
Abstract
Aims:
To investigate the long-term survival of patients with primary Sjögren’s syndrome (pSS) in China.
Methods:
Patients with pSS who fulfilled the 2002 American–European Consensus Group classification criteria were prospectively enrolled from 2004 to 2011. Their baseline clinical, laboratory, and therapeutic data were collected. The primary endpoint was all-cause death by January 2018. The standard mortality ratio (SMR) was calculated by comparing with age-matched and sex-matched mortality data of the general population. Kaplan–Meier curves were obtained by time-to-event analysis. Univariate and multivariate Cox hazards regression analyses were performed to identify risk factors for mortality.
Results:
A total of 1054 patients were enrolled and 834 patients were followed up for a median of 94.8 months, with 48 confirmed deaths. The total SMR was 3.63 [95% confidence interval (CI) 2.60–4.66]. The 3-, 5-, and 10-year survival rates were 98.4%, 97.5%, and 92.9%, respectively. Infection, malignancy, and respiratory failure were the top three causes of mortality. We identified male sex [hazard ratio (HR) = 3.00, 95% CI 1.23–7.31], age at diagnosis ⩾50 years of age (HR = 7.69, 95% CI 3.01–19.62), thrombocytopenia (HR = 1.93, 95% CI 1.01–3.72), and interstitial lung disease (HR = 5.96, 95% CI 2.24–15.82) as the independent prognostic factors of death.
Conclusions:
The mortality rates of Chinese patients with pSS are higher than those of the general population. Male patients of elder age at diagnosis complicated with thrombocytopenia and interstitial lung disease might be suggestive for poorer survival and require closer follow up.
Introduction
Primary Sjögren’s syndrome (pSS) is a systemic autoimmune disease characterized by exocrinopathy, with a prevalence of 0.16–0.77%.1,2 Patients with pSS usually present with dry eyes, dry mouth, parotid enlargement and fatigue, and 30% of patients also have systemic involvement such as arthritis, nephritis, and vasculitis. In addition, patients with pSS may suffer from troublesome complications such as lymphoma, especially non-Hodgkin lymphoma (NHL). 3 It has been reported that patients with pSS have a 15–20 times higher risk of developing NHL than the general population due to long-term B-cell activation. 4
Although pSS is a chronic benign disease, the symptoms can seriously affect patients’ quality of life and the complications can be life-threatening. Thus, it is important to understand the prognosis of pSS. Several studies have investigated the outcomes of pSS. Previous studies have reported that the standardized mortality ratio (SMR) of patients with pSS is comparable with that of the general population.5–7 However, several recent studies from Spain, Korea, and Turkey found that the SMR of patients with pSS is markedly higher than that of the general population, ranging from 1.61 to 4.66.8–10 Therefore, there is no consensus on whether the mortality rate increases in patients with pSS. The survival rates found in a Spanish study with 1045 patients with pSS at 5, 10, 20, and 30 years were 96%, 90%, 81%, and 60%, respectively. 8 Besides, cardiovascular disease (CVD), infection, and malignancy are the leading causes of pSS deaths. 11 The risk factors associated with increased mortality in patients with pSS are not consistent among studies. Brito-Zeron et al. reported that a baseline European League Against Rheumatism (EULAR)-SS Disease Activity Index (ESSDAI) score ⩾14 was associated with overall mortality, 8 while other studies have variably suggested that male sex, cryoglobulinemia, low complement levels, malignancy, and vasculitis are poor prognostic markers.7,12
China has a large number of patients with pSS due to a huge population base. However, as yet, there is no prospective prognostic study of the Chinese patients. Several genome-wide association studies (GWAS) have suggested that Han Chinese patients with pSS exhibit unique risk loci such as general transcription factor IIi (GTF2I) and IKAROS family zinc finger 1 (IKZF1), indicating that there may be some differences in the pathogenesis and clinical features of pSS among different ethnicities.13,14 Our group previously analyzed 573 patients with pSS retrospectively and found there are differences in the geographic variation of prognosis. The results showed that pulmonary arterial hypertension (PAH), interstitial lung disease (ILD), liver dysfunction and high IgM levels were associated with higher mortality. 15 However, this study may have limitations because most patients included in this study were inpatients in a severe condition. Thus, it is necessary to verify these results in a larger prospective cohort to better understand the prognosis of Chinese patients with pSS.
