
Abstract
Pivetti et al. (2021a; 2021b) examined links between COVID-related conspiracy beliefs and acceptance of vaccinations in Italy and Finland in 2020. They found that moral purity negatively predicted confidence in science, whereas political orientation predicted COVID-related conspiracy beliefs. Confidence in science, general conspiracy beliefs, and COVID-related conspiracy beliefs were found to negatively predict support for governmental restrictions and attitudes towards vaccines, and positively predict perceptions of informational contamination. Finally, attitudes towards vaccines in general strongly predicted attitudes towards the COVID-19 vaccine. The current research seeks to replicate these findings conceptually on a predominately Muslim sample (N = 570, M age = 26.69, 69.8% females) in Turkey in 2021, when the COVID vaccines were widely available. Measures of religiosity and left, center, and right political orientations were added to the original instrument. Hypothesized serial mediational models were tested using structural equation modelling. Results revealed that left and center political orientations positively predicted COVID-related conspiracy beliefs and confidence in science. Religiosity was negatively related to confidence in science. Confidence in science and COVID-related conspiracy beliefs predicted general attitudes toward vaccines. Conspiracy beliefs predicted COVID-related conspiracy beliefs, which in turn negatively predicted support for government restrictions and positively predicted distrust in mainstream media. Attitudes towards vaccines were strongly and positively related to attitudes toward COVID-19 vaccines.
[This paper was added to the Special Issue on “Conspiracy Theories about Infectious Diseases” in a post-hoc manner. Online publishing allows the addition of new papers to a published special issue, thereby permitting a special issue to grow.]
Keywords
As the success of the COVID-19 vaccination program in a country can have major health and economic consequences, it is important to understand the factors predicting people's attitudes towards COVID-19 vaccinations. Many studies have examined the socio-psychological predictors of the COVID-19 vaccination around the world (e.g., Butter et al., 2022; Mangla et al., 2021; Simione et al., 2021). During the first lockdown in April–May 2020, Pivetti and colleagues explored, via structural equation modelling (SEM), whether the acceptance of a COVID-19 vaccine, in two European countries, that is, Italy and Finland, was affected by confidence in science, general conspiracy beliefs and COVID-related conspiracy beliefs, and, only indirectly, by the role of political ideology and the endorsement of moral purity values (Pivetti et al., 2021a, 2021b). In the literature, COVID-related conspiracy beliefs were associated with reducing the intention to vaccinate against COVID-19 (e.g., Earnshaw et al., 2020; Howard & Davis, 2023), and in the US COVID-related conspiracy beliefs were the strongest predictors of COVID-19 vaccine hesitancy (Farhart et al., 2022).
As replicability is a cornerstone of the research endeavor in social psychology, an increased use of conceptual replications would improve the overall value of psychology research (Plucker & Makel, 2021). In the current study, we aimed to conceptually replicate in Turkey, a predominantly Muslim country, the studies by Pivetti et al. in Italy and Finland (2021a; 2021b) on the predictors of the attitudes towards the COVID-19 vaccination, which were organized in a comprehensive health model, with a specific focus on conspiracy beliefs. The purpose of a conceptual replication is to examine the theoretical soundness of a set of findings. Specifically, we aimed to improve the external validity of the original studies (Fabrigar et al., 2020; Stroebe & Strack, 2014; Troyer et al., 2019). We wanted to see whether we would obtain the same pattern of results in a non-Western and non-Christian country like Turkey.
Reviews have shown the lowest proportions of vaccine acceptance in Middle Eastern countries, with < 30% in Kuwait and Jordan, as compared with EU countries (Khalid et al., 2022; Sallam, 2021). The low vaccine acceptance in the Middle East was found to be related to widespread beliefs in conspiracies that negatively affected vaccination uptake (e.g., Al-Jayyousi et al., 2021). Besides affiliation to Christian religion (e.g., Corcoran et al., 2021), affiliation to Muslim religion was also significantly associated with vaccine hesitancy in low- and middle-income countries before (Cobos Muñoz et al., 2015) and during the COVID-19 pandemic (Kanozia & Arya, 2021).
Furthermore, we followed the path of replication with updates (Morrison et al., 2010) as part of the original studies were outdated. The Italian and Finnish studies were run in spring 2020, when a COVID-19 vaccine was not available and even hard to imagine. Currently, at least nine different types of COVID-vaccine are widely available in Western countries and much debate has been reported in the media and during everyday interactions about the safety and risks related to each of the existing vaccines (e.g., Melotti et al., 2022). According to the latest data from the European Centre for Disease Prevention and Control (ECDC, 2022), 66% of the European population had received two doses and 42.05% had received booster doses, as of August 1, 2022. Thus, individuals had the opportunity to form their own opinions and attitudes towards this specific vaccine, based on their own experiences and also on those of acquaintances, friends, and family members.
Turkey also differs from EU countries in terms of low vaccination rates, according to the available data. 1 Turkey shows similar patterns as EU countries in terms of the number of cases. However, it is not easy to say the same thing for the vaccination rates (ourworldindata.org; MHT, 2022). As of August 2022, 62.7% of all the Turkish population has received two doses of vaccine, compared to 73.2% of EU citizens. The rate of vaccination is still lower than many other EU countries (ourworldindata.org).
When looking at the Turkish government's policy towards the pandemic and the COVID-19 vaccine, Turkey has followed a nationalist policy both in terms of announcements of daily cases and the availability of the vaccines against COVID-19 since the beginning of the pandemic. During the first phase of the pandemic, the incumbent Turkish political authorities created a scientific board to get advice about the pandemic policies and they gave importance to the production of a national vaccine, TURKOVAC, as well as to the purchase of inactivated vaccines developed by China and Russia (Esen, 2021). In Turkey, the first vaccinations started in September 2020 with phase-3 studies of Sinovac (Chinese inactive Sars-Cov-2 vaccine). After the first part of the vaccine was delivered to the healthcare workers, many citizens showed hesitancy about the COVID-19 vaccines (Ikiisik et al., 2021). Later in May 2021, after having problems with China in terms of receiving the remaining vaccine doses, the Turkish Government underwrote an agreement with Pfizer/BioNTech for the procurement of 120 million doses of MRNA vaccines and promoted the national vaccination campaign in the summer of 2021 with the help of governmental officials (Esen, 2021).
