
Abstract
Neurological Behcet’s disease is a rare systemic vasculitis marked by recurrent oral or genital ulcers, eye manifestations of uveitis or retinal vasculitis, and skin lesions. This report details a case of neurological Behcet’s disease in a 14-year-old Somali male who presented with bilateral pan uveitis, genital ulcers, altered level of consciousness, and seizure. The patient met 2014 International Criteria for Behcet Disease. Magnetic resonance imaging demonstrated abnormal hyperintensity to bilateral hippocampi and mesial temporal lobes. Spine magnetic resonance imaging revealed patchy long segment T2 signal abnormality of the central spinal cord and patchy enhancement at T6. He received IV methylprednisolone, IV infliximab, and then oral prednisone. This case demonstrates children with neurological Behcet’s disease can present with hippocampus involvement and transverse myelitis. Physicians should consider neurological Behcet’s disease in pediatric patients presenting with altered level of consciousness or seizure. It illustrates the importance of timely intervention in mitigating the neurological complications associated with neurological Behcet’s disease.
Introduction
Behcet’s disease (BD) is an idiopathic multisystemic inflammatory disease. The vasculitis of BD can affect vessels of all sizes and may consist of arterial/venous involvement. 1 BD can present in childhood, with a mean onset of 12 years and a 4:1 male predominance.1,2 Neurologic involvement occurs in 5%–10% of BD cases with pediatric-onset neurologic involvement in ~4% of all cases. 1 Neurological involvement can include nonparenchymal (cerebral vascular sinus thrombosis, intra cranial hypertension, transverse myelitis, and parenchymal lesions). 3 We present a case report of an adolescent with neurological BD (NBD).
Case
A 14-year-old male of Somali descent presented with two episodes of conjunctivitis and painless blurry vision of the left eye. There was no family history of autoimmune disease or consanguinity. He was diagnosed with bilateral panuveitis and right cystoid macular edema and started on topical steroid drops. Work-up demonstrated positive human leukocyte antigen-B51 (HLA-B51) and toxoplasmosis IgG antibody and he was started on oral sulfamethoxazole and trimethoprim. Previous tuberculosis (TB) QuantiFERON was positive, and he had been treated remotely for latent TB (Table 1). Current chest X-ray and TB skin test were negative.
Timeline.

HLA: human leukocyte antigen; TB: tuberculosis.
Three months later, he presented with 7 days of genital ulcers, lower extremity paresthesia, and back pain. He had urinary retention, headache, and photophobia. The family mentioned he had episodes of oral ulcers for a year, which was not revealed during earlier assessment, although there was a language barrier. On exam, heart rate was 80, temperature of 36.8°C, blood pressure was 125/75, oxygen saturation 99% on room air, and respiratory rate was 11. He had loss of sensation to the left leg and portions of the right. There was clonus to the left foot and hyperreflexia to patellar and Achilles reflexes bilaterally. There were punctate ulcerations to the scrotum. He had altered level of consciousness (LOC), apnea, and a paroxysmal event thought to be a seizure treated with IV lorazepam. He desaturated post lorazepam and required intubation. He was admitted to the pediatric intensive care unit for management.
Cerebral spinal fluid showed elevated protein and white blood cell count. Infectious work up was negative (Table 2). Magnetic resonance imaging (MRI) of the brain demonstrated abnormal restricted diffusion with associated T2/Fluid Attenuated Inversion Recovery (FLAIR) hyperintensity to bilateral hippocampi and left greater than right mesial temporal lobes with patchy enhancement on the postgadolinium images (Figures 1–3). There was no abnormal leptomeningeal or pachymeningeal enhancement. Spine MRI demonstrated patchy long segment T2 signal abnormality of the central spinal cord with minimal cord expansion, and with patchy enhancement at T6 (Figures 4 and 5).
Laboratory investigations.

N/A: not applicable; L: liters; mmol: millimole; g: grams; CSF: cerebral spinal fluid.

Axial FLAIR image showing abnormal hyperintensity in the bilateral hippocampi and mesial temporal lobes.