This study prospectively followed up 1054 patients with pSS nationwide and aimed to analyze the long-term prognosis of the patients with pSS in China, including SMRs, causes of death, survival rates, and risk factors for mortality.
Methods
Study cohort
Patients with pSS who visited Peking Union Medical College Hospital from October 2004 to December 2011 and met the 2002 American-European Consensus Group (AECG) classification criteria were enrolled in the cohort. The diagnosis was confirmed by two rheumatologists. The exclusion criteria included having chronic hepatitis C virus (HCV) or HIV infection, previous lymphoproliferative diseases and other systemic autoimmune diseases. Patients without further follow-up data were excluded. This study was approved by the Ethics Committee of Peking Union Medical College Hospital (Approval number: S-225). Written informed consent was obtained from all participants.
Data collection
The time of recruitment (baseline) was defined as the time of pSS diagnosis confirmed based on the 2002 AECG classification criteria. At baseline, we collected demographic information and medical history and performed physical examination, laboratory evaluations, and diagnostic tests for pSS (ocular tests, parotid scintigraphy, and salivary gland biopsy). Data collected at baseline included age, sex, time of onset of pSS symptoms, clinical features, laboratory features, comorbidities, and treatment regimens. ILD was confirmed as the presence of characteristics of fibrotic changes on chest high-resolution computed tomography (HRCT) and as restrictive lung function impairment [forced vital capacity (FVC), and diffusing capacity of carbon monoxide (DLco) <80% of predicted]. Liver involvement was considered in patients with elevated liver enzymes without other possible reasons other than pSS. Skin vasculitis was considered in patients with urticarial vasculitis, or diffuse purpura, or ulcers related to vasculitis. Peripheral neuropathy was considered in patients with neuropathic symptoms and was confirmed by electromyography or nerve conduction studies, and the diagnosis was confirmed by two neurologists.
Follow-up and outcomes
The survival status in the patients with pSS was checked in January 2018. The study end-point was death from any cause. Death and cause of death were recorded and reported in the database based on the medical records in our hospital and telephone tracing of patients.
Statistical analysis
Quantitative data are described as the means and standard deviations. Non-quantitative data are described as counts and percentages. Continuous variables were compared using the Student t test or Mann–Whitney U test. Categorical variables including the proportions were compared using the chi-square test or Fisher exact test. Cumulative probabilities of survival were calculated using the Kaplan–Meier estimator. Further comparisons were performed using a log-rank test. All-cause mortality was used for survival statistics. Follow-up time was calculated from the date of diagnosis. Time-to-event analysis for death was presented as Kaplan–Meier curves. The SMR and corresponding 95% confidence intervals (CIs) were estimated by comparing observed deaths in the pSS cohort or subgroups of patients with pSS with expected deaths based on age-matched and sex-matched mortality data of the general Chinese population in 2010 from the National Bureau of Statistics (http://www.stats.gov.cn/). Baseline factors with clinical significance, including age at diagnosis, gender, clinical features, and laboratory data were analyzed by using univariate Cox regressions. Baseline variables that were considered clinically significant or with a p value < 0.05 in univariate analysis were included in the multivariate Cox regression model. The proportional hazard assumption based on the Schoenfeld residuals was tested. A p value < 0.05 was considered significant. Data analyses were conducted with SPSS 19.0 (SPSS Inc., Chicago, IL, USA).
