
Abstract
The risk of cardiovascular morbidity and mortality is increased in rheumatoid arthritis. The classical cardiovascular risk factors, including smoking, hypertension, dyslipidaemia, insulin resistance and diabetes mellitus, obesity and physical inactivity do not appear to explain the excess cardiovascular risk in rheumatoid arthritis, although they do contribute, albeit in a different way or to a lesser extent, to rheumatoid arthritis in comparison with the general population. A very important link between rheumatoid arthritis and cardiovascular disease is inflammation as it plays a key role in all stages of atherosclerosis: from endothelial dysfunction to plaque rupture and thrombosis. It also has an influence on and accentuates some traditional cardiovascular risk factors, such as dyslipidaemia, obesity and insulin resistance. To date, the exact pathophysiologic mechanism by which this relation between cardiovascular disease and rheumatoid arthritis can be explained is not completely clear. Cardiovascular risk management in rheumatoid arthritis is mandatory. Unfortunately, the way this should be done remains a point of discussion. In this review issues regarding cardiovascular risk in rheumatoid arthritis and its management will be addressed, according to evidence presented in the latest studies and our own experience-based opinion.
Introduction
The risk of cardiovascular (CV) disease and mortality is increased in rheumatoid arthritis (RA). A substantial number of observational studies varying in factors such as the cohort type, disease duration and length of follow up, has produced a wide range of incidence rates for CV events and mortality. Some studies show a more than doubled risk which is comparable to the CV risk in diabetes mellitus (DM) [del Rincon et al. 2001; Peters et al. 2009]. Other studies show a more modest increased risk [Gabriel et al. 1999; Goodson et al. 2005a]. However, when the results of the most relevant studies are pooled the risk of CV events and mortality seems to be approximately 50% higher in RA patients compared with the general population [Avina-Zubieta et al. 2008, 2012]. To date, the exact pathophysiologic mechanism by which this relation between CV disease and RA can be explained is not completely clear. So the most important questions regarding this problem remain: ‘How can this increased risk be explained?’, ‘When does it start?’, ‘How can we predict the CV risk in RA?’ and, most important, ‘How can we prevent CV morbidity and mortality in RA?’.
In this review we will answer these questions according to evidence presented in the latest studies and according to our own experience-based opinion.
What causes the excess CV risk?
To be able to decrease the excess CV risk in RA it is essential to know what causes this problem. One of the reasons why this puzzle has not yet been solved is that there are many pathophysiological mechanisms involved that influence each other. First of all, the traditional CV risk factors, which cause and predict CV morbidity and mortality in the general population but also in people with DM, seem to be equally or only slightly more prevalent in the RA population. Some risk factors, such as smoking, even play an important role in the onset of RA, however, traditional CV risk factors alone do not explain the higher CV risk in RA [Chung et al. 2012; Gonzalez et al. 2008]. At present, RA and atherosclerosis are both regarded as inflammatory-driven diseases and this appears to be the most important reason why these two diseases coincide [Sattar et al. 2003]. There is much evidence that endorses this hypothesis. For instance, the inflammatory and immunological processes that occur in atherosclerotic plaques are very similar to those in inflammatory synovitis and markers of inflammation, as C-reactive protein (CRP), predict CV disease not only in healthy men and women but also in RA patients [Goodson et al. 2005b; Pasceri and Willerson, 1999; Ridker et al. 1998]. Furthermore, indicators of more severe disease and more systemic inflammation in RA, such as decreased functional capability, the presence of extra-articular manifestations, longer disease duration and seropositivity, are also associated with higher CV risk [Gabriel, 2008; Goodson et al. 2002; Soderlin et al. 1998; Turesson et al. 2007].
There are many ways by which RA-related inflammation may lead to atherosclerosis. Inflammation seems to play a key role in all stages of atherosclerosis: from endothelial dysfunction to plaque rupture and thrombosis [Libby, 2006]. Inflammation also has an influence on and accentuates some traditional CV risk factors, such as dyslipidaemia, obesity and insulin resistance (IR), as they behave differently in the RA population with regard to CV risk than in the general population [Gonzalez et al. 2008; Liao and Solomon, 2013; Sattar et al. 2003]. The link between synovitis and atherosclerosis is illustrated in Figure 1.

