
Abstract
Background:
Both vertebral bodies and posterior elements of the vertebrae (facet joints, FJ) can engage in bone formation in radiographic axial spondyloarthritis (r-axSpA). However, little is known about the specific structural lesions and progression patterns of FJs in r-axSpA.
Objectives:
To identify specific lesions related to r-axSpA and to investigate the distinct progression patterns by comparing the FJ changes of r-axSpA with that of diffuse idiopathic skeletal hyperostosis (DISH), osteoarthritis (OA), and control group (CG).
Design:
Single-center, retrospective study. Longitudinal imaging data were retrieved and collected.
Methods:
Age- and sex-matched patients with complete thoracic and lumbar spine computed tomography (CT) data were included and their bilateral FJs were assessed. FJ changes were divided into erosions, ankylosis, joint-space narrowing, osteophytes, subchondral sclerosis, subchondral cysts, and vacuum phenomena. Average progressed year was defined as “number of changed vertebrae × interval years”/number of changed vertebrae.
Results:
In all, 50 patients in each group were included. Subchondral cysts and vacuum phenomena were not observed. Bilateral FJ ankylosis (FJA)/erosions in the thoracic and lumbar spine, and unilateral ankylosis/erosions in T1–4, T9–12 were significantly more common in r-axSpA. Joint-space narrowing/osteophytes/subchondral sclerosis were significantly more common in DISH and OA. FJ lesions progressed in 56.34% of vertebrae of r-axSpA. The most common pattern was “FJ normal advanced to ankylosis” (17.54%) which required 2.63 years. It was followed by “erosions advanced to ankylosis” (12.3%) which took 2.05 years, and by “normal FJ advanced to erosions” (11.04%) which took 2.29 years, respectively. Degenerative changes could also progress to FJ erosions/ankylosis (24.83%). The majority pattern in DISH/OA was “FJ changes advanced to subchondral sclerosis/osteophytes/joint-space narrowing.”
Conclusion:
Bilateral FJA/erosions are r-axSpA-specific lesions. The specific progression pattern for r-axSpA was “FJ changes advanced to ankylosis/erosions.” Repeated CT examination in intervals of at least 2 years will be more appropriate for monitoring FJ progression.
Introduction
Radiographic axial spondyloarthritis (r-axSpA) is a chronic inflammatory disease predominately affecting the axial skeleton, characterized by the presence of radiographic sacroiliitis and previously known as ankylosing spondylitis. 1 When r-axSpA involves the spine, both vertebral bodies and posterior elements of the vertebrae (facet joints, FJ) can engage in the bone formation and remodeling process. In the anterior part, ossification gradually grows vertically along or near the annulus fibrosus in the intervertebral disc forming the syndesmophytes in r-axSpA. While FJs are the synovial joints in the spine, persistent inflammation in FJ can lead to bone erosions and joint destruction. 2 In addition, FJ ankylosis (FJA) in patients with r-axSpA is associated with functional impairment and spinal mobility. 3 However, FJ structural changes in r-axSpA are not as frequently investigated as syndesmophytes. Currently, only one study concerning the detailed structural lesions of FJ in axSpA shows that FJA and FJ erosions may be “disease-specific changes.” 4 But unilateral or bilateral FJA could also be observed in patients with diffuse idiopathic skeletal hyperostosis (DISH). 5 Moreover, “degenerative changes” such as joint-space narrowing, subchondral sclerosis, and osteophytes are also frequently seen in healthy elderly population and patients with osteoarthritis (OA). 6 Thus, the diagnosis of FJ disease related specifically to r-axSpA may not be readily identifiable without erosions and ankylosis. When joint inflammation sustains, whether FJ “degenerative changes” in r-axSpA may subsequently progress to complete ankylosis is unknown. To our knowledge, there has been no longitudinal study available regarding the progression of different FJ structural lesions in r-axSpA over time.