In 2020, the vaccine hesitancy of Turkish people for the hypothetical-yet-anticipated COVID-19 vaccine was among the highest in Western countries, varying from very low (2–6% China) to very high (43%, Czech Republic, and 44%, Turkey) (Feleszko et al., 2021). Later on, when the vaccination policy was implemented in the country, a range of conspiracy theories emerged, such as Bill Gates taking control of vaccinated people by injecting microchips into their bodies, vaccines changing the structure of human DNA, or Pfizer BioNTech vaccine recipients being remotely controlled via a digital system (Arshad et al., 2021).
During our data collection, the average rate of daily confirmed cases in Turkey was 7.4%, and the average death rate was 0.3% for a population of 84 million people. From the start of vaccine administration till the end of our collection period, in Turkey 59.1% of all the population had received at least two doses of the COVID-19 vaccine. Despite the increased number of cases due to the dominant Delta variant during the summer and early autumn of 2021, vaccination campaigns accelerated all around the world, while both the pace and the daily number of vaccines administered decreased gradually from a million administrations to one hundred thousand during our data collection period in Turkey (Mathieu et al., 2021).
Model and hypothesis
Both Italian and Finnish studies shared the same instruments, hypothesis, and evaluation methods. The hypothesized relationships between variables were integrated in a serial multiple mediation model, explored via SEM. We will start by reporting the main findings common to the two studies, starting from the left side of the model, in order to proceed from the broader dimensions (e.g., political orientation and religiosity), to the more specific ones (e.g., attitudes toward COVID-19 vaccines) (see Figure 1). Then we will formulate our hypotheses relying on the findings confirmed by each of the two studies as well as on relevant literature on the impact of Muslim religion on study variables.

The Italian and Finnish models.
According to the Moral Foundations Theory (MFT; Graham et al., 2009), moral purity describes individuals’ concern for, and interest in, the control of impulses and desires (i.e., purity/sanctity moral foundations), which is connected to many conservative and religious moralities with an emphasis on group-binding loyalty (Di Battista et al., 2018, 2020; Graham & Haidt, 2012). Behaviors characterized by risks of pathogen transmission (e.g., in food preparation, hygiene, and sexual contact) are viewed with high moral condemnation when purity concerns are high. In the original model, moral purity negatively predicted confidence in science, in line with previous research (e.g., McCright et al., 2013; Rutjens et al., 2018). Generally, people with high levels of moral purity fear biological contamination and perceive the injection of disease antigens as a corruption of the body's integrity (e.g., Hornsey et al., 2018). Therefore, we predicted that moral purity would negatively predict confidence in science (H1).
As for political orientation, in both Italy and Finland, this predicted COVID-related conspiracy beliefs, with those on the right wing endorsing COVID-related conspiracy beliefs more than left-wingers. This result is partially in line with many studies showing that extreme political (left or right) orientations were associated with the endorsement of conspiracy beliefs (e.g., Krouwel et al., 2017). Across a large sample of respondents from 26 countries and two studies, Imhoff et al. (2022) found that respondents at the extreme ends of the political continuum expressed more pronounced beliefs that the world is governed by covert forces operating in the shadows. We thus predicted that right-wing political orientation would be positively associated with COVID-related conspiracy beliefs (H2).
Even if religiosity was not measured in the Italian and Finnish studies, there seems to be a connection between religiosity and COVID-related conspiracy beliefs in some countries (for a review, see van Mulukom et al., 2022). In a US sample, Republican partisanship, conservative ideology, and religiosity were each significant predictors of COVID-related conspiracy beliefs (Uscinski et al., 2020). Similarly, in a Polish sample, an increase in religious commitment during the pandemic was associated with increased conspiracy beliefs and possession of inaccurate or less knowledge about COVID-19 (Boguszewski et al., 2020). In a predominantly Muslim country such as Turkey, religiosity, right-wing ideology, and a lower level of cognitive reflection were associated with a higher level of belief in COVID-related conspiracy theories (Alper et al., 2021). Therefore, we predicted that religiosity would relate to general conspiracy beliefs (H3a) and to COVID-related conspiracy beliefs (H3b).
Religiosity was also negatively related to confidence in science in the USA (Johnson et al., 2015) and with confidence in scientific authorities in 52 countries (Chan, 2018). Therefore, we predicted that religiosity would be negatively related to confidence in science (H3c).
Confidence in science was associated with vaccine hesitancy (Jennings et al., 2021). Using representative survey data covering 126 countries, Sturgis and colleagues (2021) have shown that in countries where confidence in science is high, people are also more confident about vaccinations. In Italy, willingness to take the COVID-19 vaccine was correlated to trust in research and vaccines (Palamenghi et al., 2020). Also, more general conspiracy thinking and worldviews also contributed to science rejection, for example in the domains of vaccination and climate change (Rutjen & Većkalov, 2022). On these premises and on the results of previous studies, we predicted that confidence in science would relate positively to attitudes towards vaccines (H4a) and negatively to conspiracy beliefs (H4b).
Beliefs in conspiracy theories can be defined as beliefs in the presence of a “vast, insidious, preternaturally effective international conspiratorial network designed to perpetrate acts of a most fiendish character” (Hofstadter, 1966, p. 14). Conspiracy beliefs have been associated with both vaccination hesitancy and negative attitudes toward vaccinations (Hornsey et al., 2020; Tomljenovic et al., 2020). As conspiracy beliefs tend to be more prevalent in social crisis situations (van Prooijen & Douglas, 2017), COVID-related conspiracy beliefs proliferated in times of the COVID-19 pandemic (e.g., Sakki & Castrén, 2022; Tuzcu & Sahin, 2022). For instance, some people believe that the coronavirus is a bioweapon engineered by the Chinese government to wage war on America and Western countries (e.g., Farhart et al., 2022). COVID-related conspiracy beliefs were associated with a low intention to vaccinate against COVID-19 (e.g., Howard & Davis, 2023).
