
Abstract
Background:
Patients with ankylosing spondylitis (AS) suffer from impaired physical activity and are prone to motor vehicle accidents (MVA), but definite instruction regarding the relationship between disease evolvement and MVA and potential risk factors is lacking.
Objectives:
To explore the risk factors and their impact on recorded MVA with profound injuries in AS patients with prescriptions.
Design:
Nationwide, population-based, matched retrospective cohort study.
Methods:
Using Taiwanese administrative healthcare databases, with available claims data from 2003 to 2013, we selected 30,911 newly diagnosed adult AS patients with concurrent prescriptions from 2006 to 2012 as AS patients, along with 309,110 non-AS individuals as the control group, matched in gender, age at index date and year of the index date. The risk of recorded MVA with profound injuries was compared between the two groups in terms of incidence rate ratio (IRR) and log-rank test p-value. Using Cox regression analysis, we studied associations between the risk and AS diagnosis.
Results:
The risk of recorded MVA with profound injuries in AS patients was significantly higher than in non-AS individuals, specifically 2 years after AS diagnosis (IRR, 2.00; 95% confidence interval (CI), 1.42–2.81). For patients with follow-up periods >2 years, the adjusted risk was positively associated with suburban residence (adjusted hazard ratio (aHR), 2.18; 95% CI, 1.55–3.06), rural residence (aHR, 1.89; 95% CI, 1.27–2.80), lower insured income (aHR, 1.35; 95% CI, 1.01–1.81) and recorded MVA with profound injuries before AS diagnosis (aHR, 6.16; 95% CI, 2.53–14.96). AS diagnosis (aHR, 1.81; 95% CI, 1.27–2.59) and frequency of ambulatory visits (aHR, 1.01; 95% CI, 1.004-–1.02) were specific associated factors for them compared with those with follow-up periods ⩽2 years.
Conclusion:
For adult AS patients in Taiwan, factors such as AS disease evolution and frequent ambulatory visits for disease control in the second year of the disease course may significantly increase the risk of recorded MVA with profound injuries beyond 2 years after AS diagnosis.
Keywords
Introduction
Ankylosing spondylitis (AS), currently termed radiographic axial spondyloarthritis (axSpA), is a systemic inflammatory disease characterised by spondyloarthritis, sacroiliitis and enthesitis. Many patients with AS suffer from peripheral arthritis, hip or shoulder involvement,1,2 ankylosis and extra-articular manifestations like acute uveitis, which lead to impaired physical activity and a considerable healthcare burden. 3 With systemic involvement of AS, they also face multiple comorbidities, such as fatigue, 4 fibromyalgia, 5 sleep disturbance 6 and psychiatric disorders. 7 In Taiwan, AS featured a standardised prevalence rate of 0.24% in 2010 and an incidence rate of 0.42–0.50 cases per 1000 person-years. 8 AS was diagnosed by Taiwanese rheumatologists based on 1984 modified New York criteria 9 or 2009 Assessment of Spondyloarthritis International Society classification criteria for axSpA,10,11 and current management in Taiwan is based on the updated regional consensus recommendations. 12 With growing global emphasis on optimising quality standards in AS patients, 13 rheumatologists in Taiwan are aiming, with a holistic approach, to identify modifiable factors related to health-related quality of life.14,15
High rates and high fatality in motor vehicle accidents (MVA) are significant public issues in Taiwan.16,17 AS patients may be predisposed to a higher risk of MVA as the disease evolves. 18 This issue deserves more attention from rheumatologists making individualised long-term healthcare plans. Little research is done to elucidate the relationship between the diagnosis of AS and the risk of MVA, leaving an unmet need for definite instructions for AS patients. Without clear clarification, limited attention can be aroused to preventive intervention for injuries related to their functional impairments. In Taiwan, this issue can be addressed with the aid of population-based administrative health database research, which has facilitated many epidemiological studies. 19 In this study, we investigated the associated risk factors of recorded MVA with profound injuries and their impact on the risk in AS patients with ambulatory visits for pharmacological control and followed for up to 7 years.
Materials and methods
Study design and source of data
We conducted a nationwide, population-based, matched retrospective cohort study. Claims data were acquired from the Taiwan National Health Insurance Research Database (NHIRD) and Longitudinal Health Insurance Database 2010 (LHID 2010). The National Health Insurance (NHI) Programme is an obligatory, single-payer copayment scheme that has been implemented since March 1, 1995. It is currently the only public health insurance programme and has covered >99% of the entire Taiwanese population. NHIRD is released from a database of the system for research purposes, and it can be interlinked with the National Death Registry. Information collected includes claims data regarding registration, demographics, dates of outpatient and admission services, diagnoses and procedures with their International Classification of Diseases-Ninth Revision-Clinical Modification (ICD-9-CM) codes, medication prescriptions with their Anatomical Therapeutic Chemical Classification codes and medical expenditures covered by NHI. However, it does not include information like weight and height, personal history, alcohol and tobacco use, substances use without NHI reimbursement, laboratory measures and AS activity, damage and functional measures. As a subset of the health dataset originating from NHIRD, the LHID 2010 database randomly sampled 1 million beneficiaries from NHIRD participants in 2010. It contains the most updated claims data of sampled individuals since 1997. It is validated by Taiwanese researchers to have representative power of the nationwide population. 19 The available claims data in both databases started from January 1, 2003 to December 31, 2013.