FJA was detected most often in the thoracic spine. 7 Since the irregular structure of FJ, conventional chest radiography cannot provide crisp images of structural lesions. Computed tomography (CT) imaging with three-dimensional reconstructions is thought to be the best for the structural damage FJ assessment, being able to demonstrate the specific features of erosions, ankylosis, as well as a gamut of nonspecific changes, such as joint space narrowing, sclerosis, and osteophytes. 8 Hence, the first aim of this study was to identify specific structural lesions related to r-axSpA by comparing the FJ structural lesions of r-axSpA with those of DISH, OA, and the control group (CG) using CT. The second aim was to investigate the distinct progression patterns of FJ structural lesions in r-axSpA using longitudinal CT examination over time.
Materials and methods
Patients
This study was a retrospective analysis that primarily focused on longitudinal imaging data. We included identical gender and age patients with r-axSpA, DISH, and OA who were hospitalized in the Rheumatology and Immunology Department up to the year 2023 and had available thoracic and lumbar spine CT data. The diagnosis of r-axSpA relies on the modified New York criteria of ankylosing spondylitis. The diagnosis of DISH was established according to the criteria proposed by Resnick and Niwayama 9 of flowing osteophytes over a minimum of four vertebrae. The absence of FJA was not a mandatory requirement in the diagnosis of DISH. OA group was defined as FJ degenerative changes in any segment of the thoracic and lumbar spine such as joint-space narrowing, sclerosis, osteophytes, subchondral cysts, vacuum phenomena, or facet dislocation. 10
Furthermore, we identified a CG from our hospital’s health check-up center, meeting the following criteria: (1) Age and gender matched with the patients of r-axSpA; (2) availability of complete sets of thoracic and lumbar spine CT imaging data; (3) no evidence of degenerative changes in the FJ at the time of the initial CT examination; (4) absence of any thyroid disease or other diseases that might influence bone remodeling; and (5) absence of r-axSpA, DISH, and OA.
Data on age, gender, disease duration, and the presence of human leucocyte antigen (HLA)-B27 were also collected.
The reporting of this study conforms to the Strengthening the Reporting of Cohort Studies in Epidemiology statement. 11
CT scanning and assessments
Chest CT, thoracic spinal CT, abdominal CT, and lumbar spinal CT were performed for patients in a supine position on 64-slice multiple spiral CT (Siemens Company, Munich, Germany). CT parameters were as follows: tube voltage 120 kV, automatic tube current, matrix 512 × 512.
Bilateral FJ structural lesions were assessed independently by two readers (an experienced rheumatologist and a senior musculoskeletal radiologist) who were blinded to the patient’s clinical diagnosis. In cases of disagreement, both physicians would discuss and reach a consensus. FJ structural changes were divided into erosions, ankylosis, joint-space narrowing, osteophytes, subchondral sclerosis, subchondral cysts, and vacuum phenomena according to the classification mentioned in previous literature. 4 It was reported that FJA in axSpA was less commonly seen in T5–8. 3 Considering that the anatomical position of the heart is located in the anterior aspect of T5–T8, whether the impact from the heart’s pulsation could influence FJ changes was unknown. Thus, we divided the segments of the thoracic spine into three parts (T1–4, T5–8, and T9–12) when counting the total number of each FJ change in this study. When assessing the progression of FJ changes, the sum of the number of changed vertebrae was recorded. Average progressed year (APY) was defined as “number of changed vertebrae × interval years”/total number of changed vertebrae. Each FJ structural lesion APY was calculated.
Statistical analysis
Statistical analyses were performed using SPSS (version 25.0; IBM; Armonk NY) and R language (version 4.2.2). A two-sided p-value less than 0.05 was considered statistically significant. Continuous data were expressed as the mean ± standard deviation (SD) or median (range), and categorical data were expressed as percentages. Comparison of categorical data between groups was analyzed using the Chi-square test and Pearson’s Chi-square test. 12 Pair-wise comparisons were used with Bonferroni corrections. Inter-reader reliability was calculated using the intraclass correlation coefficient (ICC).