Turkey appears no different from any other country with respect to conspiracy theories about COVID-19. At the beginning of the outbreak, conspiracy theories about the origin of the virus and the existence of covert forces aiming to control the world via the pandemic were widespread (e.g., coronavirus is a bioweapon, the global elite has designed the virus to take control of the world; Erisen, 2022). Therefore, we predicted that conspiracy beliefs (H5a) and COVID-related conspiracy beliefs (H5b) would be associated with negative attitudes towards vaccines. Moreover, we predicted that conspiracy beliefs would be indirectly and positively associated with COVID-related conspiracy beliefs (H5c), as the latter developed from the former (Grimes, 2021).
As conspiracy beliefs frequently call into question the very institutions that can provide reliable information (Connolly et al., 2019; Rutjens et al., 2021), generic beliefs in conspiracy theories have been associated with distrust in government, health institutions, and healthcare systems during the COVID-19 pandemic in Germany (Bruder & Kunert, 2022). Belief in COVID-related conspiracy theories was associated with distrust in scientists and health organizations in multinational samples (De Coninck et al., 2021; Freeman et al., 2020; van Mulukom, 2022). Moreover, conspiracy beliefs were strongly related to distrust in information provided by the government (Pavela Banai et al., 2022; Soveri et al., 2021; Wirawan et al., 2021). Informational contamination was defined as the perception that information circulating in the media is biased and untrustworthy (Conway et al., 2020). Both in Italy and in Finland, COVID-related conspiracy beliefs were found to be negatively related to support for governmental restriction and positively related to perception of informational contamination. In line with these findings, we predicted that COVID-related conspiracy beliefs would be negatively associated with support for governmental restrictions (H6a) and positively associated with perception of informational contamination (H6b).
Finally, attitudes towards vaccines in general strongly predicted attitudes towards COVID-19 vaccine consistently both in Italy and Finland, suggesting the idea that attitudes toward the COVID-19 vaccine could be a specific case of the more general attitudes towards vaccine/vaccine hesitancy. In this perspective, the following hypothesis was put forward: attitudes toward vaccines in general would be positively related to attitudes toward COVID-19 vaccines (H7).
As for indirect effects, moral purity, political orientation, and religiosity were assumed to predict attitudes towards COVID-19 vaccines through the sequential mediation of confidence in science, conspiracy beliefs, COVID-related conspiracy beliefs, and attitudes towards vaccines, as shown in Figure 1.
Overall, we predicted that the fundamental structure of the model corroborated by Pivetti et al. (2021a, 2021b) would be confirmed in a Turkish non-Christian sample as well. The main novelties lie in the role played by religiosity as antecedent of confidence in science, (COVID-related) conspiracy beliefs, and, indirectly, attitudes towards (COVID-19) vaccines. Moreover, COVID-19 vaccines were widely available in 2021, at the time when the study was carried out, whereas they were not even countenanced during the Italian and Finnish data collection in 2020. In this sense, the Turkish participants may have had the opportunity to make up their mind and build a more specific attitude toward COVID-19 vaccines, as compared with studies carried out in the previous year.
Methods
Participants
Five-hundred seventy Turkish individuals aged from 18 to 67 (M = 26.69; SD = 7.45), mostly females (69.8%), took part in the study. The participants were recruited in 69 cities out of 81, including the Turkish capital, Ankara (n = 117). The Mid-Anatolian region had the highest number of participants with 40% among seven regions (n = 228). The participants were highly educated (96.1%), holding at least one undergraduate diploma (n = 250), and a graduate or a post-graduate degree (n = 298), and 45.3% were still enrolled in their degree programs (n = 258). Of all participants, 37.9% were either working full-time or part-time (n = 216), 13.7% were either unemployed or actively seeking a job (n = 78), while 3.1% were either on a leave, retired, or identified themselves as “housewives/househusbands.”
More than half of the participants defined themselves as “not religious” (n = 293) when asked. Among those who considered themselves “religious” (n = 277), 92.1% of them stated that they were Muslims (n = 255). As for political orientation, 33.2% positioned themselves on the left (n = 189), 12.3% stated that they were in center (n = 70), 13.5% on the right (n = 77), and the remaining 41.1% declared they were apolitical (n = 234).
As for the participants’ experience of COVID-19, 23.2% reported they caught the coronavirus at some point in the past. All the participants reported that the COVID-19 vaccine was available in their neighborhood. When they were offered it, 90.7% participants reported that they got the jab. Of those, 75.3% got vaccinated with Pfizer/Biontech and 11.4% with Sinovac, and the others with Coronavac and Moderna (missing = 9.3%).
As religiosity was not measured in the original studies, we ran some ANOVAs to preliminarily test the role of religiosity on the study variables. ANOVAs showed that religious people were more right wing (F (1, 355) = 16.28, p < .001, MReligious = 1.87, MNonReligious = 1.59), were less positive about COVID-19 vaccine (F(1, 569) = 4.72, p = .03, MReligious = 5.44, MNonReligious = 5.71), had less confidence in science (F(1, 569) = 46.26, p < .001, MReligious = 3.96, MNonReligious = 4.64), trusted media information less (F(1, 569) = 9.90; p = .002, MReligious = 4.57, MNonReligious = 5.08), and scored higher on moral purity (F(1, 569) = 13.55, p < .001, MReligious = 5.38, MNonReligious = 4.83), as compared with nonreligious people.
All the variables being studied were normally distributed. Descriptive statistics and bivariate correlations between the variables are reported in Table 1. On average participants scored quite high on moral purity and attitudes towards COVID-19 vaccines, and moderate on all the remaining variables (see Table 1).
Descriptives and Pearson's correlations among the variables

Note: for all variables n = 570; **p < .001; * p < .01.
