
Abstract
Background:
Rheumatoid arthritis is a chronic inflammatory disease with progressive joint destruction resulting in functional loss. High-resolution peripheral quantitative CT (HR-pQCT) is a novel technique for detailed volumetric assessment of joint space morphology and bone erosions. We hypothesized that effective control of inflammation in early rheumatoid arthritis (ERA) patients who can achieve sustained simple disease activity index (SDAI) remission will have less progression of joint damage and functional loss than patients who cannot achieve sustained SDAI remission (SDI).
Objectives:
To elucidate the effects of achieving SDI on the progression of joint space outcomes in patients with ERA assessed using HR-pQCT.
Design:
This was a prospective study with 109 participants receiving 1-year tight-control treatment aiming at SDAI remission.
Methods:
A total of 109 patients received 1-year tight-control treatment aiming at SDAI remission. SDI was defined as achieving SDAI remission at months 6, 9, and 12. The primary outcome was the change in joint space size and volume at metacarpophalangeal joints 2–4, determined using HR-pQCT at 12 months.
Results:
At 12 months, HR-pQCT image analysis showed that 14 out of 109 (12.8%) patients achieved SDI (SDI group). No significant differences in changes in joint space and erosion parameters were observed between the SDI and non-SDI groups. Erosion volume was reduced significantly in both groups. While new erosions (0% vs 16%, p = 0.338) and erosion progression (0% vs 27.3%, p = 0.592) were only observed in the non-SDI group, partial erosion healing was numerically more frequently observed in the SDI group (27.3% vs 10.3%, p = 0.260). At baseline, disease activity parameters were positively correlated with joint space parameters, while after 12 months, a negative correlation emerged between disease activity parameters and both mean joint space width (JSW) and minimum JSW.
Conclusion:
Although HR‑pQCT did not show a significant difference in joint damage progression at 12 months between patients with and without sustained remission, the overall cohort—managed with a tight-control strategy targeting SDAI remission—exhibited minimal bone and joint damage progression over 1 year.
Keywords
Introduction
Rheumatoid arthritis (RA) is a chronic disease characterized by persistent synovitis, systemic inflammation, and joint destruction. Joint damage results from the destruction of bone, cartilage, and soft tissue, which can be visualized through radiography as bone erosion and joint space narrowing (JSN), respectively. Studies in established RA have shown that radiographic progression is associated with functional impairment reflected by an increasing health assessment questionnaire score over time. Therefore, prevention of joint damage on radiographs is the gold standard for determining the efficacy of disease-modifying anti-rheumatic drugs (DMARDs) in RA to prevent loss of function. 1 However, most studies have failed to document this association in the early stage of the disease, 2 with most patients demonstrating little baseline joint damage or progression during trials.
Although bone erosion historically has been perceived to be the most critical indicator of permanent disability in RA patients, recent data suggest that, early in the disease process, JSN may be the more important predictor of irreversible physical disability, as measured by the residual score on the disability index of Health Assessment Questionnaire (HAQ-DI) in patients in remission. 3 In patients with early RA (ERA), adalimumab + methotrexate (MTX) inhibited both erosion and JSN progression independently of disease activity, but JSN played a more prominent role in HAQ-DI than erosion. 4
Detection of bone erosions and JSN in RA patients is usually achieved by conventional radiographs despite the low sensitivity. 5 High-resolution peripheral quantitative CT (HR-pQCT) is a sensitive technique for detailed bone microstructure analysis with high reproducibility in assessing bone erosions. 6 With its high spatial resolution (isotropic resolution: 61 μm for XtremeCT II), HR-pQCT exhibited a higher sensitivity in detecting erosion than radiographs and magnetic resonance imaging (MRI). 7 Reproducible, high-throughput, robust, fully automated methodology for evaluating the joint space width (JSW) of the metacarpophalangeal joints (MCPJ) using HR-pQCT has also been developed. 8 Clinically, quantification of 3D joint space morphology could improve early detection of joint damage in rheumatological diseases, 9 and JSW measurement was reliable in longitudinal studies. 10
To separate the reversible disability caused by ongoing inflammation (pain, stiffness, and swelling) from the irreversible joint destruction, we propose to study ERA patients who achieved simple disease activity index (SDAI) remission (SDAI ⩽3.3), that is, a state of absence of significant RA activity and thus reversible disability. We have previously demonstrated that achieving sustained SDAI remission (SDI) in ERA patients was associated with more partial erosion repair on HR-pQCT. 11 Exploring whether sustained remission is crucial to prevent the occurrence of joint destruction (cartilage loss) and, consequently, the accrual of irreversible disability in ERA would be essential. We hypothesized that effectively controlling inflammation in ERA patients who can achieve SDI will have less progression of joint damage and functional loss than those unable to achieve SDAI remission.