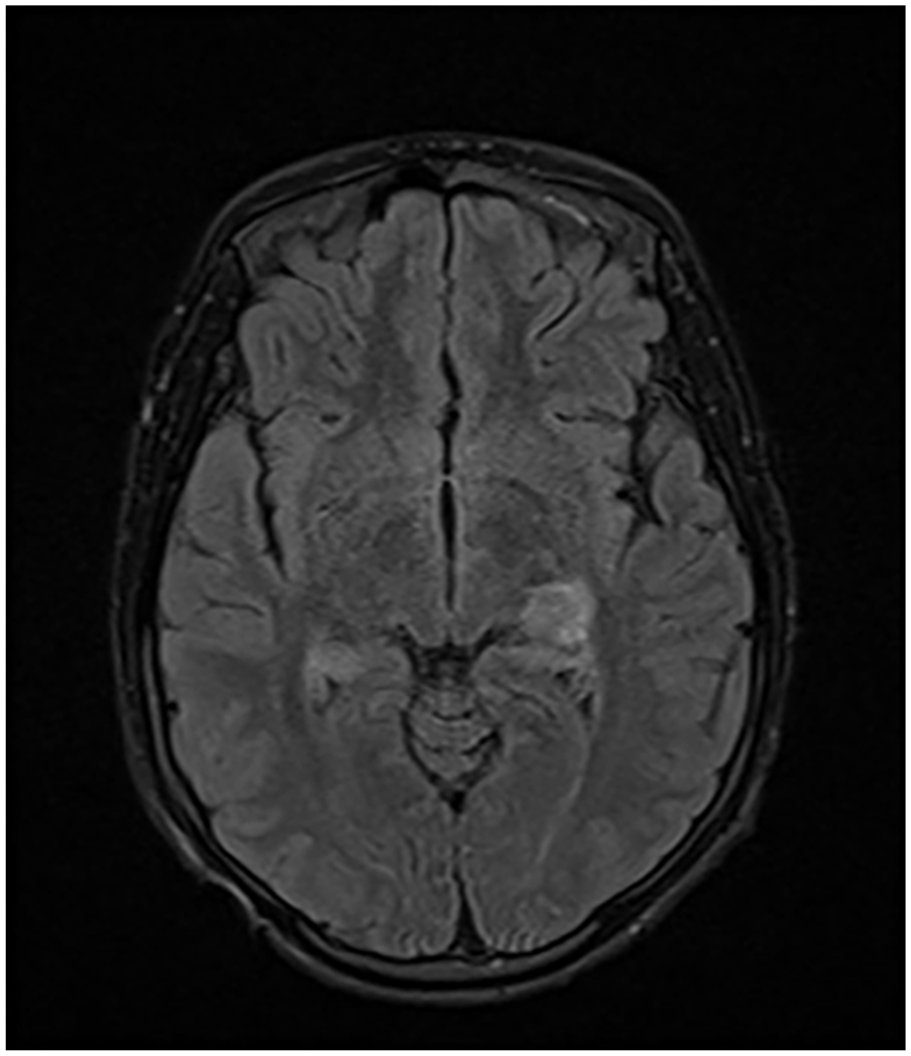
Axial FLAIR image showing abnormal hyperintensity in the bilateral hippocampi and mesial temporal lobes.
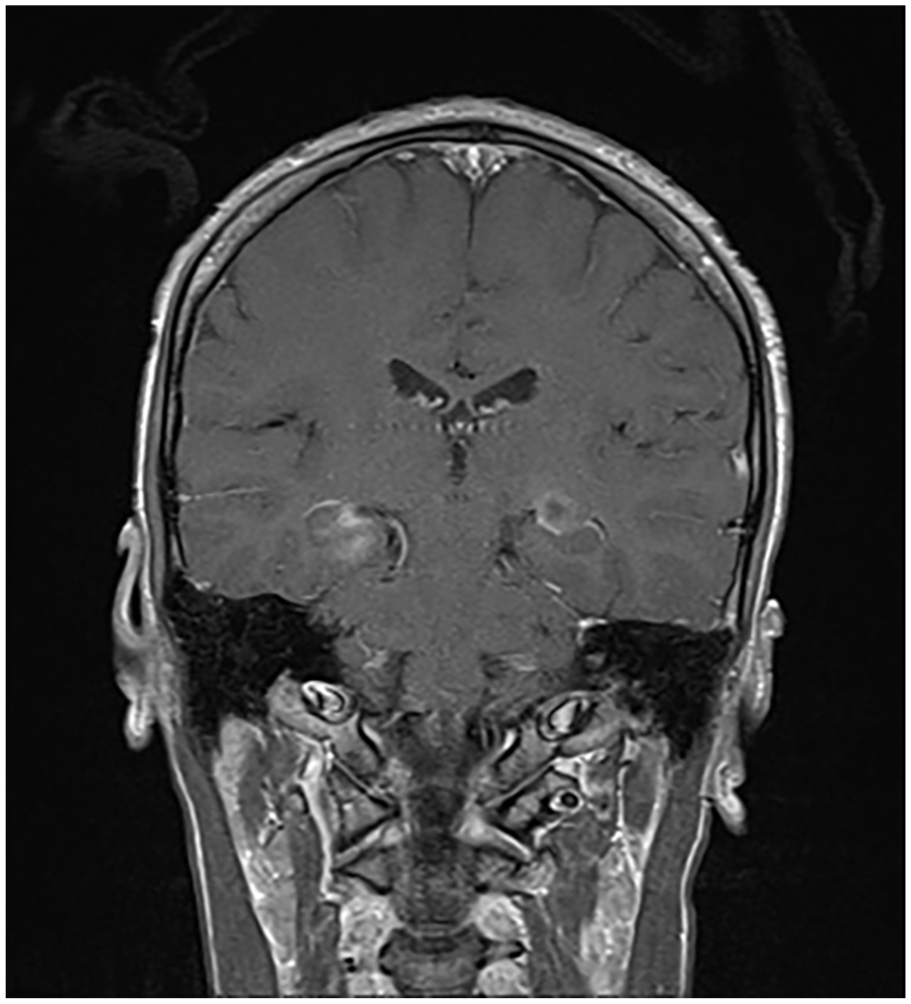
T1 post gad image showing abnormal enhancement in bilateral hippocampi and mesial temporal lobes.