Results
Demographic data
In all, 50 patients in each group were included (50 r-axSpA, 50 DISH, 50 OA, and 50 CG). The mean age was 59.6 ± 10.3 years, and 90% (45/50) were male. Regarding HLA-B27 status, 72% (36/50) of r-axSpA patients resulted in HLA-B27 positive. The disease duration in patients with r-axSpA was 1.2–50 years, with an average of 18.5 years.
FJ changes in r-axSpA, DISH, OA, and CG
The detailed FJ changes of the thoracic and lumbar spine in r-axSpA, DISH, OA, and CG are shown in Table 1. Figure 1 exhibited each FJ change distribution in four groups. ICC was 0.78–0.9 in ankylosis and erosions and 0.52–0.85 in joint-space narrowing, osteophytes, and subchondral sclerosis. Subchondral cysts and vacuum phenomena were not observed in all four groups of patients.
Structural lesions of thoracic and lumbar spine facet joints in CT.

CT, computed tomography; DISH, diffuse idiopathic skeletal hyperostosis; HC, healthy controls; OA, osteoarthritis; r-axSpA, radiographic axial spondyloarthritis.
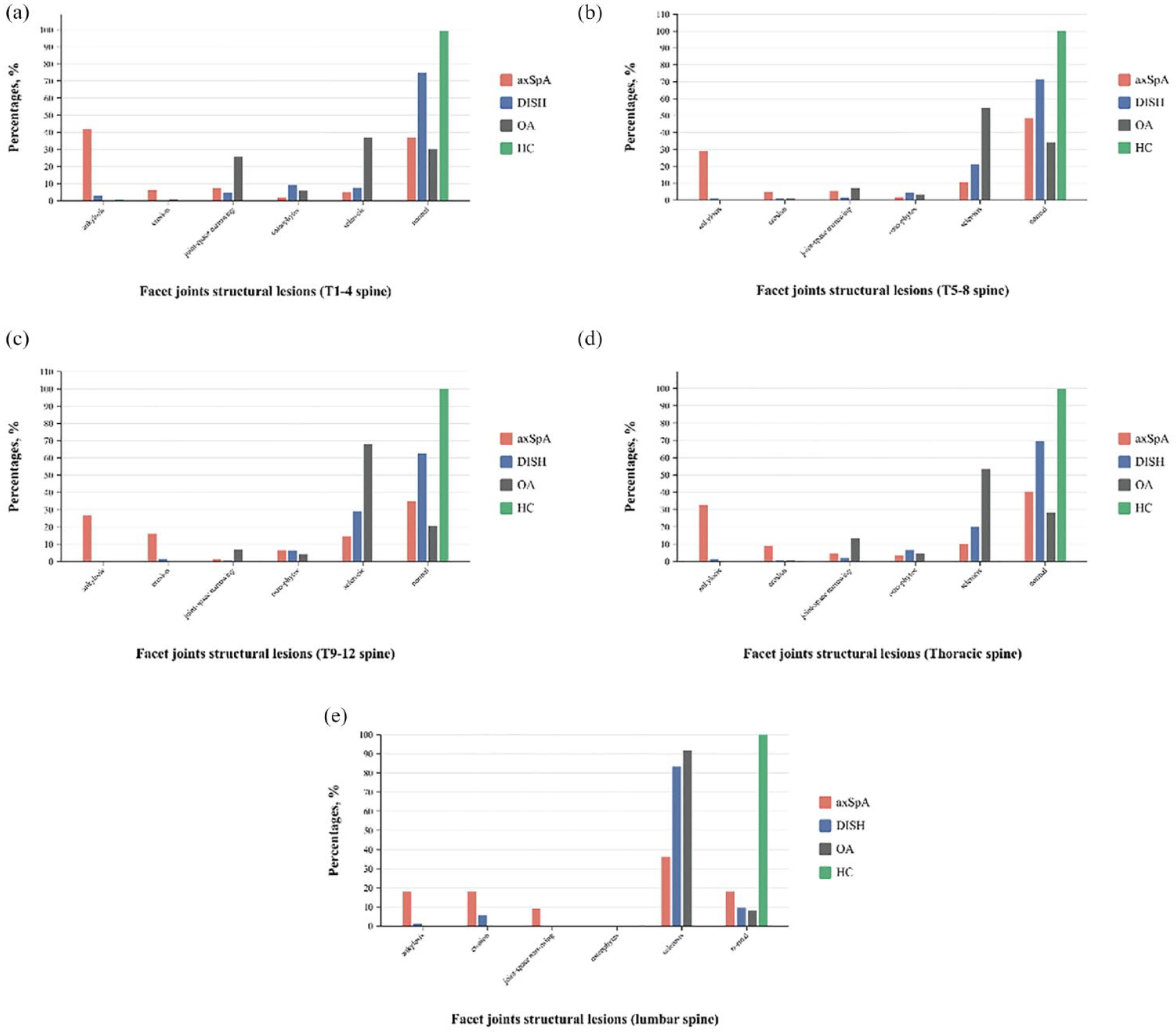
The distribution of each FJ lesion in T1–4 (a); T5–8 (b); T9–12 (c); thoracic spine (d); and lumbar spine (e) in r-axSpA, DISH, OA, and HC.
At the vertebral level, abnormal FJ structural lesions account for a substantial proportion (60.23%, 1024/1700) in r-axSpA. The percentages of FJA, erosions, joint-space narrowing, osteophytes, and subchondral sclerosis in r-axSpA were 32.32% (549/1700), 9.25% (157/1700), 4.75% (81/1700), 3.36% (57/1700), 10.56% (180/1700), respectively. We found that FJA more frequently occurred in T1–4 than in T5–8, T9–12, and the lumbar spine (p = 0.03). FJ erosions, joint-space narrowing, and subchondral sclerosis were more common in lumbar spine (p < 0.05). There is no osteophyte formation in the lumbar spine of patients with r-axSpA. The difference in the incidence of osteophytes in three parts segments of the thoracic spine was significant (p = 0.04). It showed that osteophytes occurred more often in T9–12.