Procedures
A self-report questionnaire was implemented using the Google Forms platform. Participants were recruited using a convenience sample strategy (Etikan et al., 2016) with the collaboration of two Turkish researchers, who sent the link of the questionnaire to the mailing lists of close (e.g., friends) and more distant acquaintances (e.g., colleagues). Also, snowball sampling was used. On average, the questionnaire took approximately 20 min to complete. After reading a description of the study, all the participants stated their willingness to participate in an informed consent form. A lottery incentive was used to increase the response rates in the survey. Specifically, we offered the opportunity to win 10 grocery store Migros Turkey/bookstore (D&R) coupons upon choice, approximately 50 Turkish Lira, to the participants who filled in the questionnaire properly.
We collected the data during the fourth wave of the COVID-19 in Turkey starting from when the increased numbers of infections due to the Delta variant were announced in mid-August till the beginning of the fifth wave, December 2021.
The research complied with the Ethics Code of the Italian Psychology Association (Associazione Italiana di Psicologia, 2015) and was conducted in accordance with the WMA-Declaration of Helsinki (1964/2013). Written informed consent was obtained by each participant. Approval was obtained from the Ethical Review Board for Research in Psychology, University of Bologna (IT), in April 2020 (protocol code #312669).
Measures
Participants completed a battery of items and measures mainly borrowed from the studies by Pivetti et al. (2021a, 2021b). We detail here when and why different measures than the original ones were used.
Attitudes towards the COVID-19 vaccine
As the COVID-19 vaccine was not available in Italy and Finland during 2020 data collection whereas it was available in Turkey during 2021 data collection, we had to reframe the items previously used in our studies that measured the intention to get vaccinated once the COVID-19 vaccine became available. Five items (three reverse scored) created ad hoc for this study measured specific attitudes toward COVID-19 vaccines (e.g., previously “I would not get the jab as the risks outweigh the benefits,” then “I did not get the jab as the risks outweigh the benefits”—reverse scored), on a 7-point Likert-type scale ranging from 1 (“strongly disagree”) to 7 (“strongly agree”). A composite score was obtained by averaging the five items (α = .81). Higher scores indicated more positive attitudes towards COVID-19 vaccines.
Attitudes towards Vaccines
We used the same scale as in the original studies. Ten items from the Short Version of Vaccine Acceptance Instrument (e.g., Sarathchandra et al., 2018) were translated and adapted into Turkish by the research team. Items 1–2 measured perceived safety of vaccines (e.g., “Vaccines are safe”); items 3–4 measured perceived effectiveness and necessity of vaccines (e.g., “Vaccines are effective at preventing diseases”); items 5–6 assessed the acceptance of the selection and scheduling of vaccines (e.g., “We give children too many vaccines”—reverse scored); items 7–8 assessed positive values and affect toward vaccines (e.g., “Vaccines are a major advancement for humanity”); and items 9–10 measured perceived legitimacy of authorities to require vaccinations (e.g., “The government should not force children to get vaccinated to attend school”—reverse scored). The response scale ranged from 1 (“strongly disagree”) to 7 (“strongly agree”), where higher values indicated more positive attitudes toward vaccines (α = .81).
Confidence in science
We used the same scale as in the original studies. Six items assessed participants’ beliefs and confidence in science (translated into Turkish and adapted by the research team, from Farias et al., 2013—e.g., “Science provides us with a better understanding of the universe than religion”). The response format was a 6-point Likert-type scale ranging from 1 (“strongly disagree”) to 6 (“strongly agree”), where higher values indicated more positive attitudes toward science (α = .85).
Conspiracy beliefs
Five items were administered to assess participants’ level of conspiracy beliefs. First, two original items measuring conspiracy theory beliefs were adapted by previous studies and translated into Turkish (ITANES, 2016; Mancosu et al., 2017; e.g., “Moon landings never happened, and the evidence was fabricated by NASA and the US government”). One more item was created ad hoc to the adapt to the Turkish culture (“In 1961, the incident regarding the first ever automobile designed and produced in Turkey named ‘the Revolution’ happened because other governments did not want us to be successful in producing cars and being a key player in the automotive sector”). Furthermore, two items from the original studies measuring conspiracy ideation (Lewandowsky et al., 2013) were adapted and translated into Turkish (e.g., “Lady Diana's death was not an accident but rather an organized assassination by members of the British royal family who disliked her”). The response format was a 11-point Likert scale ranging from 0 (“not plausible at all”) to 10 (“completely plausible”), where higher values indicated higher levels of conspiracy beliefs (α = .76).
COVID-related conspiracy beliefs
We used the same scale as in the original studies. Five items measured COVID-related conspiracy beliefs (e.g., “I think that coronavirus has been spread on purpose to eliminate from the population the weakest such as those elderly and those sick”). The response format was a 11-point Likert-type scale ranging from 0 (“not plausible at all”) to 10 (“completely plausible”), where higher values indicated higher levels of COVID-related conspiracy beliefs (α = .89).
Support for governmental restrictions
We used the same scale as in the original studies. Two questions measured the degree that participants supported the restrictions that their governments implemented to help stop the spread of the virus (social psychological measurements of COVID-19 restriction scale by Conway et al., 2020; “I support the government measures to restrict the citizens’ movement so as to curb the spread of the coronavirus”). The items were translated into Turkish and response format was a 7-point Likert scale ranging from 1 (“definitely disagree”) to 7 (“definitely agree”). Higher scores indicated stronger support for governmental restrictions (r = .50; p < .001).
Informational contamination
We used the same scale as in the original studies. We administered two items of the Informational Contamination subscale of the social psychological measurements of COVID-19 (Conway et al., 2020) assessing the extent to which participants felt that they distrusted the information received during pandemic (e.g., “I distrust the information I receive about the Coronavirus—COVID-19—from my government”). The items were translated into Turkish. The response format was a 7-point Likert scale ranging from 1 (“definitely disagree”) to 7 (“definitely agree”), where higher values indicated a higher level of distrust in information provided by the government (r = .70; p < .001).
