
Abstract
Background:
A strong association has been demonstrated between serum transthyretin (TTR) levels and autoimmune diseases. However, there is limited information regarding the role of serum TTR in patients with primary Sjögren’s syndrome (pSS).
Objectives:
This study was designed to explore the association between serum TTR and disease activity in patients with pSS.
Design:
This study was a retrospective observational study.
Methods:
This study included 84 patients with pSS and 135 age- and sex-matched healthy controls retrospectively, and collected data were analyzed. The European League Against Rheumatism (EULAR) Sjögren’s Syndrome Disease Activity Index (ESSDAI) and Clinical ESSDAI (ClinESSDAI) scores were used to assess the disease activity in patients with pSS.
Results:
Serum TTR levels were significantly lower in patients with pSS than those in healthy controls (181.9 ± 69.2 vs 241.8 ± 48.9 mg/L, p < 0.001). Serum TTR levels were significantly and negatively correlated with ESSDAI (r = −0.385, p < 0.001) and ClinESSDAI (r = −0.340, p = 0.002) scores in patients with pSS, respectively. Multivariable linear regression analysis showed that serum TTR was significantly associated with ESSDAI (Beta = −0.248, p = 0.017) and ClinESSDAI (Beta = −0.215, p = 0.036) scores in patients with pSS, respectively.
Conclusion:
Serum TTR is a potential marker for assessing disease activity in patients with pSS, which may contribute to the clinical management of pSS.
Introduction
Primary Sjögren’s syndrome (pSS), which also belongs to a systemic rheumatic disease, is an autoimmune disease characterized by exocrine gland dysfunction with systemic manifestations.1,2 Evaluation of disease activity is essential for the clinical therapy and management of patients with pSS. 3 Methods to evaluate disease activity in pSS include serological markers, ultrasound assessments, and stimulated salivary flow; however, these approaches have their limitations. 4 In recent years, efforts have been made to explore more available indicators to assess the disease activity in patients with pSS. Thus, some emerging laboratory biomarkers can be used as part of our routine clinical practice.
Transthyretin (TTR), also known as prealbumin, is a small protein synthesized by the liver that has been used as a laboratory biomarker of malnutrition. 5 TTR is also considered clinically to be an acute-phase response protein. 6 In the past few years, there has been a strong association between TTR and autoimmune diseases such as rheumatoid arthritis, ankylosing spondylitis, and systemic sclerosis.7–9 However, to the best of our knowledge, information regarding the role of serum TTR in patients with pSS is limited. As such, this study aimed to investigate the association between serum TTR levels and disease activity in patients with pSS.
Methods
Patients and controls
This study retrospectively included 84 patients with pSS from the Affiliated Hospital of Youjiang Medical University for Nationalities between March 2016 and May 2023. pSS was diagnosed based on American-European Consensus Group criteria. 10 Patients with pSS who had acute infection, hepatic disease, diabetes mellitus, thyroid dysfunction, malignant tumors, and other autoimmune diseases were excluded. A total of 135 age- and sex-matched healthy individuals who underwent health checkup at the same hospital were retrospectively included as controls. The study conformed to the Strengthening the Reporting of Observational Studies in Epidemiology statement. 11
Data collection
The following data were collected from electronic medical records: (i) sex, age, height, and weight; (ii) comorbidities, medication history, and clinical manifestations; (iii) laboratory test results including anti-Sjögren’s syndrome A (Anti-SSA) antibody, anti-Sjögren’s syndrome B (Anti-SSB) antibody, complement C3, complement C4, immune globulin (Ig) A, IgG, IgM, C-reactive protein (CRP), alanine aminotransferase (ALT), aspartate aminotransferase (AST), total protein (TP), creatinine (Cr), and TTR. Body mass index (BMI) was calculated by dividing weight in kilograms by height in meters squared.