FJA was seen more commonly in patients with DISH than OA and CG, which occurred more often in T1–4 (p < 0.05). However, FJ erosions and subchondral sclerosis more commonly occurred in lumbar spine (p < 0.05). FJ joint-space narrowing and osteophytes were not found in the lumbar spine in patients with DISH. They were more commonly seen in T1–4 than in T5–8 and T9–12 (p < 0.05). In patients with OA, FJ erosions, joint-space narrowing, and osteophytes were not observed in the lumbar spine. Besides, no FJA was found in the total thoracic and lumbar spine. The distribution of FJ erosions was not significantly different between T1–4, T5–8, and T9–12. However, FJ joint-space narrowing and osteophytes were more commonly seen in T1–4 (p < 0.05), and FJ subchondral sclerosis more often occurred in the lumbar spine (p < 0.05).
In group comparison analysis, the presence of FJA and erosions in the thoracic and lumbar spine was significantly more common to be seen in patients with r-axSpA. However, the results also showed that the percentage of FJA was higher in DISH than in OA and CG (p < 0.05). In the CG group, 0.25% (3/1200) had FJA in the thoracic spine. As for FJ joint-space narrowing, osteophytes, and subchondral sclerosis, the percentages of these were more often observed in DISH and OA than in r-axSpA. In the subgroup analysis, the incidences of FJ joint-space narrowing and subchondral sclerosis were significantly higher in OA than in DISH, while osteophytes were more common in DISH than in OA (p < 0.05).