Methods
Study design and participants
From April 2020 to December 2022, all new referrals to the rheumatology clinic of the Prince of Wales Hospital (PWH) and three other hospitals in Hong Kong were screened by a research assistant. Patients with at least one tender and swollen joint and symptoms lasting less than 2 years were invited to a screening visit, where a comprehensive medical history, physical examination, laboratory, and radiological assessment were performed by a rheumatologist. The study was approved by the Joint Chinese University of Hong Kong-New Territories East Cluster Clinical Research Ethics Committee (approval No.: CREC 2019.224) and the Ethics Committee of the four regional hospitals (approval No.: KW/EX-20-018(144-06), KC/KE-20-0002/ER-2, HKECREC-2019-105). All patients provided written consent. The reporting of this study conforms to the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement. 12
Patients were eligible if they fulfilled the 2010 ACR/EULAR classification criteria for RA 13 and >18 years old; had symptoms onset of <2 years and had active disease (SDAI >3.3).
Patients were excluded if they had severe clinical deformity at the 2nd, 3rd, or 4th MCPJ, which precluded a reliable HR-pQCT examination, were pregnant, or breastfeeding.
Procedures
All patients received an intensive treatment protocol and were followed up at the PWH every 3 months for 12 months (Figure S1). The following clinical and laboratory variables were assessed at each visit: erythrocyte sedimentation rate, C-reactive protein, number of tender and swollen joints, visual analog scale for pain, patient’s global assessment, and physician’s global assessment (0–10 cm = worst score, scale 0–10). SDAI was calculated at each visit. The number of damaged joints was assessed yearly. Rheumatoid factor (RF) and anti-cyclic citrullinated peptide antibodies status were determined at baseline. Functional disability was assessed by the HAQ-DI.
The therapeutic goal was to achieve SDAI remission. 14 Assessment of efficacy was performed every 3 months. If the desired therapeutic goal was not met within 3 months, therapy was changed to the next treatment protocol (Figure S1), unless the patient declined or a toxic effect precluded this approach. Prednisolone at a dose ⩽10 mg/day was allowed during the study period.
To monitor the possible side effects of the DMARDs, complete blood count, liver function tests, and renal function tests were performed at every visit. The treating physician recorded all adverse events and serious adverse events (SAEs) and, if necessary, made treatment adjustments in accordance with the protocol.
High-resolution peripheral quantitative computed tomography
Metacarpal bone erosion was assessed at MCPJ 2–4 of the most affected hand or dominant hand when both hands were equally affected, using an HR-pQCT system (XtremeCT II; Scanco Medical AG, Brüttisellen, Switzerland) at baseline, 6, and 12 months by a single investigator who was blinded to all patient clinical details. The MCPJ 2–4 were stabilized in a flat position using a specialized platform within an immobilizer cast. With a similar cast, the precision error of the mean JSW was approximately 100 μm (2.1%)—comparable to 2D radiographic precision. 9
Volumetric joint space was quantified using an algorithm developed by consensus from the Study grouP for eXtreme Computed Tomography in Rheumatoid Arthritis (SPECTRA). 15 The 3D JSW, including mean (mean JSW, mm), maximum (max JSW, mm), minimum (min JSW, mm), standard deviation (SD; JSW.SD, mm), asymmetry, and volume (JSV, mm3) were calculated. Two trained readers with HR-pQCT expertise reviewed all joints and scored for the degree of luxation and bone-on-bone contact.
