
Abstract
This article uses a geopolitical lens to assess the EU’s response to COVID-19 by exploring the Commission’s creation of an emergency medical stockpile, dubbed rescEU. The article describes the creation, financing and distribution of this stockpile, which comes under the aegis of the Civil Protection Mechanism, in its first year of operation, 2020–1. What the analysis shows is how the creation and distribution of medical assistance was justified by the need to adapt to a changing international environment, one in which Russia and China contested the EU’s solidarity, both within the EU27 and towards its neighbours. The EU has committed to investing large sums to develop pandemic resilience via stockpiling. However, what remains to be seen is how far such a policy can strengthen solidarity and counteract anti-EU narratives in the global context of the increasing strategic competition facing the EU.
Introduction
The EU response to COVID-19 took many forms, from a stimulus package to finance economic recovery to institutional reform to create an agency to enhance preparedness for future health emergencies. These measures have been framed as an attempt to carry out a further ‘rescue of the nation state in Europe’ (Brooks et al. 2021, 235) in a nod to how integration set the foundations for post-war economic reconstruction. One particularly striking aspect of the EU’s response was the move to increase pandemic resilience by promoting the stockpiling of medical countermeasures, notably personal protective equipment (PPE). However, as this article demonstrates, the rescEU stockpile, nested under the aegis of the Civil Protection Mechanism (CPM), is a public health tool created within a broader geopolitical setting, one Josep Borrell (2020) has called ‘a battle of narratives’.
The European Commission faced a complex policy dilemma when it sought to extend its competences into the domain of public health. The EU justified the need for such policies on the basis of output legitimacy: collective action would achieve results that were better than those any single member state could hope to accomplish by acting independently in conditions of interdependence (Majone 2005). This justification was particularly apt given the need to protect the interests of the smaller member states, which have limited purchasing power for medical countermeasures. The desire to build up a stockpile of PPE to mitigate the effects of the pandemic and build resilience for future health emergencies was thus linked to polity legitimacy (Ferrera et al. 2021), which had been suffering from a decade of crises.
The article proceeds by first explaining how EU medical assistance in the period 2020–1 was loaded with geopolitical considerations, because access to medical aid—both within the EU and in its immediate neighbourhood—formed part of the EU’s strategic competition with Russia and China. Second, it describes the development of the rescEU programme and how EU stockpiling is financed and organised. Third and finally, data on the distribution of Civil Protection and rescEU stockpiles is analysed to show how these resources were distributed within the EU and amongst third countries. This demonstrates how Brussels’ stockpiling policy was linked to the need to counteract Chinese and Russian attempts to demonstrate that they were more reliable partners than the EU. In this sense, the move towards stockpiling as an EU policy for developing pandemic resilience is indicative of the changing international order that has obliged the EU to rethink its global role.
The geopolitical setting of EU medical assistance during the pandemic
The EU’s response to COVID-19 took place within a setting that was from the start considered a public health emergency. The European Centre for Disease Prevention and Control informed the Commission on 7 January 2020 about the presence of a new type of viral pneumonia in Wuhan, China. Two days later, the Commission, acting on a threat assessment from the Centre, posted the first notification of this virus on the Early Warning and Response System. Not long after, on 17 January, the Health Security Committee, comprised of national public health representatives and ministries, met to discuss the pandemic threat for the first time (Kyriakides 2020). Consequently, the EU was swift to frame the risk as that of a serious cross-border threat to health, which would require a common approach as far as possible. This approach went hand in glove with that of the World Health Organization, which on 30 January 2020 declared the COVID-19 outbreak a public health emergency of international concern, before raising the stakes by defining it as a pandemic on 11 March 2020 (Davies and Wenham 2020: 1230–1).
An early intervention by the French and German governments explicitly framed the pandemic not just as a health emergency, but also as a geopolitical challenge that required a ‘new European approach based on strategic health sovereignty’ (France, Ministry for Europe 2020). In a situation of squeezed supply chains and an anticipated race to find a vaccine, the goal promoted by these two EU heavyweights was ‘to reduce EU dependency’ (France, Ministry for Europe 2020) when dealing with health shocks. Even more explicitly, the EU High Representative for Foreign Affairs and Security Policy, Josep Borrell, warned that the pandemic was accompanied by ‘a geo-political component including a struggle for influence through spinning and the “politics of generosity”’ (Borrell 2020).