An illustration of the pathways and cytokines by which synovitis can contribute to the formation of an atherosclerotic plaque and eventually CV events.
Another factor that may link atherosclerosis to RA is a common genetic background. An increasing number of studies report gene polymorphisms that are associated with a higher risk of CV risk in rheumatoid artritis [Cavagna et al. 2012]. Human leucocyte antigen shared epitope (HLA-DRB1) is a typical example of a gene that seems associated with CV mortality in RA [Farragher et al. 2008]. Together with the question of what causes the relationship between RA and atherosclerosis arises the question of when does CV risk increase? When genetics, traditional CV risk factors and autoimmune pathways are involved it could be possible that the CV risk is already increased at the time of diagnosis or even years before the first clinical symptoms appear. Actually, there is accumulating (circumstantial) evidence that CV risk is increased before the clinical onset of RA. There are studies that show that endothelial dysfunction and the first signs of atherosclerosis are already present in patients with recent-onset RA [Sodergren et al. 2010]. Most of the studies measuring carotid intima-media thickness (cIMT) in newly diagnosed RA patients versus controls found cIMT levels to be significantly elevated in the RA group and to be correlated with systemic inflammatory markers and disease severity markers [Kerola et al. 2012]. A meta-analysis looking at cIMT in established RA patients also showed statistically significant higher cIMT levels in RA versus controls but no relation with disease duration [van Sijl et al. 2012]. Also dyslipidaemia is already present in rheumatoid-factor-positive persons who later develop RA [Myasoedova et al. 2010; van de Stadt et al. 2012; van Halm et al. 2007]. One population-based cohort study reported an increased risk of coronary heart disease and myocardial infarction two years prior to RA diagnosis using the ACR 1987 criteria [Maradit-Kremers