
Abstract
Recent guidelines on rheumatoid arthritis (RA) point to the importance of achieving remission as soon as possible during the course of the disease. The appropriate use of antirheumatic drugs is critical, particularly in early RA patients, before 24 weeks, since this is a ‘window of opportunity’ for treatment to modify disease progression. A treat-to-target strategy added to an aggressive therapeutic approach increases the chance of early remission, particularly in early RA patients. We conducted an overview of current therapeutic strategies leading to remission in early RA patients. We also provide interesting predictive factors that can guide the RA management strategy with regard to disease-modifying treatment and/or drug-free remission.
Keywords
Introduction
The new strategy in rheumatoid arthritis (RA) care management consists of early diagnosis and early treatment to achieve complete suppression of disease activity, that is, remission. The prevalence of minimal disease activity is variable between studies, perhaps because there is still no universally accepted definition of remission. Comparisons between studies are difficult since different remission criteria have been published according to each disease activity score used, for example, the Clinical Disease Activity Index (CDAI), the Simplified Disease Activity Index (SDAI), American College of Rheumatology/European League Against Rheumatism (ACR/EULAR) criteria, and Disease Activity Scores (DAS 44, DAS 28) [Felson et al. 2011]. The clinical course of RA is variable and prognosis is difficult to predict. One of the major goals of the 2010 ACR/EULAR classification criteria guidelines was to provide diagnosis of RA earlier in the course of the disease [Aletaha et al. 2010]. However, several recent studies have indicated that the 2010 RA criteria convey a high risk of misclassification of early RA (ERA) patients [Zeidler, 2012]. Biological disease-modifying antirheumatic drugs (bDMARDs) or synthetic disease-modifying antirheumatic drugs (sDMARDs) have been shown to reduce markedly progression of the disease and are critical in defining patient outcome. The recent RA guidelines focused on patients with high risk of joint damage due to risk factors such as anticitrullinated peptide antibodies (ACPA), rheumatoid factor (RF) or erosions at baseline [Smolen et al. 2014]. However, all patients should benefit from a more aggressive therapy in the early stage of the disease. Disease duration has been a key determinant of response rate, whichever drug is prescribed [Gremese et al. 2013]. Indeed, we can define early ERA as 12 months from symptom onset and even very early RA (VERA) as within the first 3 months of disease onset as important outcomes in predicting remission [Gremese et al. 2013].
Actually, a ‘window of opportunity’ exists where patients are more susceptible to the benefits of active treatment (i.e. disease-modifying drugs) in the early stage of the disease compared with the late stage to stop disease progression, since joint damage appears to be more frequent during disease onset [Boers, 2003; Gremese et al. 2013; Lard et al. 2001; Mottonen et al. 2002]. Drug intervention in this period may hamper disease progression. When the diagnosis has been established, delay in initiating treatment is associated with increasing joint damage and less drug-free remission [Finckh et al. 2006; van Nies et al. 2014]. Thus, clinicians should direct specific efforts to identifying and treating ERA, because this process may also be cost-effective.
An EULAR task force highlighted the fact that ‘patients presenting with arthritis of more than one joint should be referred to and seen by a rheumatologist, ideally within 6 weeks after the onset of symptoms’ [Combe et al. 2007]. This statement remains extremely important and several referral centres for RA are currently organized to ensure timely treatment for RA patients.
Treat-to-target as the key factor to induce remission in ERA
The introduction of a treat-to-target (T2T) strategy as a standard of care in RA routine clinical practice [Smolen et al. 2010] has underscored the pressing need to induce an effective and long-term remission of disease in order to prevent joint destruction and disability.
The key elements of the T2T concept are monitoring of disease activity, adjusting medication in accordance with a predetermined protocol, and aiming at a specific target. The effectiveness of T2T has been extensively demonstrated, especially in ERA and VERA [Goekoop-Ruiterman et al. 2010; Schipper et al. 2010; Soubrier et al. 2011]. Indeed, in the Dutch RA monitoring remission induction cohort study, 47% of patients achieved remission in the first 6 months and almost 60% reached remission at 12 months [Schipper et al. 2012]. After 3 years of follow up, investigators showed high and sustained remission rates of 60%, with improvements in physical function and limited radiographic damage leading to a gain in quality-adjusted life years, proving that T2T is also cost-effective [Vermeer et al. 2013].