He singled out Russia and China as active agents in a battle of narratives that at this point in time sought to challenge the EU on its own turf by contesting the existence of European solidarity during the crisis. Both countries did so by putting on a highly politicised and performative show of medical assistance, especially towards Italy and Serbia. These two countries became enmeshed in a diplomatic tussle over the provenance of medical aid and other forms of support. The EU’s decision in mid-March 2020 to impose export restrictions on certain kinds of PPE, which initially affected Serbia even though it is an EU candidate country, was a public-relations disaster that allowed China to showcase its generosity. The European Commission was obliged to respond by removing Serbia from export restrictions and providing a substantial new aid package to support public health in the country (Ruge and Oertel 2020).
For its part, China organised significant shipments of PPE—at a time of exceptional global demand—to help Italian medical staff, using both governmental channels and private actors such as Huawei. This action again contrasted with the initial response of some EU countries, notably France and Germany, to impose national export bans on PPE and other medical equipment. Another feature of the Chinese assistance (which, unlike Russia’s, was not free of charge) was a concerted media campaign fostered by the Chinese embassy in Rome to showcase Italian gratitude. The Chinese authorities sought to highlight the EU’s inaction; as Small (2020, 51) writes, ‘it was not enough to argue that the Chinese Communist Party had succeeded; others had to be seen to fail’. EU leaders were caught off guard by the Chinese public-relations messaging that accompanied Beijing’s medical assistance. Indeed, the European Commission tried to counteract this narrative by highlighting the 56 tons of medical assistance that the EU had provided on the quiet to China in February 2020 via the CPM (Small 2020, 6).
The EU to the rescEU?
The EU’s pandemic stockpiling strategy to assist member states, announced in March 2020, was established under the aegis of the EU’s CPM. The latter dates from 2001 and is designed to coordinate the pooling and deployment of civil protection resources—drawing on EU funding—to provide emergency relief within and outside Europe. What constitutes such an emergency is broadly defined. In 2007, the Council of the EU (2007, 10) clarified that the mechanism exists to help protect ‘people but also the environment and property, including cultural heritage, in the event of natural and man-made disasters, acts of terrorism and, technological, radiological or environmental accidents, including accidental marine pollution, occurring inside or outside the Community’. The wide scope of this definition reflects the difficulties faced in finding a consensus among the member states about what kinds of civil emergencies to prioritise (Bremberg and Britz 2009). In 2019, the CPM was revised to better align with the EU priority of responding to climate change. Thus was born the ‘rescEU’ stockpile, consisting of a pooled reserve of member state resources for disaster management, notably a fleet of aircraft for fighting forest fires.
Stockpiling itself is an ancient technique of governance based on anticipatory knowledge; it can also be decentralised and delegated to private firms or citizens (Folkers 2019). Many countries stockpile resources such as oil, gas, industrial products and foodstuffs as a way to manage temporary supply disruptions or spikes in prices. Medical stockpiles, once a feature of Cold War nuclear contingency planning, gained new relevance at the turn of the twenty-first century as the 2001 US anthrax attacks, as well as the emergence of SARS (severe acute respiratory syndrome) and both avian and swine flu, reminded policymakers of the need for spare capacity to provide resilience in the face of an emergency. In fact, the very concept of ‘health security’ came to the fore in this period, as evidenced by the establishment of the EU Health Security Committee, which was first constituted as an informal committee after the 2001 anthrax attacks (Elbe et al. 2014, 443).
The H5N1 avian flu outbreak in 2005 caused a flurry of stockpiling activity across EU member states, but without centralised coordination. National governments sought to secure vast supplies of anti-viral medicine as part of pandemic preparedness measures designed to protect front-line health workers and prevent health systems from becoming overwhelmed (Elbe et al. 2014). By the time COVID-19 struck, countries such as the US, Canada, Australia, France and the UK already had experience of amassing pharmaceutical and PPE stockpiles. The EU’s decision to follow suit was prompted by Italy’s request for PPE in February 2020, when its own stocks were extremely low—which was why aid from Russia and China garnered so much attention at the time. However, the CPM was ill-prepared for this request and so the Commission urgently revised the rescEU regulation to allow for the purchase and distribution of PPE and associated medical countermeasures. This was justified on the basis of ‘taking action to get more equipment to member states’, which Commission President von der Leyen presented as ‘EU solidarity in action’, because ‘helping one another is the only way forward’ (European Commission 2020a).