Moral purity
Akin to the Finnish data, we measured moral purity foundations using three assessments of the moral judgment subscale of the Moral Foundation Questionnaire (MFQ; Graham et al., 2009; e.g., “People should not do things that are disgusting, even if no one gets hurt”; the Turkish translation is available on the moralfoundations.org spreadsheet). We choose not to use the Omission as a Compromise on Moral Foundations scale (OC-MF; Di Battista et al. 2020) used in the Italian study, as the Turkish validated translation was already available only for the MFQ, and not for the OC-MF. Participants rated morality items using a 7-point scale (from 1 = not at all; to 7 = very much), where higher values indicated a stronger endorsement of moral purity concerns (α = .80).
Political orientation
Akin to the original studies, participants were asked to indicate their political orientation on a 7-point Likert scale, where 1 stated a left-wing orientation and 7 a right-wing orientation, with the possibility to tick “apolitical orientation.” In the Italian and Finnish data collection, this option was not available. It was added to the Turkish data collection based on some feedback from Turkish participants during the pilot study. We recoded political orientation into three dichotomic dummy variables: left-wing ( = 1; no left-wing = 0), center ( = 1; no center = 0), and right-wing orientation ( = 1; no right-wing = 0). Zero on all three dummy variables thus indicates apolitical orientation.
Religiosity
Religiosity was not measured in the original studies. Participants were asked to report if they consider themselves religious (“As for religion, do you consider yourself as a religious person? yes/no”) and, if so, what was their religious orientation (“What is your religious belief/approach?”).
Experiences of COVID-19 and COVID-19 vaccines
In order to be able to describe the participants’ own experience of the COVID-19 disease and COVID-19 vaccine, we asked participants whether they had caught COVID-19 (e.g., “I caught coronavirus”; yes/no, ad hoc item), their vaccination status (i.e.,: “I got the jab / I did not get the jab”) and the type of vaccine that the vaccinated participants got.
Socio-demographic questions
In the first section of the questionnaire, participants self-reported their gender (1 = male; 2 = female; 3 = other; 4 = I don’t want to define my gender pronoun / I do not want to state the gender-related information), age, the city and region of residence in Turkey, level of education, and main occupation.
Data analyses
We used the Statistical Package for the Social Sciences (IBM SPSS and AMOS 25.0) to run descriptive, reliability, and correlational analyses. To test the hypothesized serial mediational model, we used structural equation modelling with composite scores as measured variables (EQS 6.4; Bentler, 2008). An inspection of Mardia's (1970) coefficients suggested significant deviations from multivariate normality. To reduce the impact of non-normality, Satorra and Bentler's (2001) scaled estimates were relied on to rescale the standard errors and the chi-square statistics into the Satorra–Bentler scaled chi square (S–B χ2) statistic. Fit indexes such as the comparative fit index (CFI; Bentler, 1990), the root-mean-square error of approximation (RMSEA; Bentler, 2008), and the Akaike information criterion (AIC; Akaike, 1987) were also adjusted for non-normality by incorporating the S-B χ2 into their calculations. In this article, these were referred to as robust estimates (i.e., R-CFI, R-RMSEA, R-AIC).
The hypothesized mediational model was estimated and progressively improved by examining the Lagrange Multiplier Test, which assesses whether the addition of certain paths or parameters not present in the original model would result in a significant increase in model fit (Bentler, 1986). The statistical significance of indirect (or mediational) effects was tested via EQS in which the Sobel method (1987) was implemented.
Results
The hypothesized serial mediational model specified in Figure 2 provided an inadequate fit to the data (S-Bχ2 (41) = 291-113, p = .000; R-CFI = .774; R-RMSEA = .123; R-AIC = 309.113). However, the Lagrange Multiplier Test indicated that the model fit could be significantly improved by adding the following eight paths: the three paths linking moral purity to support for government restrictions, conspiracy beliefs, and COVID-related conspiracy beliefs; the two paths linking left and center political orientation to confidence in science; the two paths linking left political orientation and religiosity to informational contamination; and the path from support for government restrictions to attitudes towards vaccines. Three of these eight paths already had significant results in one of the two previously tested models. Specifically, the moral purity → COVID-related conspiracy beliefs, and the political orientation → informational contamination paths were significant in the Finnish dataset, while the support for government restrictions → attitudes toward vaccines path was significant in the Italian dataset. The resulting model accounted for a significant amount of variance in attitudes towards COVID-19 vaccines (R2 = .54) and provided a good fit to the data (S-Bχ2 (33) = 111.229, p = .000; R-CFI = .948; R-RMSEA = .065; R-AIC = 45.299; see Figure 3).