Following a T2T strategy implies an essential principle, that is, right therapies at the right time. The right time to prescribe a DMARD in RA has been called the ‘window of opportunity’ [Boers, 2003; O’Dell, 2002]. However, remission-induction therapies represent an evolving field. The optimal strategy in ERA remains unaddressed [Graudal and Jurgens, 2010; Ma et al. 2010]. Intensive DMARD combination strategies with or without glucocorticoids (GCs) as well as the early introduction of biological therapy are currently within the scope of RA clinical research [De Cock et al. 2014; Moreland et al. 2012; O’Dell et al. 2013; van Vollenhoven et al. 2009].
Therapeutic window of opportunity in RA
The notion of a therapeutic window as a time when disease responds best to treatment and long-term remission is within reach has been supported by randomized clinical trials, meta-analysis and observational studies in RA [Nell et al. 2004; Raza et al. 2012; Raza, 2010].
The association of better outcomes with earlier treatment was first suggested in the late 1980s [Healey and Wilske, 1989]. Later on, this concept was reaffirmed by multiple clinical studies showing that disease duration before treatment inception is probably the most important determinant of therapeutic response, independent of the prescribed drug. Van Nies and colleagues recently showed that each week of delay in the introduction of active therapy in RA reduced the chance of DMARD-free remission in 1% of patients [van Nies et al. 2014]. ERA patients are more susceptible to obtaining a benefit compared with the late stage because the occurrence of joint damage is more frequent during this early period of time [Boers, 2003; Gremese et al. 2013; Lard et al. 2001; Mottonen et al. 2002]. A meta-analysis found that patients who received early treatment had 33% less radiographic progression compared with those with delayed treatment, even when patients less than 2 years of RA onset were considered [Finckh et al. 2006]. The benefits described for such early therapeutic intervention, that is, within the window of opportunity, include: (a) reduction of disease progression and chronicity; (b) halting of joint destruction; (c) significantly better drug-free remission rates.
The timeframe of such a window is currently a matter of analysis. In the Finnish Rheumatoid Arthritis Combination Therapy (FIN-RACo) trial, patients were randomized to a single DMARD versus a combination of DMARDs. The delay in therapy (over 4 months) solely was a negative predictor for remission in the single-DMARD group [Mottonen et al. 2002]. In accordance with this timeframe, the Combination of Methotrexate and Etanercept in Active Early Rheumatoid Arthritis (COMET) study evidenced that methotrexate (MTX) associated with etanercept in the first 4 months obtained better results in terms of remission and disease activity compared with the same combination after 4 months [Emery et al. 2012]. More accurate data were obtained from two large cohorts of ERA patients. The Leiden Early Arthritis Clinic (EAC) and the Evaluation et Suivi de Polyarthrites Indifférenciées Récentes (ESPOIR) cohort have set time points for DMARD introduction to approximately 11 weeks from symptom onset for ACPA-positive RA patients and 15 weeks for ACPA-negative subjects. Regarding the achievement of DMARD-free sustained remission, the window appeared to end at 14.9 weeks for patients in the Leiden cohort and 19.1 weeks in the ESPOIR cohort [van Nies et al. 2015]. Therefore it seems that the window begins to close between the third and fourth month of symptom onset. More precise information about the exact timeframe of the therapeutic window will be obtained once pivotal mechanisms determining RA onset have been fully elucidated. Indeed, Raza and colleagues have described a different phenotype of synovial fluid based on T cell, macrophage and stromal cell-related cytokines, which is exhibited during an early stage of RA synovitis and is not present in later established RA [Raza et al. 2005]. This unique feature reflects the fact that early synovial inflammation is qualitatively different and probably more manageable with the introduction of prompt treatment.
Remission-induction therapy strategies
In ERA, long-term remission induction is a realistic target and should be reached in the majority of patients, since it is a predictor of a 5-year outcome. Nonetheless, the optimal way to achieve such an objective is still debated among experts. The issue should be considered as an evolving field, given the expansive development of new components for the treatment of RA. In fact, some of the clinical trials that originated the concept of intensive strategies to reach prompt remission have been carried out with drug combinations that are no longer in use today. All the concepts presented here regarding the ERA therapeutic approach are summarized in Figure 1.