From an initial budget of €50 million, the Commission successfully argued for a huge increase in funding for rescEU as part of the 2021–7 multiannual financial framework, leading to an allocation of €1.1 billion, which will be supplemented by €1.9 billion from NextGenerationEU funds (European Council 2020). Commissioner for Crisis Management Janez Lenarčič announced this increased financing by explaining that ‘When the coronavirus hit Europe, there was a lack of many kinds of medical equipment across Member States. Yet the EU did not have the power or the means to offer equipment; we could only encourage cooperation. Citizens expect the EU to act during a crisis. We all need to be better prepared and learn the lessons. rescEU will be massively strengthened to leave no EU country behind during a crisis’ (European Commission 2020b).
The stockpile, for which the Commission pays 100% of the availability, deployability and operational costs to mitigate what the Implementing Decision (European Commission 2021b, 36) calls ‘low probability risks with a high impact’, co-exists alongside the CPM. That is, the former is invoked in exceptional circumstances when the latter is insufficient to provide adequate assistance. Hence the stockpile is designed as a measure of last resort, for when national capacities are overwhelmed. It is also intended to provide lasting capacity beyond the immediate exigencies of the current pandemic. For instance the German-based rescEU stockpile of PPE has been contracted to operate until the end of 2027, with a mandate to make stocks available for transport within 12 hours of notification. As of June 2021, nine member states had offered to host rescEU stockpiles and thereby assume logistical responsibility for procurement: Belgium, Denmark, Germany, Greece, Hungary, Romania, Slovenia, Sweden and the Netherlands (European Commission 2021a).
Distributing EU resources