et al. 2005a]. There are some more recent studies that reported increased CV risk and mortality early in the RA disease course [Franklin et al. 2010; Holmqvist et al. 2010; Naz et al. 2008; Sodergren et al. 2010]. Altogether, it appears that CV risk already starts to increase as soon as the first signs of autoimmunity and inflammation appear which is often a few months to years prior to the actual RA diagnosis and increases further during disease progression as the inflammatory burden accumulates.
The role of traditional CV risk factors
Although the classical CV risk factors, including smoking, hypertension, dyslipidaemia, DM, obesity and inactivity do not seem to explain the excess CV risk in RA, they do contribute, albeit in a different way or to a lesser extent in RA in comparison with the general population. The following sections and Table 1 summarize and interpret data from recent studies on individual traditional CV risk factors and their contribution to CV risk in RA specifically.
Studies examining the prevalence of several traditional CV risk factors in RA patients.
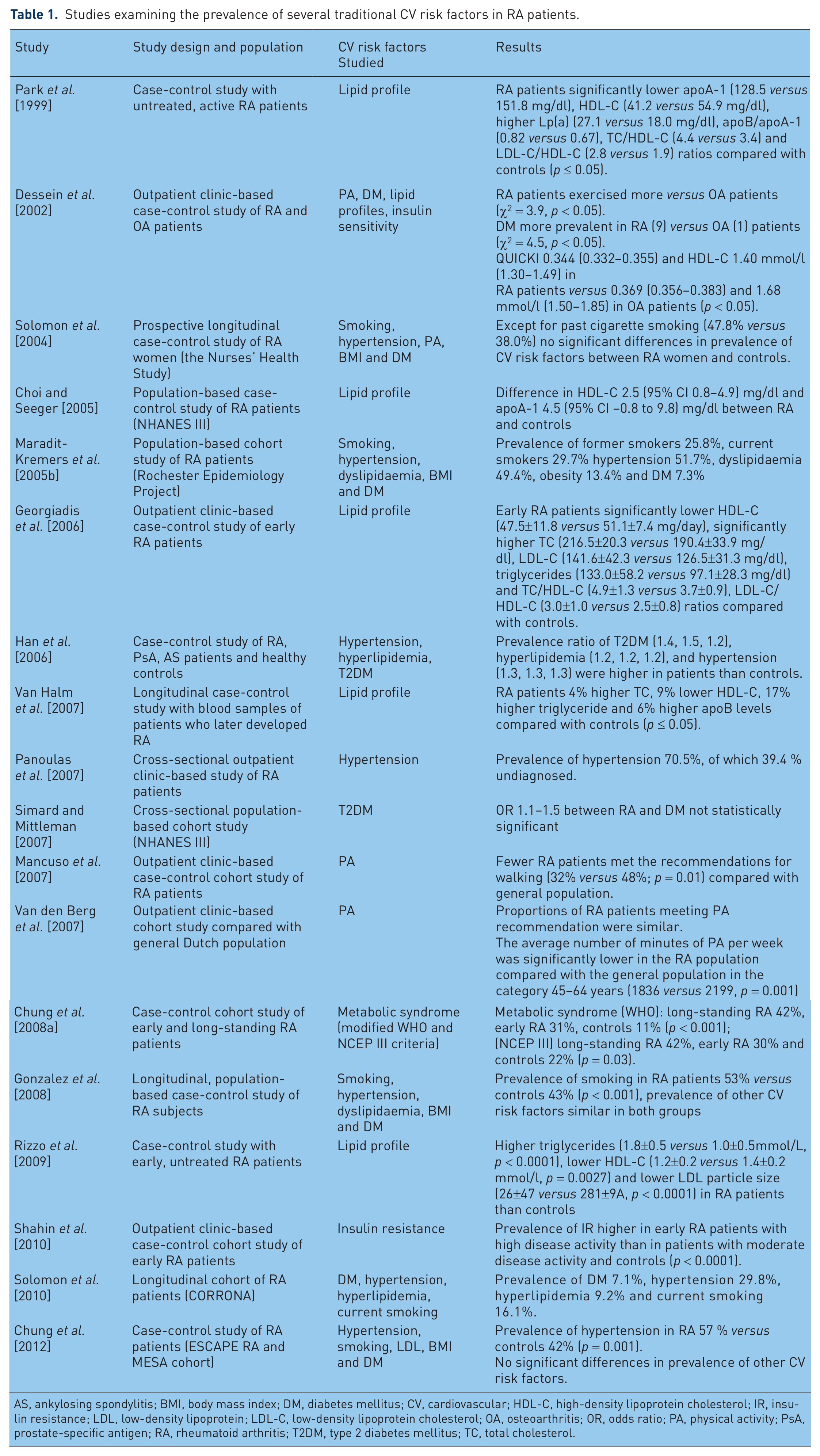
AS, ankylosing spondylitis; BMI, body mass index; DM, diabetes mellitus; CV, cardiovascular; HDL-C, high-density lipoprotein cholesterol; IR, insulin resistance; LDL, low-density lipoprotein; LDL-C, low-density lipoprotein cholesterol; OA, osteoarthritis; OR, odds ratio; PA, physical activity; PsA, prostate-specific antigen; RA, rheumatoid arthritis; T2DM, type 2 diabetes mellitus; TC, total cholesterol.
Smoking
As already mentioned, cigarette smoking is classified not only as a predisposing factor for CV events but also for RA, particularly rheumatoid-factor-positive RA [Costenbader et al. 2006; Costenbader and Karlson, 2006; Heliovaara et al. 1993]. For rheumatologists this alone should be a trigger to advise every newly diagnosed RA patient who smokes to quit, apart from the notion that smoking probably also has an adverse influence on RA disease severity and prognosis [Saag et al. 1997].