Results
Study population and baseline characteristics
A total of 1054 patients with pSS were enrolled, and 320 patients without follow-up data were excluded. Overall, 834 patients were finally enrolled in the study (Figure 1). The national geographical distribution of these patients is shown in Supplemental Figure S1. The baseline characteristics are shown in Table 1. The mean age of the patients with pSS at diagnosis was 48.4 ± 12.7 years with a marked female predominance (96.3%). The median duration from disease onset was 2.5 years, ranging from 0 to 40.8 years. At diagnosis, 89.0% of patients presented with dry mouth, 71.2% presented with dry eyes, 72.5% presented with ocular signs, 61.5% had positive salivary gland biopsy, 54.6% had salivary gland involvement, and 78.7% had positive autoantibodies. The frequencies of the five main extraglandular manifestations were 29.5% for joint symptoms, 8.5% for ILD, 20.1% for liver involvement, 5.5% for skin vasculitis, and 7.6% for peripheral neuropathy. Immunoserological findings of the patients showed that the positive rates for antinuclear antibody (ANA), anti-SSA, anti-SSB, and rheumatoid factor (RF) were 61.2%, 49.5%, 25.1%, and 61.4%, respectively. As for the therapeutic regimens used by the studied patients, 97.4% patients were treated with glucocorticosteroids, 27.0% were treated with antimalarial drugs, and 21.1% were treated with immunosuppressants, and there were no significant differences of therapeutic regimens between survivors and non-survivors. Compared with patients who were alive, the dead patients consisted of more males and were significantly older when diagnosed with pSS. Moreover, patients with ILD, low C4 levels, and chronic morbidities, including hypertension and CVD, had higher mortality rates.
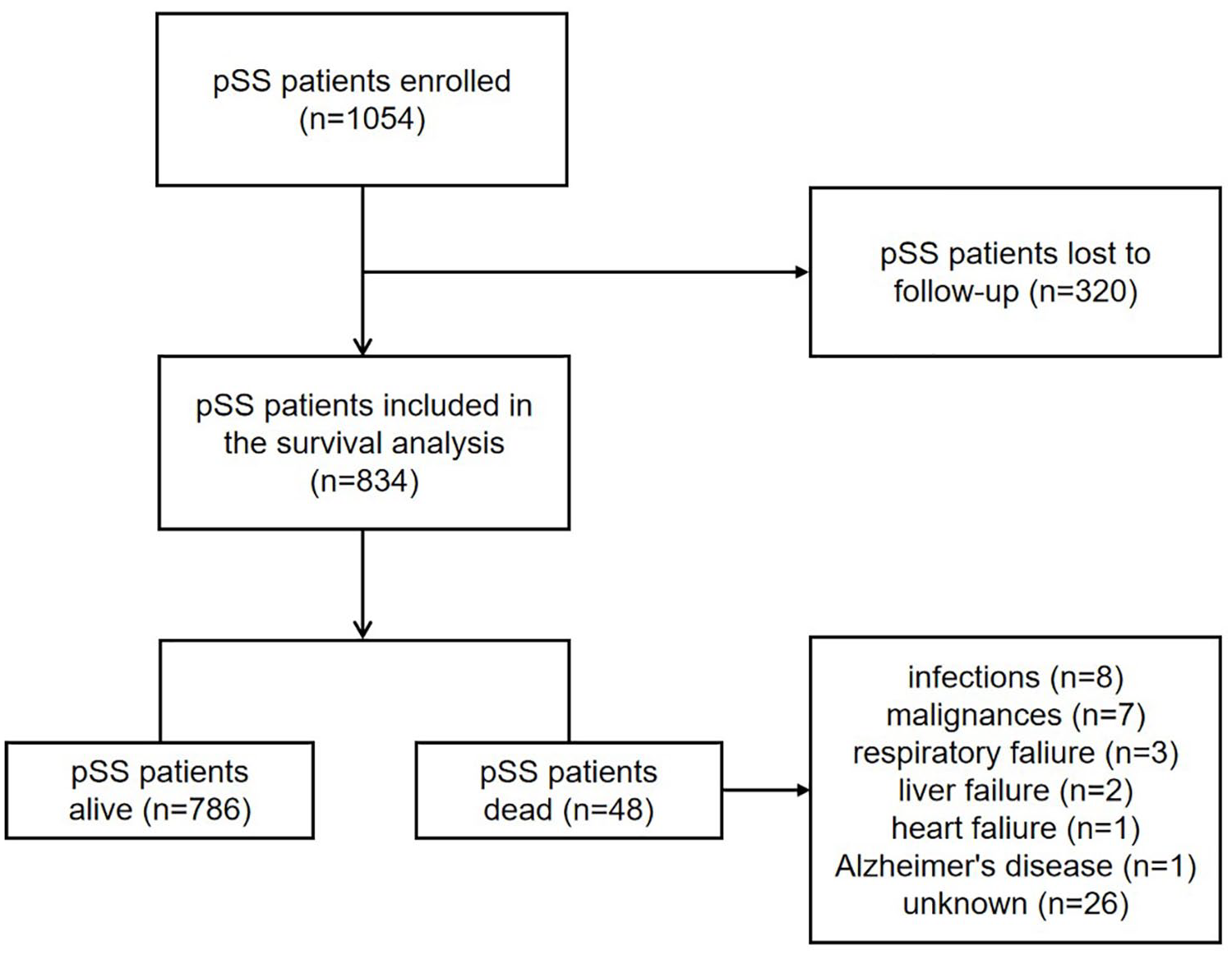
Study diagram. We enrolled 1054 patients with pSS from 2004 to 2011; 320 patients were lost to follow-up. Finally, 834 patients were included in the survival analysis and 48 patients died.