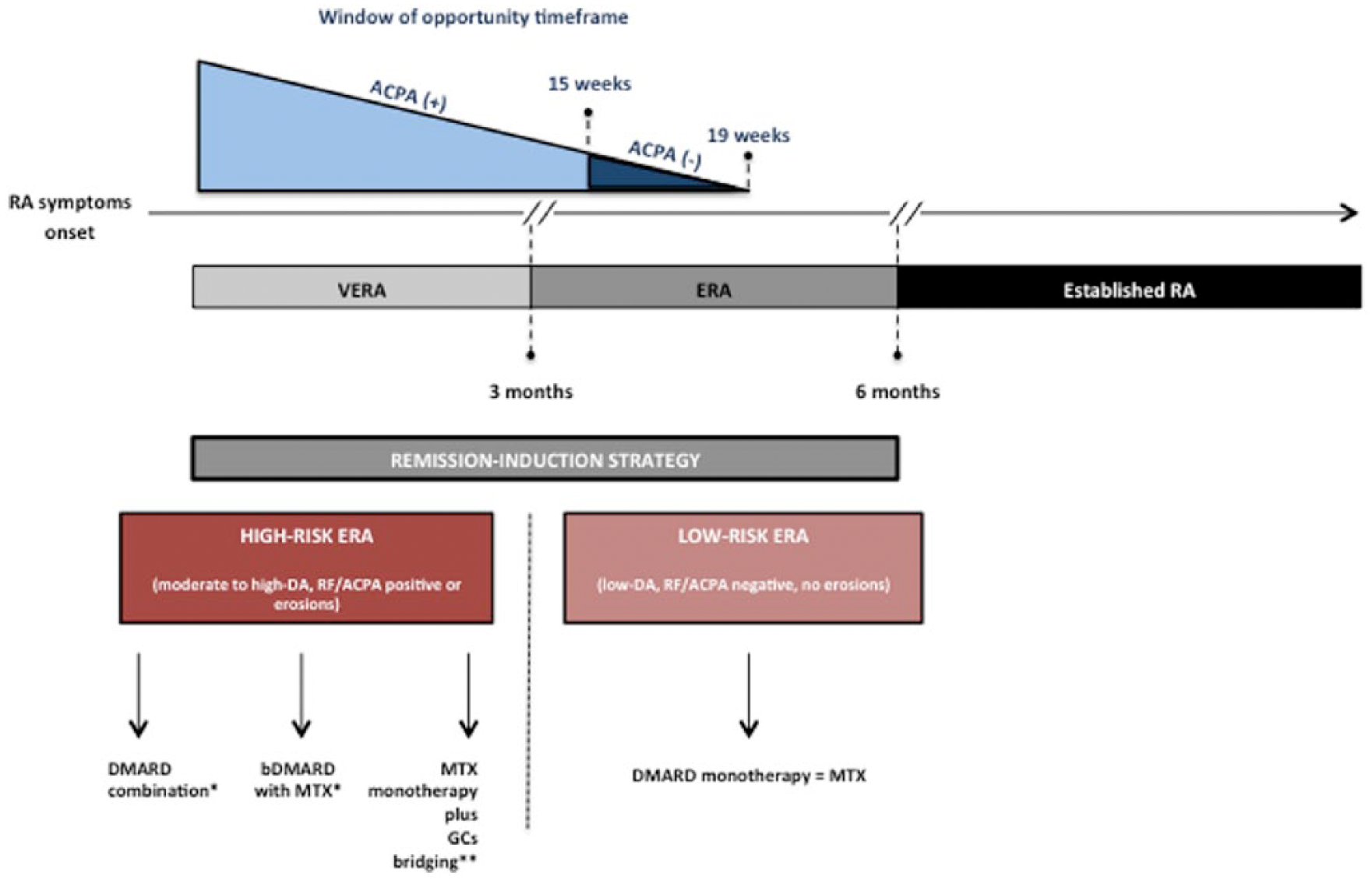
Global vision of therapeutic strategy in early rheumatoid arthritis (ERA): the principle of ‘right therapies at the right time’. In the upper part of the figure, the ‘window of opportunity’ is represented with a differential timeframe between seropositive and seronegative patients. Very early rheumatoid arthritis (VERA) and ERA definitions are also integrated. In the lower part, the therapeutic approach has been summarized in low-risk and high-risk rheumatoid arthritis (RA) patients. ACPA, anticitrullinated peptide antibody; DA, disease activity; DMARD, disease-modifying antirheumatic drug; GC, glucocorticoid; MTX, methotrexate; RF, rheumatoid factor. *Consider adding low-dose GCs (10 mg/day prednisone or equivalent) in patients with moderate to high RA disease activity. **Bridging GC therapy: step down from 30 mg/daily prednisone or equivalent at onset to 7.5 mg/daily at 16 weeks.