Nine member states received emergency assistance from the EU in the first year of the rescEU scheme’s operation (March 2020 to March 2021). Italy benefited from support on 6 of the 22 occasions when the CPM, notably in the form of teams of doctors or other emergency responders, or rescEU was activated to supply a country in need. Croatia and Slovakia received aid on four occasions, while Bulgaria, Czechia, France, Ireland, Lithuania and Spain received assistance three times or fewer (see Table 1). At the same time, the CPM and the rescEU stockpile also distributed medical countermeasures to a range of non-EU countries. In the period from April 2020 to April 2021, these mechanisms were used 37 times to distribute PPE, hand sanitiser, ventilators and ambulances, or to send medical teams to 12 countries (as well as Dutch and French Caribbean islands). The largest beneficiaries of this COVID-19 assistance, in terms of the number of separate deliveries, were Montenegro (19), North Macedonia and Serbia (10 each), and Moldova (7). The remaining recipients, which included Ukraine, Kosovo, Georgia and Bosnia received fewer than five deliveries each (see Table 2).
Intra-EU emergency assistance, March 2020–March 2021.
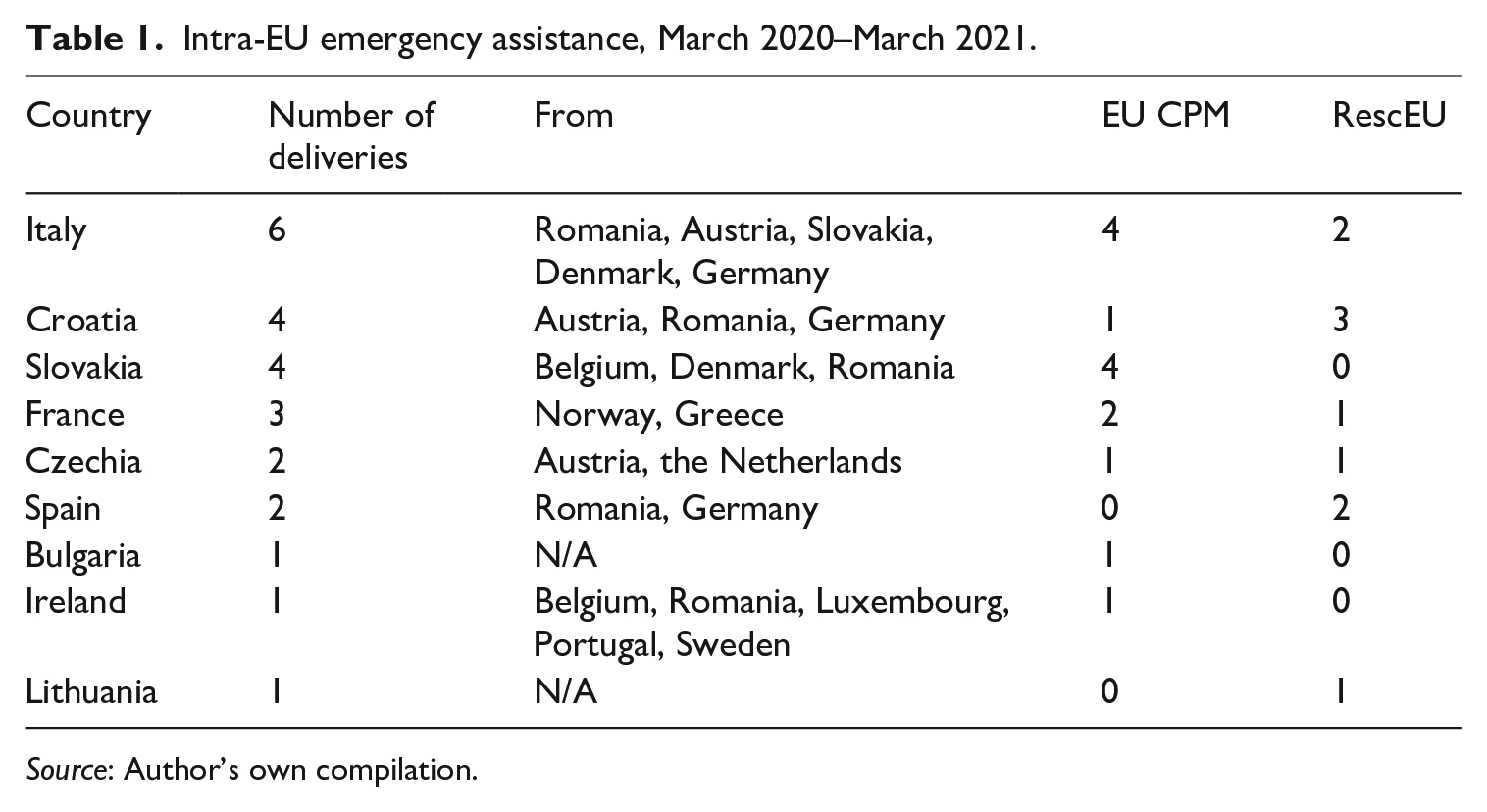
Source: Author’s own compilation.
Emergency assistance outside the EU, March 2020–March 2021.
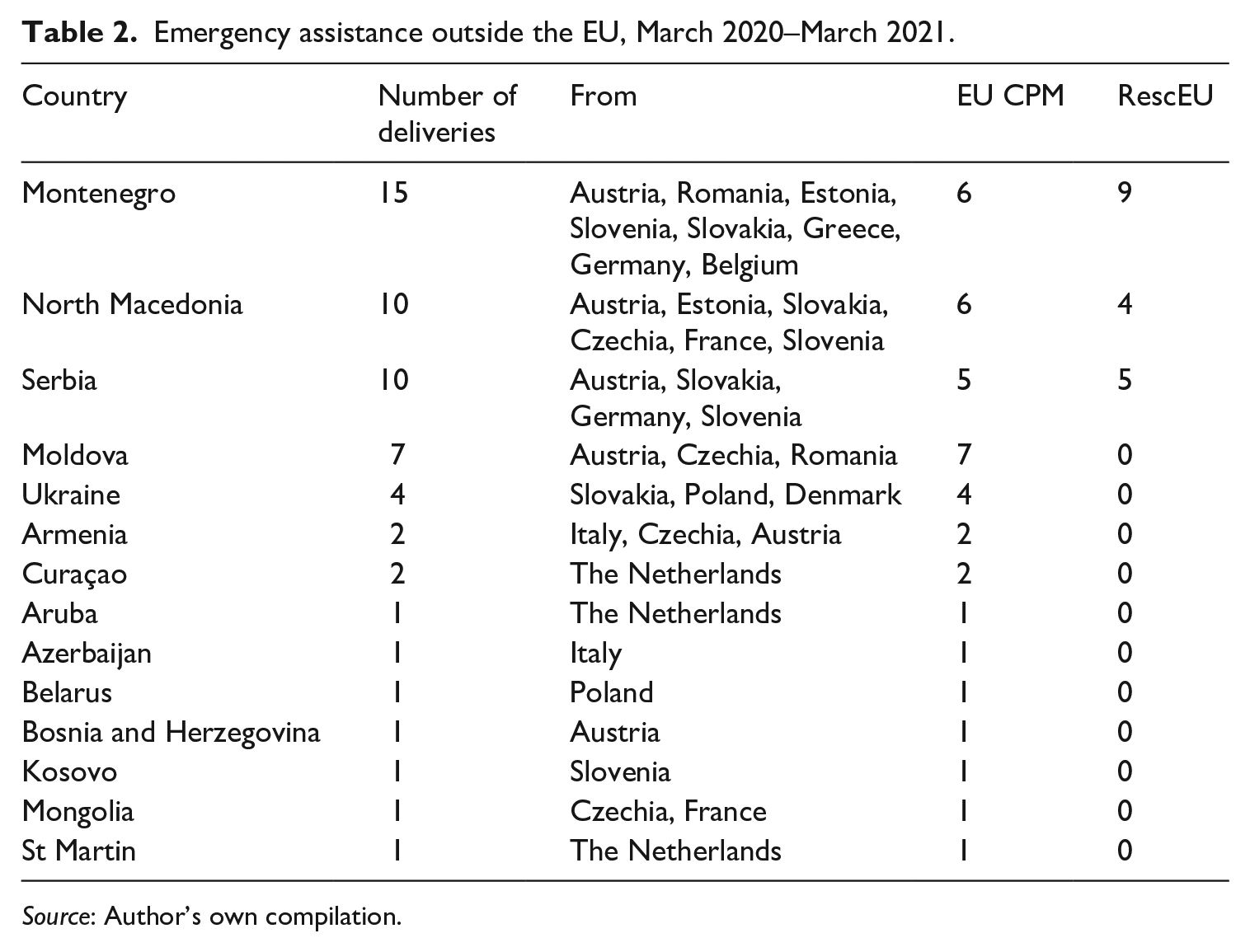
Source: Author’s own compilation.
The nature of the distribution of EU emergency assistance demonstrates Brussels’ geopolitical understanding of the pandemic. Within the EU, it was Italy that benefited most, reflecting the fact that it was not just on the front line of the pandemic but was also a test case for demonstrating intra-European solidarity to counter Russian and Chinese narratives to the contrary. Outside the EU, the pressure on Brussels to fulfil its promises of support were felt particularly acutely in the Balkans, where again Russia and China sought to sow division. Indeed, the European Parliament was so concerned about the