
Abstract
Background:
Behçet disease (BD) is a rare disease in childhood and its uveitis may lead to blindness if not properly treated.
Objectives:
We aim to describe a cohort of paediatric BD patients with uveitis.
Design:
This is a multicentric retrospective study.
Methods:
Six paediatric rheumatology units in Italy were involved including children with a diagnosis of paediatric BD according to the International Criteria for BD Criteria and/or to the International Study Group Criteria for BD, or Paediatric BD classification criteria if they had uveitis. Demographic, laboratory and clinical data were collected and followed up to March 2023. Ocular characteristics and treatment response were assessed according to Standardization Uveitis Nomenclature.
Results:
Among the 97 children with BD followed, 33 (34%) had uveitis (22 males, 66.7%). The median age at onset of BD and uveitis were, respectively, 11.5 years (2.5–17.1) and 11 years (3–17.3). Uveitis preceded BD diagnosis in 18 children (54.5%). Seventeen children had HLA B51 positivity (51.5%). Uveitis was bilateral in 25 (75.8%), and panuveitis in 16 (48.5%). All the patients received at least 1 systemic treatment for uveitis: 25 adalimumab, 2 tocilizumab, 1 abatacept, 3 infliximab, 4 azathioprine, 1 methotrexate and 1 corticosteroid. The remission was achieved with 30/35 treatments (85.7%) after a median time of 8 months (6–24). Six children had a relapse in therapy after the achievement of remission (20%). Fourteen patients stopped the therapy for persistent remission, but 5 relapsed (35.7%) after a median time of 9 months (range 1–48).
Conclusion:
Uveitis in BD is a sight-threatening condition, and it is more frequently a panuveitis. Biologic treatments seem to be often required to control ocular inflammation.
Background
Behçet disease (BD) is a rare multisystemic vasculitis involving vessels of different sizes, with typical onset between the second and fourth. 1 However, the increasing awareness about this disease among paediatric rheumatologists is increasing the number of diagnoses also in childhood. Clinical manifestations may be extremely variable encompassing recurrent bipolar aphthosis, recurrent fever, uveitis, pustulosis, arthralgia/arthritis, thrombosis, neurological and gastrointestinal involvement.2 –4 In childhood, the rarity of the condition and its atypical and incomplete presentation at disease onset make the diagnosis challenging and several complications may occur. Uveitis, typically a pan-uveitis or anterior uveitis, is one of the hallmarks of BD manifestations and if not timely recognized and treated, may lead to irreversible damage, including blindness. 5 Recently, a study identified five clusters of the phenotype of BD based on the prevalent manifestation shown by the patients, differentiating the ocular, the gastrointestinal, the articular, the central nervous system (CNS) and the mucocutaneous subtype. 6
The use of anti-TNF drugs over the last decades significantly changed the prognosis of this severe complication. However, only small cohorts are available in children, and the majority of the therapeutic experiences are borrowed from adults.5,7 –13 As well as most of the experience about paediatric uveitis is borrowed from Juvenile Idiopathic arthritis in whom two randomized controlled trials have been performed about the use of adalimumab (ADA) too.14 –17
Therefore, the purpose of the present study was to describe the ocular outcomes and the treatment response of a large cohort of paediatric BD with uveitis.
Methods
In a multicentric retrospective cohort study involving six tertiary paediatric rheumatology centres in Italy including Florence (Meyer Children’s Hospital IRCCS), Catanzaro (Department of Medical of Health Sciences, Magna Graecia University), Brescia (STT Spedali Civili di Brescia), Torino (Regina Margherita Hospital), Lecce (Ospedale Vito Fazzi, Lecce) and Bari (Ospedale Pediatrico Giovanni XXIII – Azienda Ospedaliero-Universitaria Consorziale-Policlinico), we collected the data of a paediatric cohort of BD with uveitis. The study followed The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) Statement: guidelines for reporting observational studies. 18
Study population
Patients were included if they fulfilled the present inclusion criteria: (a) patients with a diagnosis of BD according to the International Criteria for Behçet’s Disease Criteria and/or to the International Study Group Criteria for BD, or Paediatric BD classification criteria (2–4); (b) with disease onset before 16 years old; and (c) with a diagnosis of chronic uveitis according to Standardization Uveitis Nomenclature (SUN) criteria.19,20
Patients were not included in the following study if (a) they refused to participate, (b) they developed uveitis after 18 years old and (c) they carried a tumour necrosis factor alpha-induced protein 3 (TNFAIP3) gene mutation and had been therefore diagnosed as HaploA20 insufficiency.