Furthermore, in those clinical studies the timeframe for considering ERA was up to 2 years. Proudman and colleagues compared an intensive treatment with MTX, cyclosporine (CyC) and intra-articular GCs with sulfasalazine (SSZ) monotherapy [Proudman et al. 2000]. The CIMESTRA trial, assessed the addition of CyC to a regimen of MTX and GCs [Hetland et al. 2008]. Furthermore, the timeframe for considering ERA was longer than currently considered. The classical studies BeSt and TEAR included patients with ERA with disease duration of 2 and 3 years, respectively [Goekoop-Ruiterman et al. 2005; Moreland et al. 2012]. In other words, an important part of the highly valuable trials that supported the concept of T2T are no longer a proper guide with respect to optimal therapeutic schemata in ERA (less than 12 months after symptom onset).
Recent recommendations made by the 2015 ACR guideline for the treatment of RA have taken into account these issues, setting less than 24 weeks as a cut-off for ERA versus established RA, while establishing treatment guidelines [Singh et al. 2016]. Basically, current therapeutic regimens could be divided into DMARD monotherapy (most often defined as the use of MTX therapy), DMARD combination (two or more sDMARDs), or the early introduction of bDMARDs with sDMARDs. A generalized consensus exists today about the therapeutic approach in low-risk ERA (low disease activity, absence of baseline erosions and RF/ACPA negative). In those patients, MTX should be the preferred initial resource due to its good profile of efficacy and low rate of side effects. On the other hand, a different approach must be considered in the induction phase of DMARD-naïve patients with unfavourable prognostic factors such as high-disease activity, seropositivity (RF and/or ACPA), and erosions. Common choices in this setting are focused on sDMARD combination and early introduction of MTX associated with a bDMARD, with no indication of preference between them [Leirisalo-Repo, 2013]. Triple sDMARD combination, MTX+SSZ+hydroxychloroquine (HCQ) (i.e. FIN-RACo trial), or double therapy, MTX+SSZ or leflunomide and step-down GCs (i.e. Combinatietherapie Bij Reumatoide Artritis [COBRA] scheme), showed superiority compared with DMARD monotherapy. Also, bDMARDs (tumour necrosis factor [TNF] inhibitors, abatacept, tocilizumab and rituximab) plus MTX have demonstrated a clear benefit over MTX alone in reaching remission and delaying radiologic progression (PREMIER study, COMET study, the Golimumab in Active Rheumatoid Arthritis Despite Methotrexate Therapy [GO-BEFORE] study, Active Controlled Study of Patients Receiving Infliximab for Treatment of Rheumatoid Arthritis of Early Onset (ASPIRE), etc.) [Breedveld et al. 2006; Emery et al. 2012, 2015; Smolen et al. 2006].
Nevertheless, comparisons between combined DMARDs (triple therapy) and early introduction of bDMARDs associated with MTX did not reveal significant differences in terms of efficacy (the NEO-RACo trial, the Optimized Treatment Algorithm in Early Rheumatoid Arthritis [OPERA] study and the Infliximab as Induction Therapy in Early Rheumatoid Arthritis [IDEA] study) [Horslev-Petersen et al. 2014; Nam et al. 2014; Rantalaiho et al. 2014]. Actually, remission rates were close to 60% in the first year with slight differences in structural outcomes in favour of bDMARDs in some cases. Early introduction of bDMARDs during the course of the disease allows later drug discontinuation still maintaining a sustained drug-free remission. On the other hand, some studies have focused on early inflammatory arthritis (Induction Therapy with Methotrexate and Prednisone in Rheumatoid or Very Early Arthritic Disease [IMPROVED] study, the Strategies in Early Arthritis Management [STREAM] trial, the Abatacept Study to Determine the Effectiveness in Preventing the Development of Rheumatoid Arthritis in Patients with Undifferentiated Inflammatory Arthritis and to Evaluate Safety and Tolerability[ADJUST]) [van Eijk et al. 2012; Emery et al. 2010; Heimans et al. 2014]. In those subjects, bDMARDs decreased the rate of patients who finally meet criteria for RA, suggesting this strategy might interrupt progression towards established disease. Unfortunately, this was not the case for all patients, and despite the cumulative evidence now available, the use of bDMARDs as first-line therapy remains controversial.