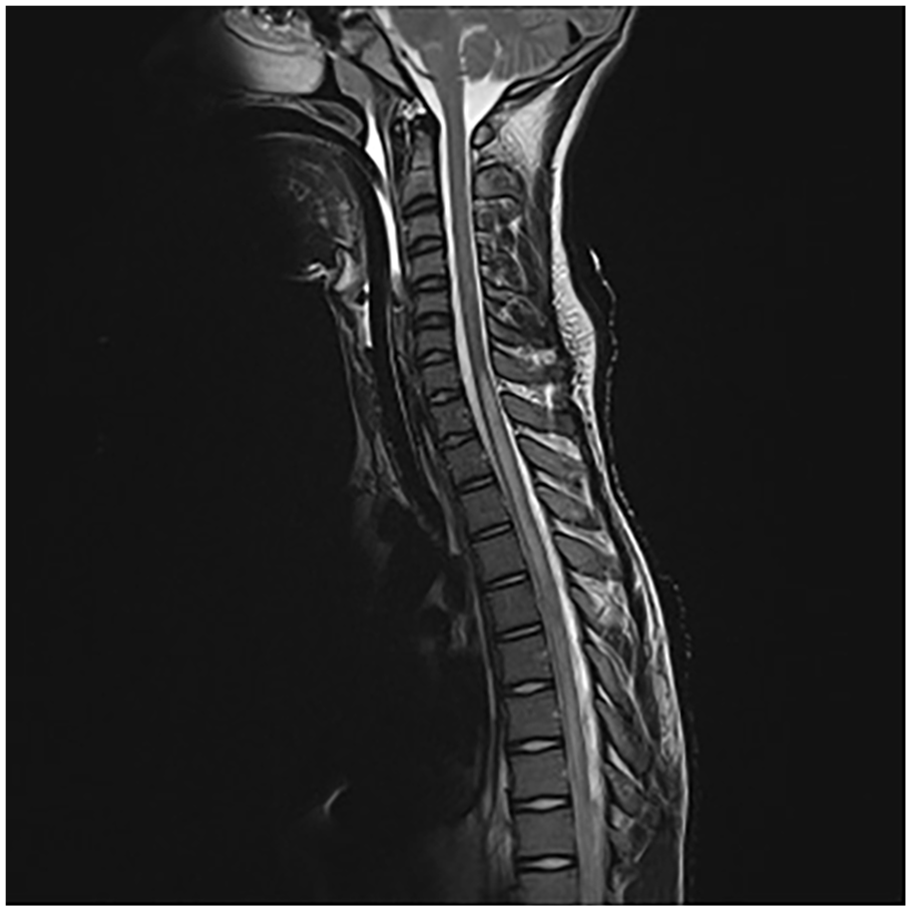
T2 spine showing diffuse signal abnormality in the thoracic region of the spinal cord.

T1 post gad, nonfat saturation image showing an abnormally enhancing lesion at T6 in the thoracic region of the spinal cord.
The differential included nonherpetic viral encephalitis, transverse myelitis, NBD with transverse myelitis, neuromyelitis optica (NMO), multiple sclerosis (MS), systemic lupus erythematous, TB, and toxoplasmosis. Upon discussion with radiology and neurology, and review of the literature and clinical and MRI features, he was diagnosed with NBD with transverse myelitis. Based on 2014 BD International Criteria he met criteria for BD with seven points (two points each for uveitis, genital ulcers, and oral ulcers, and one point for neurological involvement).