Erosions were defined as sharply marginated bone lesions with juxta-articular localization, with a cortical break seen in at least two adjacent slices, often with a loss of the adjacent trabecular bone according to the SPECTRA definition. 16 The largest erosion of each MCPJ was characterized by the maximal width and depth of the lesion in the axial, sagittal, and coronal planes using ITK-SNAP 3.8.0 (open-source software; Penn Image Computing and Science Laboratory, University of Pennsylvania, Philadelphia, PA, USA). Erosion volume was automatically calculated by the Bone Analysis Modules of an open-source image analysis tool (3D Slicer). 17
The signs of bone apposition at the margin of the erosion were as documented before. 11 Quantitative osteosclerosis was calculated by choosing the area around bone erosion in MCPJ 2–4 as region of interest (ROI). 18 The ROI’s density was calculated as the mean pixel attenuation of that area. 3D registration was applied to obtain a consistent segmentation of the periosteal surface in the vicinity of the cortical break, which was crucial for accurate quantification of bone damage. One experienced reader who was unaware of the patients’ treatment independently measured all parameters of bone erosion: width, depth, volume, and marginal osteosclerosis.
Partial erosion repair was defined as a decrease in erosion volume exceeding the Least Significant Change (LSC) and an increase in marginal osteosclerosis exceeding LSC, while an increase in erosion volume exceeding LSC and a decrease in marginal osteosclerosis exceeding LSC was classified as erosion progression.19,20
To determine the LSC, 20 randomly selected erosions for volume and marginal osteosclerosis from the study cohort were scored twice by the reader. LSC was calculated as: LSC = ±2.77×
The intra-observer and inter-observer reproducibility were assessed using the intraclass correlation coefficient to validate the consistency in JSW and erosion analysis. All acquired images were selected for motion-grade assessment. Image quality of each acquisition was graded according to the manufacturer-suggested image grading system. 21 The images with good quality (grade 1–3) were used for further analysis. In addition, scans with implausible joint space measurements identified as statistical outliers were excluded. Joints with evaluable images at both baseline and follow-up were included in the paired analyses. Joints with missing data at either time point were excluded.
Radiographs
Radiography images at baseline and 12 months were analyzed in paired, chronological order using the Sharp-van der Heijde (SvdH) method by one trained reader. Twenty-three randomly selected patients’ images were re-analyzed in paired order to assess intra-reader reproducibility and determine the smallest detectable change (SDC).
22
SDC was calculated as: SDC = ±1.96 × SDΔ (patients’ change-score)/
Statistical analyses
Data normally distributed were expressed as mean ± SD, while non-normally distributed data were shown as median (interquartile range, IQR). Mann–Whitney U test and Chi-square test were used to evaluate differences between groups. Subgroup analyses were performed according to SDI status (SDI vs non-SDI). Differences in the changes in outcome measurements between groups were ascertained using the Mann–Whitney U test, the Chi-square test, or the Fisher exact test where appropriate. The Wilcoxon signed-rank test was used for within-group comparison. The Friedman test was used to explore the association between achieving SDI and progression of joint space size and volume, and erosion size with adjustment for baseline characteristics. Generalized Estimating Equation (GEE) regression model was used to investigate the relationship between changes in bone erosion parameters on HR-pQCT between the two groups over 1 year, considering within-patient correlation and adjusting baseline parameters. Spearman correlation was used to investigate the associations between disease activity parameters, erosion and joint space parameters, SvdH score, and HAQ-DI at different timepoints. Patients without evaluable follow-up data or with missing values were analyzed using a complete-case analysis approach. A two-tailed probability value of p < 0.05 was considered statistically significant. Analyses were conducted using IBM SPSS Statistics Version 29 (IBM, Armonk, NY, USA).