Baseline characteristics of patients with pSS.

Defined as a positive result for at least one of the following two tests: Schirmer’s I test, and Rose bengal score or other ocular dye score.
Focus score of LSG ⩾ 1, defined by the number of mononuclear-cell infiltrates containing ⩾50 inflammatory cells per 4 mm2.
Defined by a positive result for at least one of the following diagnostic tests: unstimulated whole salivary flow, parotid sialography, and salivary scintigraphy.
Positive anti-SSA or anti-SSB antibody, or both.
p ⩽ 0.01.
AECG, American–European Consensus Group; ANA, antinuclear antibody; C3, complement C3; CVD, cardiovascular disease; DM, diabetes mellitus; Hb, hemoglobin; IgG, immunoglobulin G; ILD, interstitial lung disease; LSG, labial salivary gland; PLT, platelet; pSS, primary Sjögren’s syndrome; RF, rheumatoid factor; WBC, white blood cell.
SMR
SMRs adjusted for age and gender with the general Chinese population were calculated. The total SMR in our cohort was 3.63 (95% CI 2.60–4.66). Male patients (10.06, 95% CI 2.07–18.07) had a higher SMR than female patients (3.97, 95% CI 2.77–5.17). The SMR of the patients with ILD was 21.87 (95% CI 5.01–38.73).
Survival analysis
The median follow up was 94.8 months (range, 2.2–162.0 months). The mean survival time was 153.6 months. A total of 48 (5.8%) deaths occurred, of which 42 (87.5%) were in females and 6 (12.5%) in males. The causes of the deaths included infection in 8 patients, malignancy in 7 (including 2 cases of liver cancer, 1 of ovarian cancer, 1 of breast cancer, 1 of pancreatic cancer, 1 of melanoma, and 1 of rectal cancer), respiratory failure in 3 (including 1 case of diffuse alveolar hemorrhage, 1 of ILD, and 1 of an unknown reason), liver failure in two, heart failure in 1 and neurological reasons (Alzheimer’s disease) in one; in the remaining 26 cases, the cause of death was unknown or unclassifiable. The 3-, 5- and 10-year survival rates for patients with pSS were 98.4%, 97.5%, and 92.9%, respectively (Figure 2). We also compared the survival rates in our cohort with those reported in previous studies (Table 2).

Cumulative survival of all patients with pSS.
Summary of studies on survival of patients with pSS.

The number of deaths of particular cause.C4, complement 4; CI, confidence interval; CTD, connective tissue disease; CVD, cardiovascular disease; NA, not available; ESSDAI, the European League Against Rheumatism Sjögren’s Syndrome Disease Activity Index; ILD, interstitial lung disease; pSS, primary Sjögren’s syndrome; SMR, standard mortality ratio.