Hypertension
Whether hypertension is more common in RA than in the general population has not been elucidated yet, because reports are contradictory [Liao and Solomon, 2013]. However, one of the most recent studies found a significant increased prevalence of hypertension in RA patients versus controls [Chung et al. 2012]. The reported prevalence of hypertension in RA varies substantially, depending on the study population, sample size and on the definition of hypertension used in the different studies [Panoulas et al. 2008b]. This does not mean that hypertension has no impact on CV risk in RA. Hypertension is a very common problem in the general as well as the RA population and is still underdiagnosed and undertreated, particularly in young RA patients [Panoulas et al. 2007]. There is no real evidence that the current disease-modifying antirheumatic drugs (DMARDs) have a beneficial effect on blood pressure. On the contrary, there are DMARDs and other drugs used for the treatment of RA that can induce high blood pressure, such as leflunomide, cyclosporine, glucocorticoids and the nonsteroidal anti-inflammatory drugs (NSAIDs) [Panoulas et al. 2008b; Van Doornum et al. 2006]. This means adequate blood pressure control and treatment could be of great influence to the CV risk in the RA population.
Dyslipidaemia
Abnormal cholesterol levels, particularly high levels of total cholesterol, triglycerides, low-density lipoprotein (LDL) and low levels of high-density lipoprotein (HDL) are strongly associated with CV disease. LDL particles can transport cholesterol in the arterial wall, which leads to atherosclerosis, while HDL particles are able to remove cholesterol from the arterial wall. Most studies which have investigated cholesterol levels in RA have found lower HDL levels and as a result an unfavourable atherogenic profile (total cholesterol/HDL cholesterol ratio) compared with healthy controls, even 10 years before the onset of RA [Choi and Seeger, 2005; Georgiadis et al. 2006; Myasoedova et al. 2010; Park et al. 1999; van de Stadt et al. 2012; van Halm et al. 2007; Yoo, 2004]. The data on total cholesterol, LDL and triglyceride levels are not so conclusive [Nurmohamed, 2007]. However, many studies demonstrate a very similar lipid pattern as seen in several other inflammatory conditions, indicating a profound influence of inflammation on lipid profile in RA [Khovidhunkit et al. 2000; Rizzo et al. 2009]. All in all, when LDL and HDL composition are also taken into account, the lipid profile in active RA tends to be highly proatherogenic [Hahn et al. 2008].
Diabetes mellitus and insulin resistance
There is a lot of data that points to an association between RA and IR, which is very likely caused by inflammation, as many studies showed a correlation between IR and disease activity or markers of inflammation such as CRP and erythrocyte sedimentation rate (ESR) [Chung et al. 2008a, 2008b; Dessein et al. 2002; Dessein and Joffe, 2006; Shahin et al. 2010; Svenson et al. 1987, 1988].
Several studies have investigated the prevalence of type 2 diabetes mellitus (DM2) in RA patients, expecting to find a positive association. However, apart from two studies, which found a modest significantly higher occurrence of DM2 in RA patients [Han et al. 2006; Solomon et al. 2010], all other studies found no significantly increased prevalence [Gabriel et al. 1999; Liao et al. 2009; Simard and Mittleman, 2007; Solomon et al. 2004]. This seems quite remarkable given the fact that IR often preceeds DM2 and indicates that further research is needed to clarify this issue. However, both IR and DM appear to be independent CV risk factors in patients with RA, as also seen in the general population [Chung et al. 2008a; del Rincon et al. 2005; Dessein et al. 2003; Maradit-Kremers et al. 2005b; Shahin et al. 2010].
Obesity
Obesity, specifically central or abdominal obesity, characterized by a large waist circumference, is a risk factor for CV disease in the general population [Mathieu et al. 2010]. The adipose tissue, especially abdominal visceral fat, may contribute to low-grade inflammation by producing pro-inflammatory cytokines such as tumour necrosis factor (TNF)-α and interleukin (IL)-6 [Despres and Lemieux, 2006].