Outcomes
The primary outcome was the effect of achieving SDI at 6, 9, and 12 months (SDI group) on the progression of joint space size and volume over a 12-month period as evaluated by HR-pQCT compared to those unable to sustain SDAI remission (non-SDI group).
The secondary outcomes were changes in size of erosion (depth, width, and volume) and marginal osteosclerosis using HR-pQCT; changes in SvdH score at 12 months between the SDI group and non-SDI group, and association between joint space and erosion size on HR-pQCT and HAQ-DI at baseline, 6, and 12 months to determine the impact of joint damage on reversible and non-reversible disability.
Sample size estimation
A sample size determination was conducted for the primary outcome measurement, the change in mean JSW at 12 months, using Power Analysis and Sample Size Software (PASS version 11, NCSS, LLC, Kaysville, Utah, USA). Our previous research on ERA patients showed a JSW change of 0 mm ± 0.034 mm and −0.043 mm ± 0.099 mm for those achieving and not achieving SDI over a year, with an effect size of 0.60. Another previous study indicated a SDI rate was 30%. 11 At least 98 patients would be required to achieve a statistical power of 0.8 with a two-sided α of 0.05. With an estimated dropout rate of 10%, a sample size of 110 would be required. Due to a lower interim SDI rate of 12.1%, we aimed to recruit 10 additional patients during the COVID pandemic to meet the study’s goals.
Results
A total of 120 patients were recruited. Among them, 109 patients underwent HR-pQCT assessment at month 12 and were included in the final analysis for JSW and erosion progression (Figure 1). SDAI remission was achieved by 14 (13%), 28 (26%), 40 (37%), and 42 (39%) of patients at 3, 6, 9 months, and at 1 year, respectively (Figure S2). Treatment used over a year is summarized in Figure S3. On average, SDAI remission was achieved in 19% of the visits. Treatment was escalated in 77.6% of visits when SDAI remission was not met. Reasons for non-escalation of treatment are summarized in the Table S2. Eight episodes of SAEs were reported (Table S3). No unexpected SAEs or deaths were observed.

Trial profile.
Fourteen patients (12.8%) achieved SDI from 6 to 12 months (SDI group). At baseline, the SDI group exhibited a lower prevalence of RF and lower disease activity (Table 1). The usage of conventional synthetic DMARDs (csDMARDs), biologic/targeted synthetic DMARDs (b/tsDMARDs), nonsteroidal anti-inflammatory drugs, and glucocorticoids was similar between the two groups (Table 1). After 12 months, improvement in disease activity was observed in both groups, and the SDI group had significantly lower disease activity than the non-SDI group, and a significantly higher proportion of patients in the non-SDI group were exposed to sulfasalazine and hydroxychloroquine (Table S1).
Clinical, demographic, and radiographic parameters and medication use at baseline.

Data are reported as mean ± SD, median (interquartile range) or number (%).
Anti-CCP, anti-cyclic citrullinated peptide antibody; b/tsDMARDs, biologic and synthetic disease-modifying anti-rheumatic drugs; CRP, C-reactive protein; csDMARDs, conventional synthetic disease modifying anti-rheumatic drugs; DAS 28-CRP, disease activity score 28-CRP; ESR, erythrocyte sedimentation rate; HAQ-DI, health assessment questionnaire-disability index; JSN, joint space narrowing; NSAIDs, nonsteroidal anti-inflammatory drugs; RF, rheumatoid factor; SDAI, simple disease activity index; SDI, sustained SDAI remission; VAS, visual analog scale; vdH-Sharp score, van der Heijde-Sharp score.
Due to motion artifacts or severe joint damage at individual visits, paired JSW analyses were available for 104 patients at MCPJ 2, 101 at MCPJ 3, and 97 at MCPJ 4. In addition, paired erosion analyses were available for 98 erosions in 106 patients.
