
Abstract
Background:
Rheumatoid arthritis (RA) increases the risk of premature mortality, primarily due to cardiovascular diseases (CVD). While Systematic Coronary Risk Evaluation (SCORE) and its updated version SCORE2 are used to estimate CVD risk, these tools may not adequately capture the full cardiovascular risk profile in RA patients.
Objectives:
This study aims to compare the effectiveness of SCORE2 versus SCORE in predicting the presence of carotid plaques or increased intima-media thickness (IMT), as detected by ultrasound, in RA patients.
Design:
This was a single-center cross-sectional study and included adult RA patients with moderate to severe disease who initiated treatment with Janus kinase inhibitors or anti-tumor necrosis factor inhibitors between September 2022 and April 2023.
Methods:
Both SCORE and SCORE2 were calculated for each patient. Carotid ultrasound examinations documented the presence of plaques, and IMT was measured.
Results:
A total of 122 patients were included. The mean SCORE was 2.48%, while SCORE2 was significantly higher at 4.07% (p < 0.01). SCORE identified 12 (10%) patients as high risk, while SCORE2 identified 99 (81%). Atherosclerotic plaques were present in 34% (n = 42) of participants. Traditional cardiovascular risk factors (dyslipidemia, diabetes, hypertension, and smoking) were significantly associated with ultrasound-detected risk. In 87 cases where SCORE was underestimated, 34 patients (39%) classified as low–moderate risk by SCORE were correctly reclassified as high risk by SCORE2. However, 54 cases classified as high risk by SCORE2 had normal carotid ultrasounds. The sensitivity of SCORE for predicting plaque presence was 21%, compared to 100% for SCORE2. Combining SCORE with carotid ultrasound increased the detection of high-risk patients from 10% to 38%. However, adding carotid ultrasound to SCORE2 did not increase the detection rate beyond 81%.
Conclusion:
Our findings highlight the superior performance of SCORE2 compared to SCORE in identifying RA patients with carotid ultrasound abnormalities, thus indicating a higher cardiovascular risk.
Plain language summary
Cardiovascular disease including heart disease and stroke, is a major concern for people with rheumatoid arthritis (RA), an illness that primarily causes joint pain and damage. Researchers have been using tools called SCORE and SCORE2 to guess the risk of heart disease in these patients, but these tools might not be accurate enough. Our study looked at which tool, SCORE or SCORE2, is better at predicting heart problems by examining the neck arteries using ultrasound—a safe imaging technique that uses sound waves to create pictures of the inside of your body. We included 122 adults with moderate to severe RA who were taking certain RA medicines. We calculated their SCORE and SCORE2, which estimate how likely someone is to have heart issues within the next ten years. Then, using ultrasound, we checked for plaque buildup and the thickness of their artery walls—signs that can tell us about their risk of heart disease. We found that the SCORE2 number was often higher than SCORE, which means it was suggesting a higher risk of heart disease. SCORE2 also matched the ultrasound findings better than SCORE did. While SCORE only found a high risk in about 10% of patients, SCORE2 identified a high risk in over 80%. When we looked at the ultrasounds, we saw that 34% of the patients had plaque in their arteries. Also, patients with usual heart risk factors like high cholesterol, diabetes, high blood pressure, and smoking were more likely to have risky ultrasound results. In summary, SCORE2 was better at picking out patients with signs of heart disease on the ultrasound. This suggests that using SCORE2 could help doctors better understand a patient’s risk for heart disease and possibly prevent it before it becomes more serious.
Introduction
Rheumatoid arthritis (RA) is a chronic autoimmune disease primarily characterized by joint inflammation and cartilage destruction. This condition affects millions of people worldwide, with a higher prevalence in women than in men. 1 The etiology of RA is complex and not fully understood; but it is believed to result from an interplay of genetic, environmental, and immunological factors. Beyond its well-known joint manifestations, RA has systemic implications, particularly affecting the cardiovascular system.2 –4
Patients with RA are at increased risk of premature death, largely due to cardiovascular diseases (CVD), such as myocardial infarction (coronary artery disease) and stroke. This heightened risk stems from a combination of traditional cardiovascular risk factors and chronic inflammation associated with RA.2 –5 The incidence and prevalence of CVD in RA patients vary depending on the population studied, disease subtypes, and the diagnostic methods used.4,5 Tools like the Systematic Coronary Risk Evaluation (SCORE) 6 and its updated version SCORE2 7 are commonly employed to estimate the risk of CVD. These tools consider factors such as age, gender, smoking status, systolic blood pressure, and cholesterol levels to predict the 10-year risk of fatal cardiovascular events. However, they may underestimate the actual cardiovascular risk in RA patients, indicating the need for more comprehensive evaluation methods.