Predictors of mortality
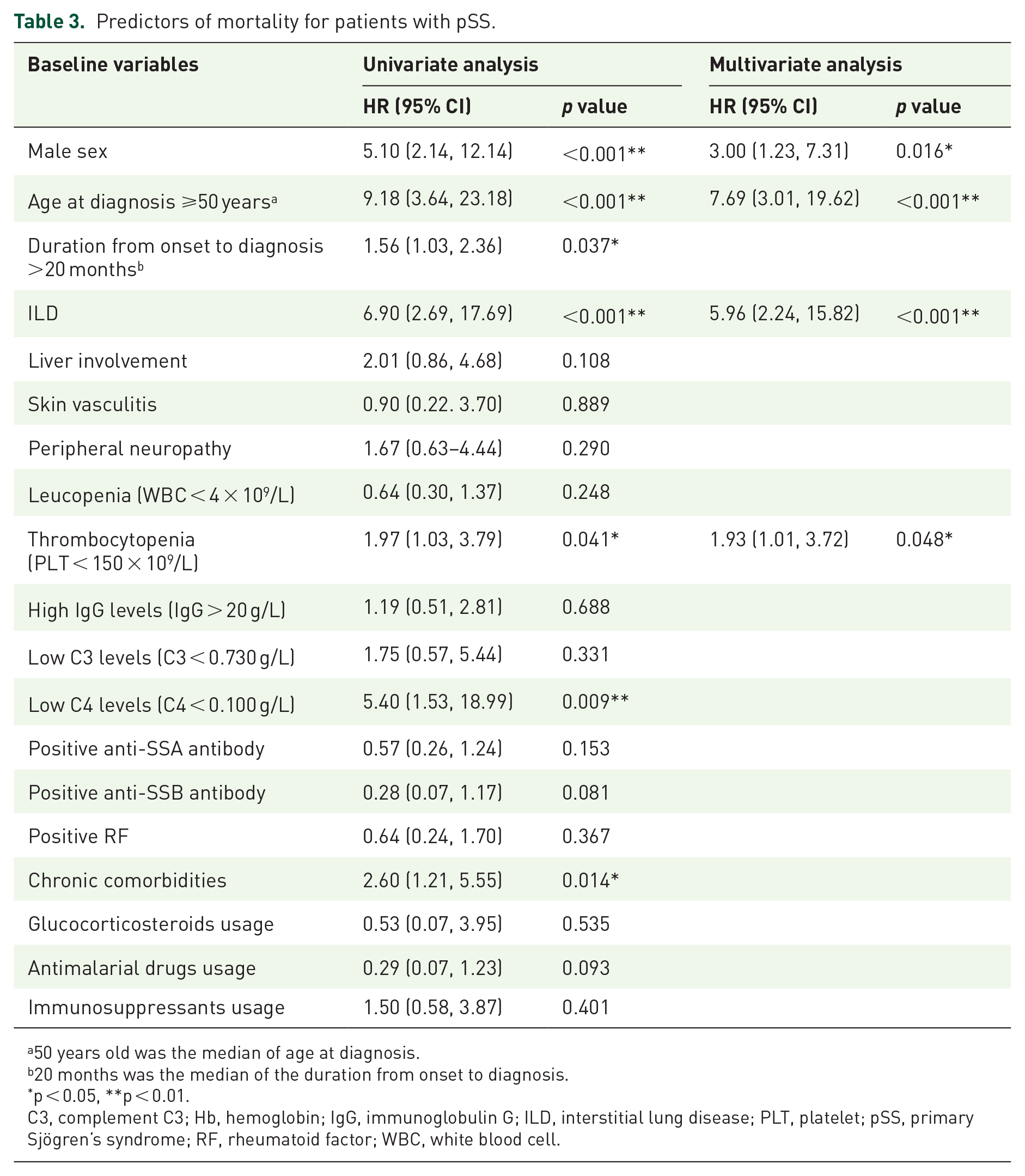
According to the univariate COX analysis, the following baseline factors were associated with mortality (Table 3): male gender [hazard ratio (HR) = 5.10, 95% CI 2.14–12.14, p < 0.001], age at diagnosis ⩾50 years old (HR = 9.18, 95% CI 3.64–23.18, p < 0.001), duration from onset to diagnosis >20 months (HR = 1.56, 95% CI 1.03–2.36, p = 0.037), ILD (HR = 6.90, 95% CI 2.69–17.69, p < 0.001), thrombocytopenia (HR = 1.97, 95% CI 1.03–3.79, p = 0.041), low C4 level (HR = 5.40, 95% CI 1.53–18.99, p = 0.009), and chronic comorbidities (HR = 2.60, 95% CI 1.21–5.55, p = 0.014). However, treatment such as glucocorticosteroids usage (HR = 0.53, 95% CI 0.07–3.95, p = 0.535), antimalarial drugs usage (HR = 0.29, 95% CI 0.07–1.23, p = 0.093), and immunosuppressants usage (HR = 1.50, 95% CI 0.58–3.87, p = 0.401) were not associated with mortality. Multivariate COX regression analyses showed that male sex (HR = 3.00, 95% CI 1.23–7.31, p = 0.016), age at diagnosis ⩾50 years old (HR = 7.69, 95% CI 3.01–19.62, p < 0.001), ILD (HR = 5.96, 95% CI 2.24–15.82, p < 0.001), and thrombocytopenia (HR = 1.93, 95% CI 1.01–3.72, p < 0.048) were independent risk factors for death (Figure 3). We further compared the prognostic factors for mortality in our cohort with those reported in previous studies (Table 2).