Regarding the assessment of joint space, no significant changes were observed in all parameters at MCPJ 2–4 over the 1-year period in both groups (Figure 2, Table S4). After 12 months, a significant reduction in erosion volume and a significant increase in marginal osteosclerosis were observed in both groups (Figure 3, Table S5). Although no statistical differences were observed between the two groups, new erosions (0% vs 16.1%, p = 0.338) and erosion progression (0% vs 27.3%, p = 0.592) were only observed in the non-SDI group, while partial erosion repair was numerically more frequently observed in the SDI group (27.3% vs 10.3%, p = 0.26; Table 2, Figure 3). In the GEE model adjusting for within-subject variation, patients in the SDI group had numerically higher odds of erosion repair (odds ratio: 3.25, 95% confidence interval: 0.8–13.8, p = 0.11). The changes in erosion depth and width were similar between the two groups (Figure 3, Figure S4).

Graphs depicting the results of a Friedman test comparing the effects of achieving sustained SDI remission on 3D joint space. The minimum to maximum value and interquartile range are presented within a bounding box. (a) Joint space volume. (b) Mean JSW. (c) Maximum (max) JSW. (d) Minimum (min) JSW. (e) JSW SD. (f) JSW AS.

Graphs depicting erosion results by HR-pQCT. (a) Individual erosion volume of the SDI and non-SDI group at 3 time points over 1 year. IQR and 1.5 times the IQR below the first quartile and above the third quartile are presented within a bounding box. Changes in erosion parameters between the SDI and non-SDI group (median and IQR). (b) Erosion volume. (c) Erosion width. (d) Erosion depth. (e) Marginal osteosclerosis. (f) Outcome of erosion progression (%), partial repair (%), and new erosions detected in patients (%) across the study period.
Outcomes of pre-existing individual erosion.
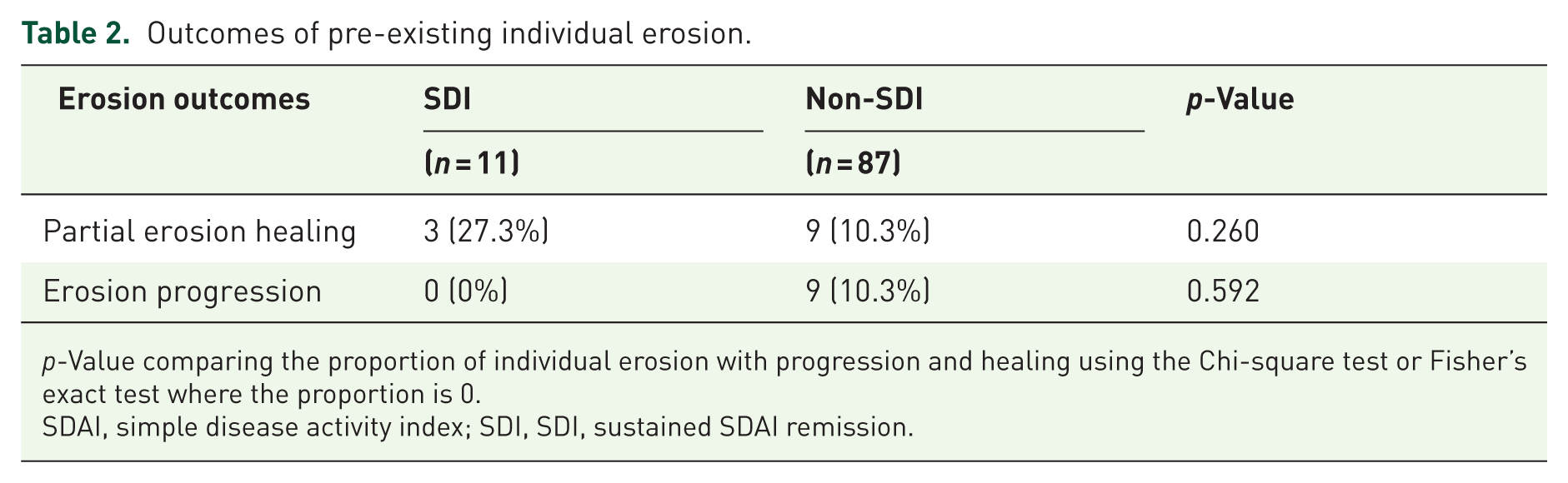
p-Value comparing the proportion of individual erosion with progression and healing using the Chi-square test or Fisher’s exact test where the proportion is 0.