Surprisingly, most studies reported a higher CV mortality in RA patients with a low body mass index (BMI) (<20 kg/m2) compared with patients with a higher BMI (≥30 kg/m2), although the prevalence of adiposity did not differ in RA compared with the general population [Chung et al. 2012; Escalante et al. 2005; Gabriel, 2008; Gonzalez et al. 2008; Kremers et al. 2004; Maradit-Kremers et al. 2005b; Rall and Roubenoff, 2004; Walsmith and Roubenoff, 2002]. This discrepancy can be explained by a phenomenon called rheumatoid cachexia, a condition characterized by decreased lean muscle mass and increased adiposity, which leads to an abnormal body composition in RA [Rall and Roubenoff, 2004; Summers et al. 2008; Walsmith and Roubenoff, 2002]. One study clearly demonstrated that RA patients had a different distribution of abdominal fat and especially visceral fat, despite no significant differences in BMI or waist circumference compared with non-RA controls [Giles et al. 2010]. Loss of lean muscle mass in RA seems associated with TNF-α [Roubenoff et al. 1994; Walsmith et al. 2004]. In conclusion, the chronic inflammatory state in RA seems to create an abnormal body composition characterized by muscle wasting and increasing visceral fat, whereby BMI can be perfectly normal and thereby less reliable when it comes to predicting CV risk.
Physical activity
RA patients tend to be less physically active due to disease symptoms, such as joint pain and stiffness and fear of aggravating their disease [Mancuso et al. 2007; Metsios et al. 2008; Roubenoff et al. 2002; van den Berg et al. 2007]. Exercise can prevent CV disease and it has a positive impact on all of the individual CV risk factors, such as adiposity, dyslipidaemia, IR and DM, hypertension and possibly even inflammation [Bensimhon et al. 2006; Blair et al. 1993; Kasapis and Thompson, 2005; Kelemen et al. 1990; Wallberg-Henriksson et al. 1998]. Physical inactivity has been associated with CV risk in RA [Metsios et al. 2009]. This could mean that stimulating RA patients to be more physically active could have even more effect on CV risk in RA patients than in healthy persons.
Cardiovascular risk scores: are they useful in RA?
Large longitudinal cohort studies performed in the 20th century have discovered which factors most adequately predict the risk for CV disease in the general population resulting in several CV risk estimation models, such as the Framingham Risk Score (FRS), the Reynolds Risk Score (RRS) and the Systematic Coronary Risk Evaluation (SCORE) [Conroy et al. 2003; D’Agostino et al. 2008; Ridker et al. 2007]. Although these CV risk assessment tools are based on the whole population, including people with chronic diseases, they often cannot be used for accurately predicting CV risk in these specific populations. A very good example of such a group is DM patients. They have a higher CV risk and therefore special risk scores, such as the UK Prospective Diabetes Study (UKPDS) score, have been developed [Stevens et al. 2001]. In the Netherlands, another way of calculating the excess CV risk of DM is being used. Instead of a separate risk model for DM, the SCORE risk model is adjusted by adding 15 years to the actual age of DM patients, because the excess CV risk in DM seems to match that of healthy persons 15 years older, the so-called ‘vascular age’ [Booth et al. 2006].
The same problem is true for RA patients: their vascular age also seems to be similar to that of healthy persons 10–15 years older and there are actually studies that have shown a CV risk that matches the CV risk of DM patients [Lindhardsen et al. 2011; Peters et al. 2009; Stamatelopoulos et al. 2009; van Halm et al. 2009].
The European League Against Rheumatism (EULAR) has set up guidelines with recommendations regarding CV risk management in RA and advised to add a multiplier of 1.5 to conventional risk assessment tools for estimating CV risk in RA patients, based on the evidence present at that time [Peters et al. 2010].
However, to date there is no evidence that this multiplier or any other CV risk estimation model or adjustment method accurately predicts CV risk in RA. Future research should therefore focus on developing accurate CV risk prediction models for the RA population.
Cardiovascular disease prevention in RA: what (not) to do?
Tight disease control
As stated above, CV risk in RA cannot be explained by traditional CV risk factors alone and is largely increased because of chronic systemic inflammation. Therefore, tight and sustained control of RA disease activity is necessary to effectively prevent CV disease development in RA. This starts by early recognition and diagnosis of RA followed by immediate aggressive treatment to diminish the grade of inflammation as quickly as possible to prevent damage in not only the joints but also the arteries. Although we do not know when the excess CV risk exactly starts to arise, it is likely at the same time signs of inflammation occur and it could even be sooner than that. The treatment goal should be remission, since even low-grade inflammation and especially cumulative (low-grade) inflammation can eventually cause atherosclerosis and CV events [Provan et al. 2011]. Indirectly, effective treatment can result in improved physical activity, subsequently leading to a decreased risk of obesity, diabetes, hypertension and in the end CV disease. Effective treatment of RA can therefore substantially reduce CV risk in RA, however some medications, such as corticosteroids and NSAIDs, often used in RA are known to enhance CV risk.