On the other hand, the therapeutic role of supplementary steroids in RA is not under discussion, as they convey long-term benefits even years after withdrawal. Indeed, the Better Anti-Rheumatic PharmacoTherapy (BARFOT) study revealed that the beneficial effect of low-dose GCs (prednisolone 7.5 mg daily during the first 2 years of RA) on radiological damage is still detectable after 4 years of follow up [Hafstrom et al. 2009]. Moreover, the use of moderate- to high-dose GC bridging associated with MTX might represent an alternative option during the window of opportunity. Recently, the Care in Early RA (CareRA) trial has compared three versions of the COBRA scheme (Classic, Avant-Garde and Slim) in high-risk ERA patients (moderate to high activity with seropositivity and/or erosions). The Slim version, consisting of MTX associated with GC step-down (from 30 mg/daily to 7.5 mg/daily at 16 weeks), was as effective in inducing remission (73% versus 70% and 68% in Classic and Avant-Garde, respectively) as DMARD combination therapy, although it exhibits a more favourable short-term (16 weeks) safety profile [Verschueren et al. 2015]. All this evidence has been integrated in recent RA guidelines, which recommend adding low-dose GCs (10 mg/day of prednisone or equivalent) to patients with moderate to high RA disease activity when starting DMARDs, and also consider the use of moderate- to high-dose GCs while waiting for DMARD efficacy [Singh et al. 2016].
Predictive factors of remission in ERA
Therapy for RA has changed profoundly over the past 25 years. Since the introduction of bDMARDs, the goal of treatment has moved from symptomatic response to a stringent full remission, with minimal or no residual symptoms [Felson et al. 2011]. The course of RA is determined by an early diagnosis and early initiation of antirheumatic drugs leading to better long-term outcomes [Gossec and Dougados, 2003; Mottonen et al. 2002; Quinn and Emery, 2003]. Thus, identifying predictive factors of remission in ERA could guide treatment strategy towards a favourable disease course and outcome.
Predictive clinical factors of remission related to RA therapy
Several studies have investigated remission rates in patients receiving antirheumatic treatments (Table 1). Baseline predictive factors of treatment response could be helpful to define a first-line treatment strategy (either an sDMARD or a bDMARD). Indeed, some of the early prognostic factors (i.e. 3 months response after drug initiation) could point to optimal monitoring of treatment response and adaptations when needed. Gossec and colleagues identified prognostic factors for remission (DAS < 1.6) in a cohort of 191 ERA patients (symptoms < 1 year) followed prospectively for 5 years [Gossec et al. 2004]. Patients were treated with sDMARDs (usually MTX, SSZ or a combination of both), and the regimen could be modified during the study according to efficacy and tolerance (biological agents were not allowed). A total of 48 patients (25.1%) fulfilled the remission criteria at the 3-year follow-up visit, and 30 (15.7%) at 3 and 5 years. They described how remission at 3 years and persistent remission at 5 years correlate with baseline clinical, laboratory, genetic and radiographic data. On univariate analysis, remission status at 3 years and 5 years was closely correlated with low baseline values for DAS, C-reactive protein (CRP) level, Ritchie Articular Index score, Stanford Health Assessment Questionnaire (HAQ) score, duration of morning stiffness, and to a lesser extent, baseline total radiological scores and RF negativity. Logistic regression analysis showed that the baseline independent variables predictive of remission were low DAS, Ritchie Articular Index score, morning stiffness duration and total radiographic score.
Overview of predictive factors of remission among baseline drug-naïve early rheumatoid arthritis patients receiving disease-modifying antirheumatic drugs.