FJA and FJ erosions in r-axSpA and DISH
DISH and r-axSpA are both prototypes of hyperostotic diseases of the axial skeleton. And FJA and FJ erosions could also be seen in DISH. Thus, we compared the radiographic data of these two FJ changes between r-axSpA and DISH, aiming to identify the specific structural lesions related to r-axSpA in different segments of the spine.
Details are presented in Tables 2 and 3. The results revealed that either unilateral or bilateral FJA could occur in DISH. However, the presence of unilateral or bilateral FJA was significantly more frequent in any segments of the thoracic spine of patients with r-axSpA. In the lumbar spine, a statistically significant difference was reached only for the comparison of bilateral FJA. As for FJ erosions, the results showed that either unilateral or bilateral FJ erosions were significantly more frequent in T1–4 and T9–12 of patients with r-axSpA. While in T5–8 and the lumbar spine, only bilateral FJ erosions were more frequently seen in patients with r-axSpA.
Radiographic data of facet joints ankylosis in patients with r-axSpA and DISH.

DISH, diffuse idiopathic skeletal hyperostosis; r-axSpA, radiographic axial spondyloarthritis.
Radiographic data of facet joint erosion in patients with r-axSpA and DISH.

DISH, diffuse idiopathic skeletal hyperostosis; r-axSpA, radiographic axial spondyloarthritis.
The progression of FJ changes in r-axSpA, DISH, OA, and CG
To investigate the progression of structural changes in the FJs among different diseases, we further screened 50 patients from each disease group who had at least two complete sets of thoracic and lumbar spine CT data to be included in this part of the study. Totally, 50 patients with r-axSpA, 37 patients with DISH, 44 patients with OA, and 45 CG had at least two complete sets of thoracic and lumbar spine CT data. The longest interval years were 9, 6, 12, and 10 years for r-axSpA, DISH, OA, and CG, respectively. To help understand the progression patterns, we calculated APY for FJ changes. The larger the APY value, the longer it takes for the FJ structure to progress. Figure 2 presents a schematic diagram of FJ changes and APY.
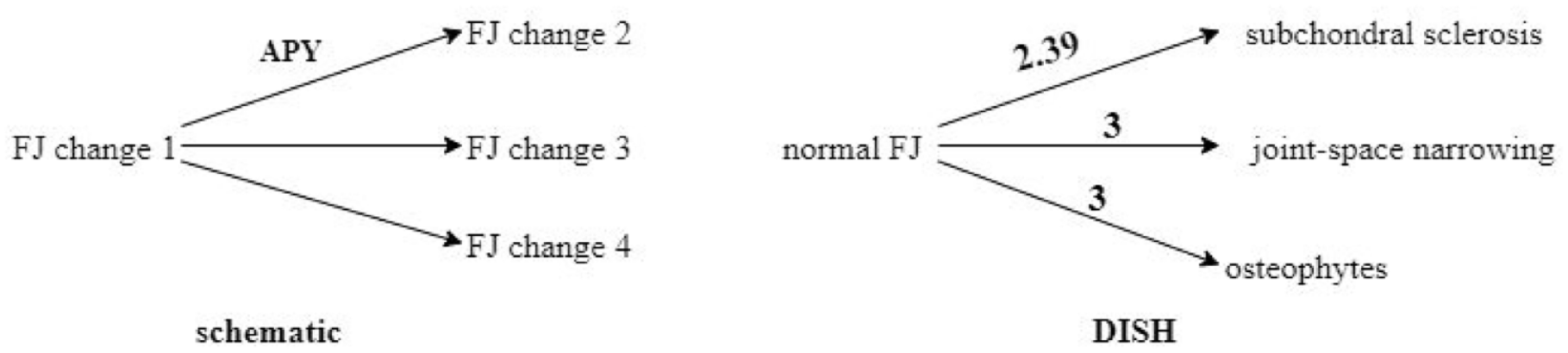
Schematic diagram of FJ changes and FJ changes progression in DISH.