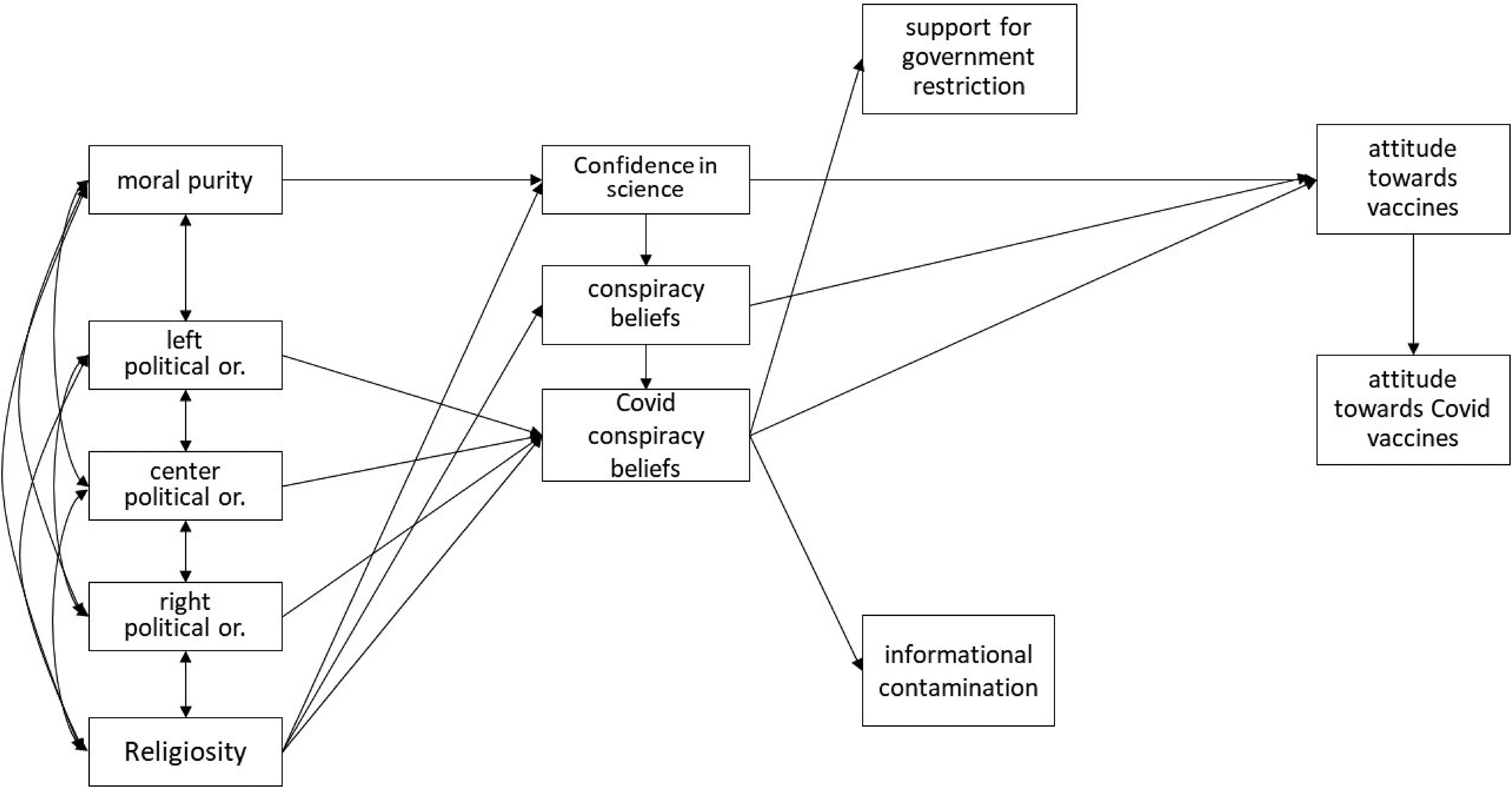
Hypothesized model.

The final model.
Direct, indirect, and total effects for the final model are reported in Table 2. Contrary to our assumption, moral purity directly and positively predicted support for government restrictions (β = .24), conspiracy beliefs (β = .35), and COVID-related conspiracy beliefs (β = .20), but not confidence in science (H1): those who endorsed moral purity were more supportive of strong governmental restrictions to control the pandemic and shared generic and COVID-related conspiracy beliefs. Left and center political orientation positively predicted not only COVID-related conspiracy beliefs (βs = −.10 and −.07, respectively) (supporting H2), but also confidence in science (βs = .24 and .09), with more left-wing or center participants endorsing less COVID-related conspiracy beliefs and having more confidence in science. Religiosity was negatively related to confidence in science (β = −.26) (supporting H3c), and informational contamination (β = −.10), but not to general or COVID-related conspiracy beliefs (not supporting H3a and H3b), with religious participants having less confidence in science and perceiving the media information as less contaminated than nonreligious participants.
Significant direct, indirect, and total effects in the final model

Note: Values reported refer to standardized effects significant at p < .05. D = direct effects, I = indirect effects, T = total effects.
Confidence in science and COVID-related conspiracy beliefs, but not generic conspiracy beliefs, predicted general attitudes towards vaccines (βs = .34 and −.38), with those having more confidence in science and endorsing less COVID-related conspiracy beliefs having more positive attitudes towards vaccines in general (supporting H4a and H5b, but not H5a). Contrary to our expectations, confidence in science did not predict conspiracy beliefs (not supporting H4b). Conspiracy beliefs predicted COVID-related conspiracy beliefs (β = .53) with those endorsing more conspiracy theories, also endorsing more COVID-related conspiracy beliefs (supporting H5c).
COVID-related conspiracy beliefs negatively predicted support for governmental restrictions and positively informational contamination (βs = −.18 and .30), with those endorsing more COVID-related conspiracy theories also being less supportive of governmental restrictions and more convinced that the information circulating in the media are not trustworthy (supporting H6a and H6b).
Support for government restrictions was related to attitudes towards vaccines in general (β = .23), but informational contamination was not: those more in favor of strong governmental restrictions had more positive attitudes toward vaccines in general. Finally, attitudes towards vaccines were strongly and positively related to attitudes towards COVID-19 vaccines in particular (β = .74) (supporting H7).
Besides the above direct effects, many indirect effects were found (see Table 2). Specifically, moral purity was related to attitudes toward vaccines mainly via support for government restriction (β = .06), COVID-related conspiracy belief (β = −.08) and the serial mediation of generic conspiracy beliefs and COVID-related conspiracy beliefs (β = −.07). Those who endorsed more moral purity values were more supportive of governmental restrictions and endorsed more generic and COVID-related conspiracy beliefs. In turn, support for government restrictions was related to having more positive attitudes towards vaccines, whereas generic and COVID-related conspiracy beliefs were related to having more negative attitudes towards vaccines. Hence, for moral purity we found indirect effects of the opposite kind, a phenomenon known as inconsistent mediation, although the overall impact of moral purity on attitudes toward vaccines was negative (β = −.11). Also, left-wing and center political orientation were positively related to attitudes toward vaccines via confidence in science (β = .08 and .03) and COVID-related conspiracy beliefs (β = .04 and .03), with left-wing and center participants trusting science more and endorsing COVID-related conspiracy beliefs less, which in turn was related to having more positive attitudes toward vaccines in general. Moreover, religiosity predicted attitudes towards vaccines via confidence in science (β = −.08): compared to nonreligious participants, religious ones trusted science less and in turn had more negative attitudes towards vaccines in general. Generic conspiracy beliefs were related to attitudes toward vaccines mainly via COVID-related conspiracy beliefs (β = .20): the more participants endorsed generic conspiracy beliefs, the more they endorsed conspiracy beliefs related to COVID-19, which in turn predicted more negative attitudes toward vaccines in general. Finally, attitudes towards vaccines in general strongly predicted attitudes towards COVID-19 vaccines (β = .74), thereby mediating the direct and indirect effects of other variables investigated (see Figure 2 and Table 2). Among the variables investigated, the ones that resulted overall more strongly indirectly linked to attitudes toward COVID-19 vaccines were COVID-related conspiracy beliefs (β = −.31), confidence in science (β = .25), generic conspiracy beliefs (β = −.21), and support for government-imposed restrictions (β = .17). Significant, albeit weaker, indirect effects were also found for left-wing and center political orientation (β = .09 and .05, respectively), moral purity (β = −.08), and religiosity (β = −.06).