The study was carried out according to the Declaration of Helsinki and was approved as part of a registry study by the ethics committee of Meyer Children’s Hospital IRCCS (27/2022). Informed consent was signed by legal/guardian and by patients.
Data collection
The following data were retrospectively collected based on medical charts review for each patient by the identified investigator for each centre:
- Demographic data include sex assigned at birth, ethnicity, family history for autoimmune disease, past medical history, comorbidity, age at onset of BD, age at onset of uveitis, if the ocular involvement was developed before BD diagnosis.
- Clinical characteristics: manifestations of BD including recurrent fever, recurrent oral ulcers, recurrent genital ulcers, presence of skin rash (as erythema nodosum, pustulosis, aspecific rash and others), gastrointestinal involvement (e.g. diarrhoea), thrombosis, CNS involvement (excluding headache) and others.
- Ocular data included the anatomical location of uveitis according to SUN classification criteria,19,20 laterality, the presence of ocular signs and symptoms at onset, the presence of ocular complications at onset and during the disease course (including cataract, increase/decrease intraocular pressure, posterior synechiae, band keratopathy, optic disc swelling, macular oedema, choroidal neovascular membrane, retinal scars), the visual acuity expressed in LogMAR to allow comparison and then stratified according to SUN as normal (<0.4), impaired (0.4–1), blindness (>1). 19
- Laboratory data included HLA B51 status, Anti-Nuclear Antibody (ANA) status, erythro-sedimentation rate (ESR) in mm/h at onset and C-reactive protein (CRP) in mg/dl.
- Data regarding the systemic treatment performed before uveitis onset and then the treatment for the management of ocular inflammation. For each systemic treatment due to uveitis, we collected the following data: type of systemic drugs (as methotrexate (MTX), azathioprine (AZA), ADA, infliximab (IFX), tocilizumab (TOC), canakinumab (CAN) and others), the timing for drug initiation since diagnosis, achievement of improvement ocular inflammation according to SUN criteria, 19 achievement of inactivity on treatment according to SUN criteria, 18 time to achieve inactivity on treatment, relapse on therapy, time to first relapse, drug withdrawal, relapse off therapy, time to first relapse out of therapy.
- Data regarding ocular surgical treatments such as cataract surgery with intraocular lens implant, cataract surgery with no intraocular lens implant, vitrectomy, trabeculectomy, glaucoma tube surgery and others.
Main measures of outcomes
As the main outcomes for the present study, we considered:
- The proportion of patients with BD with ocular involvement.
- The treatment response is evaluated according to the SUN Working Group definition. 19 Where improvement of inflammation is defined as two steps of decrease in anterior chamber cells (AC)/or < 0.5AC, or less than or equal to 0.5+ BIO score/NEI vitreous haze scale, no active retinal or choroidal lesions, no more than two steroid eye drops per day and no declaration of treatment failure due to intolerability or safety concerns. Inactive disease was defined as less than or equal to 0.5+ AC, less than or equal to 0.5+ BIO score/NEI vitreous haze scale and no active retinal or choroidal lesions in the absence of corticosteroid treatment.
- The achievement of remission on treatment is defined as persistent inactive disease for 6 consecutive months according to SUN definition. Time intercourse between diagnosis and achievement of remission was defined as the time necessary to achieve disease remission, as previously defined.