Disease activity assessments
The European League Against Rheumatism (EULAR) Sjögren’s Syndrome Disease Activity Index (ESSDAI) and the Clinical ESSDAI (ClinESSDAI) were used to assess the disease activity in patients with pSS.12,13 The assessment of ESSDAI includes 12 domains; each domain is divided into 3–4 levels according to the activity levels, which are scored as 0 (no activity), 1 (low activity), 2 (moderate activity), or 3 (high activity). The score for each domain was obtained by multiplying the activity levels by the domain weight, and the final score was the sum of all domain scores. 12 As for the development of the original ESSDAI, the ClinESSDAI comprises all ESSDAI domains except the biological domain with the adjustment for weights of the remaining domains. 13
Statistical analysis
Continuous variables are expressed as mean ± standard deviation or median (interquartile range) according to whether the continuous variables were normally distributed. Categorical variables are expressed as frequency (percentages). Differences in the categorical variables between the two groups were compared using Chi-square test or Fisher’s exact test when appropriate. The differences in continuous variables between the two groups were compared using Student’s t-test or Mann–Whitney U test, as appropriate. Correlations between the continuous variables were analyzed using the Spearman or Pearson correlation test, according to data distribution. Multivariable linear regression analysis was used to identify potential associations with the dependent variable. Differences with p < 0.05 were considered to be statically significant. Statistical analyses were performed using SPSS version 25.0 (IBM Corporation, Armonk, NY, USA).
Results
Characteristics of patients with pSS and healthy controls
The characteristics of the patients with pSS and healthy controls are summarized in Table 1. Serum TTR levels were significantly decreased in patients with pSS compared with healthy controls (181.9 ± 69.2 vs 241.8 ± 48.9 mg/L, p < 0.001). However, there were no significant differences in sex, age, BMI, ALT, AST, TP, and Cr between patients with pSS and healthy controls (all p > 0.05).
The characteristics of patients with pSS and healthy controls.
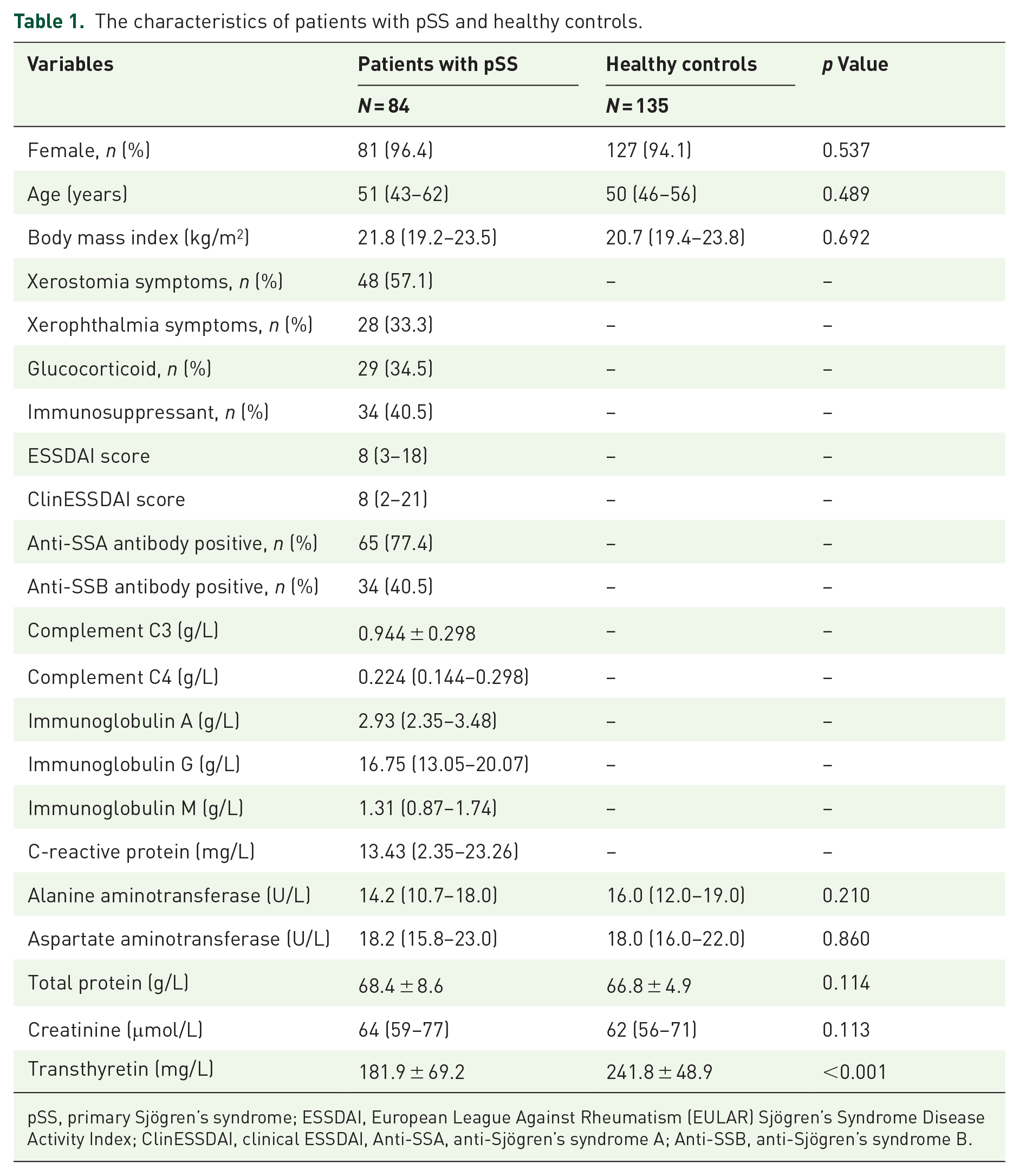