DMARDs
Methotrexate (MTX), the cornerstone DMARD in the treatment of RA, has been shown to reduce all-cause CV morbidity and mortality in RA and appears to have cardioprotective properties [Choi et al. 2002; Marks and Edwards, 2012; Prodanovich et al. 2005; van Halm et al. 2006; Westlake et al. 2010]. However, there are studies that found an association between MTX use and hyperhomocysteinemia, an independent CV risk factor, which could be explained by a depletion of folic acid levels [Haagsma et al. 1999; Hornung et al. 2004]. Hence, supplemental use of folic acid is advised to restore normal homocysteine levels [Morgan et al. 1998; Prodanovich et al. 2005]. Data on the effect of other DMARDs on CV morbidity and mortality are very scarce. Only two studies have looked at CV events and DMARD use and reported reductions in CV morbidity with sulfasalazine and leflunomide [Naranjo et al. 2008; van Halm et al. 2006]. There are, however, more studies that have looked at the effect of DMARDs on CV risk factors, such as DM, metabolic syndrome and dyslipidaemia. Hydroxychloroquine use in RA has been associated with improvement of lipid profiles, a reduced risk of developing DM and moreover exerts antithrombotic effects [Atzeni et al. 2010; Wasko et al. 2007]. Both leflunomide and cyclosporine can induce high blood pressure, hence are not DMARDs of first choice in patients with hypertension or increased CV risk [Kvien et al. 2002; Rozman et al. 2002].
Biologicals
TNF blockers are very effective drugs for RA and multiple other inflammatory diseases. Current available data show a positive but weaker effect of TNF blockers on CV disease occurrence, compared to MTX [Barnabe et al. 2011; Westlake et al. 2011]. Whether TNF blockers really exert a smaller CV risk reduction than MTX or the difference can be explained by other factors, such as study population and disease severity, is not clear yet. Altogether, it seems that TNF blockers have a positive influence on several CV risk factors, such as IR, HDL composition and endothelial function [Peters et al. 2012].
Tocilizumab (TCZ), an IL-6 inhibitor, also seems to have beneficial effects on endothelial function, despite the increase of total and LDL cholesterol. No data of the effect of TCZ on hard CV endpoints are available yet. The same counts for abatacept, a selective T-lymphocyte costimulation modulator and rituximab, a B-lymphocyte depleting agent. Since all of these medications are very effective at reducing inflammation, perhaps all of these biologicals exert CV risk reduction in RA patients who respond to treatment with these immunomodulating medication. However, this remains to be proven in the future.
Glucocorticosteroids
Glucocorticosteroids (GCs) are very powerful anti-inflammatory drugs and are commonly used as treatment for RA. They have strong anti-inflammatory properties which could mean that GCs have anti-atherosclerotic effects [Boers et al. 2003].
However, in the general population, therapeutic doses of oral GCs (≥7.5 mg/day) have been associated with increased CV disease and all-cause mortality [Souverein et al. 2004; Wei et al. 2004]. There are several population-based cohort studies that have looked at the effect of GC use at hard CV endpoints, such as myocardial infarction and cerebrovascular disease in RA patients with conflicting results [Avina-Zubieta et al. 2011, 2013; Ruyssen-Witrand et al. 2011]. Although data are not all congruent, GCs tend to have deleterious effects on several risk factors, as lipid profile, glucose tolerance, IR, blood pressure and abdominal obesity in RA [Avina-Zubieta et al. 2011, 2013; Dessein et al. 2004; Hafstrom et al. 2007; Panoulas et al. 2008a; Ruyssen-Witrand et al. 2011; Toms et al. 2008]. For now it remains unclear whether GC use in RA has a beneficial or detrimental effect on CV risk, since no randomized controlled trials of glucocorticoids versus placebo in RA patients have been conducted. In addition, confounding by indication probably plays an important role in the outcomes of studies that have looked at the effect of GCs on CV mortality and morbidity [Davis et al. 2005]. The effect of GCs on the CV risk probably depends on several factors, such as the population of RA patients, the circumstances and way it is used, the dosage and treatment duration [Davis et al. 2007; Mazzantini et al. 2010]. When GCs are used to treat highly active RA, during a short period as a ‘bridging therapy’, with an oral dosage as low as possible or via an intramuscular or intra-articular injection and preferably in patients who do not have DM or hypertension, the CV benefit/risk ratio could perhaps be positive. It is advisable to check blood pressure and glucose levels before start and during GC treatment, especially if the patient has DM or hypertension and GCs are prescribed for a longer period.
