
Supplemental material, sj-docx-3-pac-10.1177_18344909231181763 for Should we take care of each other? Enhancing COVID-19 protective behaviors, a study in Chile, Mexico, and Colombia by Camila Salazar-Fernández, María José Rivera Baeza, Natalia Salinas-Oñate and Diego Manríquez-Robles in Journal of Pacific Rim Psychology
Footnotes
Acknowledgments
The authors would like to thank all the researchers in Chile, Mexico, and Colombia who contributed to disseminating the survey and data collection.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Fondo Nacional de Desarrollo Científico y Tecnológico (grant no. 11181020).
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.