Statistical analysis
Statistical analyses were performed using IBM SPSS for Windows v28. Categorical variables and continuous variables were summarized as frequencies and percentages, and median and range respectively. The Chi-square test and Fisher’s exact tests were used to compare categorical variables. Moreover, we performed the McNemar test for pre–post-treatment comparisons. Continuous variables were compared using the Kruskal–Wallis test and/or Wilcoxon signed-rank test for paired samples.
Survival analysis was conducted, and Kaplan–Meier curves were generated to evaluate the time to achieve disease remission.
Results
At the time of the present study, 97 children with BD, fulfilling the diagnostic criteria are currently followed: 33 in Florence, 32 in Catanzaro, 10 in Brescia, 9 in Lecce, 7 in Torino and 6 in Bari. Among them, 33 patients (34%) showed inflammatory eye involvement and were considered eligible for the present study (Figure 1).
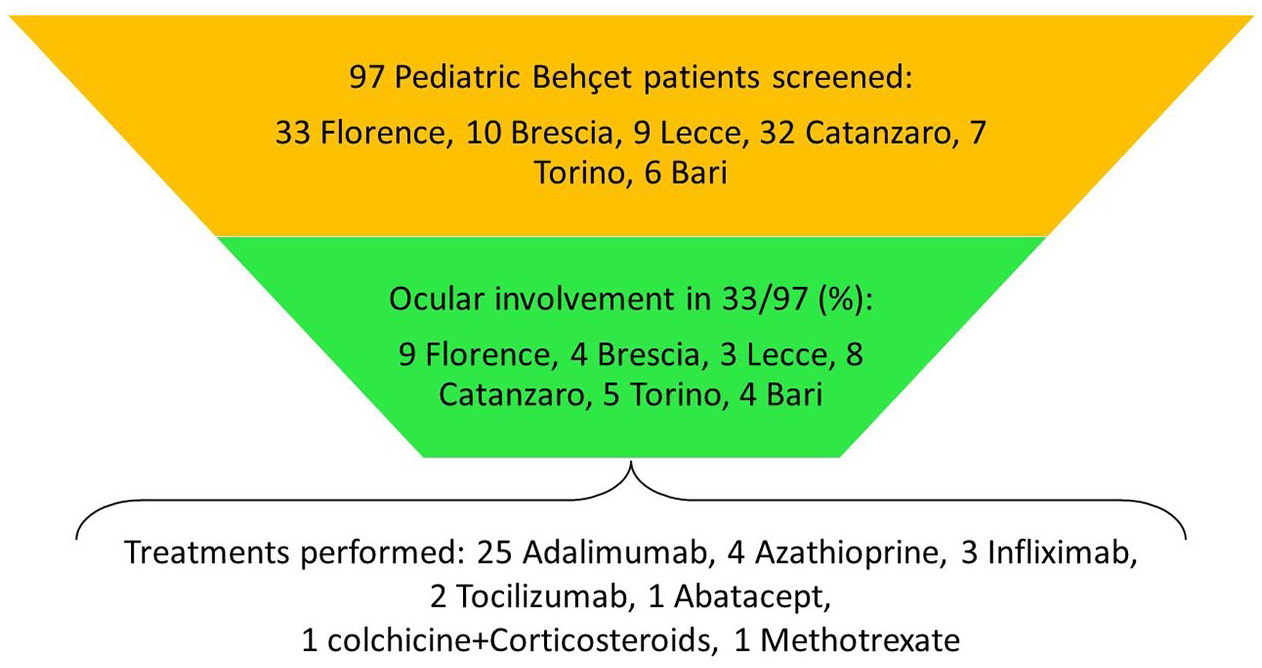
The selection process of a cohort of patients with uveitis in Behçet disease.
Among these 33 patients, 22 were males (66.7%), with a median age at onset of BD of 11.5 years (2.5–17.1) and uveitis onset of 11 years (3–17.3). Uveitis diagnosis preceded Behçet diagnosis in 18 children (54.5%), while in 6 was concomitant (18.2%) and in 9 was subsequent (27.3%). Among the 33 children, 28 Caucasian (84.8%), 3 African (9.1%) and 2 Chinese (6.1%). Ten patients showed a familial history of autoimmune diseases (30.3%).