NSAIDs
NSAIDs are often used as pain medication in many rheumatic diseases, including RA. NSAIDs and also cyclooxygenase-2 inhibitors (COXIBs) are known to increase the risk for hypertension and myocardial infarction [Bolten, 2006; Farkouh and Greenberg, 2009; Kearney et al. 2006a; Morrison et al. 2007; Schjerning Olsen et al. 2011; Trelle et al. 2011; van der Linden et al. 2009]. Moreover, a population-based Danish case-control study found that the use of NSAIDs was associated with a twofold increased risk of venous thromboembolism (VTE) [Schmidt et al. 2011]. The different NSAIDs seem to have different effects on CV risk and especially naproxen seems less harmful than the rest of the NSAIDs [Kearney et al. 2006b; Solomon et al. 2008; Trelle et al. 2011]. Although there are not many studies that looked specifically at the effect of NSAIDs and COXIBs on CV risk in RA, one study showed no negative effects on CV mortality in patients with inflammatory polyarthritis [Goodson et al. 2009].
In summary, although evidence regarding the effects of NSAIDs on CV risk in RA is not conclusive, most data point to a negative influence, therefore the use of NSAIDs should be avoided if possible, at least in RA patients with known renal dysfunction, hypertension, heart failure or high CV risk. If NSAID use is unavoidable, blood pressure and renal function must be checked regularly and naproxen is probably the first choice. Furthermore, the combination of NSAIDs and aspirin is not advisable, since NSAIDs may impair the antiplatelet function of aspirin [Catella-Lawson et al. 2001; Hudson et al. 2005].
CV risk management
Although traditional CV risk factors may not explain the excess CV risk in RA, they do play an important role and should not be neglected when it comes to CV risk prevention. Since there are no CV risk assessment models for RA specifically, the national guidelines for CV risk management can best be used to determine CV risk and treatment, as advised by the EULAR guidelines for CV risk management in RA [Peters et al. 2010]. To adjust for the excess CV risk in RA, a multiplication factor of 1.5 is recommended in the presence of two of the following criteria: disease duration of more than 10 years, rheumatoid factor and/or anti-cyclic citrullinated peptide antibodies (anti-CCP) positivity or the presence of extra-articular manifestations. However, this multiplication factor needs validation, as there is indirect evidence that this multiplication factor improves CV risk estimation in RA. The same applies for the three above-mentioned criteria that are taken up in the EULAR recommendations to filter the RA patients that presumably have the highest CV risk. Although cumulative disease and therefore disease duration probably enhances CV risk, this does not mean CV risk treatment should only be started after 10 years of disease duration [Crowson and Gabriel, 2011]. Whether anti-CCP or rheumatoid factor positivity are real risk factors for CV disease or simply associated with CV disease because they are also associated with disease severity remains to be investigated. This means CV risk could be underestimated in RA patients who do not qualify to two of the three criteria. In the Dutch multidisciplinary guidelines for CV risk management RA has been recognized as an independent CV risk factor, equal to DM, and CV risk estimations are calculated using the SCORE formula, adjusted for data from Dutch studies. For both DM and RA patients, 15 years are added to the actual age of all patients to express the excess CV risk burden. However, this is also based on expert opinion and indirect evidence and, hence, needs to be validated.