SDAI, simple disease activity index; SDI, SDI, sustained SDAI remission.
Radiographic joint damage at baseline, although present in a substantial proportion of this population with ERA, was limited, with a median SHS score (IQR) of 6 (2,12) (Table 1). After 1 year, the median SHS score (IQR) was 7 (2,13). JSN and erosions were seen in MCPJ 2–4 in around 20% of patients (Figure S5). After 12 months, the non-SDI group showed a significant increase in the total SvdH score, JSN score, and erosion score, while all the scores remained unchanged in the SDI group (Table S6). If the results are confined to MCPJ 2–4, no significant changes between the two groups were observed.
Significant improvement in HAQ-DI was observed in both groups, and the changes in the HAQ-DI at 12 months were not significantly different between the two groups (Figure S6 and Table S1).
In view of the nonlinear change in disease activity (rapid decrease in the first 6 months, Figure S2), cross-sectional correlation analysis between disease activity, function, and the joint space parameters was assessed at baseline, 6, and 12 months (Figure 4). At baseline, disease activity parameters correlated positively with JSV and max JSW. Notably, at MCP4, a significant positive correlation was found between max JSW and SDAI (r = 0.268, p = 0.008), also DAS28-CRP (r = 0.331, p < 0.001). At month 6, a negative correlation started to emerge between patient-reported outcomes and residual inflammation with mean and min JSW. At month 12, HAQ-DI was negatively correlated with mean JSW (r = −0.206, p = 0.04) and min JSW (r = −0.237, p = 0.017) of the MCP2. Similarly, negative correlation was observed between min JSW of the MCP3 and disease activity parameters like SDAI (r = −0.222, p = 0.028).

Heatmap of correlation coefficient between disease activity, function, and the joint space parameters from baseline to month 12.
Discussion
This is the first prospective, ERA cohort that applied a treat-to-target (T2T) strategy aiming at SDAI remission to ascertain the impact on bone and joint damage accrual using HR-pQCT and radiography. Improvement in disease activity parameters was observed in both groups after 1-year treatment despite the fundamental difference between the two groups at baseline. In this study, contrary to our hypothesis, no significant changes in 3D joint space metrics were detected in the two groups. There are several reasons why we failed to detect differences in the joint space metrics between the two groups. First, considering the average size of a female MCPJ (1.2–2.2 mm), 23 the magnitude of changes in the JSW parameters (median changes 0.0–0.06 mm) may indicate a lack of clinically relevant cartilage damage in these ERA patients. Similarly, two previous studies in ERA patients (n = 33), other inflammatory arthritis (n = 10), and established RA (n = 48) also failed to demonstrate any significant group-level changes in JSW over 9–12 months. 24 The second reason may be related to the small proportion of patients achieving SDI (12.8%), which was lower than our previous study (30.2%). The small number of patients who achieved sustained remission undermines the statistical power and limits the scope of reliable inference. Nonetheless, the current study had a larger sample size (109 patients compared with 63 patients). 11 The rate of SDAI remission achievement from months 3 to 12 (13%–39%) in the current study was comparable to another recent T2T study using abatacept (9%–27%) 25 and the Ra BiODaM (BiOmarkers of joint DaMage) cohort (16%–26%). 26 Further research may be required to determine whether this finding reflects the absence of a true difference between groups or limitations in detection with HR-pQCT. A third reason is that only 20% of the radiographic JSN were observed in the MCPJ 2–4 (Figure S4), suggesting that including wrist and metatarsophalangeal joint JSW measurements could be necessary to reveal true differences in future studies. Fourth, a 1-year follow-up may be too short to capture meaningful JSW changes. During active inflammation, synovitis can transiently increase joint space volume; after inflammation subsides, joint space may decrease, unmasking cartilage loss. Therefore, a longer observation period would better distinguish JSW changes driven by transient synovitis from those reflecting true structural cartilage loss. Given these constraints, we cannot determine whether the absence of between-group differences reflects a true lack of effect or insufficient sensitivity to detect early cartilage change. Future work should include larger sample sizes, longer follow-up, and broader joint coverage. Incorporating cartilage-sensitive modalities—such as gadolinium-enhanced MRI techniques (e.g., dGEMRIC) or alternative quantitative MRI sequences—may improve detection of early proteoglycan loss and better elucidate the impact of sustained remission on JSW. 27