Five/33 (15.2%) patients had ANA positivity at low titre, 1:80; 17/33 HLA B51 positivity (51.5%), a median ESR at onset of 13.5 mm/h (range 0–104) and a median CRP at onset of 0.29 mg/dl (0–20) (Table 1). Three patients exhibited elevated ESR and CRP parameters due to the concomitant presence of fever in one (ESR 60, CRP 20), and gastrointestinal involvement in two (ESR: 104 and 60; CRP: 2 and 6.1).
Ocular characteristics of childhood uveitis associated with Behçet disease.

CRP, C-reactive protein; ESR, erythro-sedimentation rate; FU, Follow-Up; NS, not significant.
According to SUN classification, 25 children had a bilateral involvement (75.8%), 16 had pan-uveitis (48.5%), 8 an anterior uveitis (24.2%), 4 an intermediate uveitis (12.1%) and 5 a posterior uveitis (15.2%) (Figure 2 and Table 1). Twenty-five children have symptomatic uveitis (75.8%), characterized by ocular hyperaemia in 20 (60.6%), photophobia in 13 (39.4%), changes in visual acuity in 18 (54.5%), and ocular pain in 9 (27.3%).

Figurative clinical and ocular manifestations of our cohort pediatric Behçet disease.
From a systemic perspective, these patients showed recurrent fever in 3 cases (9.1%), recurrent oral ulcers in all (100%), recurrent genital ulcers in 6 (18.2%), gastrointestinal symptoms in 4 (12.1%), skin rash (including pustulosis and erythema nodosum) in 11 (33.3%), a CNS involvement in 4 (12.1%), joints pain in 2 (6%), thrombosis in 2 (6%), and facial palsy in 1 (3%) (Figure 2).
Before receiving specific treatment due to uveitis, 15 children (45.5%) received a median of 1 previous therapy (range 0–3): 9 MTX (27.3%), 9 AZA (27.3%), 4 colchicine (CLC; 12.1%), 3 ADA (9.1%), 1 mycophenolate (3%) and 1 anti-IL1 (3%).
The 33 children with BD and uveitis included in the present study received 37 systemic treatments for the management of uveitis (Figure 1 and Table 2), at a median age of 151 months (range 61–211), after a median time from onset of 15 months (range 0–141). All the patients who received a biological drug (anti-TNF or anti-IL6) underwent tuberculosis screening and they resulted negative. Eighteen children received a concomitant therapy: seven mehotrexate (18.9%), seven AZA (18.9%), one CLC (2.7%), five cyclosporine (13.5%), one AZA + CLC (2.7%) and one MTX + AZA + CLC (2.7%). The two patients treated with tocilizumab were previously treated with ADA, while among the three patients treated with IFX, only one received another biologic before this (ADA). The median duration of treatment was 25.5 months (range 4–73 months). The inactivity was achieved with 30 treatments (81.1%), after a median time of 8 months (range 6–24 months). Among the 30 patients who achieved ocular remission, 5 (16.7%) relapsed on treatment after a median time of 8.5 months (range 0–40). Fifteen children were able to stop the treatment in the study; however, five relapsed (33.3%) after a median time of 8 months (range 1–48 months). Considering that most of the patients received the same treatment (ADA), we were not able to perform a comparison among the different treatments received, to assess if there was one better than another in terms of time of drug administration, duration of treatment, achievement of ocular remission, time to remission on treatment, flare on therapy and time to flare on therapy, drug withdrawal and relapse after drug withdrawal (Table 2).
Treatment performed for uveitis associated with Behçet disease and significant differences among them.

ABA, abatacept; ADA, adalimumab; AZA, azathioprine; CCS, systemic corticosteroid; CLC, colchicines; IFX, infliximab; MTX, methotrexate; TOC, tocilizumab.