instrumentalisation of Russian and Chinese medical support in Serbia that in its March 2021 country report it asked the Commission and the member states to ensure sufficient vaccine supplies for the entire Western Balkans (European Parliament 2021). The Parliament explicitly noted that Serbia was a battleground for COVID-19 geopolitical narratives, stating that it ‘deplores the disinformation campaign concerning EU assistance during the pandemic by government officials’ (European Parliament 2021, 11). Hence it is no coincidence that the vast majority of non-EU assistance via the EU CPM went to the Western Balkans, the countries of which were also the only recipients of aid via the rescEU stockpile.
Conclusion
The above analysis has demonstrated that the developments in the field of pandemic resilience and solidarity are best situated within a geopolitical understanding of contemporary EU policymaking. By assuming the mantle of protector of European health during the pandemic, the Commission made itself dependent on securing support through policy results. However, an essential part of the debate over polity legitimacy was the need to engage in a ‘battle of narratives’ with those who downplayed EU solidarity in a time of need. The distribution of EU assistance via the CPM and the new rescEU stockpile hence seems to have taken into account the way particular countries, such as Italy and Serbia, became spaces of contestation over the extent of EU pandemic support. Looking to the future, the questions will be whether this trend continues, as stockpiling is set to play a central role in EU health security, and how far the provision of medical countermeasures aligns with the goal of strategic autonomy. After all, procurement from outside the EU remains the mainstay for supplying PPE (European Court of Auditors 2021).
Footnotes
Acknowledgements
I would like to thank Ndeye Diop for her brilliant assistance in helping to collect and sort data.
Author biography