Recent advances in noninvasive imaging techniques, such as vascular ultrasound, have provided valuable tools for detecting atherosclerosis. These techniques have been validated as biomarkers of CVD in both the general population and RA patients, allowing for more accurate risk classification and adjustment of CVD thresholds.8 –14 One of the most widely used and well-validated imaging methods is carotid intima-media thickness (IMT) measurement via ultrasound.8,9 Considering this, the European League Against Rheumatism (EULAR) developed specific recommendations for cardiovascular risk evaluation and management in RA patients, including a multiplication factor of 1.5 for the SCORE system and the consideration of carotid ultrasound findings. 15
Against this backdrop, our study aims to compare the effectiveness of SCORE2 with the traditional SCORE system in predicting the presence of carotid plaques or increased IMT, as detected by ultrasound, in RA patients. Through this comparison, we assess the ability of these tools to accurately identify cardiovascular risk in this patient population.
Methods
Study design and population
A cross-sectional, single-center study was conducted to evaluate the cardiovascular risk profile in adult patients diagnosed with moderate to severe RA who had initiated treatment with Janus kinase inhibitors (JAKi) or anti-tumor necrosis factor inhibitors (TNFi). Disease activity was measured following current EULAR recommendations, 16 and all patients met the ACR/EULAR classification criteria for RA. 17 Patient recruitment occurred between September 2022 and April 2023 using non-probabilistic convenience sampling, with balanced representation in both treatment groups. Subjects with other autoimmune disorders, major cardiovascular events, and/or previous carotid interventions were excluded. The study design is depicted in Figure 1. The reporting of this study conforms to the Standards for Reporting Diagnostic Accuracy (STARD) guidelines. 18

A total of 122 patients with RA were included in the study, with 61 patients receiving TNFi and 61 receiving JAKi. Patients underwent an evaluation that included a review of clinical history, cardiovascular risk assessment, tender and swollen joint count, a blood panel, and a carotid ultrasound. The evaluations were conducted by a rheumatologist who was blinded to the clinical data.
Data collection and cardiovascular risk evaluation
Upon inclusion, comprehensive data were collected from electronic medical records, including demographic information (age, gender, ethnicity), clinical parameters (duration of RA, current medications, steroid use), and traditional cardiovascular risk factors (smoking status, hypertension, dyslipidemia, and diabetes).
Participants attended a scheduled hospital visit for evaluation, which included measurements of arterial blood pressure, weight, height, and a carotid ultrasound examination. A blood test sample was drawn at least 15 days prior to the visit. Participants were also asked about their smoking habits (former smoker/smoker/non-smoker), physical activity levels, family history of early CVD (in first-degree relatives: <55 years in men and <65 years in women), and previous history of cardiovascular risk factors.
High blood pressure was defined based on a prior diagnosis and current pharmacological treatment with blood pressure measured according to standard guidelines. Diabetes mellitus was diagnosed following ADA criteria, and dyslipidemia was defined as total cholesterol above 220 mg/dL in 2 or more measurements, serum triglycerides over 150 mg/dL, or current use of lipid-lowering agents.
Both SCORE 6 and SCORE2 7 risk stratification tools were used to estimate the overall cardiovascular risk for each participant. For patients over 70 years of age, the SCORE2-OP calculator was applied. In accordance with EULAR recommendations, the SCORE values (but not the SCORE2 values) were multiplied by 1.5 to account for the elevated cardiovascular risk in RA patients. 15
Carotid ultrasound examination
All participants underwent a detailed carotid ultrasound examination conducted by an experienced evaluator trained in vascular ultrasound, who was blinded to the clinical data (C.C.F.). The ultrasound examination involved B-mode imaging of the arterial wall, color Doppler flow analysis, and visualization of the common, internal, and external carotid arteries. The presence, absence, and number of atherosclerotic plaques were documented.
