
Abstract
Protein-losing gastroenteropathy (PLGE) is a rare manifestation of primary Sjögren’s syndrome that is most commonly reported in Japan. Herein, the case of a 71-year-old Chinese male patient, diagnosed with PLGE and Sjögren’s syndrome, is reported. The patient presented with peripheral oedema, and PLGE was diagnosed based on the result of technetium-99m (99mTc)-labelled albumin scintigraphy. In addition to a positive Schirmer’s test, the patient had atrophy of the salivary gland with lymphocyte infiltration, impaired parotid-gland secretory and excretory function, and an increased level of anti-SSA antibodies, fulfilling the criteria for Sjögren’s syndrome. He was successfully treated with methylprednisolone. Follow-up 99mTc-labelled albumin scintigraphy results correlated well with clinical improvement and increased serum albumin levels. The present case study highlights the necessity of considering a diagnosis of protein loss enteropathy associated with primary Sjögren’s syndrome when patients have unexplained hypoproteinaemia.
Introduction
Protein-losing gastroenteropathy (PLGE) is an uncommon disorder, defined as the abnormal loss of plasma protein into the gut lumen. 1 PLGE has been associated with a wide range of illnesses, including cardiac diseases, many gastrointestinal disorders and various bacterial or viral infections, 2 and is sometimes seen to occur in autoimmune diseases, particularly systemic lupus erythematosus.3–5 PLGE-associated with Sjögren’s syndrome is extremely rare, with most published cases coming from Japan,6–10 and three cases reported from Taiwan.11,12 To date, no cases have been reported from mainland China. Because sicca symptoms may be atypical, primary Sjögren’s syndrome causing PLGE can easily be overlooked. Here, the case of a 71-year-old male, who was diagnosed with primary Sjögren’s syndrome with PLGE, is reported.
Case report
A 71-year-old Chinese male patient (height, 172 cm and weight, 62 kg) was admitted to Fujian Provincial Hospital, Fuzhou, China in May 2018, due to bilateral oedema in both lower legs for 2 months. The patient had normal appetite, with no nausea, vomiting, melena, abdominal pain, or diarrhoea. He did not have dry eyes or mouth, nor any skin rash, arthralgia, or foamy urine. The patient had a previous history of good health.
On physical examination, no cardiac murmurs were heard, but respiratory sounds were weak in the right pulmonary area. The abdominal wall was soft without tenderness, and bowel sounds were normal. Marked bilateral oedema of the lower legs was noted.
Laboratory results revealed that the total protein and albumin nadirs during this hospitalization were 3.2 g/dl and 1.6 g/dl, respectively. Other blood values on initial hospital admission were as follows: haemoglobin, 11.6 g/dl; prealbumin, 117.9 mg/l; erythrocyte sedimentation rate, 67 mm; and total cholesterol, 5.63 mmol/l (normal <5.2 mmol/l). His renal and liver function were otherwise normal. Stool tests were negative for occult blood, parasite ova, and faecal fat. Urinalysis showed urinary protein of 0.232 g/day without casts. Abdominal sonography and doppler echocardiography excluded the presence of liver or cardiac disease. Chest computed tomography revealed a small amount of right pleural effusion.
Upper gastrointestinal endoscopy revealed chronic atrophic gastritis and lower gastrointestinal endoscopy showed colonic polyps. Biopsy of the colonic polyps disclosed intestinal adenoma with low grade neoplasia and only slight lymphocytic infiltration, however, technetium-99m (99mTc)-labelled serum albumin scintigraphy for intestinal protein loss showed a clear image of leakage from the ascending colon (Figure 1a). Protein-losing enteropathy was diagnosed according to the result of 99mTc-labelled albumin abdominal scintigraphy. 13

Representative technetium-99m (99mTc)-labelled human serum albumin scintigraphy images from a patient with protein-losing gastroenteropathy associated with Sjögren’s syndrome, showing: (a) dense tracer retention in the ascending colon (black circle); and (b) the disappearance of tracer retention following treatment with methylprednisolone.
A thorough investigation was performed to look for the underlying cause. Schirmer’s test was abnormal with an oculus dexter value of 5 mm and an oculus sinister of 1 mm. Results of 99mTc sialoscintigraphy disclosed impaired parotid-gland secretory and excretory function, and histopathological examination of the salivary gland showed salivary gland atrophy with infiltration of lymphocytes. Serum antinuclear antibody was positive with a titre of 1:1 000. Tests for serum single-stranded DNA, Sjögren’s syndrome (SS)A and SSB antibodies were positive, but tests for anti-double-stranded DNA antibody, anti-Sm antibody, anti-neutrophil cytoplasmic antibody, anti-glomerular basement membrane antibody and anti-ribonucleoprotein antibody were negative. Serum rheumatoid factor was normal. The patient was subsequently diagnosed with Sjögren’s syndrome according to the American College of Rheumatology/European League Against Rheumatism classification criteria. 14
The patient received human albumin (10 g daily) by intravenous (i.v.) infusion for 1 month before diagnosis, and his serum albumin level increased slowly, but remained lower than 2.7 g/dl. Following diagnosis, treatment was initiated on 13 July 2018 with 40 mg methylprednisolone, i.v., once daily for 1 week, followed by 40 mg methylprednisolone, orally, once daily for 3 weeks. After discharge from hospital, the patient attended monthly outpatient appointments for approximately 10 months, to adjust the treatment regimen and assess serum albumin levels. Methylprednisolone was reduced by 4 mg/month until the patient was receiving 8 mg methylprednisolone, orally, once daily, and this dosage was maintained for long-term maintenance therapy.