Predictors of mortality for patients with pSS.
50 years old was the median of age at diagnosis.
20 months was the median of the duration from onset to diagnosis.
p < 0.05, **p < 0.01.
C3, complement C3; Hb, hemoglobin; IgG, immunoglobulin G; ILD, interstitial lung disease; PLT, platelet; pSS, primary Sjögren’s syndrome; RF, rheumatoid factor; WBC, white blood cell.

Cumulative survival rates for patients with pSS with risk factors. (a) Cumulative survival of male (n = 31) and female (n = 803) patients. (b) Cumulative survival of patients with age at diagnosis <50 (n = 427) and ⩾50 years old (n = 407). (c) Cumulative survival of patients with (n = 147) and without (n = 612) thrombocytopenia at baseline. (d) Cumulative survival of patients with (n = 21) and without (n = 813) baseline ILD.
Discussion
In this study, we investigated the long-term prognosis of pSS in China based on a prospective cohort. Our data showed that patients with pSS in China have a higher SMR than the general population, and the causes of death are quite different from those in previous reports. We further analyzed and identified the prognostic factors associated with mortality. Overall, our study adds to the present knowledge of the prognosis of Chinese patients with pSS and provides survival information for clinicians to recognize high-risk patients at baseline.
The 3-, 5-, and 10-year survival rates of patients with pSS in our cohort were 98.4%, 97.5%, and 92.9%, respectively. The 5-year survival rate was comparable with that of previous studies (96.0–98.2%). Notably, the 10-year survival rate of our study is higher than that reported (89.5–92.8%), indicating that Chinese patients might have a favorable long-term survival compared with patients with pSS in other countries.8–10,12,16 Moreover, pSS was associated with higher all-cause mortality than that in the general population. The total SMR in our study was 3.63, which is lower than that in a Spanish study (SMR = 4.66), but higher than that in Korean (SMR = 1.61) and Turkish (SMR = 2.11) studies.8–10 However, a meta-analysis has reported an overall SMR of 1.38 (95% CI 0.94–2.01). 11 There may be a population-based differences in prognosis; however, time–lead bias, disease severity, therapeutic strategy, and study design should also be considered. Interestingly, subgroup analysis of SMR adjusted for age and sex showed that male patients had a much higher SMR (10.06, 95% CI 2.07–18.07) than female patients (3.97, 95% CI 2.77–5.17) when compared with the general population. Four studies also analyzed gender differences in pSS mortality previously, three of which also suggested a higher SMR of male patients than female patients, which was consistent with our results.9,10,18 However, a Finnish cohort reported the opposite result. Thus, further studies are required to explore gender differences in mortality. 19
Infection ranks as the leading cause of death, and malignancy, especially solid-organ malignancy, ranks as the second cause of death. Although lymphoma and hematologic malignancies are lethal complications of pSS, we did not observe any lymphoma. 4 Liang et al. found that Asian patients are at a lower risk for overall cancers and NHL than those in Europe and America. 20 Other common causes of death include respiratory failure, liver failure, heart failure, and neurological reasons. CVDs are reported to be the main cause of death in patients with pSS. 11 However, deaths from CVD were not observed in our study. Patients with pSS may suffer less from CVDs, partly explained by less smoking and steroid use. 3 A meta-analysis showed that, although patients with pSS were at a higher risk of cardiovascular morbidities, including coronary morbidity, cerebrovascular morbidity, and thromboembolic morbidity, overall cardiovascular mortality did not increase. 21
We identified male sex, age at diagnosis ⩾50 years old, thrombocytopenia, and ILD as independent predictors of death. However, the therapeutic regimens were not risk factors according to univariate and multivariate COX analysis, and these results were in line with a previous study in which the univariate analysis results showed that glucocorticosteroid and immunosuppressant use were associated with higher mortality, and antimalarial drugs use was associated with lower mortality; however, the multivariate analysis suggested these factors were not independent predictors for mortality. 10 ILD is a common complication of pSS, and the baseline ILD prevalence in our cohort was 8.5%, which was lower than that in a recent meta-analysis. 22 However, approximately 55% of patients with pSS may develop ILD after pSS onset. 23 Patients with pSS with ILD present with dyspnea and cough, hemoptysis, fever, and recurrent respiratory infections with limited pulmonary capacity. 24 A cohort study suggested that the patients with ILD had a lower survival rate (HR = 2.16) compared with the general population. 5 In addition, 5% of patients died of lung complications. 23 Therefore, ILD poses a great threat to long-term survival. Together, these data suggest that ILD is a predictor of poor prognosis.