The patient was extubated 2 days later. He was treated with 5 days of daily 1000 mg IV methylprednisolone and then a tapering dose of oral prednisone (30 mg twice daily). Within 48 h of starting pulsed methylprednisolone there was clinical improvement with no further seizures. IV Infliximab 6.6 mg/kg was started as a steroid-sparing agent with resolution of the oral and genital ulcers. Given the seizure, he received oral Levetiracetam for a planned 6-month course. He had significant neuropathic pain and started on oral pregabalin and received an IV ketamine infusion with good response.
He received IV acyclovir, ceftriaxone, and vancomycin, and these were discontinued when the infectious work up was unremarkable. Prophylactic oral sulfamethoxazole and trimethoprim were continued given the history of toxoplasmosis. As per infectious disease, he did not require prophylaxis for TB, although he was at risk of reactivating it. They suggested monitoring for TB symptoms and continuing sulfamethoxazole and trimethoprim prophylaxis to prevent toxoplasmosis reactivation. He was transferred to a rehabilitation hospital and subsequently discharged home. He appropriately was stressed, scared, and worried about his prognosis. He has not had further seizures and repeat imagining demonstrated resolution of the lesions after treatment. This case report conforms to Case Report Guidelines. 4
Discussion
We describe a unique case of a patient with NBD with transverse myelitis and hippocampal involvement. The incidence of transverse myelitis in NBD is 4% and is less common than brain parenchyma presentations.2,5 Spinal MRI in the acute phase demonstrates noncontiguous multifocal lesions with cervical and thoracic spine predominance.2,6 This case had thoracic spine and lumbar involvement, which is atypical. Spinal cord involvement may mimic NMO or MS and these should be considered on the differential. 2 Given transverse myelitis can occur in the context of rheumatic diseases, it is wondered if NMO is a manifestation of a genetic predisposition to autoimmune disease versus is NMO a complication of multisystem rheumatic disease. 7
Parenchymal lesions primarily involve the subcortical and mesodiencephalic cortical regions.1,8 Imaging is not definitive, as brain MRI can be normal in NBD.9,10 This case is unique as there was parenchymal involvement of the hippocampus which is more common in adults. 8 To our knowledge, this is the third case reported in the pediatric NBD literature with hippocampal involvement.11,12 Adult patients with hippocampal lesions tend to have persistent lesions thought to be secondary to arterial vessel involvement, our patient’s lesions resolved. 9
The pathogenesis of Behcet’s is likely multifactorial, with HLAs, variants in tumor necrosis factor (TNF) signaling, abnormalities in the interleukin 23 and 17 pathways, and infectious agents being implicated in the disease. 13 TB, Streptococcus, and herpes simplex have been identified triggers in those that are immunologically predisposed. 13 Literature is sparse regarding the role of toxoplasmosis and NDB. 14 This patient had a positive HLA-B51 and had been treated for latent TB with a positive Toxoplasmosis IgG, this combination of genetic predisposition and infectious exposure may have contributed to the development of NBD. 14
For parenchymal disease, treatment with pulsed methylprednisolone for 3–7 days is typical, which this patient received then transition to oral prednisone tapered over 2–3 months. Maintenance steroid-sparing therapy such as azathioprine, cyclophosphamide, methotrexate, interferon alpha, or anti-TNF therapy should be used. 15 Anti-TNF therapy was used in this case and is often first line in severe or refractory cases. 15 Tocilizumab has demonstrated benefit, although studies are limited. 15 Cyclosporin should not be used in patients with NBD even if the CNS disease is no longer active given the potential side effect of neurotoxicity, which may potentiate CNS involvement. 15
Strengths to this case include diagnosis of NBD in the context of atypical findings on MRI and management with excellent clinical response. Limitations include the patient was not started on systemic immunosuppression therapy initially given no confirmed diagnosis and concern regarding infectious etiologies.
Conclusion
In summary, Behcet’s is an idiopathic vasculitis. It can present with neurological features secondary to parenchymal, spinal cord, or brain vasculature involvement. This case illustrates children with NBD can present with hippocampal parenchymal involvement and transverse myelitis. Phy-sicians should consider NBD in the differential diagnosis of patients presenting with altered LOC, seizures, or transverse myelitis.
Footnotes
Ethical considerations
Our institution does not require ethical approval for reporting individual cases or case series.
Consent to participate
The patient/family provided written informed consent to this case report.
Consent for publication
Written informed consent was obtained from a legally authorized representative(s) for anonymized patient information to be published in this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.