In patients with r-axSpA, 2975 vertebrae were evaluated, in which 56.34% (1676/2975) had FJ changes progression. 57.64% (966/1676) vertebrae advanced to FJA, 20.88% (350/1676) vertebrae advanced to erosions, 13.78% (231/1676) vertebrae advanced to joint-space narrowing, 5.19% (87/1676) vertebrae advanced to osteophytes, and 2.51% (42/1676) vertebrae advanced to subchondral sclerosis, respectively. FJ changes developing to FJA in r-axSpA are presented in Figure 3. The results showed that the most common pattern was “normal FJ advanced to FJA” (294/1676, 17.54%), followed by “FJ erosions advanced to FJA” (206/1676, 12.3%) and “normal FJ advanced to erosions” (185/1676, 11.04%). Besides, degenerative changes that develop to FJ erosions or ankylosis were found in 24.83% of vertebrae. As for calculating the APY, we can see that it took 2.63 years for normal FJ to progress to FJA, whereas the APY of erosions developing to FJA was smaller at 2.05 years. Normal FJ developing to erosions took 2.29 years. APY for joint-space narrowing, osteophytes, and subchondral sclerosis that developed to FJA were 1.75, 2, and 2 years, respectively. Besides, normal FJ, joint-space narrowing, and subchondral sclerosis could develop into erosions (Figure 3). Among them, 7.7% (129/1676) was “FJ subchondral sclerosis advanced to erosions,” and 1.9% (32/1676) was “FJ joint-space narrowing advanced to erosions.”

FJ changes advanced to ankylosis and erosions in r-axSpA, and FJ changes progression in OA.
In patients with DISH, 25.29% (430/1700) of vertebrae had FJ changes progression. Details are shown in Figure 2. The most common pattern was “normal FJ advanced to subchondral sclerosis” (323/430, 75.12%), followed by “normal FJ advanced to osteophytes” (70/430, 16.28%). In all, 37 (8.6%) vertebrae advanced to joint-space narrowing. APY of normal FJ progressing to subchondral sclerosis, joint-space narrowing, and osteophytes were 2.39, 3, and 3 years, respectively.
In patients with OA, 49.59% (902/1819) of vertebrae had FJ changes progression. The most common pattern was “FJ subchondral sclerosis advanced to joint-space narrowing” (389/902, 43.13%). But it took 3.33 years to have this progression. Normal FJ developing to subchondral sclerosis was seen in 36.36% (328/902) vertebrae. Detailed APY is shown in Figure 3. In CG, 20.25% (358/1768) of vertebrae had FJ changes progression. APY of normal FJ developing to subchondral sclerosis, joint-space narrowing, and osteophytes were 1.81, 2.89, and 1.88 years, respectively.
Discussion
Being the true synovial joints, the involvement of FJ in the course of r-axSpA is not uncommon.13–15 However, the specific disease-related FJ changes and the progression of FJ in r-axSpA are not exactly known. Aiming to confirm the above process, the present study attempted to compare the FJ changes and progression pattern of r-axSpA with hyperostotic diseases (DISH), degenerative disease (OA), and CG using conventional CT for the first time.