Study subjects and identification of AS patients and matched non-AS individuals
In our study, newly diagnosed AS patients aged ⩾20 years with pharmacological control were identified via NHIRD to include those having ⩾3 rheumatology ambulatory visits with ICD-9-CM code of AS and a concurrent prescription of non-steroidal anti-inflammatory drugs, methotrexate or sulfasalazine for disease control from January 1, 2006 to December 31, 2012 (Supplemental Table S1). When AS was identified as ⩾2 visits with the corresponding ICD-9-CM code given by a rheumatologist, the reported positive predictive value was 81% and sensitivity was 67% from experience in the United States. 20 The selected patients were called the AS patient group. The other subset of patients with at least one ambulatory visit from January 1, 2006 to December 31, 2012 was identified via LHID 2010. After excluding those with a diagnosis of AS, the remaining patients were defined as non-AS individual groups that acted as the control group. In both groups, subjects with incomplete records or loss of follow-up by 2012 were excluded. Patients in both groups were each assigned an index date, which was the date of their first AS diagnosis for AS patients, and the date of first ambulatory visit for non-AS individuals. After matching for the year of index dates and pairing individuals across the two groups, we then determined if the occurrence of potential risk factors within a year before AS diagnosis had influenced the risk after AS diagnosis. We matched the AS group with the non-AS group at a ratio of 1:10 for gender, age at the index date and year of the index date. After matching, selected study subjects in both groups were included for final analysis. The process for the selection of study subjects for ultimate analysis is shown in Figure 1.
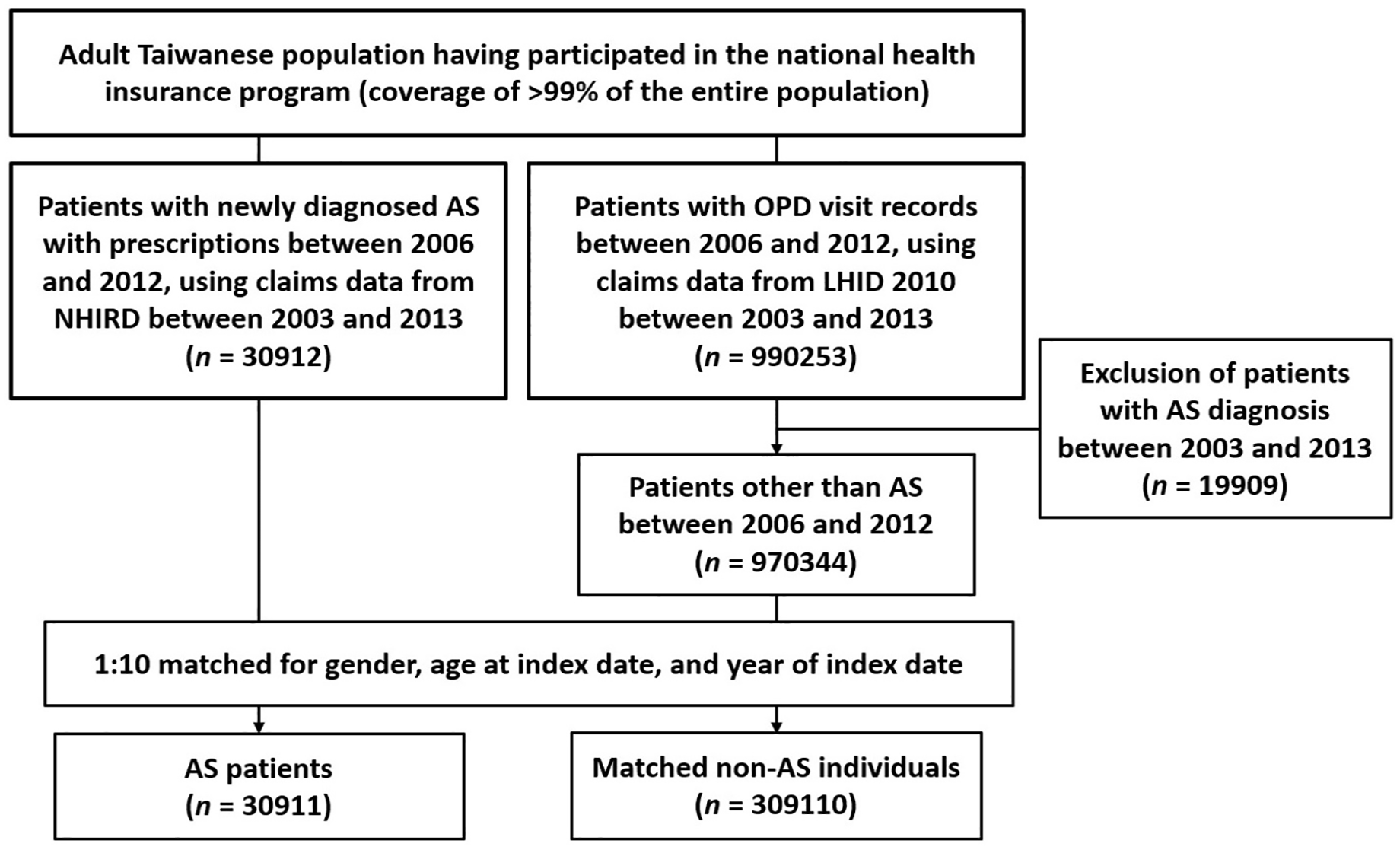
Flow diagram of enrolment, categorisation and matching for comparison of the study population.