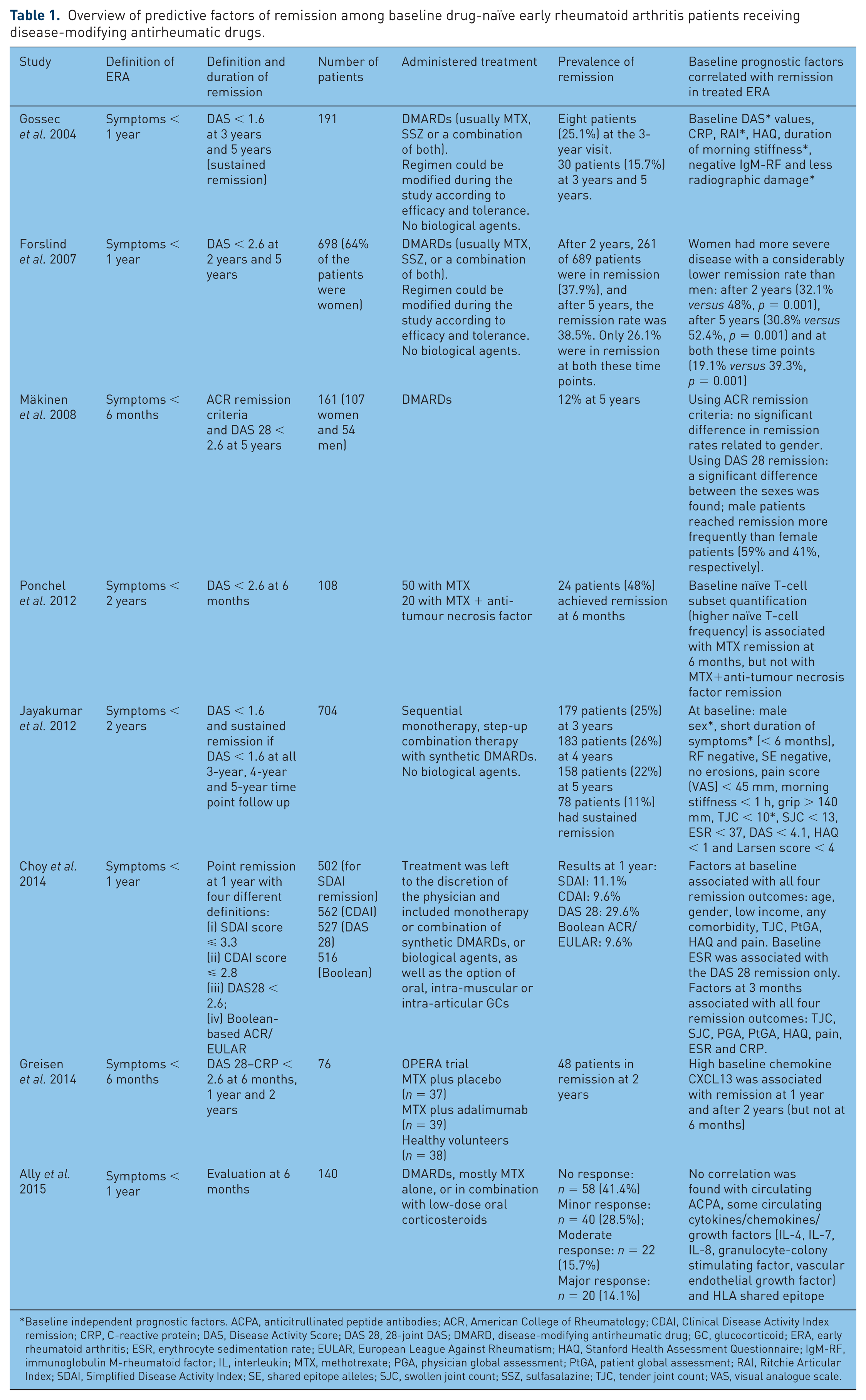
Baseline independent prognostic factors. ACPA, anticitrullinated peptide antibodies; ACR, American College of Rheumatology; CDAI, Clinical Disease Activity Index remission; CRP, C-reactive protein; DAS, Disease Activity Score; DAS 28, 28-joint DAS; DMARD, disease-modifying antirheumatic drug; GC, glucocorticoid; ERA, early rheumatoid arthritis; ESR, erythrocyte sedimentation rate; EULAR, European League Against Rheumatism; HAQ, Stanford Health Assessment Questionnaire; IgM-RF, immunoglobulin M-rheumatoid factor; IL, interleukin; MTX, methotrexate; PGA, physician global assessment; PtGA, patient global assessment; RAI, Ritchie Articular Index; SDAI, Simplified Disease Activity Index; SE, shared epitope alleles; SJC, swollen joint count; SSZ, sulfasalazine; TJC, tender joint count; VAS, visual analogue scale.