pSS, primary Sjögren’s syndrome; ESSDAI, European League Against Rheumatism (EULAR) Sjögren’s Syndrome Disease Activity Index; ClinESSDAI, clinical ESSDAI, Anti-SSA, anti-Sjögren’s syndrome A; Anti-SSB, anti-Sjögren’s syndrome B.
Correlation between serum TTR levels and disease parameters in patients with pSS
Among the patients with pSS, we found that serum TTR levels were significantly and negatively correlated with CRP (r = −0.398, p < 0.001) and IgG (r = −0.261, p = 0.016) and that serum TTR levels were significantly and positively correlated with BMI (r = 0.278, p = 0.010) in patients with pSS. Notably, serum TTR levels were significantly and negatively correlated with ESSDAI (r = −0.385, p < 0.001) and ClinESSDAI (r = −0.340, p = 0.002) scores in patients with pSS, respectively. However, serum TTR levels were not significantly correlated with age, complement C3, complement C4, IgA, IgM, ALT, AST, TP, and Cr in patients with pSS (all p > 0.05).
Multivariable linear regression analysis between serum TTR levels and disease activity in patients with pSS
In the two multivariable linear regression models where sex, age, BMI, glucocorticoid use, immunosuppressant use, IgG, and CRP were served as adjusted variables, and serum TTR levels were used as dependent variables, as shown in Tables 2 and 3. Multivariable linear regression analysis revealed that serum TTR remained significantly association with ESSDAI (Beta = −0.248, p = 0.017) and ClinESSDAI (Beta = −0.215, p = 0.036) scores in patients with pSS, respectively. The two multivariable linear regression models also indicated that serum TTR was significantly associated with BMI (Beta = 0.198, p = 0.042; Beta = 0.201, p = 0.041, respectively) and CRP (Beta = −0.330, p = 0.001; Beta = −0.335, p = 0.001, respectively) in patients with pSS.
Multivariable linear regression analysis shows the association between serum TTR and ESSDIA score in patients with pSS.

ESSDIA, European League Against Rheumatism (EULAR) Sjögren’s Syndrome Disease Activity Index; pSS, primary Sjögren’s syndrome; TTR, transthyretin.
Multivariable linear regression analysis shows the association between serum TTR and ClinESSDAI score in patients with pSS.

ClinESSDAI, clinical ESSDAI; ESSDIA, European League Against Rheumatism (EULAR) Sjögren’s Syndrome Disease Activity Index; pSS, primary Sjögren’s syndrome; TTR, transthyretin.