While JSW parameters remained relatively stable, the current study demonstrated that erosion parameters detected by HR-pQCT are still playing a prominent role in terms of representing structural changes in ERA patients. A significant reduction in erosion volume and a significant increase in osteosclerosis were observed in both groups, suggesting that a T2T strategy aiming at SDAI remission can indeed prevent bone damage. Nevertheless, the absence of new erosion development and erosion progression, along with a numerically higher proportion of partial erosion repair in the SDI group, were findings consistent with our previous study, 11 and suggest a trend that achieving sustained disease control may be able to reverse damage, even in this group of patients treated with csDMARDs only. Partial erosion repair has been reported previously in other RA studies, 24 and in patients treated with csDMARDs or b/tsDMARDs, including anti-TNF 28 and anti-IL-6 therapies. 29 Future studies should include patients on b/tsDMARDs in SDI to elucidate the potential for complete erosion healing.
Radiographic joint damage as reflected by the SvdH score was significantly increased in the non-SDI group but remained unchanged in the SDI group. In a 2-year result in the PREMIER trial, SDI was associated with a virtual arrest of joint damage, irrespective of treatment type, aligning with our results. They also demonstrated that preceding disease activity significantly influences radiographic progression over time, emphasizing the need to not only achieve but also maintain remission as long as possible. 30 The current study also provided important information regarding the superior sensitivity of HR-pQCT over conventional radiography (CR) in detecting erosion progression or healing in ERA patients, with no significant differences in SvdH score changes in MCPJ 2–4 between the two groups.
With regards to the association between joint space metrics and inflammation, a positive correlation between disease activity markers and JSV and JSW probably indicates subclinical joint swelling in this ERA study in the cross-sectional analysis at baseline. Similar findings were also reported in a previous study after 3 months of TNF inhibition. 28 However, a negative correlation between disease activity parameters and JSW (mean and min) in the cross-sectional analysis emerged at 6 months and persisted at 12 months. Our previous study in long-standing psoriatic arthritis patients also reported that a higher inflammatory burden was negatively associated with JSW. 31 These data suggest that joint space indices may be a sensitive biomarker for monitoring changes in inflammatory burden (synovitis and subclinical joint swelling) in the initial phase of active disease.
Except for the negative association between HAQ-DI with mean and min JSW at month 12 in the cross-sectional analysis, no other associations were found between bone erosion volume, radiographic damage, and HAQ-DI (data not shown). This aligns with another study reporting that MRI-assessed inflammation, not damage, in ERA wrists is associated with patient-reported physical impairment. Patient global assessment of disease activity and pain influences hand function, but not between MRI/radiographic bone erosion and JSN. 32 Moreover, the MCPJ damage scores did not independently correlate with HAQ-DI. The fact that the current study did not find an association between HAQ-DI and HR-pQCT erosion/radiographic damage may be explained by the low level of damage in these ERA patients.
Some limitations of HR-pQCT should be discussed. First, it cannot detect soft tissue changes effectively, better assessed by US and MRI. Second, evaluating MCPJ 2–4 instead of the entire hand. Although this cannot be interchanged with CR imaging of all 44 joints, as the gold standard, for tracking erosive diseases, it can add valuable complementary information to that obtained by CR of hands, wrists, and feet. Moreover, the second to fourth MCP joints chosen are based on their frequent involvement in erosive RA and are recommended in the endorsed imaging protocol. 33 HR-pQCT of only two MCP joints was also suggested comparable to CR by its diagnostic accuracy for classifying patients with established RA as having erosive diseases. 34 Indeed, a substantial proportion of patients with erosive progression are overlooked using CR only to monitor erosive progression. 19 In addition, subtle changes in JSW in these regions were potentially correlated with functional outcome, unlike the SvdH score. With minor joint destruction in ERA patients, the HR-pQCT is more feasible due to its high sensitivity.