According to the Mannheim Consensus, a plaque was defined as any focal structure protruding into the arterial lumen by at least 0.5 mm, being 50% larger than the surrounding IMT value, or having a thickness greater than 1.5 mm from the media-adventitia to the intima-lumen interface. 19
The Esaote MyLab™ 9XP (Esaote, Genoa, Italy) with a linear high-resolution transducer (L4-15) was used for the ultrasound, and carotid IMT was measured using Esaote’s QIMT (Quality Intima Media Thickness) software.
Statistical analysis
Frequencies and percentages were reported for categorical variables. Differences between groups were analyzed using Pearson’s nonparametric Chi-square test for nonparametric data, with Fisher’s exact test applied for 2 × 2 tables. Continuous variables were compared using factorial ANOVA, with multiple comparisons adjusted using the Bonferroni correction. For composite indices, factorial ANOVAs were adjusted for sex, age, drug exposure duration, and RA progression years. These models were implemented using general linear models with robust estimations to manage potential violations of model assumptions. Marginal means and 95% confidence intervals were reported.
To evaluate the concordance between the methods, several approaches were used:
Pearson correlation and the Kappa Index to measure agreement between different measurement instruments or evaluators.
A Bland–Altman plot to assess the behavior or differences between methods.
ROC curve for each index relative to the Risk/No risk classification obtained via ultrasound. The optimal cutoff value, determined by maximizing Youden’s index (sensitivity + specificity −1), provided the best approximation of actual risk classification.
Statistical analyses were performed using IBM SPSS Statistics 26 (IBM, New York, USA). A significance level of 5% (α = 0.05) was applied.
Results
Demographic and clinical profile
A total of 122 patients were included, with 61 receiving anti-TNF treatment and 61 receiving JAKi. Baseline characteristics and demographics are summarized in Table 1. The mean duration of RA among the patients was 11.43 years, with a standard deviation (SD) of 7.58 years (25th percentile: 5 years; 75th percentile: 16 years). Disease activity, measured by the DAS28 score at the initial assessment, had a mean value of 4.00 (SD 1.13; 25th percentile: 3.15; 75th percentile: 4.85).
Demographic and clinical characteristics of RA patients.
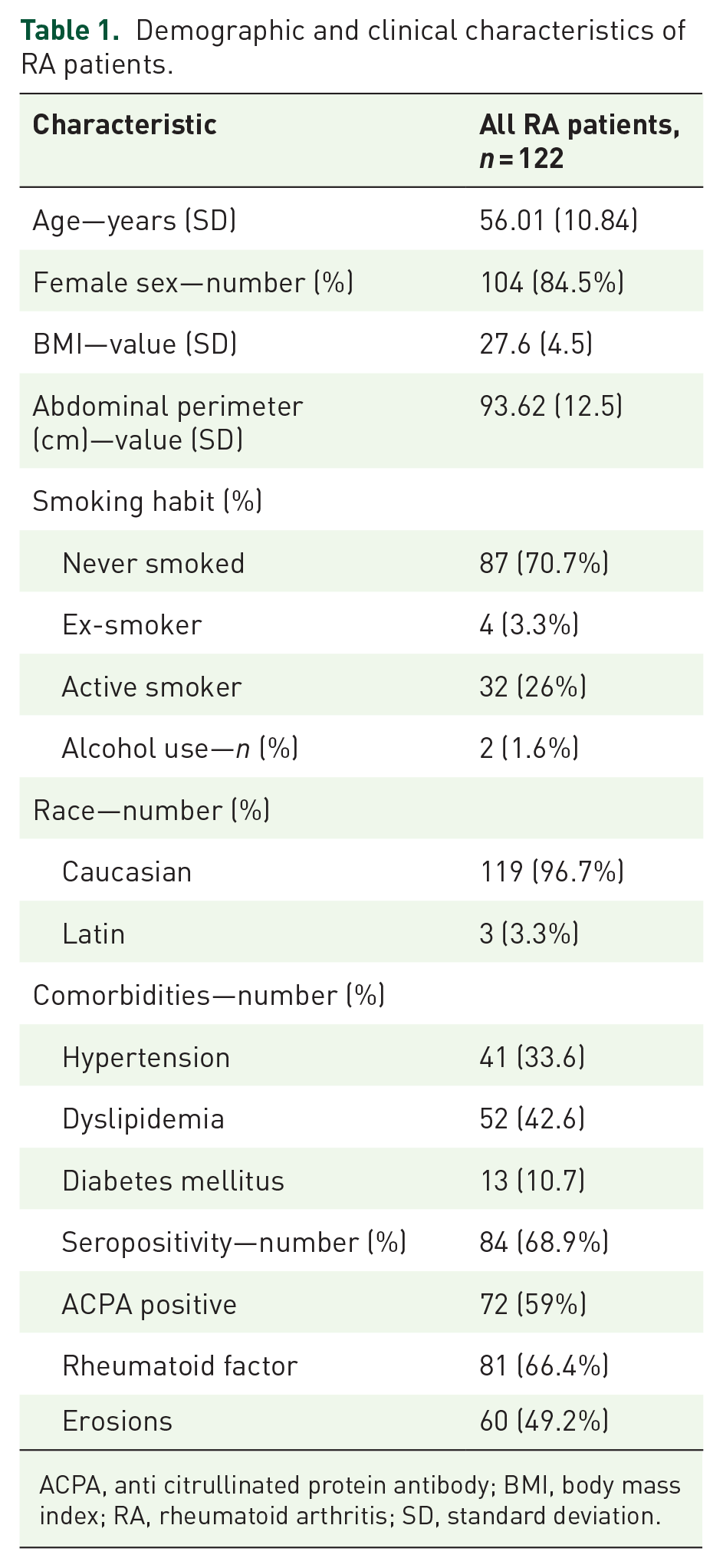