Study outcomes
The primary investigated outcome was MVA with profound injuries that necessitated emergent medical exams or management, such as fractures or acquired spondylolisthesis, recorded as the chief diagnosis at emergency department visits, which was identified by ICD-9-CM codes (E810-E819) and concomitant injury codes (800-999) (Supplemental Table S1). The follow-up period of each patient was the interval between the index date and the first of the following censoring events: occurrence of recorded MVA with profound injuries, December 31, 2013, date of withdrawal from the NHI programme for any reason or death.
For subjects experiencing recorded MVA with profound injuries at the emergency department, the associated complications (major fractures and acquired spondylolisthesis) during and from episodes of MVA, and short-term adverse outcomes (surgeries and death) within 1 month after MVA were demonstrated, which were identified by at least one ambulatory or inpatient visit with corresponding ICD-9-CM codes and interlinked data from National Death Registry (Supplemental Tables S1 and S2).
Potential confounders for MVAs
We listed several covariates to be adjusted, including the AS diagnosis, gender, age at the index date, socioeconomic status by urbanisation level and insured monthly income, and MVA with profound injuries recorded at the emergency department before the index date. Some covariates that had occurred within 1 year before the index date were also adjusted, including history of spinal or joint surgeries (Supplemental Table S2), frequency of recorded outpatient department visits, comorbidities, extra-articular manifestations and use of medications including systemic corticosteroids and those predisposing patients to trance. Age at index date was classified into four groups by quartile distribution to observe the trend of the risk concerning age of diagnosis. The Taiwanese stratification model of urbanisation level was assessed based on population density, physician availability, the proportion of elders, agricultural workers and residents with college-level education in each subject’s residential district. 21 Selected comorbidities for adjustment included myocardial infarction, cerebrovascular diseases, chronic obstructive pulmonary disease, peptic ulcer disease, mild liver disease, diabetes mellitus, anxiety disorders, depressive disorders, bipolar disorders, psychotic disorders and alcohol-related disorders. The extra-articular manifestations, including uveitis, psoriasis and inflammatory bowel disease, were diagnosed specifically by corresponding specialists. The presence of comorbidities and extra-articular manifestations was identified by ⩾3 ambulatory visits or 1 inpatient visit with corresponding ICD-9-CM codes within a year before the index date. The use of medications within a year before the index date was identified through Anatomical Therapeutic Chemical classification codes. These medications included hypnotics (benzodiazepine-related drugs and benzodiazepines), antihistamines, antidepressants, antipsychotics and systemic corticosteroids. The above diseases, events, manifestations, medications and their corresponding codes are summarised in Supplemental Table S1.
Methods to enhance diagnostic accuracy and sensitivity analyses
We included patients with ⩾3 ambulatory visits with a diagnostic code of AS and a concurrent prescription given merely from rheumatologists. The inclusion of covariates within 1 year before the index date was set as only ⩾3 ambulatory visits or one inpatient visit with administrative codes. The included extra-articular manifestations were concurrently recorded by corresponding specialists (i.e. uveitis also recorded by ophthalmologists). These measures were aimed at enhancing diagnostic accuracy.
We compared baseline characteristics in matched study subjects having >2 years of follow-up (Supplemental Table S3). We also compared incidence rate ratio (IRR) with log-rank test p-value, and conducted Cox regressions using the time horizon of within and beyond 2 years after index date for sensitivity analysis.
Statistical analyses
Continuous variables were represented as mean ± standard deviation and categorical variables as the number (percentage) of patients. We compared continuous variables between the two groups using an independent t-test, and categorical variables using the Chi-square test or Fisher’s exact test. Incidence rate in both groups, IRR and results of log-rank tests were generated. Kaplan–Meier curves of cumulative incidence in matched study subjects were compared. The association between AS diagnosis and the risk as determined with Cox proportional hazard regressions to adjust for covariates was presented as an adjusted hazard ratio (aHR) with 95% confidence intervals (CIs). A probability (p) value of <0.05 was considered statistically significant. Statistical calculations were performed using Statistical Package for the Social Sciences, Windows Version 13.0 (SPSS Inc., Chicago, IL, USA).