Discussion
In this study, we provided a conceptual replication in Turkey, a predominantly Muslim country, of a comprehensive health model predicting the attitudes towards COVID-19 vaccinations (Pivetti et al. 2021a; 2021b). While the original studies run in the EU investigated only the intention to get vaccinated once the COVID-19 vaccine became available, we now investigated whether the relationship between study variables would hold also when COVID-19 vaccine was widely accessible, as was the case in the winter of 2021. The proposed model was also found to hold in Turkey and when the COVID-19 vaccine had become widely available, improving the external validity of the original model.
In summary, consistently across Italy, Finland, and Turkey, we found that political orientation predicted COVID-related conspiracy beliefs (β = .09, .15, and −.10/−.07 2 , respectively), which in turn negatively predicted support for governmental restriction (β = −.35, −.14, and −.18) and attitudes towards the vaccines (β = −.29, −.31, and −.39) and positively informational contamination (β = .53, .30, and .30). Moreover, confidence in science predicted attitudes towards the vaccines (β = .23, .20, and .34), which in turn predicted attitudes toward the COVID-vaccine (β = .75, .56, and .74). Finally, moral purity predicted attitudes towards the vaccines (which, in turn, predicted attitudes towards the COVID-vaccine) only indirectly through mediating paths, which changed from one country to another. Reading from the left to the right of the model, political orientation predicted COVID-related conspiracy beliefs, with left-wing and center participants endorsing COVID-related conspiracy beliefs less. This result is in line with original studies and with a 26-country study showing support for consistent relations between political orientation and the propensity to believe in conspiracies. Respondents at the extreme ends of the political continuum expressed more pronounced beliefs that the world is governed by covert forces operating in the shadows (Imhoff et al., 2022). However, our study shows that in Turkey only being left-(and not right-)wing was associated with conspiracy beliefs.
In turn, endorsing COVID-related conspiracy beliefs predicted believing that the information shared on media was not trustworthy and predicted lower support for government restrictions in times of COVID, in line with the original model validated in Italy and Finland. However, mixed results are found in literature, with positive relations between COVID-related conspiracy beliefs and trust in mainstream media in the US and UK (e.g., Earnshaw et al., 2020; Xiao et al., 2021). Also, we have found that people who endorse more COVID-related conspiracy beliefs did not trust formal institutions to handle the pandemic, in line with many previous findings (e.g., Pellegrini et al., 2021; Šrol et al., 2021). This is to be expected given the nature of conspiracy beliefs, which are often based on distrust in the actions of the government, scientists, and other authorities. It should be mentioned that trust in media and institutions are considered sometimes as antecedents (e.g., Stojanov & Douglas, 2022) and sometimes as consequences of conspiracy beliefs, as is the case in our model. Further longitudinal studies are needed to clarify the direction of this relationship.
Confidence in science was related to a positive attitude towards vaccines in general, whereas COVID-related conspiracy beliefs were related to negative attitudes toward vaccines, both directly and indirectly, in line with the original model. In previous studies, confidence in science played a crucial role in predicting COVID-19 vaccination intention, for instance in Italy (Barattucci et al., 2022), Germany (Seddig et al., 2022), and in the USA (Huang & Green, 2022). The association between COVID-related conspiracy beliefs and vaccination hesitancy was consistently found across many studies in different countries (e.g., Bacon & Taylor, 2021; Đorđević et al., 2021; Sallam, 2021). In a meta-analysis, conspiracy beliefs were found to explain lower vaccination and social distancing responses (Bierwiaczonek et al., 2022).
Attitudes toward vaccine were strongly related to attitudes towards the COVID-19 vaccine, pointing to a single dimension on attitudes towards vaccines, the COVID-19 vaccine being only a specific case. The same result was found in the original studies. Those data consistently suggest the existence of a broader attitude toward vaccinations, which includes COVID-19 vaccination. For instance, Soares et al. (2021) found that being unwilling to take the “flu vaccine was associated with both refusal and delays in COVID-19 vaccine uptake.”
When it comes to indirect predictors of attitudes toward COVID-19 vaccines, COVID-related conspiracy beliefs and conspiracy beliefs were negative indirect predictors, whereas confidence in science and support for governmental restrictions were positive indirect predictors. This result is in line with a Turkish study showing that belief in the artificial origin of COVID-19 was related to vaccine hesitancy (Salali & Uysal, 2022). Conspiracy beliefs and confidence in science were found to strongly predict attitudes towards COVID-19 vaccines also in the Finnish sample, whereas COVID-related conspiracy beliefs indirectly predicted attitudes towards COVID-19 vaccines via attitudes toward vaccines, in the Italian sample.