Strong points include that we have not only assessed the damage features in the MCPJ using HR-pQCT, but also included radiographs of the hands and feet to explore potential explanations for the observed relationships. We believe that our patient population with ERA, treated in a tight control setting with limited joint damage, represents the RA patients of this and future decades. In addition, our utilization of a GEE model, which can adjust for different confounders, is suitable for non-normally distributed data like bone erosion on HR-pQCT, ensuring robust analysis.
Conclusion
In conclusion, although no significant difference in joint damage progression on HR-pQCT was observed at 12 months between patients with or without sustained remission, treatment with a tight control strategy was effective in limiting bone and joint damage progression over 1 year on HR-pQCT in the whole ERA cohort. The potential correlation between joint damage assessed by HR-pQCT and functional outcome could have important implications for evaluating treatment success if confirmed by future studies.
Supplemental Material
sj-docx-1-tab-10.1177_1759720X261439714 – Supplemental material for Effects of achieving simple disease activity index remission on joint space outcomes progression in early rheumatoid arthritis: an exploratory study using high-resolution peripheral quantitative computed tomography
Supplemental material, sj-docx-1-tab-10.1177_1759720X261439714 for Effects of achieving simple disease activity index remission on joint space outcomes progression in early rheumatoid arthritis: an exploratory study using high-resolution peripheral quantitative computed tomography by Qihan Wu, Ho So, Isaac T. Cheng, Yingzhao Jin, Sze-Lok Lau, Tin-Yuet Chan, Evelyn Chow, Ling Qin, Vivian W. Hung, James F Griffith, Kitty Kwok, Isaac Yim, Shirley Ying, Ka Lai Violet Lee, Jack J. W. Lee and Lai-Shan Tam in Therapeutic Advances in Musculoskeletal Disease
Supplemental Material
sj-docx-2-tab-10.1177_1759720X261439714 – Supplemental material for Effects of achieving simple disease activity index remission on joint space outcomes progression in early rheumatoid arthritis: an exploratory study using high-resolution peripheral quantitative computed tomography
Supplemental material, sj-docx-2-tab-10.1177_1759720X261439714 for Effects of achieving simple disease activity index remission on joint space outcomes progression in early rheumatoid arthritis: an exploratory study using high-resolution peripheral quantitative computed tomography by Qihan Wu, Ho So, Isaac T. Cheng, Yingzhao Jin, Sze-Lok Lau, Tin-Yuet Chan, Evelyn Chow, Ling Qin, Vivian W. Hung, James F Griffith, Kitty Kwok, Isaac Yim, Shirley Ying, Ka Lai Violet Lee, Jack J. W. Lee and Lai-Shan Tam in Therapeutic Advances in Musculoskeletal Disease
Supplemental Material
sj-docx-3-tab-10.1177_1759720X261439714 – Supplemental material for Effects of achieving simple disease activity index remission on joint space outcomes progression in early rheumatoid arthritis: an exploratory study using high-resolution peripheral quantitative computed tomography
Supplemental material, sj-docx-3-tab-10.1177_1759720X261439714 for Effects of achieving simple disease activity index remission on joint space outcomes progression in early rheumatoid arthritis: an exploratory study using high-resolution peripheral quantitative computed tomography by Qihan Wu, Ho So, Isaac T. Cheng, Yingzhao Jin, Sze-Lok Lau, Tin-Yuet Chan, Evelyn Chow, Ling Qin, Vivian W. Hung, James F Griffith, Kitty Kwok, Isaac Yim, Shirley Ying, Ka Lai Violet Lee, Jack J. W. Lee and Lai-Shan Tam in Therapeutic Advances in Musculoskeletal Disease