Reporting standards
The reporting of this study conforms to the Strengthening the Reporting of Observational Studies in Epidemiology statement. 22
Results
Baseline characteristics of the study population
We included 30,911 patients with newly diagnosed adult AS with prescriptions from NHIRD in the AS group and 309,110 matched individuals from LHID 2010 in the non-AS group, among which no subject was excluded due to missing data or loss of follow-up (Figure 1), and baseline characteristics of study subjects of the two groups are shown in Table 1. The study population consisted predominantly of male subjects (collectively 62.9% in the two groups). The mean age of AS patients at diagnosis for the first time was 42.1 ± 16.8 years, represented as the age at index date. We observed no preponderance in the age of AS diagnosis. In comparison, a higher proportion of AS patients resided in urban districts at diagnosis, received more than the median monthly income, had undergone spinal or joint surgeries within 1 year before AS diagnosis (p < 0.001) and had experienced previous emergency department visits due to MVA with injuries (p < 0.001). AS patients also had significantly more frequent outpatient department visits before AS diagnosis (p < 0.001). Statistically greater proportions of AS patients were diagnosed with comorbidities and all extra-articular manifestations before AS diagnosis, with the exceptions of cerebrovascular diseases and psychotic disorders. Regarding medications, greater proportions of AS patients had been prescribed all specified medications before their AS diagnosis (all p < 0.001).
Baseline characteristics in matched study subjects.

Age at first AS diagnosis for AS patients, and date of first ambulatory visit for non-AS individuals.
Insured monthly income lower than median monthly income (⩽21,000 New Taiwan dollars/month).
AS, ankylosing spondylitis; MVA, motor vehicle accident; OPD, outpatient department; SD, standard deviation.
For subjects with longer than 2 years of follow-up, we found no predominant distribution of residence between groups, a greater proportion of AS patients with a history of cerebrovascular diseases and no difference regarding history of psychotic disorders and alcohol-related disorders. Otherwise remained consistent (Supplemental Table S3).