Over the years, a variety of methods have been employed to examine structural lesions in the spine, with conventional radiography emerging as the most prevalent approach. However, FJ is difficult to visualize on radiographs. In recent years, low-dose CT (ldCT) has demonstrated its adequacy and feasibility and has been effectively utilized in the assessment of FJs in patients with r-axSpA.3,16 However, ldCT may not provide a clear visualization of degenerative changes such as sclerosis and joint erosion. By contrast, conventional CT offers superior imaging of FJ structural alterations and is considered to be the best modality for investigating FJ structural lesions currently. 8 As the first study to identify specific FJ lesions in r-axSpA, we found that bilateral FJA/erosions in the thoracic and lumbar spine are r-axSpA-related lesions, while unilateral FJA/erosions in T1–4 and T9–12 also appear to have diagnostic significance. Tan et al. 15 utilized CT to investigate FJ fusion in 55 AS patients and found that 51% of patients had FJ fusion in at least one vertebral level. In our study, all patients had FJ lesions in at least one vertebral level in the thoracic and lumbar spine. FJA was the most frequent lesion in r-axSpA (32.32%), which occurred more commonly in the thoracic spine, especially in T1–4. Our results were consistent with the previous reports. 3 However, the different appearance of FJA of r-axSpA in T5–8 and T9–12 was not significant in our study. In the study of Jung et al., 3 the lowest occurrence was noted in T5–8. One possible explanation for this discrepancy of FJA appearance among different segments in the thoracic spine was that anatomical or mechanical factors from the heart or aorta could restrict the motion of the thoracic spine. 8 FJ erosions accounted for 9.25% of structural abnormalities of r-axSpA in our study. In the analysis of group comparison, we found that FJA and erosions of the thoracic and lumbar spine were significantly more common in r-axSpA, while FJ joint-space narrowing, osteophytes, and subchondral sclerosis were significantly more frequent in DISH and OA. Ultimately, FJA was occasionally found in a small proportion of patients with DISH and CG. Thereupon, further comparative analysis between r-axSpA and DISH was conducted. The results demonstrated that unilateral or bilateral FJA in thoracic spine, bilateral FJA in lumbar spine, unilateral or bilateral FJ erosions in T1–4, T9–12, and bilateral FJ erosions in T5–8, and lumbar spine were r-axSpA specific-related changes. These FJ abnormalities can help us differentiate r-axSpA from DISH. Takuya et al. 5 used the whole spine CT to evaluate the radiological characteristics of 111 patients with DISH and 27 patients with r-axSpA and found that only bilateral FJA in r-axSpA was significantly different from DISH in thoracic T1–6, T7–12, and lumbar spine. The inconsistent results in our study with Takuya’s study may be due to the following reasons: (1) The sample size of patients with r-axSpA was larger in our study. (2) We addressed confounding variables by matching each study patient in regard to age and sex. (3) Considering the influence of mechanical stress from the heart, we divided the thoracic spine into T1–4, T5–8, and T9–12.
One highlight of our study was to evaluate the structural progression of all disease-specific and degenerative FJ changes, other than FJA. So far, no study focused on the progression of different FJ changes including FJ erosions and degenerative FJ changes in r-axSpA. Only a small number of studies have mentioned the progression of FJA.7,17–19 Rosalinde et al. 7 enrolled 60 patients with r-axSpA for risk factors related to FJA 2-year-progression using low-dose CT and found that 18% of patients had progression of FJA. Lee et al. 17 analyzed longitudinal data from 1106 r-axSpA patients and assessed 4986 spinal radiographs obtained up to 16 years of follow-up. The result showed that 17.8% presented with ankylosis in at least one cervical FJ. In our study, the mean follow-up time for r-axSpA was 4.13 years, with the longest follow-up of 9 years. We evaluated the FJ structural progression at the vertebral level and found that more than half of the vertebrae had FJ progressed changes. The vast majority of the progressed FJ were advanced to FJA (57.64%). Other than that, the most common FJ progression pattern for r-axSpA was “normal FJ advanced to FJA” (17.54%), which required 2.63 years. The second frequent progression pattern was “FJ erosions advanced to FJA” (12.3%), which took 2.05 years, followed by “normal FJ advanced to erosions” (11.04%), which took 2.29 years. Other than that, our study also showed that “degenerative changes” in r-axSpA could subsequently progress to FJ erosions or ankylosis (24.83%). Therefore, more attention needs to be given to FJ lesion progression even if there are no disease-specific changes at initial presentation. From the APY perspective, our study showed that the time required for normal FJ to progress to erosions was shorter than that required for normal FJ to progress to FJA. Our results might hint that erosions could be a process that occurs before FJ fusion. The mechanism diagram for specific FJ progression process in r-axSpA is shown in Supplemental Figure 1. Overall, based on our results and the previously published literature, 17 it recommended that repeated CT examinations at least 2 years apart will be more appropriate for detecting FJ progression.