ACPA, anti citrullinated protein antibody; BMI, body mass index; RA, rheumatoid arthritis; SD, standard deviation.
In terms of concomitant medication, 31 patients (25%) were taking steroids—17 (28%) in the JAKi group and 14 (23%) in the anti-TNF group. Four patients (3%) were on 2.5 mg of prednisone at the time of the analysis, while 27 (22%) were on 5 mg. In addition, 35 patients (29%) were receiving treatment for high blood pressure, 43 (35%) for dyslipidemia, and 13 (11%) for diabetes mellitus. Some patients were diagnosed with hypertension, dyslipidemia, and/or diabetes after the study procedures.
Drug exposure duration differed between the two treatment groups. Patients in the JAKi group had an average drug exposure of 29 months (SD 17), while the TNFi group had an average exposure of 7 months longer. Furthermore, 31 patients (25%) were receiving steroid therapy at the time of the study.
SCORE and SCORE2 results and concordance analysis
The SCORE and SCORE2 risk calculators yielded moderate to high estimates for the 10-year risk of fatal cardiovascular events. The mean SCORE was 2.48%, whereas SCORE2 was significantly higher at 4.07% (p < 0.01). For SCORE2, there were significant differences in the incidence of classical cardiovascular risk factors (dyslipidemia, diabetes, hypertension, and smoking), with risk increasing as more factors were present. In the low to moderate risk range, SCORE reflected a higher incidence of diabetes and hypertension, whereas SCORE2 captured these and other factors like dyslipidemia and smoking more accurately.
SCORE identified 12 (10%) patients as high risk, while SCORE2 detected 99 (81%). Among the patients classified as low risk by SCORE, two were reclassified as high risk by SCORE2. Of the 108 categorized as moderate risk by SCORE, 71% were reclassified as high risk by SCORE2. Out of the 10 patients identified as high risk by SCORE, 4 were also classified as high risk by SCORE2, while the remaining 6 were reclassified as very high risk. Of the two patients identified as very high risk by SCORE, one was confirmed by SCORE2, while the other was reclassified as high. SCORE and SCORE2 results are shown in Figure 2. Sensitivity and specifity comparison are shown in Figure 3.

Comparative risk stratification using the two scoring systems.

ROC curves illustrate the performance of SCORE and SCORE2 in predicting cardiovascular risk according to ultrasound results.