As compared with original study, one novelty lies in the role of religion as antecedents of confidence in science and (COVID-related) conspiracy beliefs. We found that religious people have less confidence in science (for a review, see Chan, 2018) and trust the information circulating on the media less, as compared with nonreligious people. Previous work has found that Muslims, Protestants, and Catholics nurture less trust in scientific authority (McPhetres & Zuckerman, 2018). However, religiosity was not associated with COVID-related conspiracy beliefs. This is in contrast with previous studies showing that in Turkey, religiosity was related to higher levels of belief in COVID-related conspiracy theories (Alper et al., 2021). Further studies are needed to clarify this relationship.
As found in the Finnish (but not in the Italian) study, moral purity predicted COVID-related conspiracy beliefs. Along the same line, previous work has found that the moral foundations that related positively to conspiracy beliefs were those of the binding kind (as moral purity is), pertaining to group—and community—concerns, and not those of individualizing moral foundations pertaining to individual well-being (Leone et al., 2019).
Moreover, a novel result not found in the previous studies should be mentioned here: the positive relation between moral purity and support for governmental restrictions. As binding moral foundations (i.e., authority/respect, in-group/loyalty, and purity/sanctity) link the individual to the values and norms of the group in order to foster the group's well-being, we speculate that individuals endorsing higher moral purity values would also be more sensitive to the protection of the group in terms of the implementation of the strong restrictive governmental measures, to slow down the spread of the pandemic. Also, moral purity indirectly predicted attitudes towards the vaccine with the mediation of COVID-related conspiracy beliefs and support for governmental restrictions.
As found in the Italian study (but not in the Finnish one), support for governmental restrictions was related to attitudes towards vaccines with those supporting the government's policies being more in favor of vaccines. As vaccination campaigns are promoted by the state, it is likely that trust in government would translate into a positive attitude towards COVID-19 vaccination, via the indirect mediation of attitudes towards vaccination. Similarly, in a longitudinal UK study, mistrust of government and pharmaceutical companies and dislike of coercive policies were found to be specific barriers to COVID-19 vaccine uptake (Phillips et al., 2022).
The positive association between left-wing political orientation and informational contamination is a novel result that should be mentioned. Given the conservative and populist orientation of the current Turkish Government, we speculate that left-wingers would be suspicious of the media news coming from the conservative government as a consequence of an ingroup-outgroup effect, with outgroup members usually viewed with suspicion and expected to discriminate against the ingroup (e.g., Tajfel, 1982; Moy & Ng, 1996).
Study limitations
First, the cross-sectional nature of our study does not allow us to draw causal inferences from the data. Second, the generalizability of the results is limited by the convenient nature of the sample. For instance, our sample was slightly more educated and more willing to get vaccinated than the average Turkish population. In our sample, approximately 91% indicated they got the jab when they were offered as compared with 60% of vaccinated people in the general population. Since level of education and attitudes towards science are related (e.g., Bak, 2001), it is possible that our sample being more educated than the average population has resulted in more positive attitudes towards science and less hesitancy about COVID-19 vaccination. However, we did not aim to conduct a prevalence study focusing on vaccine hesitancy in terms of actual acceptance of the COVID-19 vaccine. We aimed to test whether the same pattern of results found in Italy and Finland would hold also in a non-Western and non-Christian country such as Turkey. Third, as we collected data only via online questionnaires, it is possible that the participants were self-selected, with older citizens and/or those less familiar with social media not filling in the questionnaire.
The construct of general conspiracy beliefs seems problematic as it was not predicted by confidence in science, nor was it related to attitudes towards vaccines, as expected based on the results of the original studies. It is possible that the contents of the specific items, borrowed from the Italian and Finnish studies, did not resonate with the Turkish people, leading to a problem of construct validity for this dimension in the Turkish context.
Implications and conclusions
The predictive health model already validated in two EU countries was found to hold also in a Middle Eastern predominantly Muslim country, such as Turkey. As conspiracy beliefs and suspicion in institutions undermines institutions’ function of regulating social relationships, institutional distrust and conspiracy beliefs could erode the fabric of society by reducing trust between strangers and prosocial behavior, and increasing prejudice and intergroup conflict (van Prooijen et al., 2022).
Even if COVID-19 vaccines continue to be developed and improved, providing information alone does not change vaccination uptake intention (Kerr et al., 2021). Our study suggests that debunking conspiracy beliefs and building trust in science and institutions would provide leverage to increase vaccine intention, as booster doses against new variants are more likely every day.
As conspiracy beliefs have been defined as attempts to explain the ultimate causes of significant social and political events with secret plots orchestrated by powerful and malevolent actors (Douglas et al. 2019), it is likely that those beliefs are associated with mistrust towards legitimate authorities (Freed et al., 2011; Swami et al., 2011). Consequently, public campaigns addressing trust in authorities and debunking conspiracy beliefs must proceed hand in hand / pari passu. For instance, information campaigns based on information about the vaccine's approval process and about the strong economic impact of the pandemic were found to be effective in increasing the vaccination rate in an experimental US study (Diament et al., 2022).
Supplemental Material
sj-sav-1-pac-10.1177_18344909231170097 - Supplemental material for COVID-19 conspiracy beliefs and vaccinations: A conceptual replication study in Turkey
Supplemental material, sj-sav-1-pac-10.1177_18344909231170097 for COVID-19 conspiracy beliefs and vaccinations: A conceptual replication study in Turkey by Monica Pivetti, Francesca-Giorgia Paleari, Irem Ertan, Silvia Di Battista and Esra Ulukök in Journal of Pacific Rim Psychology
Supplemental Material
sj-sav-2-pac-10.1177_18344909231170097 - Supplemental material for COVID-19 conspiracy beliefs and vaccinations: A conceptual replication study in Turkey
Supplemental material, sj-sav-2-pac-10.1177_18344909231170097 for COVID-19 conspiracy beliefs and vaccinations: A conceptual replication study in Turkey by Monica Pivetti, Francesca-Giorgia Paleari, Irem Ertan, Silvia Di Battista and Esra Ulukök in Journal of Pacific Rim Psychology
Footnotes
Data availability statement
Raw data and SEM dataset have been uploaded as supplementary material.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article
Supplemental material
Supplemental material for this article is available online.
Correction (July 2023):
The article category has been updated.
Notes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.