Discussion
This study investigated the serum TTR levels in patients with pSS. The biological mechanisms by which decreased serum TTR is associated with disease activity are poorly understood; however, proinflammatory cytokines may play an important role in the association between serum TTR levels and disease activity in patients with pSS. The pSS is an autoimmune disease characterized by systemic chronic inflammation, which is reflected by the imbalances of cytokines in local glands and systemic blood, and proinflammatory cytokines are upregulated in the salivary glands, saliva, and serum of patients with pSS. 14 Peripheral plasma interleukin-1β (IL-1β) levels are significantly elevated in patients with pSS compared with healthy controls.15,16 The number of tumor necrosis factor-α (TNF-α) and IL-1β secreting cells is significantly higher in patients with pSS than in controls, which points to the pathogenic impact of TNF-α and IL-1β in pSS. 17 Hulkkonen et al. 18 suggested that increased plasma IL-6 levels were related to specific clinical manifestations of pSS. It has been reported that the elevated salivary levels of IL-6 also are significantly associated with pSS. 19 Importantly, increased serum TNF-α and IL-6 levels have been demonstrated to be associated with ESSDAI in patients with pSS.20,21 Obviously, increased levels of proinflammatory cytokines are associated with the pathological mechanisms of pSS.
Acute-phase reactants are proteins whose serum concentrations significantly change during inflammation. 6 It is widely accepted that TTR is a negative acute-phase reaction protein because its synthesis is inhibited in inflammatory states. 22 Inflammatory signaling is a potent inhibitor of visceral protein synthesis. 23 Acute-phase reaction proteins are regulated by proinflammatory cytokines from the systemic circulation or local cell populations, such as IL-1β, IL-6, and TNF-α.6,24 IL-1β, IL-6, and TNF-α are the primary mediators of gene expression of acute-phase reaction proteins. 25 Acute-phase reaction proteins, including TTR, are important substances produced by the liver under acute and chronic inflammatory conditions. 6 Although TTR is an acute-phase reaction protein, the elevated proinflammatory cytokines, such as IL-1, IL-6, and TNF-α, can inhibit TTR synthesis in the liver, thereby reducing TTR levels in the peripheral circulation. 6 This evidence would hence suggest that with increased disease activity, the elevated production of proinflammatory cytokines may inhibit TTR synthesis in patients with pSS.
Several lines of evidence have demonstrated significantly decreased TTR levels in patients with rheumatoid arthritis.26–28 However, Ni et al. 7 found that serum levels of TTR levels were significantly increased in patients with early rheumatoid arthritis compared with healthy controls, and that serum TTR levels in late RA had no significant difference compared with healthy controls. Monu Agnihotri P et al. 29 reported significantly higher plasma TTR levels in rheumatoid arthritis than in healthy controls. Moreover, in other autoimmune diseases, significantly decreased serum prealbumin levels have been observed in patients with more severe systemic sclerosis, 9 serum TTR levels have been found to be significantly decreased in patients with ankylosing spondylitis compared with healthy controls, 8 and significantly reduced plasma TTR levels have been detected in patients with systemic lupus erythematosus compared with healthy controls. 30 In our study, we observed lower serum TTR levels in patients with pSS than in healthy controls. In summary, considering the contradictory results for the levels of TTR in patients with autoimmune diseases, we speculate that differences in disease course, disease severity, and medication use may be important reasons. Our study also revealed a significant negative association between serum TTR and CRP levels in patients with pSS. Similarly, a significant negative association between serum prealbumin and CRP levels has been reported in patients with rheumatic musculoskeletal diseases. 31
Serum TTR is a common nutrient marker in addition to being an inflammatory biomarker; poor nutritional status significantly reduces serum TTR levels. 5 BMI is a physiological parameter used to mirror nutritional status. 32 Unsurprisingly, we observed a significant positive correlation between serum TTR and BMI in patients with pSS. Given that nutritional status may affect serum TTR levels, after adjusting for BMI in the multivariable regression analysis, we still observed that serum TTR levels were significantly associated with ESSDIA and ClinESSDAI scores in patients with pSS, indicating that the association between serum TTR levels and disease activity is independent of nutritional status in patients with pSS.
Although the present study provides an interesting role of serum TTR in patients with pSS, several underlying limitations should be noted. First, the sample size was small. Second, the associations between serum TTR and proinflammatory cytokines, such as IL-1β, IL-6, and TNF-α, were not evaluated in patients with pSS. Third, serum TTR levels were not measured in patients with pSS who achieved clinical remission after treatment.
In conclusion, serum TTR levels were significantly lower in patients with pSS than in healthy controls and significantly negatively correlated with both ESSDIA and ClinESSDAI scores of pSS patients. These findings suggest that serum TTR is a potential marker for the evaluation of disease activity in patients with pSS, providing insights that could enhance the clinical management of pSS.