Incidence rates of MVA with profound injuries in AS patients and non-AS individuals
The incidence rate was 58 per 100,000 person-years for AS patients, compared with the rate of 38 per 100,000 person-years for non-AS individuals, and AS patients recorded significantly more frequent MVA with profound injuries than non-AS individuals (IRR, 1.53; 95% CI, 1.18–1.98; log-rank test p-value: 0.001) (Table 2). Despite no statistical difference in incidence rate between the two groups based on the period within 2 years after the index date (IRR, 1.13; 95% CI, 0.76–1.69; log-rank test p-value, 0.545), the difference became significant when the period of comparison extended beyond 2 years after the index date (IRR, 2.00; 95% CI, 1.42–2.81; log-rank test p-value: <0.001). Kaplan–Meier curves of cumulative incidence between the two groups showed consistent results (Figure 2).
IRR of motor vehicle accidents with profound injuries between matched study subjects.
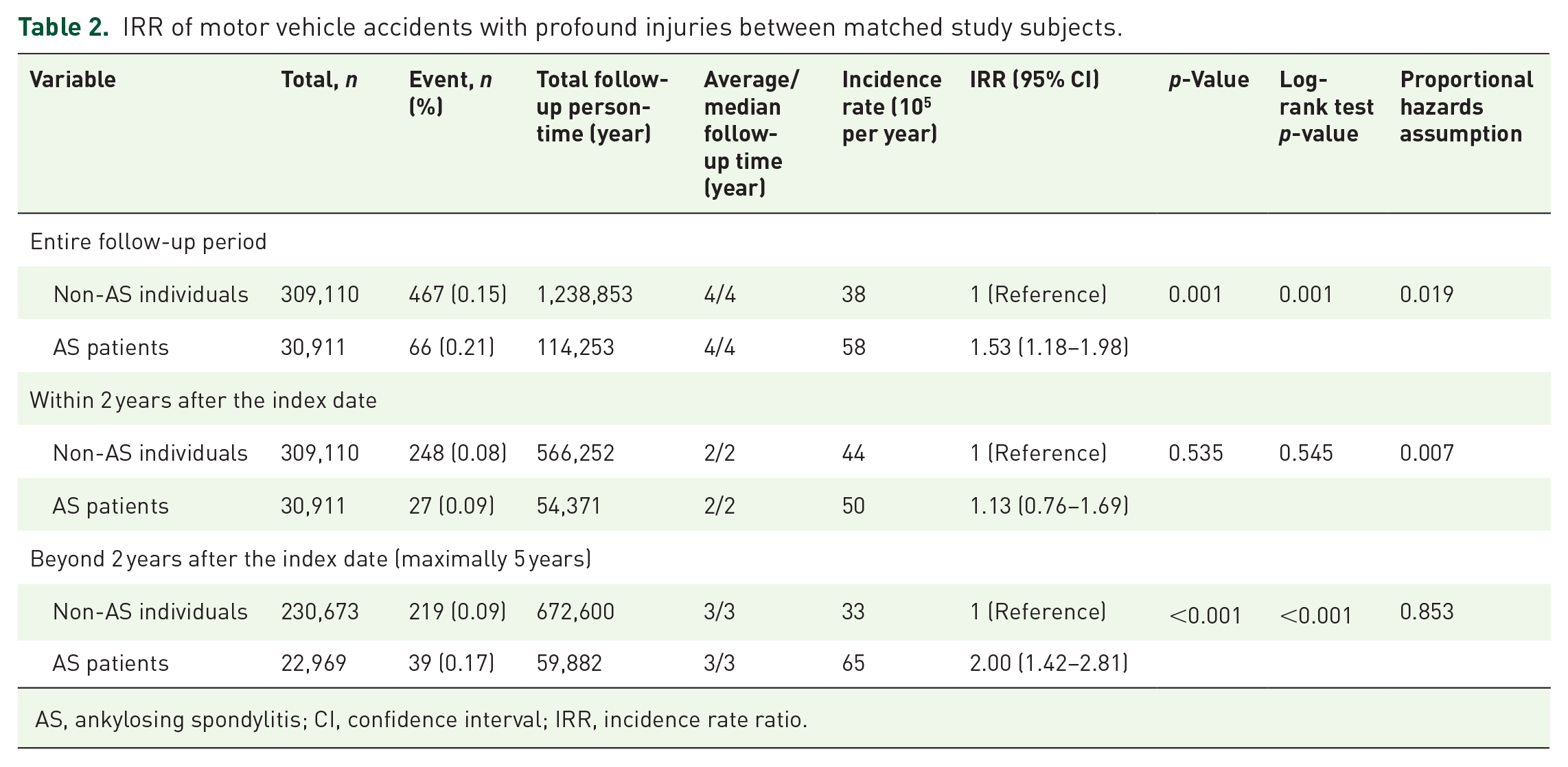
AS, ankylosing spondylitis; CI, confidence interval; IRR, incidence rate ratio.

Kaplan–Meier curves of cumulative incidence of motor vehicle accidents with profound injuries among matched study subjects. (a) During the entire follow-up period. (b) Period within 2 years after the index date. (c) Period beyond 2 years after the index date.
Outcomes of study subjects experiencing MVA with profound injuries
Among subjects experiencing recorded MVA with profound injuries at the emergency department, 1.5% of them underwent spinal or joint surgeries within 1 year before MVA (Table 3). During their recorded episodes, no difference was found in the proportions of subjects complicated with major fractures and acquired spondylolisthesis, nor were proportions of those facing surgeries and death within 1 month after MVA as the short-term adverse outcomes. Regarding longer-term influences, no difference in the proportions of subjects with recorded major fractures and acquired spondylolisthesis from their recorded episodes. The results were unchanged in the periods within and beyond 2 years after the index date.
Outcomes of study subjects experiencing recorded MVAs with profound injuries at the emergency department.
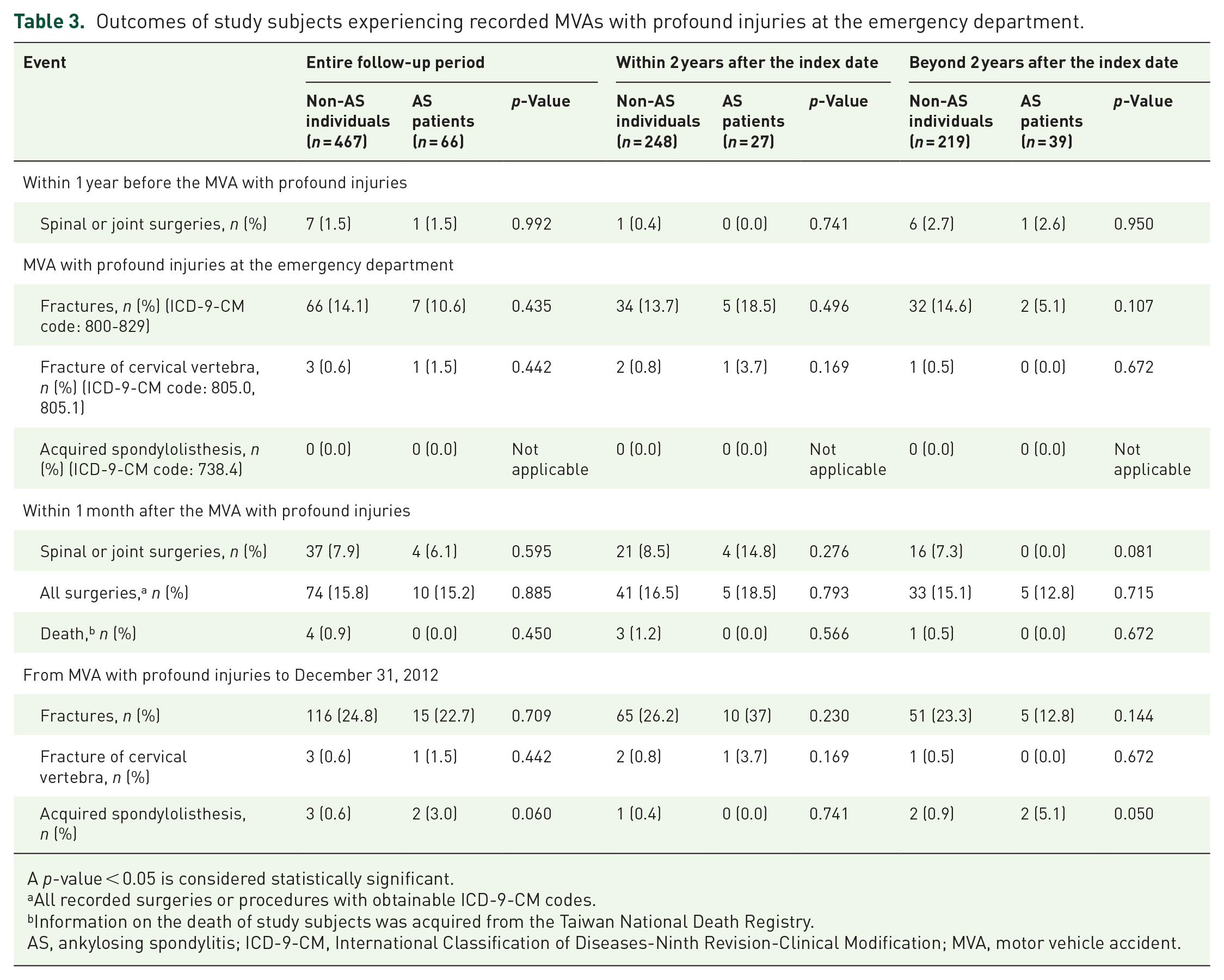
A p-value < 0.05 is considered statistically significant.