After initial therapy with methylprednisolone for 1 month, the bilateral oedema in both lower legs of the patient disappeared and the right pulmonary respiratory sounds returned to normal. The 99mTc-labelled albumin scintigraphy showed no leakage of albumin from the gastrointestinal tract (Figure 1b). Serum albumin level increased within 1 month of therapy (serum albumin level, 2.9 g/dl; Figure 2), and serum albumin levels were maintained at a normal range from 15 September 2018 and throughout the follow-up period (Figure 2).
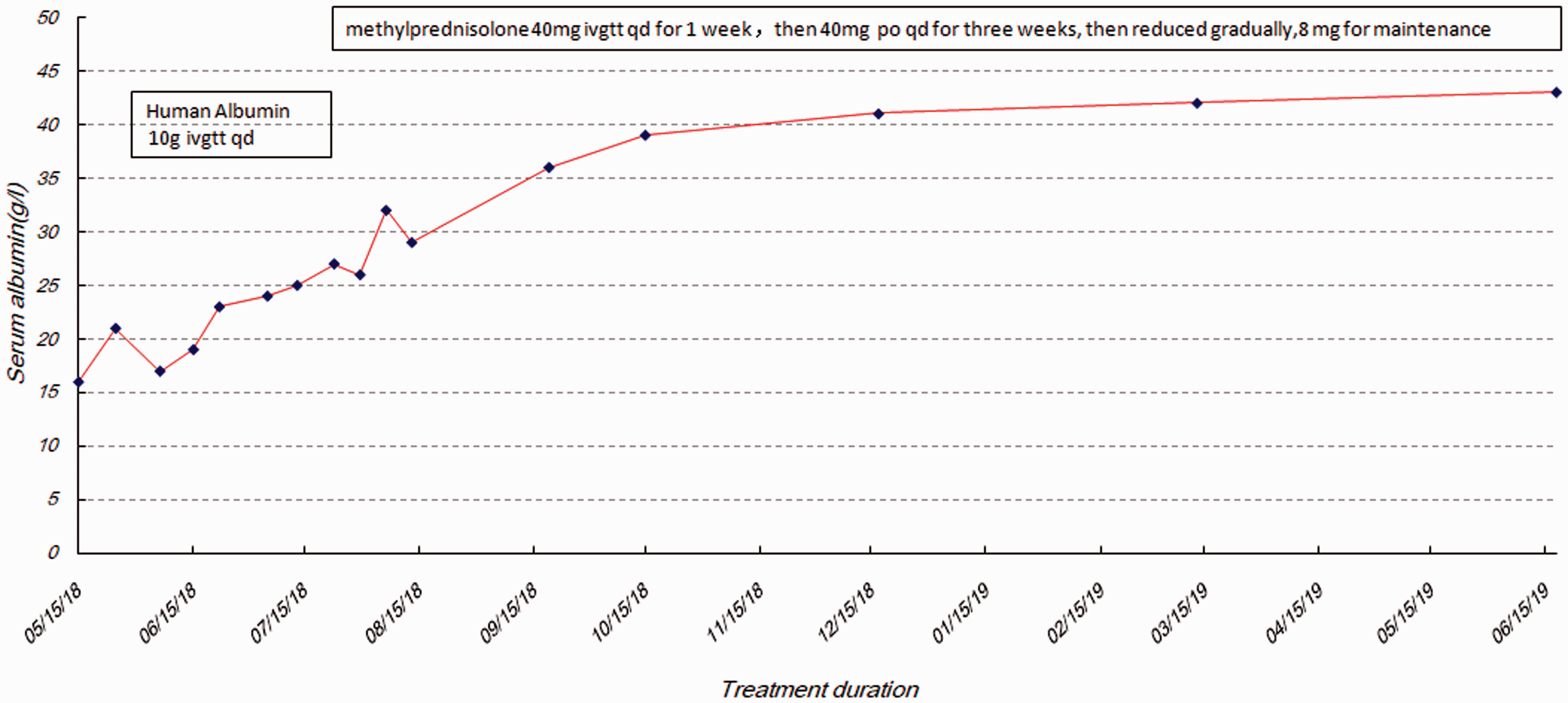
Clinical course of a patient with protein-losing gastroenteropathy associated with Sjögren’s syndrome. Serum albumin increased to normal levels during treatment with methylprednisolone.