The nonparametric Spearman correlation indicated a moderate correlation between SCORE and SCORE2 (Rho = 0.584, p < 0.001). However, a Wilcoxon test for paired samples yielded a p-value of 0, indicating a significant difference between the two methods. The scatter plot between the two methods, available in the Supplemental Material, demonstrated that neither the linear fit (R2 = 0.195) nor the quadratic fit (R2 = 0.298) were optimal for the relationship between these tools. A Bland–Altman plot showed a bias (mean of the differences) of −1.594, with the regression line indicating a constant and proportional bias between the two methods.
When low and moderate categories were combined to align with SCORE2 classifications, the Kappa concordance index between the two systems was notably low (0.070, p < 0.001), with 87 cases (71% of the sample) showing discordant risk levels. These discrepancies were most pronounced when SCORE classified patients as high risk while SCORE2 classified them as very high risk or vice versa, which occurred in 77% of such cases.
Carotid ultrasound findings
Atherosclerotic plaques were detected in 34% (n = 42) of participants, with no significant differences between the JAKi and TNFi groups (p = 0.703). Bilateral plaques were observed in 13% (n = 16) of patients. Plaques were present in the right carotid artery in 10% (n = 12) and in the left carotid artery in 11% (n = 14) (Table 2).
Carotid ultrasound findings.

IMT, intima-media thickness; RA, rheumatoid arthritis; SD, standard deviation.
The presence of traditional cardiovascular risk factors (dyslipidemia, diabetes, hypertension, and smoking) was significantly associated with ultrasound-detected risk, except for alcohol consumption, which showed no significant association. Specifically, dyslipidemia was significantly more frequent in patients with ultrasound-identified risk (43%) compared to those without it (29%, p < 0.001). Similarly, diabetes mellitus was more common among those at risk according to ultrasound (19%) versus those not at risk (6%, p = 0.036). Hypertension was also significantly associated with ultrasound-estimated risk, with 56% of those at risk having hypertension compared to 22% of those not at risk (p < 0.001). Smoking demonstrated a significant, although less pronounced, association with ultrasound-identified risk, with 35% of individuals classified as at-risk being smokers compared to 18% of those not at risk (p = 0.033). By contrast, alcohol consumption did not show a significant relationship with ultrasound-estimated risk (p = 0.660).
Predictive value of SCORE systems
Among the 87 cases in which SCORE underestimated cardiovascular risk, 34 cases (39% of the 87) were classified as a low–moderate risk by SCORE but presented high risk according to the carotid ultrasound (33 with plaque presence, 3 with IMT >0.9 mm, and 34 with one or both). These 34 patients were correctly classified by SCORE2. However, there were 54 cases where patients were classified as high risk by SCORE2 but had normal carotid ultrasounds. Therefore, the sensitivity of SCORE in predicting plaque was 21% compared to 100% for SCORE2. Specificity could not be calculated, as a normal ultrasound does not necessarily imply low cardiovascular risk.
To evaluate whether the addition of carotid ultrasound improves the detection of risk cases compared to using SCORE alone, the analysis focused on low–moderate risk cases:
SCORE detected 12 high-risk cases, while carotid ultrasound detected an additional 34 patients (31% of the 110 classified as low risk by SCORE).
SCORE2 detected 99 high-risk cases, and carotid ultrasound did not identify any additional high-risk cases in the population classified as low risk by SCORE2.
Thus, using SCORE in combination with carotid ultrasound increased the detection of high-risk cases patients from 10% to 38%. However, using SCORE2 in conjunction with carotid ultrasound did not increase the detection of high-risk cases beyond what SCORE2 alone identified, with the figure remaining at 81%.
Further analysis using ROC curves between the two scoring systems and the risk classification estimated by carotid ultrasound revealed an area under the curve (AUC) of 0.740 (95% confidence interval (CI): 0.645–0.835) for SCORE and 0.886 (95% CI: 0.826–0.946) for SCORE2. The Hanley and McNeil test for comparing AUCs showed that they were statistically different (Z = −2.885, |z| > 1.96, p < 0.05), indicating that SCORE2 is a significantly better classifier than SCORE.
The cutoff point that maximized Youden’s index (sensitivity + specificity −1) for SCORE was 2.25, yielding a sensitivity of 0.674 and specificity of 0.797. For SCORE2, the optimal cutoff point was 4.5, with a sensitivity of 0.814 and specificity of 0.848.