All recorded surgeries or procedures with obtainable ICD-9-CM codes.
Information on the death of study subjects was acquired from the Taiwan National Death Registry.
AS, ankylosing spondylitis; ICD-9-CM, International Classification of Diseases-Ninth Revision-Clinical Modification; MVA, motor vehicle accident.
Independent risk factors associated with MVA with profound injuries in AS patients
Results of Cox proportional hazard regression analyses during the entire follow-up period showed that the risk would be associated with AS diagnosis (aHR, 1.42; 95% CI, 1.08–1.87), male gender (aHR, 1.35; 95% CI, 1.11–1.64), suburban residence (aHR, 1.82; 95% CI, 1.45–2.28), rural residence (aHR, 1.84; 95% CI, 1.42–2.39), lower insured income (aHR, 1.44; 95% CI, 1.19–1.74) and MVA with profound injuries recorded at emergency department before index date (aHR, 9.40; 95% CI, 5.70–15.48) (Supplemental Table S4). Based on the period within 2 years after index date, it would be associated with male gender (aHR, 1.46; 95% CI, 1.11–1.94), suburban residence (aHR, 1.73; 95% CI, 1.27–2.36), rural residence (aHR, 1.80; 95% CI, 1.26–2.58), lower insured income (aHR, 1.44; 95% CI, 1.10–1.87) and recorded MVA with profound injuries before index date (aHR, 11.57; 95% CI, 6.31–21.22) (Supplemental Table S5). When analysed based on the period beyond 2 years after the index date, it would be associated with AS diagnosis (aHR, 1.81; 95% CI, 1.27–2.59), suburban residence (aHR, 2.18; 95% CI, 1.55–3.06), rural residence (aHR, 1.89; 95% CI, 1.27–2.80), lower insured income (aHR, 1.35; 95% CI, 1.01–1.81), recorded MVA with profound injuries before the index date (aHR, 6.16; 95% CI, 2.53–14.96) and frequency of ambulatory visits within the second year after the index date (aHR, 1.01; 95% CI, 1.004–1.02) (Table 4). The risk would be negatively associated with age at the index date for those initially diagnosed before the age of 30 as reference, which remained consistent within both time horizons of follow-up periods.
Risk factors of MVA with profound injuries in AS patients beyond 2 years after the index date.

A p-value < 0.05 is considered statistically significant.
Age at first AS diagnosis for AS patients, and date of first ambulatory visit for non-AS individuals.
Insured monthly income lower than median monthly income (⩽21,900 New Taiwan dollars/month).