Interestingly, thrombocytopenia was an independent prognostic factor in our study. Thrombocytopenia indicates hematological involvement and is a disease activity index. Brito-Zeron et al. found that thrombocytopenia is a prognostic factor for deaths of patients with pSS from systemic diseases (HR = 5.52, 95% CI 2.07–14.75), but not for overall deaths (HR = 1.34, 95% CI 0.74–2.45) 8 The potential prognostic significance of thrombocytopenia warrants further investigation.
Subgroup analysis of SMR adjusted for age and sex showed that male patients had a much higher SMR than female patients. Male sex is a poor prognostic factor for pSS in many studies.8,11 Although pSS is more prevalent in females, male patients have a lower survival rate than female patients. It seems that male patients with pSS are more prone to developing extraglandular complications such as ILD and lymphoma, which could be explained partly by the fact that male patients often have a more progressive disease.25,26 In addition, age at diagnosis ⩾50 years old was identified as a poor prognostic factor. Similarly, results from Skopouli et al. suggested that older age at diagnosis is correlated with higher mortality, 17 which is consistent with our study, indicating that elderly patients should be more closely monitored in clinical practice.
Our study has several limitations. Firstly, 320 patients were lost to follow up. However, no significant differences in the baseline characteristics between patients analyzed and those lost to follow up were noted (data not shown). Secondly, the start date of our study was earlier than the release of the ESSDAI. Although data on hematological, biological, and glandular domains were recorded, data on other domains were missing, which led to inaccessibility in calculating the ESSDAI. Patients with pSS with a high baseline score (ESSDAI score ⩾14) reportedly have a higher risk of death; however, it would be necessary to collect complete ESSDAI data on more patients to confirm this point. Overall, a future study with an increased sample size and more factors is required to ensure a more valid result.
In summary, this is the first study conducted to analyze the long-term outcomes and mortality predictors of patients with pSS in mainland China. We found that the Chinese patients have higher mortality than the general population. Infection, malignancy, and respiratory failure are the leading causes of death in pSS. More importantly, male sex, age at diagnosis ⩾50 years old, thrombocytopenia, and ILD are independent predictors of pSS mortality. These results could help identify high-risk patients during routine evaluation and those requiring closer follow up and more rigorous therapy.
Supplemental Material
sj-jpg-1-tab-10.1177_1759720X211020179 – Supplemental material for Ten-year survival analysis of patients with primary Sjögren’s syndrome in China: a national prospective cohort study
Supplemental material, sj-jpg-1-tab-10.1177_1759720X211020179 for Ten-year survival analysis of patients with primary Sjögren’s syndrome in China: a national prospective cohort study by Junyan Qian, Chengmei He, Ya Li, Linyi Peng, Yunjiao Yang, Dong Xu, Yunyun Fei, Wen Zhang, Yan Zhao, Yi Dong, Yongzhe Li, Xuan Zhang, Hua Chen, Yanlei Yang, Zhilei Chen, Suying Liu, Li Wang and Fengchun Zhang in Therapeutic Advances in Musculoskeletal Disease
Footnotes
Conflict of interest statement
The authors declare that there is no conflict of interest.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by National Key R&D Program of China (2016YFA0101003, 2016YFC0903901); National Natural Science Fund (81771764); CAMS Innovation Fund for Medical Sciences (2017-I2M-3-007); Youth Program of National Natural Science Foundation of China (81900054).
Data availability statement
The data that support the findings of this study are available with the permission of corresponding author.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.