When it comes to CV risk treatment in RA the first step is lifestyle adaptation. The two key messages for the rheumatologist to patients are to stop smoking and to get physically active [Stavropoulos-Kalinoglou et al. 2012]. The second step involves the determination of the CV risk profile, including at least assessment of blood pressure and lipid profile. On the basis of these and other easily accessible data (e.g. age, sex, family history of premature CV disease, etc.) and the aid of calculators such as Framingham and SCORE, the 10-year CV risk of a particular RA person can be calculated. Primary prevention involving treatment with statins and/or antihypertensives is only necessary if this 10-year CV risk is above a certain value. For instance, in the Netherlands this would be a 10-year risk of CV morbidity or mortality of 20% or more, based upon a Dutch version of the SCORE.
Unfortunately, thus far no intervention trials with statins or antihypertensives and CV disease prevention in RA have been published. Based on data from epidemiological studies and post hoc subgroup analyses of large, secondary CV prevention trials, the effects of statins on cholesterol levels in RA patients appear to be at least equivalent to the effects of statins in the general population [Rollefstad et al. 2012; Semb et al. 2011, 2012]. In contrast, one recently published population-based longitudinal study found that the effectiveness of statins varied in chronic diseases, including RA, and tended to be less effective than in the rest of the population [Sheng et al. 2012b]. There are, however, numerous other studies that show beneficial effects of statins and angiotensin-converting enzyme (ACE) inhibitors on CV risk in RA [Charles-Schoeman et al. 2007; Flammer et al. 2008; Hermann et al. 2005; Maki-Petaja et al. 2007; Sheng et al. 2012a; Van Doornum et al. 2004]. Actually, in RA the effects of cardioprotective agents might be more pronounced as the pleiotropic effects of statins, ACE inhibitors and angiotensin blockers include anti-inflammatory properties [Abud-Mendoza et al. 2003; Dagenais and Jamali, 2005; McCarey et al. 2004; Tikiz et al. 2005].
Randomized controlled intervention trials are necessary to assess the actual effect of statins, ACE inhibitors and other lifestyle intervention strategies on CV risk in RA.
Conclusion
RA patients are more susceptible to developing CV disease and therefore both tight disease control and also CV risk management in these patients is mandatory. An important issue is who is responsible: is it the rheumatologist or the primary care physician? Currently, this varies from country to country and even from practice to practice. Obviously, someone should take responsibility and this should be locally agreed upon.
Adequate CV risk management requires efforts from both the responsible doctor, whether this is the rheumatologist or the primary care physician, and the patient. A RA patient, who smokes, should quit smoking to decrease their CV risk substantially. However, it is up to the responsible doctor to point this out to the patient and to provide adequate support. This means periodically (annually) screening for CV risk factors, such as high blood pressure, blood glucose and cholesterol levels, but also to monitor physical activity, diet, waist/hip circumference and BMI. CV risk screening takes time, but is not difficult and can also be performed by adequately trained nurses. On the other hand, CV risk treatment and lifestyle advice takes a lot more time and effort and cannot be easily done by nurses practitioners, since it often involves prescribing medication. This requires innovative thinking and investing and is probably only feasible when rheumatologists work together with specialized nurses and other specialists, such as primary care physicians, internal doctors and cardiologists.
Since specific CV risk prediction models are not yet available for RA and the question remains which RA patients present the highest CV risk, it is advisable to start by screening all RA patients, preferably at an early stage of the disease and to treat them according to the existing national CV risk management guidelines. The enhanced CV risk in RA can be expressed by a multiplier 1.5, as advised by the EULAR guidelines. Meanwhile, research will have to continue to try to discover the exact pathophysiological mechanism behind the relation of atherosclerosis and rheumatic inflammatory diseases, so that adequate CV risk formulas can be developed for this group of patients. Moreover, large randomized controlled trials are needed to determine whether lifestyle interventions, statins and antihypertensives work as well or even better in rheumatic patients, but also to once and for all give clarity regarding the effects on CV risk of GCs, NSAIDs and other medications that are often prescribed to RA patients.
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Conflict of interest statement
The author declares that there are no conflicts of interest.