AS, ankylosing spondylitis; CI, confidence interval; HR, hazard ratio; MVA, motor vehicle accident; OPD, outpatient department.
Discussion
For adult AS patients with pharmacological control in Taiwan, we found a higher risk of recorded MVA with profound injuries 2 years after diagnosis of AS compared with non-AS individuals. Factors including suburban and rural residence, lower insured income and recorded MVA with profound injuries at the emergency department before AS diagnosis might be associated with the risk in the following 7 years of AS course. Nonetheless, for those with follow-up periods >2 years, AS evolution and frequent ambulatory visits for disease control in the second year of the disease course were independent factors and considered to significantly increase the risk beyond 2 years after AS diagnosis. Diagnosis of AS at older ages, specifically >30 years, might be associated with a lower risk.
We observed a higher risk of recorded MVA with profound injuries with a temporal dependency, specifically in the period beyond 2 years after AS diagnosis, suggested by the significantly higher IRR for AS patients in this period and that AS diagnosis was an independent risk factor for those with follow-up periods >2 years. How AS disease progression might have affected the risk was rarely studied in the available epidemiological literature. Functional impairment in AS is largely associated with structural progression 23 and is correlated with radiographic progression in the spine or sacroiliac joints. 24 Prior studies revealed that the progression of radiographic sacroiliitis could be found as early as <2 years in patients with early axSpA25,26 and that structural changes in sacroiliac joints could be detected radiographically in an estimated 5%–10% of patients with non-radiographic axSpA within the first 2 years, increasing to 5%–40% within 10 years after diagnosis. 27 Based on the correlation between structural deterioration and mobility impairment, 28 our results did not contradict the abovementioned findings because we also presented the reduction in physical function connected with the progression of AS. Restriction in driving in AS patients was reported to be attributed to cervical spine involvement. 29 Concerning cervical spine involvement along the course of disease evolution, a Moroccan observational study reported that 19.6% of patients had radiological involvement after 5 years, and such involvement kept increasing in percentage thereafter, which indicated that cervical spine involvement causes physical disability mainly in later disease stages. For Taiwanese AS patients, a higher risk of developing obstructive sleep apnoea was reported, 30 and this was likely correlated with MVA. Of note, as recorded MVAs with profound injuries at the emergency department were investigated only, people experiencing MVAs that did not combine with injuries or those who did not seek medical attention could not be estimated from this study.
We also demonstrated the delayed diagnosis of axSpA as a major clinical challenge in Taiwan, with a mean diagnostic age of 42.1 years, and over half of the study subjects were diagnosed over the age of 40. Delayed diagnosis of AS is known to have worse functional outcomes. 31 To date, there are no available data on the definite duration of diagnostic delay in Taiwan, nor studies reporting clinical presentations in patients with diagnostic delay as the disease propagates. Such potential bias needs to be considered in the interpretation of our results.
Independent risk factors associated with MVA with profound injuries in both periods within and beyond 2 years after the index date included suburban and rural residence, lower insured income and recorded MVA with profound injuries before diagnosis. Factors in the period beyond 2 years after the index date additionally included AS diagnosis and frequent ambulatory visits for AS in the second year of the disease course, which was considered to prominently raise the risk thereafter. Morton et al. 32 found that diagnosis of axSpA is a factor associated with driving difficulty and that patients with uveitis showed greater difficulty with dynamic driving scenarios from their univariate regression analysis. Though our cohort had more study subjects, the development of uveitis was not found to be associated with the risk in our multivariable Cox regression models. This discrepancy is likely related to differences in study design and regression models, as well as reasons causing uveitis not recorded by ophthalmologists. Male patients are known to have more severe radiological progression, specifically in their early disease stages,33,34 and our results showed no contradiction. Patients residing in nonmetropolitan districts and receiving lower monthly income were shown with a higher risk. It coincided with Taiwanese real-world presentations 16 and these patients might tend to be older, in physical-intensive roles, and face presenteeism and reduced work productivity. 35 History of MVA with profound injuries before AS diagnosis was recognised as the most dominant risk factor throughout the follow-up period. Because prior mechanical stress or injury could trigger immune activation and cause the onset and progression of AS in susceptible patients, 36 disabling sequelae and disease progression might incur following MVA. In Taiwanese real-world practice, frequent ambulatory visits likely reflect disease conditions, inflammatory severity or complications necessitating close monitoring. The association between frequent ambulatory visits within the second year of disease follow-up and the risk in patients with follow-up periods >2 years suggested a persistently higher inflammatory activity or complications associated with the higher risk. Lastly, we found those with AS initially diagnosed at ages >30 years to be negatively associated with MVA with profound injuries. However, one study suggested both age-related and AS-specific changes might make elder AS patients more at risk. 37 This finding did not coincide with what prior studies demonstrated,16,17 which might partially reflect that elder AS patients had suffered from severe physical impairments that restricted them from motor vehicle use. Also, juvenile-onset patients are more likely to manifest with peripheral involvement. 38 Therefore, early administration of effective treatment is necessary. 39
We revealed no significant influence of selected psychiatric comorbidities and psychoactive agents on the risk though they were considered risk factors for MVA.40–42 This might reflect the prominent underdiagnosis of included psychiatric comorbidities in Taiwan. The impact of dosages of selected psychoactive agents and subjects’ adherence to medications were not sufficiently explored in this study. These might potentially bias our results.