Thus, for patients with a SCORE value above 2.25, the system correctly detected 67% of the risks identified by ultrasound. Conversely, for values below 2.25, it correctly classified 80% of non-risk cases. For SCORE2, a value above 4.5 correctly identified 81% of the risks, while a value below 4.5 correctly classified 85% of non-risk cases.
Discussion
Our study compared the predictive capabilities of the SCORE and SCORE2 risk calculators in patients with RA, specifically in detecting signs of cardiovascular risk assessed by carotid ultrasound, including carotid plaques and/or increased IMT. This investigation was motivated by the need to improve cardiovascular risk assessment in RA patients, where cardiovascular events are the leading causes of morbidity and mortality.1 –5,11 –15 Our findings suggest that SCORE2 is a more effective tool than SCORE in predicting CVD, as evidenced by carotid plaques and IMT in RA patients.
In reviewing the demographics, it is notable that our study included a representative sample of RA patients typically seen in clinical settings. The average age was 56 years, and women constituted 85% of the cohort, consistent with the established gender distribution of RA. 1 Most participants were Caucasian, and a quarter were smokers, aligning with known behavioral risk factors for CVD.12 –14,20,21 Disease activity, as measured by the DAS28 score, averaged 4, indicating moderate activity range, with variability as shown in SD. A notable 25% of patients were receiving steroid treatment, a therapy associated with cardiovascular risks, though this figure is lower than in other published cohorts. Overall, the characteristics of our cohort are consistent with findings from other studies evaluating cardiovascular risk factors in RA patients.12 –14,20,21
Clinical decision-making for the cohort followed EULAR recommendations, aiming to achieve remission through a “treat-to-target” approach. 16 We specifically included patients treated with JAKi or anti-TNF agents, allowing us to evaluate cardiovascular risk in those receiving modern RA therapies known to influence cardiovascular health. This selection focused on individuals diagnosed with moderate to severe RA, a group at higher risk of cardiovascular complications due to more aggressive disease.
SCORE2 offers several advantages over SCORE, including the use of larger derivation and validation cohorts, the estimating of both fatal and non-fatal cardiovascular risk, improved risk discrimination by adjusting for age, and consideration of different risk regions. 22 Previous studies in the general population have shown that SCORE2 reclassifies a significant number of patients from low-risk categories, as determined by SCORE, into higher-risk.23 –25 We observed similar findings in our RA cohort, where many patients whose risk might have been underestimated by SCORE required more intensive cardiovascular management based on their SCORE2 results.
SCORE2 was significantly higher than SCORE, even after applying the multiplicator factor recommended by EULAR. 15 This suggests that SCORE2 may be either more precise or overestimate cardiovascular risk. A detailed analysis showed that SCORE2 is particularly sensitive when all cardiovascular risk factors (dyslipidemia, diabetes mellitus, hypertension, and smoking) are present, while SCORE relies more heavily on diabetes and hypertension. Interestingly, in the low to moderate risk range, SCORE classified more patients with diabetes and hypertension than SCORE2, possibly reflecting an underestimation by SCORE of dyslipidemia and smoking, while overestimating the risk associated with hypertension and diabetes.
Overall, SCORE identified only 10% of our sample as high risk, compared to 81% with SCORE2. Notably, one of the two patients classified as low risk by SCORE was reclassified as high risk by SCORE2. This significant discrepancy between the two tools, along with the correlation tests failing to demonstrate a strong correlation between them, highlights the limitations of SCORE in accurately capturing cardiovascular risk. The Bland–Altman analysis showed that SCORE2 measured 1.594 units higher than SCORE on average. In addition, the Kappa concordance index (0.070) between the two methods indicates poor agreement in risk classification, suggesting that SCORE may systematically underestimate cardiovascular risk.