Another highlight of our study was comparing the different FJ progression patterns of r-axSpA with DISH and OA. Presently, there are no comparative studies published on FJ lesion characteristics and FJ progression between r-axSpA and DISH or OA. The majority of FJ progression patterns in DISH and OA were “FJ changes advanced to subchondral sclerosis/osteophytes/joint-space narrowing” (Supplemental Figure 1). The inconsistent progression patterns in r-axSpA, DISH, and OA might be related to different genetic backgrounds. r-axSpA is an inflammatory disorder that includes inflammatory back pain, genetic predisposition (HLA-B27), and sacroiliitis. In the late stage of the disease, patients have spine fusion, including FJ. 1 However, DISH and OA have long been considered degenerative diseases. Besides, the time required for FJ changes advanced to osteophytes was longer than the time required for FJ changes advanced to subchondral sclerosis or joint-space narrowing either in DISH or in OA. These results suggest that osteophytes occur more often in the later course of the disease in DISH and OA.
Our study has some limitations though. First, due to the retrospective nature of this study and one of its main objectives being to identify the specific structural lesions FJs in r-axSpA, we did not investigate the correlation between clinical parameters such as laboratory data, disease activity, treatment, with the FJ lesions progression. Second, our inclusion criteria required participants to have at least two complete sets of thoracic and lumbar spine CT data. However, we did not mandate the collection of MRI data, which resulted in incomplete information regarding the inflammatory status of the spine for some patients. It is unknown whether spinal inflammation will affect the progression of the structural changes in the FJ. Third, the sample size of this study was relatively small, which may lead to sample selection bias. Last, annual or biennial CT scan was not available for each patient. FJ changes progression may arise before the actual time of repeated CT examination. Therefore, a large-sample size prospective longitudinal study that includes other indicators to evaluate the FJ structural progression is needed in the future.
Conclusion
Bilateral FJA and erosions in the thoracic and lumbar spine are r-axSpA-specific-related lesions. While in T1–4 and T9–12, unilateral FJA and erosions also appear to have diagnostic significance. In r-axSpA, erosions could be a process that occurs before FJ fusion. However, other than erosions, degenerative changes could also subsequently progress to ankylosis. The most common progression pattern was “FJ changes advanced to FJA,” followed by “FJ changes advanced to erosions.” By contrast, the majority of FJ progression patterns in DISH and OA were “FJ changes advanced to subchondral sclerosis/osteophytes/joint-space narrowing.” More attention needs to be focused on FJ lesions progression in r-axSpA. We recommended that repeated CT examinations in intervals of at least 2 years will be more appropriate for monitoring FJ progression.
Supplemental Material
sj-doc-2-tab-10.1177_1759720X241281201 – Supplemental material for Distinct characteristics and progression patterns of facet joint structural lesions in radiographic axial spondyloarthritis
Supplemental material, sj-doc-2-tab-10.1177_1759720X241281201 for Distinct characteristics and progression patterns of facet joint structural lesions in radiographic axial spondyloarthritis by Simin Liao, Liuquan Cheng, Zheng Zhao, Jian Zhu and Feng Huang in Therapeutic Advances in Musculoskeletal Disease
Supplemental Material
sj-docx-1-tab-10.1177_1759720X241281201 – Supplemental material for Distinct characteristics and progression patterns of facet joint structural lesions in radiographic axial spondyloarthritis
Supplemental material, sj-docx-1-tab-10.1177_1759720X241281201 for Distinct characteristics and progression patterns of facet joint structural lesions in radiographic axial spondyloarthritis by Simin Liao, Liuquan Cheng, Zheng Zhao, Jian Zhu and Feng Huang in Therapeutic Advances in Musculoskeletal Disease
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.