Before starting systemic treatment for uveitis patients showed a median visual acuity of 0 LogMar (range 0–1.7), with normal visual acuity in 27 patients (82.4%), 4 impaired visual acuity (12.1%) and 2 blindness (6%). At the time of drug initiation, 26 children showed complications (78.8%), with a median number of complications of 2 (range 0–4). Among the complications we observed, 13 eyes showed cystoid macular oedema (19.7%), 13 optic disc swelling (19.7%), 10 epiretinal membranes (15.1%), 10 eyes posterior synechiae (15.1%), and 7 band keratopathy (10.6%).
At the last available follow-up (median 33 months, range 6–108 months), among children with data regarding the variables in the study showed a median visual acuity of 0 LogMar (range 0–0.4), with a normal visual acuity in all patients except one (97%). Ten children showed ocular complications (30.3%), with a median number of complications of 0 (range 0–3). We observed that seven eyes showed band keratopathy (10.6%), six retinal scars (9.1%), three epiretinal membranes (4.5%), three cystoid macular oedema (4.5%) and zero posterior synechiae or optic disc swelling.
We evaluated a significantly decreased proportion of patients who showed complications at the last available follow-up compared to patients at the time of starting treatment (McNemar test p < 0.0001), while we did not evaluate a significant difference in the median number of complications, visual acuity evaluated as a continuous and categorical variable (Table 1).
Survival Kaplan–Meier curves regarding the time to achieve disease remission on treatment showed that roughly 50% (16/33) achieve disease remission after 8 months of treatment (Figure 3).

Survival curve that represents the time to achieve ocular inactivity on treatment.
Among the 14 children that were able to stop the treatment, 9 children were still in remission at the longest available follow-up (median 8 months, range 1–48 months), whilst 5 (35.7%) patients relapsed and exhibited a disease flare within 12 months from treatment discontinuation.
Surgical procedures have been performed in 3/33 (9%) children: 1 received argon laser for cataract, 1 iridectomy and 1 cataract surgery with lens implant bilaterally.
Discussion
To the best of our knowledge, this is one of the largest cohorts of paediatric BD reporting data regarding eye involvement. Since 25% of uveitis may be completely asymptomatic, regular ocular screening for paediatric BD may be advocated and considered. Most of these children had bilateral panuveitis and showed several ocular complications at onset, requiring most of the time a biologic treatment, specifically an anti-TNF, ADA as well as IFX. In a few cases, the use of anti-IL6 showed excellent results when anti-TNF failed to achieve ocular control.
The proportion of 34% of ocular involvement in our national cohort of paediatric BD results in accordance with current literature, nonetheless a wide variable proportion of ocular involvement ranging from 9% up to 76% is reported considering the ethnic group and the region.1,3,21 –24 In accordance with large childhood cohort studies with BD and uveitis, we observed rarely a gastrointestinal involvement, but almost always oral ulcers.6,25
In our study, we observed a slightly lower median age at onset of BD and uveitis compared to other studies,12,21,24,26,27 but a similar gender distribution with a higher proportion of males.12,21,24,26,27
From a laboratory perspective, we observed a few cases of ANA positivity with a very low titre, which was an occasional finding. The inflammatory indexes resulted in normal values in most of the cases, with only a few cases with very high values due to concomitant systemic manifestations. As in other international paediatric and adult cohorts of BD, uveitis was most frequently a bilateral panuveitis, with a typical retinal vasculitis, followed by anterior uveitis.12,26 –28 However, a recent study identified that uveitis in paediatric BD is mainly a panuveitis. 6 Intriguingly not all the patients had symptomatic uveitis (75%) at onset, and several of the symptoms at onset referred were aspecific, that is the hyperaemic conjunctiva.