Jayakumar and colleagues evaluated prevalence and predictive factors of sustained remission in a prebiological inception cohort of RA [Jayakumar et al. 2012]. A total of 704 patients with recent onset (< 2 years) DMARD-naïve RA were monitored yearly. Point remission was defined by DAS < 1.6, and sustained remission by DAS < 1.6 at each time point (3-year, 4-year and 5-year follow up). The percentages of patients in remission at 3 years, 4 years and 5 years were 25%, 26% and 22%, respectively; 11% (n = 78) achieved sustained remission. Male sex, short duration of symptoms and less tender joints at baseline were independent predictors of sustained remission. The authors confirmed that male gender was a positive independent predictor of remission as previously described in other studies [Forslind et al. 2007; Mäkinen et al. 2008]. These patients had fewer DMARD therapies and less radiographic progression after 5 years. Moreover, this study emphasized that early introduction of DMARDs was associated with a better disease outcome, as demonstrated by Lard and colleagues who compared two cohorts (one with early treatment at 15 days and the other with delayed treatment at 123 days) [Lard et al. 2001]. After 2 years, the early treatment group had better disease outcome.
Choy and colleagues studied clinical and biological factors at baseline and 3 months to determine correlation with ERA remission at 1 year [Choy et al. 2014]. Among a cohort of ERA patients (between 6 weeks and 12 months of symptoms), they evaluated remission using four different definitions: (a) SDAI score ⩽ 3.3 (502 patients); (b) CDAI score ⩽ 2.8 (562 patients); (c) DAS 28 < 2.6 (527 patients); (d) Boolean-based ACR/EULAR clinical trial definition (516 patients). Treatment was left to the discretion of the physician and included monotherapy or a combination of sDMARDs and bDMARDs, as well as the option of oral, intra-muscular, or intra-articular GCs. Measurements at 3 months were strongly correlated with outcomes at 12 months compared with baseline variables. Factors at 3 months associated with remission were lower physician global assessment (PGA) (for all criteria used), lower pain (though not for DAS 28 remission), lower HAQ scores (not for CDAI and Boolean remission), younger age (not for CDAI remission), lower CRP (only for CDAI remission), lower erythrocyte sedimentation rate and male gender (only for DAS 28), and patient global assessment (only for Boolean remission). Not surprisingly, this study pointed out that a higher PGA measured at 3 months was consistently associated with worse remission outcome at 12 months in ERA.
Predictive biological factors of remission related to RA therapy
Characterization of the pathophysiological processes of ERA could enable the identification of biomarkers useful in guiding and personalizing treatment decisions during the window of opportunity. Chemokine CXCL13 has recently been identified as a good candidate in DMARD-naïve ERA patients, since its plasma levels were associated with joint inflammation. Greisen and colleagues examined CXCL13 plasma levels at baseline and 6 months and its association with treatment outcome after 1 year and 2 years in 76 patients with treatment-naïve ERA (symptoms < 6 months) [Greisen et al. 2014]. Patients were randomized in a double-blind clinical trial into two different treatment regimens: MTX plus placebo (n = 37) or MTX plus adalimumab (n = 39). High baseline CXCL13 in the DMARD-treated group was associated with low SDAI and visual analogue scale score at 1 year. Sustained remission after 2 years (DAS 28 CRP < 2.6) was associated with high baseline plasma CXCL13 levels. Others biomarkers, such as the receptor activator of nuclear factor kappa-B ligand, vasoactive intestinal peptide or interleukin (IL-15), may help to intensify treatment [Gonzalez-Alvaro et al. 2015].