MVA is a great concern for patients as it can cause permanent damage or disabilities. We revealed the 2 years of disease evolution before a significantly increased risk of MVA with profound injuries, which is shorter than the pooled mean diagnostic delay of 6.7 years. 43 Our results indicated that strategies aiming for timely recognition, effective treatment and comprehensive monitoring of early axSpA might be mandatory. For rheumatologists, definitive instructions on the risk of MVA accompanying disease evolution and corresponding prevention deserve a thorough education for those patients with the risk factors. Our results can provide a reference for Taiwanese administrative authorities to support the implementation of prompt policies.
This study has several limitations. First, some limitations regarding database research exist. Diagnostic accuracy of AS, covariates and outcomes in administrative databases could not be fully confirmed though validated in previous studies, and thus the misclassification bias could not be prevented, either. Potential confounders such as occupation, education level, smoking status, 44 alcohol use, 45 disabilities without obtainable diagnostic codes, alternative substances use, dosages of prescriptions, patients’ compliance to prescriptions, stressful events, 46 family history, laboratory recordings and disease activity could not be adjusted. Neither could issues regarding regional terrain and climate, process of patient involvement in MVA, types of involved vehicles and profiles of regional traffic networks and habits. However, we had enhanced diagnostic accuracy by some measures mentioned in our methods. We matched for gender, age at index date and year of index date to adjust for age of initial AS diagnosis and AS disease duration. We also explored the association between the frequency of ambulatory visits and MVA as the proxy of the association between persistently higher inflammatory activity and MVA. We had adjusted for potential confounders, including psychiatric disorders and alcoholism, as possible under accessible resources of administrative database research. Second, the causal relationship could not be confirmed due to retrospective use of claims data, so we stated association and associated factors in this study. Third, the time horizon of within 1 year before the index date was set to detect continuous exposure to potential confounders and the range of available claims data from 2003 to 2013, determination of the influence of potential confounders occurring longer before the index date was limited. Fourth, because the study population does not represent the entire AS population, but rather represents relatively more severe patients, we cannot extrapolate the results to AS patients with milder severity or without prescriptions. Fifth, the generalisability of our results to regions other than Taiwan was limited owing to regional geographical and administrative differences.
Despite these limitations, population-based administrative databases provided reliable data and minimised selection bias. Also, we conducted sensitivity analyses using different time horizons of disease courses for risk stratification. Following studies bearing prospective designs, longer follow-up periods or methods allowing definitive recording of real exposed dosage and duration of medications, use of tobacco and alcohol, comorbidities, and information on disease activity are warranted to confirm our findings.
Conclusion
This nationwide, population-based cohort study on adult Taiwanese AS patients with pharmacological control showed that factors such as AS disease evolution and frequent ambulatory visits for disease control in the second year of the disease course may significantly increase the risk of recorded MVA with profound injuries beyond 2 years after AS diagnosis.
Supplemental Material
sj-docx-1-tab-10.1177_1759720X241273039 – Supplemental material for Risk of motor vehicle accidents with profound injuries in patients with ankylosing spondylitis: a nationwide, population-based cohort study
Supplemental material, sj-docx-1-tab-10.1177_1759720X241273039 for Risk of motor vehicle accidents with profound injuries in patients with ankylosing spondylitis: a nationwide, population-based cohort study by Chung-Mao Kao, Wei-Li Ho, Yi-Ming Chen, Tsu-Yi Hsieh, Wen-Nan Huang, Yi-Hsing Chen and Hsin-Hua Chen in Therapeutic Advances in Musculoskeletal Disease
Supplemental Material
sj-docx-2-tab-10.1177_1759720X241273039 – Supplemental material for Risk of motor vehicle accidents with profound injuries in patients with ankylosing spondylitis: a nationwide, population-based cohort study
Supplemental material, sj-docx-2-tab-10.1177_1759720X241273039 for Risk of motor vehicle accidents with profound injuries in patients with ankylosing spondylitis: a nationwide, population-based cohort study by Chung-Mao Kao, Wei-Li Ho, Yi-Ming Chen, Tsu-Yi Hsieh, Wen-Nan Huang, Yi-Hsing Chen and Hsin-Hua Chen in Therapeutic Advances in Musculoskeletal Disease
Footnotes
Acknowledgements
We would like to thank Ms. Chia-Hui Yu and the Biostatistics Task Force of Taichung Veterans General Hospital for their assistance in performing the statistical analysis.
Declarations
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.