In the context of RA, only one similar study, by Ferraz-Amaro et al., found a high correlation between the SCORE, SCORE2, and carotid ultrasound findings, particularly for IMT and carotid plaque presence. Like our study, Ferraz-Amaro et al. observed that SCORE2 classified a significantly higher number of patients as high or very high risk compared to SCORE. 20
Regarding carotid ultrasound findings, 34% of our sample showed carotid plaques, with a distribution emphasizing the importance of bilateral examination, as only 13% had bilateral plaques. Ultrasound findings correlated well with traditional cardiovascular risk factors, except for alcohol consumption, reported in only three cases. Dyslipidemia, in particular, was strongly associated with ultrasound-detected risk. These findings underscore the importance of considering traditional risk factors in patients with ultrasound-detected cardiovascular risk, as the presence of such risk factors was significantly higher in patients identified as at risk by ultrasound. By contrast, alcohol consumption did not show a significant correlation in our study. The elevated carotid IMT and a significant proportion of patients with atherosclerotic plaques further reinforce the elevated cardiovascular risk in this population.
In a recent study, Bao et al. evaluated the impact of subclinical carotid atherosclerosis on the performance of SCORE2 in a Swedish cohort of over 4000 healthy participants. They found that adding carotid plaques or IMT to SCORE2 significantly improved its predictive ability for cardiovascular events. Their study highlighted that SCORE2 tends to overestimate 10-year cardiovascular risk in individuals without carotid plaques but underestimates it in those with carotid plaques. Incorporating carotid ultrasound could help refine risk predictions and further personalize preventive therapies, even for high-risk patients. 26
While our findings are promising, there are limitations to this study. Its cross-sectional design precludes causal inferences, and the single-center nature may limit the generalizability of our results. In addition, we were unable to calculate the specificity of SCORE2 from our dataset, which requires further investigation. A longitudinal study design would allow for a more comprehensive understanding of SCORE2’s predictive capabilities by tracking actual cardiovascular events over time, offering insights into the temporal relationship between risk factors and outcomes in RA patients.
Conclusion
The most significant finding of our study is that, in patients with carotid ultrasound abnormalities, 28% of cases had their cardiovascular risk underestimated by SCORE, while SCORE2 correctly identified these patients as high risk. Moreover, although 54 patients classified as high risk by SCORE2 had normal carotid ultrasounds, this does not necessarily imply a false positive, as a normal ultrasound does not equate to low cardiovascular risk. These patients may still be at elevated risk, warranting careful monitoring and follow-up. Importantly, none of the patients classified as low risk by SCORE2 showed ultrasound evidence of CVD, underscoring SCORE” reliability in correctly classifying low-risk individuals. The combination of SCORE with carotid ultrasound significantly improved the detection of high-risk patients, while adding carotid ultrasound to SCORE2 did not further enhance its predictive value. These findings have practical implications for the management of RA patients since incorporating SCORE2 into clinical practice may identify patients with higher cardiovascular risk without a carotid ultrasound examination. Anyway, given that some patients classified as high risk by SCORE2 had no carotid abnormalities, future research should investigate whether other biomarkers or imaging modalities can improve risk prediction.
In summary, our study underscores the superior accuracy of SCORE2 over SCORE in detecting elevated cardiovascular risk in RA patients, particularly those with carotid ultrasound abnormalities. The integration of advanced imaging techniques, such as carotid ultrasound, with cardiovascular risk scores, offers a more comprehensive approach to risk stratification, potentially improving the outcomes for patients with RA.
Supplemental Material
sj-pptx-1-tab-10.1177_1759720X241302667 – Supplemental material for SCORE2 is superior to SCORE in predicting the presence of carotid plaques and intima-media thickness in rheumatoid arthritis patients: a cross-sectional study using carotid ultrasound
Supplemental material, sj-pptx-1-tab-10.1177_1759720X241302667 for SCORE2 is superior to SCORE in predicting the presence of carotid plaques and intima-media thickness in rheumatoid arthritis patients: a cross-sectional study using carotid ultrasound by Cristina Campos Fernández, Jorge Juan Fragío Gil, Roxana González Mazarío, Pablo Martínez Calabuig and José Andrés Román Ivorra in Therapeutic Advances in Musculoskeletal Disease
Footnotes
Acknowledgements
We would like to extend our deepest gratitude to the patients who participated in this study for their valuable time and cooperation. We also wish to express our sincere appreciation to the entire staff of the Rheumatology Department at Hospital General Universitario de Valencia. Special thanks to the nurses and administrative personnel whose dedication made the data collection and patient care processes smoother.
Declarations
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.