This datum, if confirmed in larger and multicentric cohorts, may prompt involved physicians to reach a consensus regarding an ocular screening program in patients with BD that may avoid and/or prevent sight-threatening complications. Indeed, at uveitis onset, 80% of our paediatric cohort showed at least one complication, and 18% showed a visual impairment. However, compared to other cohorts, we observed a similar distribution, but a lower proportion of each complication, with maculae oedema and optic disc swelling the most represented, followed by posterior synechiae and band keratopathy.1,12,22,26,28 However, in contrast to other cohorts, we did not observe cases of cataracts which is considered one of the most frequent complications of uveitis-associated BD.1,12,22,26,28
Before uveitis onset, about two-thirds of our patients had been treated with common disease-modifying anti-rheumatic drugs. At the time of uveitis onset, the majority of the BD children received anti-TNF: 25 ADA and 3 IFX. According to literature data, they represent the optimal and proper treatment when this complication arises over the BD course, in adulthood as well as in childhood.3,8 –11,13,24,27 –31 Furthermore, a recent systematic review summarized the current treatment approach for the management of paediatric BD, and uveitis seems to be one of the main reasons to use anti-TNF in children with BD. 11 Indeed, 76% of children included in the systematic review received an anti-TNF because of Batu et al. 11
In our cohort, ocular control was achieved in most of the cases with different treatments. However, two patients, previously treated with ADA, were switched to tocilizumab because of treatment failure with an optimal response, showing that anti-IL6 may be a good choice when an anti-TNF fails. This specific result seems to be in accordance with recent reports in the adult BD where tocilizumab has already shown its effectiveness.13,30,32 Conversely to adult studies, there is no current evidence regarding the use of interferon (IFN) for the management of childhood uveitis associated with BD. In adult cohorts, there is instead quite large evidence that IFN represents an appealing and valuable option for severe uveitis associated with BD.33 –35
During the follow-up, we observed an improvement in ocular outcomes, with a significant reduction in patients with complications (80% vs 30%), additionally, all the eligible children achieved a visual acuity in the normal range at the last available follow-up. Considering paediatric BD patients belonging to different cohorts, we observed a better visual acuity compared to the Turkish cohort, 26 similar to Koné-Paut et al. 36 However, as recently reported in an adulthood cohort, complications and visual acuity showed a significant improvement over time over the treatment. 5
Before drawing our conclusions, we need to discuss several limitations of the present study. Firstly, this study is retrospective. In addition, the sample size did not allow specific and single comparisons among the different treatments or the prognosis according to the different anatomical subtypes of uveitis. However, considering the rarity of the disease, this cohort represents one of the largest cohorts in childhood of BD with uveitis.
Moreover, we need to consider that our cohort of children with BD shows a wide range of age at onset, with few early onset. However, these patients have been tested for Haplo-insufficiency A20, resulting in negative. Thus, this cannot be advocated as recruiting bias for this cohort.
To picture, in a comprehensive fashion, a potential ocular phenotype in childhood BD, different from other phenotypes in childhood BD, a specific comparison with a matched cohort of childhood BS without eye involvement might be for sure worthy and useful.
Our study did not aim to address this issue. However, it might also be considered that the childhood-onset BD may be considered a specific cluster, belonging to the Bechet syndrome spectrum as a unique entity, different from the identified clusters of adult BD. According to this point of view, the need to further split childhood BD into sub-clusters by organ involvement may be a result not completely informative of the specificity of the childhood onset.
Conclusion
In conclusion, uveitis is a common manifestation of BD even in childhood, and one-fourth of patients are completely asymptomatic. The possibility of a regular eye screening might be considered, and it might be useful to identify a population that would better benefit from this based on specific risk factors/specific patterns of manifestation. Additionally, anti-TNF may be a proper choice for treating childhood uveitis in BD. Nonetheless, if they fail to achieve ocular control, tocilizumab may be an option. Larger and multicentre studies are needed to confirm our results.
Supplemental Material
sj-docx-1-tab-10.1177_1759720X241275822 – Supplemental material for Uveitis in paediatric Behçet disease: a large multicentric Italian cohort
Supplemental material, sj-docx-1-tab-10.1177_1759720X241275822 for Uveitis in paediatric Behçet disease: a large multicentric Italian cohort by Ilaria Maccora, Sara Immacolata Orsini, Romina Gallizzi, Davide Montin, Marco Cattalini, Francesco La Torre, Alessandra Spagnolo, Federico Diomeda and Gabriele Simonini in Therapeutic Advances in Musculoskeletal Disease
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.