Ally and colleagues measured circulating ACPA and a panel of circulating cytokines/chemokines/growth factors (IL-4, IL-7, IL-8, granulocyte-colony stimulating factor, vascular endothelial growth factor) at baseline and 6 months post-therapy [Ally et al. 2015]. They evaluated their correlation with response to DMARD treatment and the presence of shared epitope in a cohort of 140 ERA patients (symptoms < 12 months), without finding any of the biomarkers predicting response to therapy.
Ponchel and colleagues compared 108 drug-naïve early RA patients (symptoms < 24 months) with 100 healthy controls and found an immune deregulation of T-cell subsets among ERA patients under MTX therapy (decreased naïve T cells, lower age-adjusted Treg cells and higher inflammation-related cell frequency) [Ponchel et al. 2014]. Regarding treatment response, ACPA/age-adjusted analysis observed a higher naïve T-cell frequency (relative to the healthy controls) associated with remission in the 50 patients treated with MTX. Remission with MTX+anti-TNF (n = 20) was not found to be associated with naïve T-cell frequency. Finally, the remission rate increased from 24% (MTX monotherapy group) to 42% (MTX+anti-TNF group) for patients with reduced naïve T cells.
Predictive factors of sustained remission after stopping RA therapy
Two other studies evaluated persistent remission of the disease after discontinuation of therapy (Table 2). Van der Woude and colleagues assessed drug-free remission at 1 year in 454 ERA patients (symptoms < 2 years) from the Leiden EAC and in 895 patients from the British Early Rheumatoid Arthritis Study (ERAS) who fulfilled the ACR 1987 revised criteria for the classification of RA. They were treated with sequential monotherapy or combination therapy of sDMARDs (i.e. HCQ, chloroquine, SSZ, MTX) [van der Woude et al. 2009]. Sustained DMARD-free remission was achieved by 68 patients (15.0%) in the Leiden EAC and by 84 patients (9.4%) in the ERAS. Acute onset, short symptom duration before inclusion, low disease activity at baseline (only for ERAS), no tobacco, low radiographic damage at baseline, absence of IgM-RF, and absence of HLA shared epitope were predictive of remission. Multivariate analyses revealed symptom duration and the absence of autoantibodies (ACPA2 and IgM-RF) as independent predictors.
Overview of predictive factors of persistent remission among early rheumatoid arthritis patients after therapy discontinuation.

DAS, Disease Activity Score; DMARD, disease-modifying antirheumatic drug; EAC, Leiden Early Arthritis Clinic cohort; ERAS, British Early Rheumatoid Arthritis Study cohort.
Van der Kooij and colleagues evaluated the predictive factors of 1-year drug-free remission in ERA patients (symptoms < 2 years) [van der Kooij et al. 2009]. Initially, 508 patients were treated by four different therapeutic strategies for RA (sequential monotherapy, step-up combination therapy, initial combination therapy with prednisone, and initial combination therapy with infliximab). Patients who achieved a DAS < 1.6 for at least 6 consecutive months, while treated with monotherapy in a maintenance dose, tapered and discontinued all medication. After 4 years of continued DAS-driven treatment, 43% of patients were in clinical remission. At 4 years, 13% of all patients were still in drug-free remission. The absence of ACPA, male gender and short symptom duration were independently associated with drug-free remission.
Conclusion
The major objective in ERA patients is to reach remission at the earliest possible time point. Few studies have attempted to determine prognostic factors for remission in this population. All these studies are characterized by their heterogeneity with regard to definition of remission, time point of remission, duration of sustained remission and RA treatment. Nevertheless, we can summarize similar remission baseline prognostic factors in ERA-treated patients: clinical factors that reflect low disease activity (low DAS, Ritchie score, morning stiffness duration, and less tender joints), male gender, RF negativity and low radiographic damage. Short duration of symptoms before study inclusion is an additional and important predictive factor, as suggested by other studies [Jayakumar et al. 2012; Lard et al. 2001; van der Woude et al. 2009].
In daily practice, these simple baseline factors appeared easy to estimate and could really help clinicians in decision making: to treat early, to determine the best treatment option (sDMARDs or bDMARDs), to plan patient follow up and to early adjust treatment strategies (because a 3-month treatment response can predict later responders). Currently, biomarkers for remission are missing. Thus, there is an emergent need to provide additional tools in order to predict drug efficacy or drug-free sustained remission.
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Conflict of interest statement
The authors declare that there is no conflict of interest.