This study was approved by the Ethics Committee of Fujian Provincial Hospital and the patient provided written informed consent for publication of the case report.
Discussion
This report described the case of an elderly Chinese male patient with primary Sjögren’s syndrome in association with PLGE in mainland China. A review of the literature revealed that most cases of PLE associated with primary Sjögren’s syndrome have been reported in patients from East Asia, particularly Japan (Table 1),6–12,15 and the disease is uncommon in mainland China. PLGE was suspected in the present case following exclusion of other factors causing low protein, such as liver dysfunction, nephrotic syndrome, cardiovascular disease, malnutrition and cachexia. Given the presence of active systemic Sjögren’s syndrome, a diagnosis of PLGE, the presence of characteristic manifestation of Sjögren’s syndrome, and exclusion of other causes of PLGE, the patient was diagnosed with PLGE associated with Sjögren’s syndrome.
A summary of the characteristics of patients with protein-losing gastroenteropathy associated with Sjögren’s syndrome, reported in previously published case studies.

A PLGE diagnosis can be determined by 24-h faecal clearance of alpha-1 antitrypsin, 16 however, stool clearance of alpha-1-antitrypsin cannot identify the site of albumin leakage. Conversely, the site of protein leakage can be located using 99mTc-labelled albumin scintigraphy. 17 Reported locations of protein leakage vary between published studies, and include the stomach,8,11,12 duodenum,7,8,18 upper jejunum,7,8,18 ileum,6,8 small intestine 12 and intestines. 12 While albumin leakage in the present patient was from the ascending colon, the locations of protein leakage have no particular regularity, and the reasons for the different sites remain unclear. In the present case, the cessation of albumin leakage into the gastrointestinal tract after treatment was revealed by the follow-up 99mTc-labelled albumin scintigraphy, and correlated with a rise in serum albumin levels and the disappearance of peripheral oedema. Therefore, 99mTc-labelled albumin scintigraphy can be effective in establishing diagnosis, locating sites of protein loss, and monitoring the curative effect of treatment.
The exact mechanisms behind protein losing enteropathy in association with primary Sjögren’s syndrome remain unknown, however, several hypotheses are proposed based on pathological findings. Leakage of protein due to the breakdown of the mucosal barrier has been suggested by biopsy findings. 19 but in the present biopsy samples, only slight lymphocytic infiltration was found. Therefore, it may be assumed that there is some defect in the tight junction complex. 20 Increased capillary permeability associated with immunoglobulin and complement deposition or cytokine-mediated damage in intestinal mucosal vascular endothelial cells may lead to PLGE. 21
There is no standard treatment for PLGE associated with Sjögren’s syndrome, and treatment options include glucocorticoids, hydroxychloroquine, cyclophosphamide and rituximab.6–12,15 In general, as in the present case, patients tend to respond favourably to glucocorticoids. However, some steroid-resistant patients require other immunosuppressive agents, for example, cyclophosphamide.10,15 It has also been reported that rituximab has completely alleviated symptoms in some patients who are resistant to steroid and cyclophosphamide treatments. 8
In a previously published case report, PLGE was suggested to be the characteristic manifestation of primary Sjögren’s syndrome. 10 In conclusion, PLGE associated with primary Sjögren’s syndrome is a rare condition, and most reported cases have involved patients from East Asia, particularly Japan. These patients are usually characterized by profound oedema and severe hypoalbuminemia (summarised in Table 1), and always lack typical presenting symptoms of Sjögren’s syndrome, such as dry eye and mouth. Therefore, PLGE associated with primary Sjögren’s syndrome may easily be overlooked, and it is necessary to consider the possibility of PLGE associated with primary Sjögren’s syndrome when patients have unexplained hypoproteinaemia. 99mTc-labelled albumin scintigraphy can be an effective technique in diagnosing, locating protein loss sites, and monitoring curative treatment effects in patients with PLGE associated with primary Sjögren’s syndrome. Immunosuppressive agents, such as glucocorticoids and ciclosporin, should be evaluated as therapeutic options in PLGE associated with primary Sjögren’s syndrome.
Footnotes
Declaration of conflicting interest
The authors declare that there is no conflict of interest.
Funding
This study was supported by grants from Fujian Major Program of Basic Science Project Foundation (2014Y0006), the Provincial Health and Family Planning Commission of Fujian Province (2014-1-7), and Fujian Provincial Training Project of Young Talents in Health System (2013-ZQN-ZD-4) . The funders had no role in the study design, data collection and analysis, decision to publish, or preparation of the manuscript.